
Abstract
The Coronavirus Disease of 2019 (COVID-19) pandemic has caused significant delays in the delivery of cancer treatments in Canada. As cancer treatment and imaging volumes return to normal, radiologists will encounter more cases of chemotherapy-induced toxicities. These toxicities have varied appearances on imaging, and can affect multiple organ systems. The purpose of this review is to offer a unified resource for general radiologists regarding the imaging appearances of chemotherapy-induced toxicities.
Introduction
Chemotherapy has been a longstanding option in the treatment armamentarium for malignancy. In recent years, there has been a shift in the traditional treatment of cancer towards precision medicine, with new chemotherapeutic agents targeting a tumor’s specific genetic or molecular profile to decrease treatment side-effects and ultimately improve treatment efficacy.
The Coronavirus Disease of 2019 (COVID-19) pandemic has caused significant delays in the delivery of cancer treatments in Canada. As vaccine campaigns continue to gain traction globally, and a return to normal ensues, many patients in the upcoming months will be diagnosed with cancer and begin treatment. Consequently, we anticipate radiologists will encounter chemotherapy-related toxicities at a higher rate than in past years.
The purpose of this review is to offer a unified resource for general radiologists regarding the varied imaging appearances of chemotherapy-induced toxicities.
Overview of Chemotherapeutic Agents
There are many classes of chemotherapy agents which have different mechanisms of action. Traditional chemotherapy agents act on different stages of the cell cycle to result in cell death. Although traditional chemotherapy has a greater impact on rapidly proliferating malignant cells, normal host cells with a shorter cell cycle, such as those in the gastrointestinal tract, can still be affected. Newer chemotherapeutic agents, such as monoclonal antibodies or immune checkpoint inhibitors (ICI), utilize the host’s immune system to specifically target cancer cells, in an effort to make the treatment target more specific and mitigate the impact on healthy host cells.
Chemotherapy Agent Classes, Mechanism of Action, and Examples.
Imaging Appearance of Chemotherapy Toxicities
Neurologic
Brain
Magnetic resonance imaging (MRI) is the imaging modality of choice in diagnosing chemotherapy-induced neurotoxicity, although distinguishing this entity from disease progression, infection, or paraneoplastic syndromes remains challenging. Medication history and/or improvement with cessation of therapy is often crucial in arriving at this diagnosis.
Toxic leukoencephalopathy is an encephalopathy that manifests due to injury of white matter, particularly myelin.
1
Clinical presentation is variable, depending on the acuity of disease and the white matter tracts affected.
1
Symptoms range from confusion to severe neurological dysfunction.
1
Chemotherapeutic agents are a well-described class of medications that can result in toxic leukoencephalopathies. For example, methotrexate can result in a leukoencephalopathy when given in high doses, such as in the treatment of hematologic malignancies.
2
Other chemotherapeutic agents that have been associated with toxic leukoencephalopathies include carmustine, cisplatin, cytarabine, 5-fluorouracil, ifosfamide, thiotepa, interleukin-2, and interferon alpha.
3
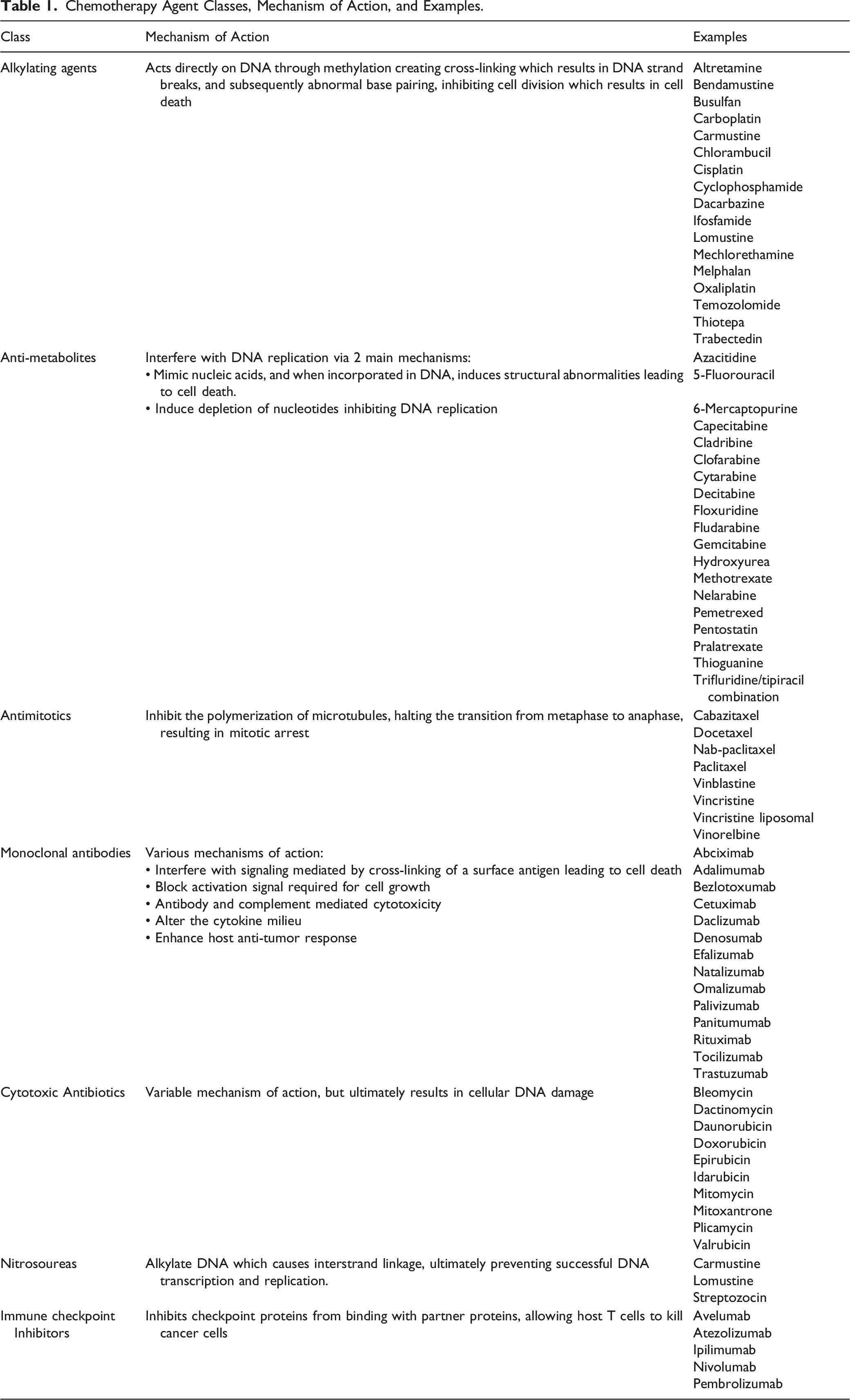
MRI findings include confluent and symmetric T2 hyperintense white matter abnormalities, that can involve the corpus callosum, without associated mass effect (Figure 1).
3
Restricted diffusion is variable, and contrast enhancement is usually absent.
3
Toxic leukoencephalopathy in a 70-year-old female with left parietal CNS lymphoma treated with chemotherapy. Axial FLAIR images (Figures 1A and 1B) show symmetric high signal intensity in the bilateral periventricular white matter, corona radiata, and centrum semiovale. Increased signal is also identified in the genu of the corpus callosum. There is also subcortical white matter signal abnormality in the left parietal lobe (arrows), in the original location of the tumor.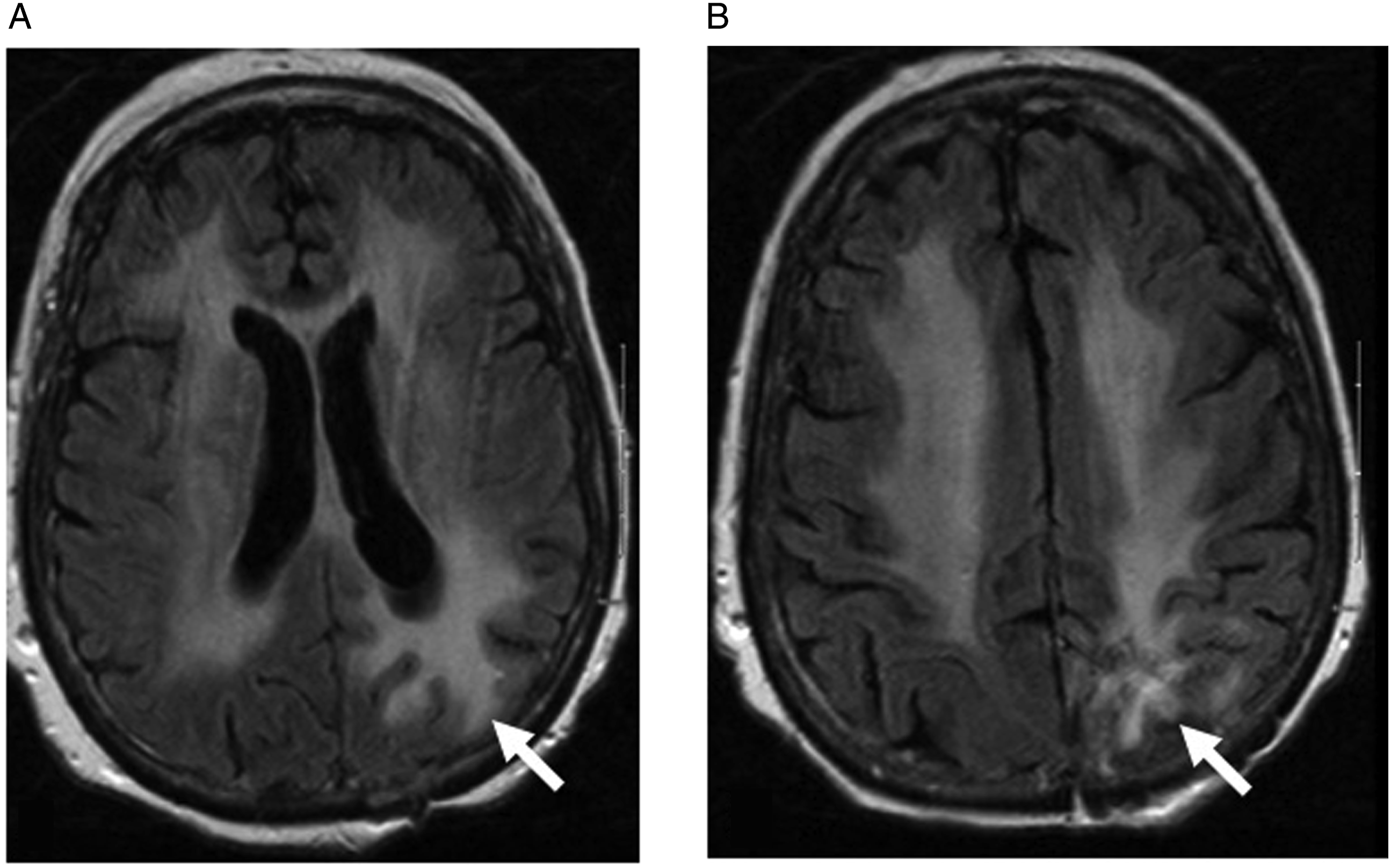
Posterior reversible encephalopathy syndrome (PRES) is a neurotoxic state due to a disorder of cerebrovascular autoregulation, with hyperperfusion in the posterior circulation, resulting in vasogenic edema. Posterior reversible encephalopathy syndrome is more commonly associated with the treatment of solid tumors rather than hematologic malignancies or primary brain tumors.
4
Chemotherapy agents that have been associated with PRES include cisplatin, cyclophosphamide, methotrexate, bevacizumab, and rituximab.3,4 MRI is the gold standard in making this diagnosis, with computed tomography (CT) appearing normal in up to 37% of patients.
4
MRI shows symmetric subcortical white matter T2 hyperintensity, classically involving the occipital and parietal lobes, without restricted diffusion or enhancement (Figure 2). Atypical PRES can also be seen in the subcortical white matter of the frontal and temporal lobes.
5
Imaging findings are typically reversible once the offending agent is removed, although this is not always the case. Chemotherapy-induced PRES in a 46-year-old female with altered level of consciousness and bilateral visual deficits. Axial FLAIR images (Figures 2A and 2B) show high signal intensity in the subcortical white matter of both parietal and occipital lobes.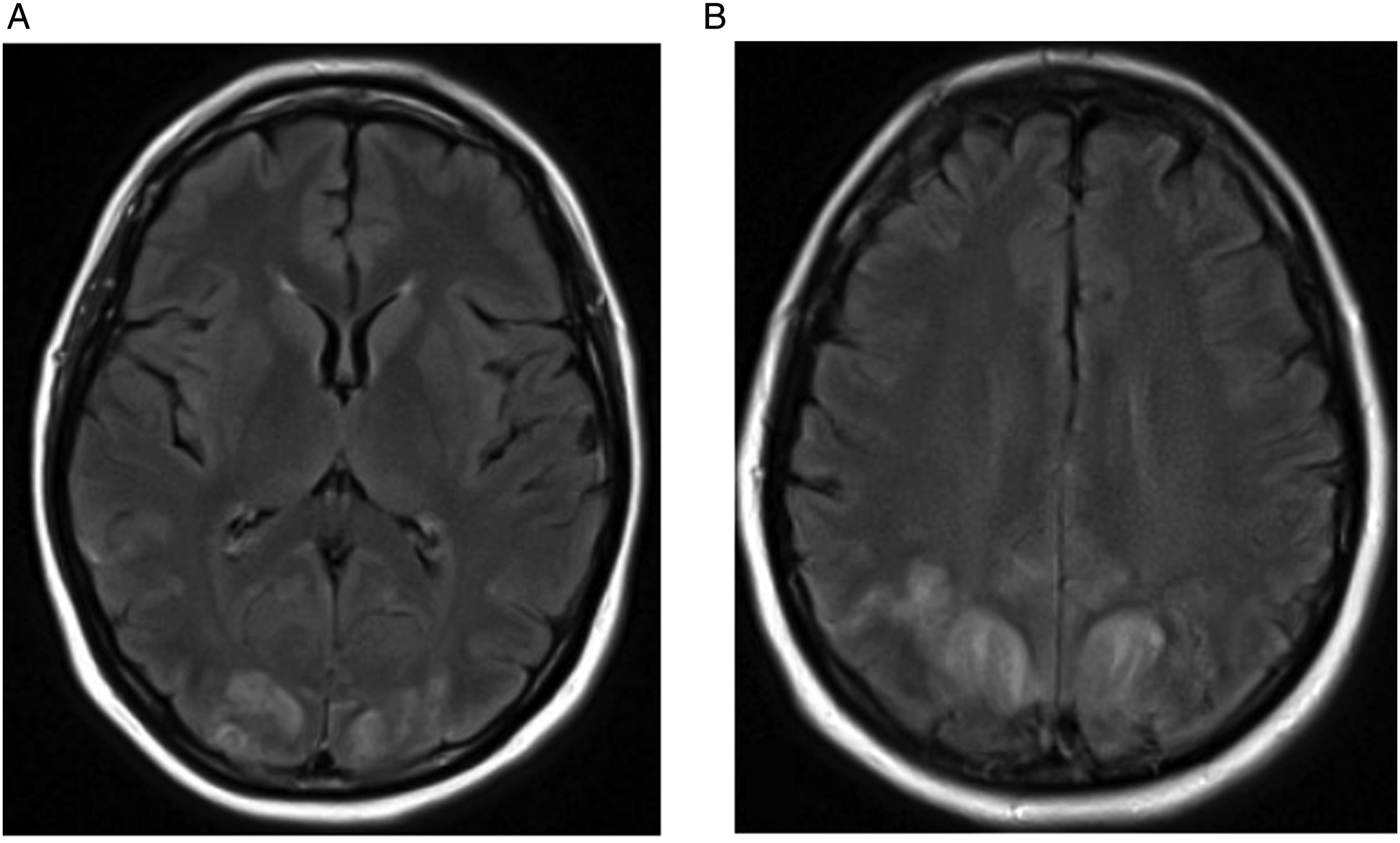
Chemotherapy-related hypophysitis is a well-described phenomenon, particularly with ICIs such as ipilimumab, nivolumab, and pembrolizumab.
6
The incidence of hypophysitis with this class of medications is up to 9%.
6
Clinically, headache is the most commonly reported initial symptom. Additional symptoms include confusion, memory loss, erectile dysfunction, polyuria, polydipsia, and cold intolerance.
6
Classically on MRI, there is diffuse enlargement of the pituitary gland, with or without infundibular thickening (Figure 3).
3
Neuroimaging abnormalities precede the clinical symptoms in approximately 50% of cases.
6
A baseline MRI of the pituitary gland was normal (not shown). Sagittal T1-WI post gadolinium MRI (Figure 3A) 2 months later demonstrates an enlarged and thickened pituitary gland and infundibulum in a patient receiving immune checkpoint inhibitors for melanoma. Follow-up MRI (Figure 3B) 7 weeks after discontinuation of immunotherapy and administration of steroid treatment showed resolution of findings.
Cerebral venous sinus thrombosis (CVST) is another possible complication related to chemotherapy. The underlying pathogenesis of how this class of medications results in increased thrombosis remains unclear. Hypotheses include direct vascular injury or endothelial cell dysfunction. Cisplastin-based chemotherapy, bevacizumab and L-asparaginase have been reported as causative agents.3,7,8 CT or MR venogram is used to diagnose CVST, which is characterized by filling defects within the cerebral venous sinuses, with potential complications including ischemic or hemorrhagic infarcts.
Spine
Myelopathy is increasingly recognized as a chemotherapy-related toxicity, particularly when the chemotherapy agent is administered via an intra-thecal approach. This type of myelopathy occurs most frequently with methotrexate and cytarabine regimens.9-11 MRI findings include cord edema with variable contrast enhancement. Many authors have described a predilection of dorsal column involvement which can mimic subacute combined degeneration of the cord.9,10
Thyroid
Thyroiditis has been described as a possible complication of chemotherapy.12-14 Once again, this is more recognized with ICIs, as this class of medication is associated with autoimmune toxicity. 12 Typically, thyroiditis is diagnosed clinically with bloodwork, evidenced by elevated T3/T4 and low TSH levels, and positive thyroid peroxidase antibodies. Thyroid ultrasound may show heterogeneous thyroid parenchyma with hyperemia.
Chest
Lungs
Pulmonary abnormalities are the most common imaging manifestation of chemotherapy-related toxicity. Chemotherapy-related lung injury is not associated with the duration of treatment, although there is a relationship with dose. 10 Bleomycin and ICIs in particular can result in drug-related pulmonary complications. 15 The highest frequency of drug-induced pneumonitis has been reported in patients undergoing treatment for breast and lung cancer. 15 Frequent clinical symptoms are dyspnea, dry cough, and fever. 15
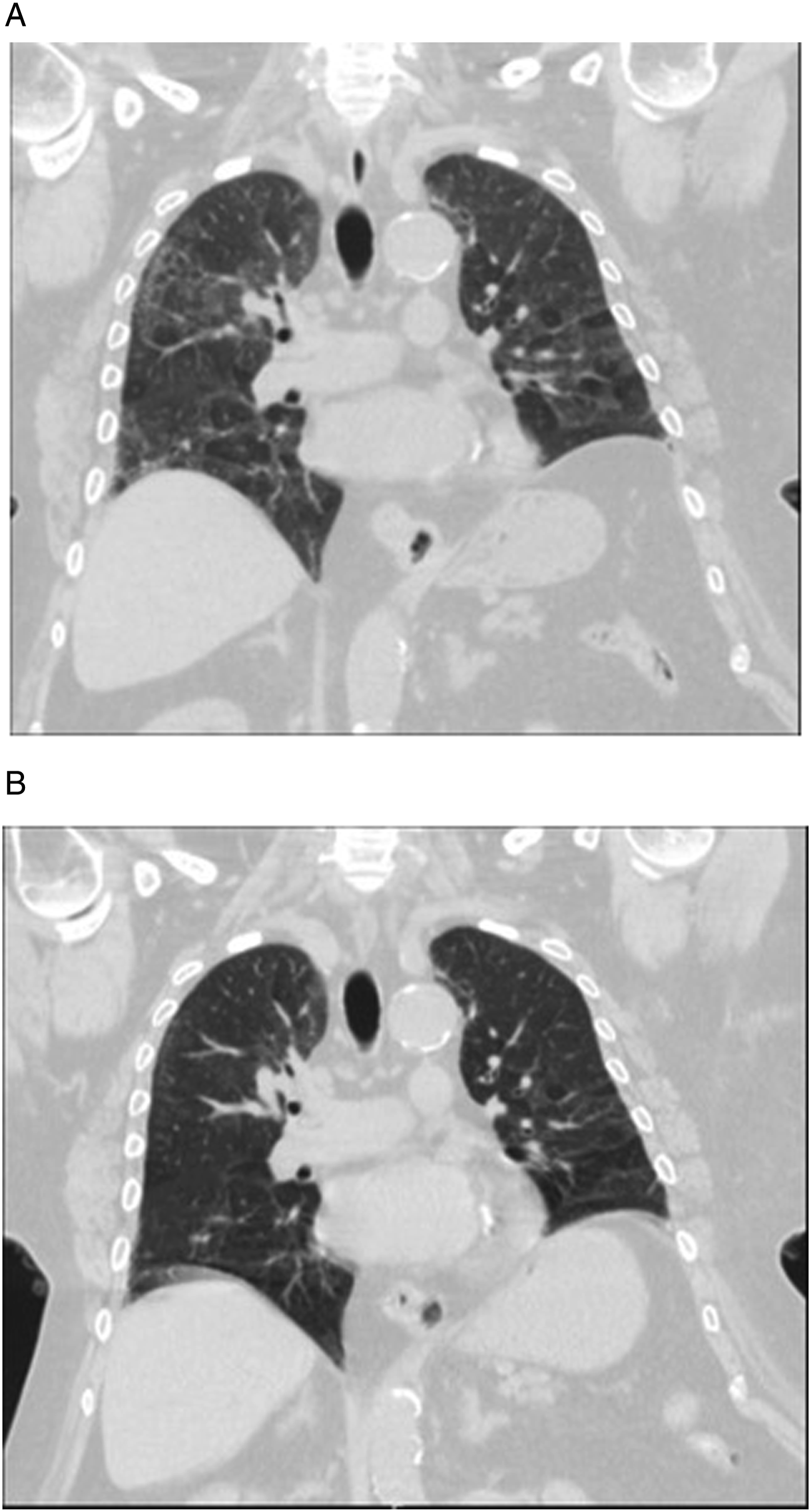
The most common radiological patterns for chemotherapy-related lung injury using the American Thoracic Society classification for idiopathic interstitial pneumonia are non-specific interstitial pneumonia (NSIP), cryptogenic organizing pneumonia (COP) (Figure 4), acute interstitial pneumonia (AIP), hypersensitivity pneumonitis (Figure 5), and unclassifiable interstitial pneumonia.
15
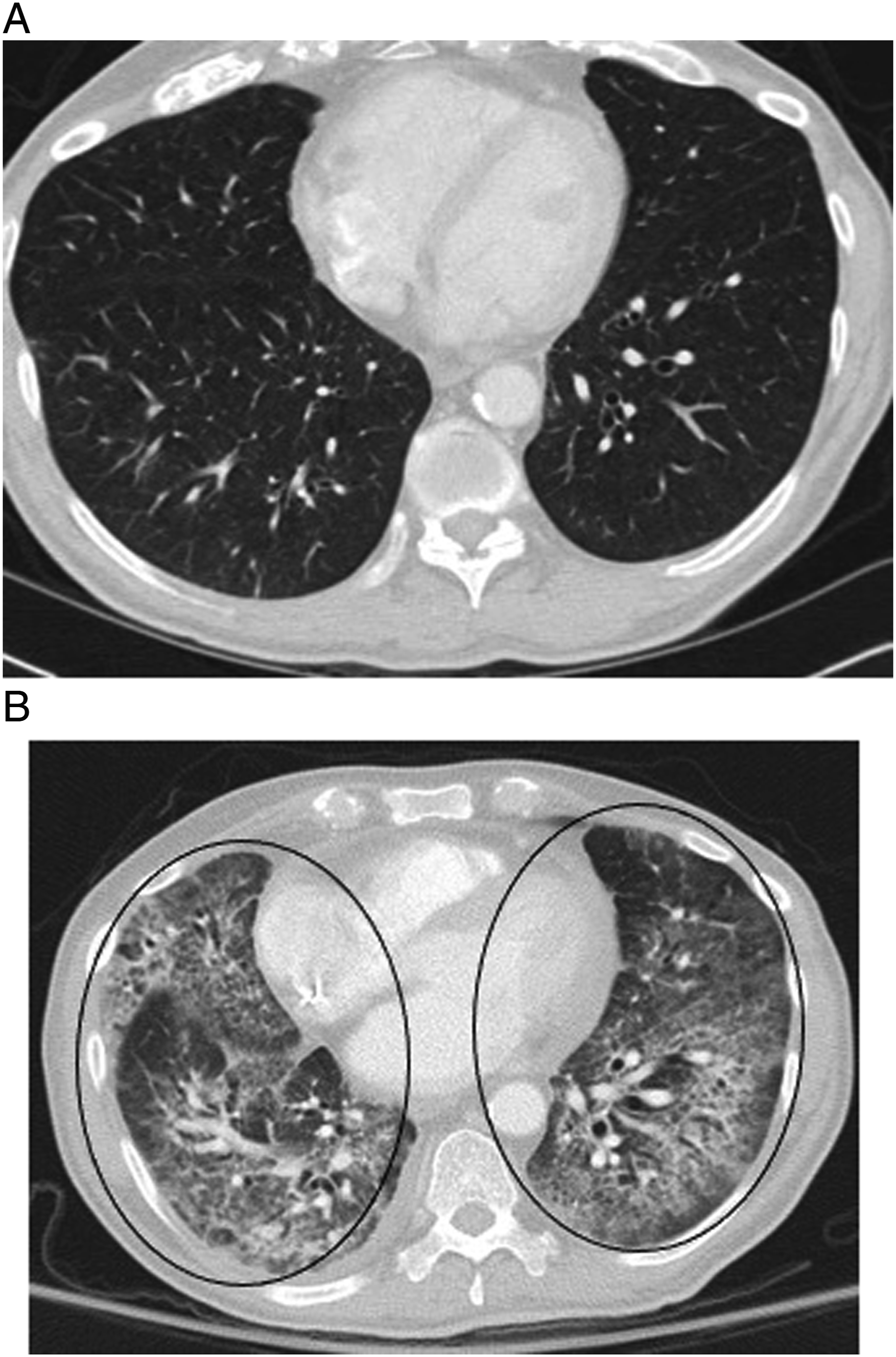
Ground-glass opacities are a common finding, and given that infection is the leading differential, bronchoscopy may be required to clarify the diagnosis (Figure 6). One study found that 60% of patients with chemotherapy-related lung injury who were initially asymptomatic, but were continued on their treatment regimen, eventually developed symptoms.
15
It is thus critically important that radiologists raise the possibility of drug-related lung injury when appropriate. Treatment includes cessation of therapy, usually with a course of steroids. 55-year-old man with melanoma involving the upper back receiving immunotherapy treatment with nivolumab who developed multiple subpleural predominant nodular opacities (white arrows) with a periobronchovascular distribution on axial contrast-enhanced chest CT (Figure 4A). A chronic right pleural effusion was also present. Follow-up chest CT at 4 months showed evolution of these nodular peribronchovascular opacities, some of which have a more ill-defined ground-glass appearance (black arrowhead), and others demonstrating a reverse halo or atoll sign (black arrows) suggestive of organizing pneumonia (Figure 4B). Nivolumab was stopped and follow-up imaging 6 months later showed significant improvement with subtle residual ground-glass opacities (white arrowheads) (Figure 4C). 75-year-old female on paclitaxel for breast cancer with symptoms of dry cough and exertional shortness of breath. Coronal chest CT revealed mosaic attenuation of the lungs with upper lobe predominant peripheral reticulation most compatible with a hypersensitivity pneumonitis imaging pattern (Figure 5A). Paclitaxel was discontinued and the patient was given a short course of prednisone. A follow-up chest CT 3 months later showed improvement in the previously seen imaging findings (Figure 5B). Case courtesy of Dr [Prasaanthan Gopee-Ramanan]. 65-year-old male with metastatic parotid cancer treated with docetaxel who fell and was found to be profusely hypoxic. Chest CT shows extensive ground-glass opacities (circles) and bronchiectasis throughout the lungs (Figure 6B). Imaging from 1-month prior revealed normal lung parenchyma (Figure 6A). The imaging findings raised suspicion for docetaxel-induced lung injury. Bronchoscopy with bronchial lavage showed 70% lymphocytes confirming the diagnosis of docetaxel-induced pneumonitis/lung injury.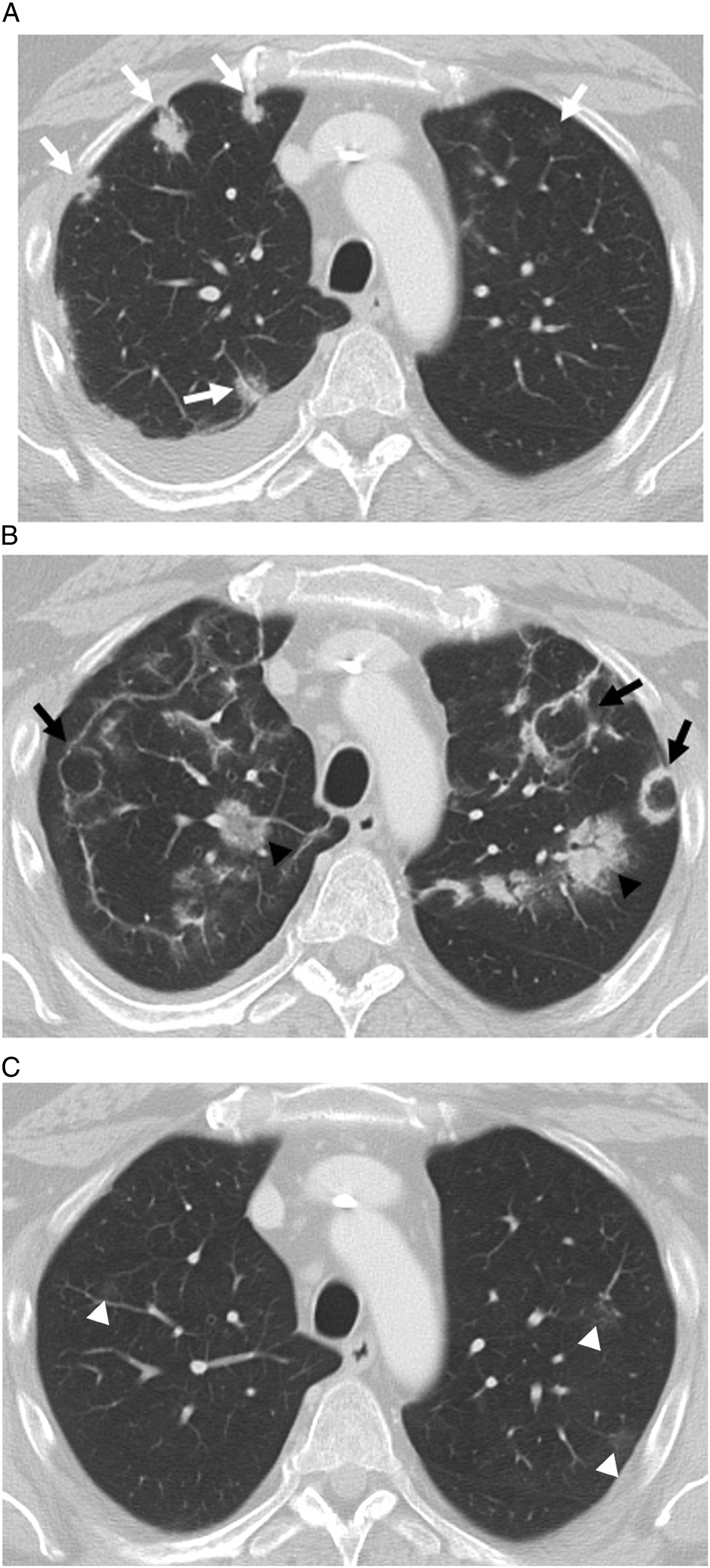
Capillary leak syndrome is a condition characterized by an increase in vascular permeability causing an extravasation of fluid and proteins that can result in interstitial pulmonary edema. 16 It is associated with several chemotherapy agents including interleukin-2, interferons, and gemcitabine. The most common imaging findings are diffuse airspace disease and ground-glass opacities. 16 Radiologists can add value by suggesting this diagnosis in cases of new-onset pulmonary edema as the treatment requires steroids in addition to diuretic therapy. 16
Pleura
Chemotherapy-induced pleural effusions are uncommon. Patients with acute promyelocytic syndrome treated with all-trans retinoic acid may be more susceptible to developing pleural effusions. 17
Vascular System
Chemotherapy-induced atherosclerosis is common and can lead to a number of cardiovascular complications including hypertension, valvular disease, and cardiomyopathy. 18
Accelerated atherosclerosis has been documented following treatment with tyrosine kinase inhibitors (TKIs), anti-metabolites, and anthracyclines which consequently causes hypertension and an increased risk for cardiovascular disease. 18
Bevacizumab, 5-FU and carboplatin-based agents are associated with increased risk of arterial thromboembolic events, especially in those above the age of 65. 19 Acute thrombotic occlusion of the aorta is extremely rare, but has been documented following cisplatin-based therapy. 20
Venous thromboembolism (VTE) has been associated with several chemotherapeutic agents. The pathophysiology for this is not well understood, with one theory suggesting that chemotherapy-induced apoptosis may cause weakening of the endothelium, exposure of the basement membrane, and then activation of the coagulation cascade. 16 Immunomodulatory imide drugs, such as thalidomide, have been associated with a 10–40% risk of VTE in multiple myeloma patients when given in combination with glucocorticoids or other chemotherapy agents. 21 Cisplatin, and less commonly fluorouracil, have also been associated with increased VTE risk. 21
Heart
Chemotherapy-related cardiomyopathy varies in its phenotype, with some agents damaging myocytes, while others cause coronary artery damage.
Chemotherapy-related cardiac toxicity is most commonly associated with anthracycline treatment.
22
Anthracycline-related cardiomyopathy is typically characterized by dilated atria, a dilated left ventricle, and mitral and tricuspid valve insufficiency.
22
Chemotherapy-induced cardiac toxicity is best monitored using echocardiography by trending a patient’s ejection fraction.
22
Cardiac MRI may have a role in detecting myocardial edema, inflammation, or fibrosis (Figure 7).23,24 CT and PET are less useful, but can be used to identify coronary artery atherosclerosis and cardiac inflammation, respectively.25,26 75-year-old woman treated with pembrolizumab for metastatic urothelial carcinoma. The patient developed shortness of breath and an echocardiogram showed decreased cardiac function. T2 mapping (Figure 7A) shows elevated T2 signal within the myocardium consistent with inflammation. Late gadolinium-enhanced images (Figure 7B) show patchy mid myocardial enhancement of the inferior wall of the left ventricle in the base and mid ventricle. Findings were consistent with tyrosine kinase inhibitor toxicity.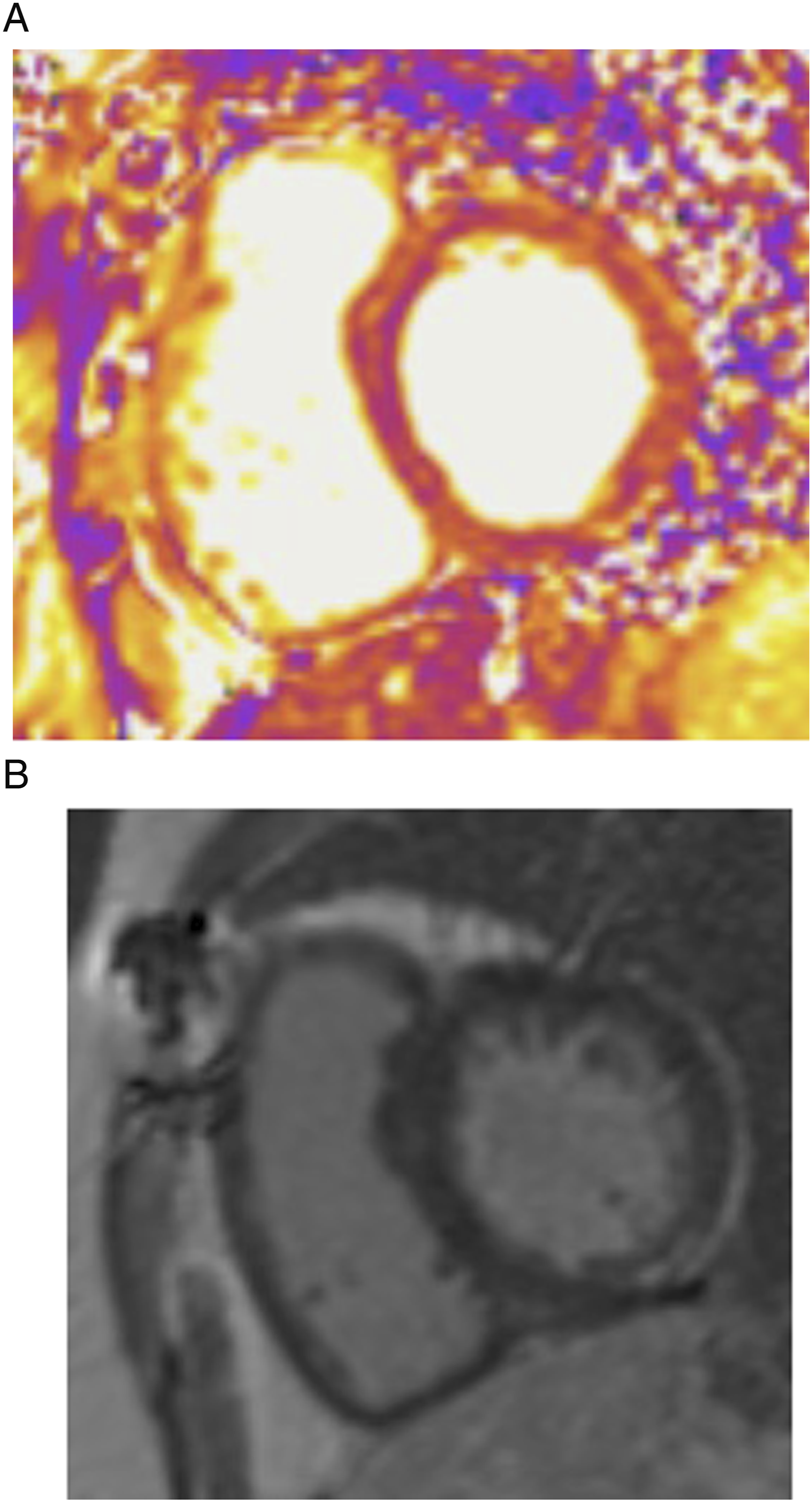
Pericardial effusions and pericardial disease have been observed following treatment with anthracycline, all-trans retinoic acid, alkylating agents, and cyclophosphamides.27-30 Suggested mechanisms of injury include increased capillary permeability and pericardial fibrosis. 31
Abdomen
Liver
Chemotherapy-induced hepatopathy includes a variety of parenchymal and vascular pathologies. Specific agents which can cause hepatotoxicity are extensive, and depend on whether the agent is dependent on liver metabolism or if it causes direct hepatic toxicity. 32 Clinically, the presentation can vary from asymptomatic with increased liver enzymes on bloodwork, to fulminant hepatic failure. 32 Although liver function tests are monitored throughout treatment, hepatotoxicity is not always accompanied by biochemical derangements. 33 Consequently, radiologists play a key role in highlighting findings of hepatotoxicity to treating clinicians.
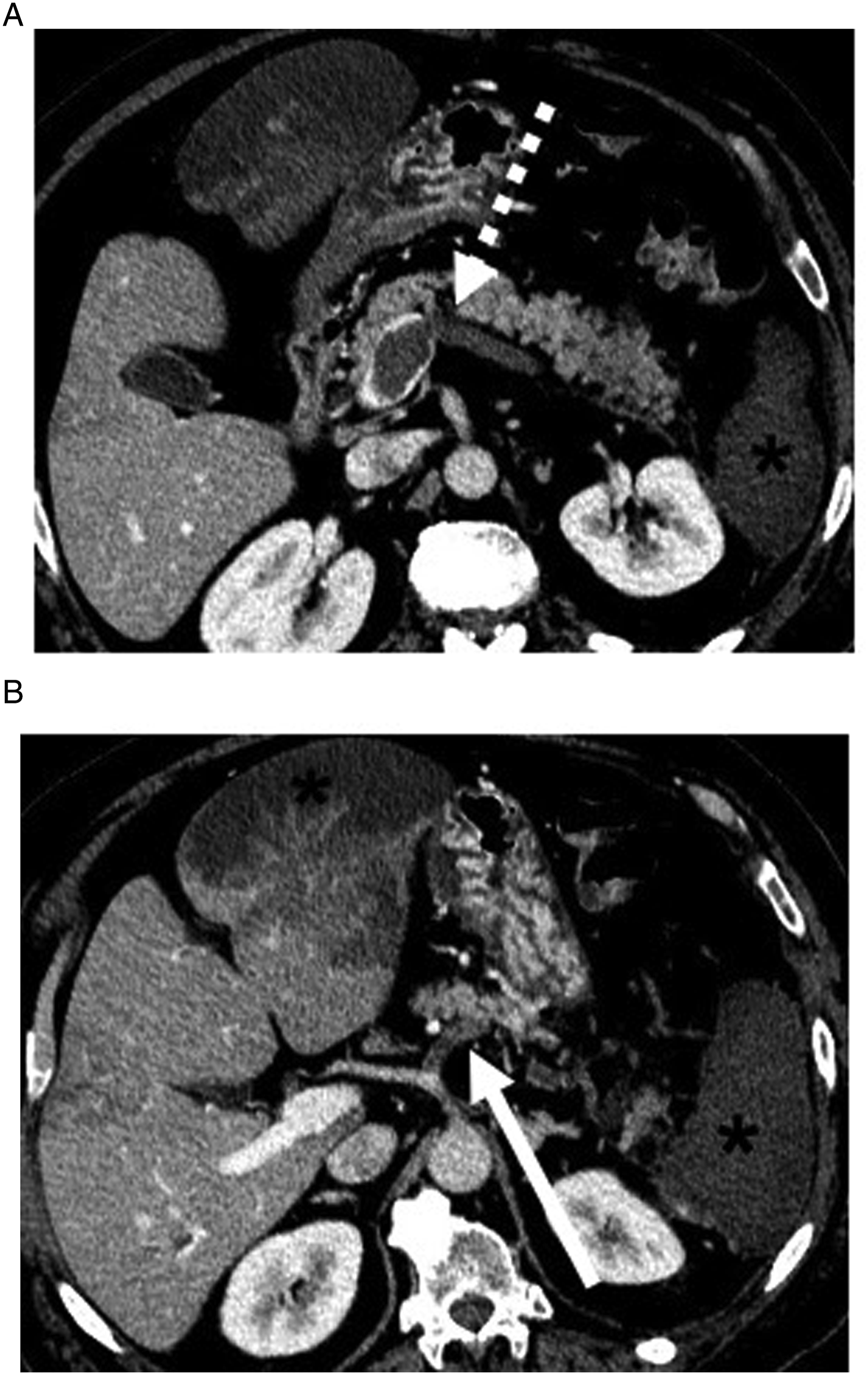
From an imaging perspective, acute hepatocellular injury demonstrates non-specific imaging appearances ranging from hepatomegaly, heterogeneous liver enhancement, pseudolesions (Figure 8), ascites, arterial or venous thrombus (Figure 9), altered portal venous flow, and periportal edema.
34
Findings associated with chronic injury include focal or diffuse fibrosis, pseudocirrhosis, and portal hypertension. 54-year-old male with non-small cell lung cancer treated with ceritinib. CT of the abdomen and pelvis revealed multiple new hypodense lesions in the liver initially interpreted as disease progression. The patient underwent liver biopsy which confirmed TKI drug-induced hepatitis. 68-year-old male with non-small cell lung cancer, right lower quadrant pain and leukocytosis. Axial contrast-enhanced CT of the abdomen and pelvis revealed thrombosis of the left and right hepatic arteries (not shown), splenic artery (Figure 9B, solid arrow), and portal venous system (Figure 9A, dashed arrow) with resultant liver and splenic infarcts (*). Findings were related to cisplatin-induced arterial and venous thrombosis.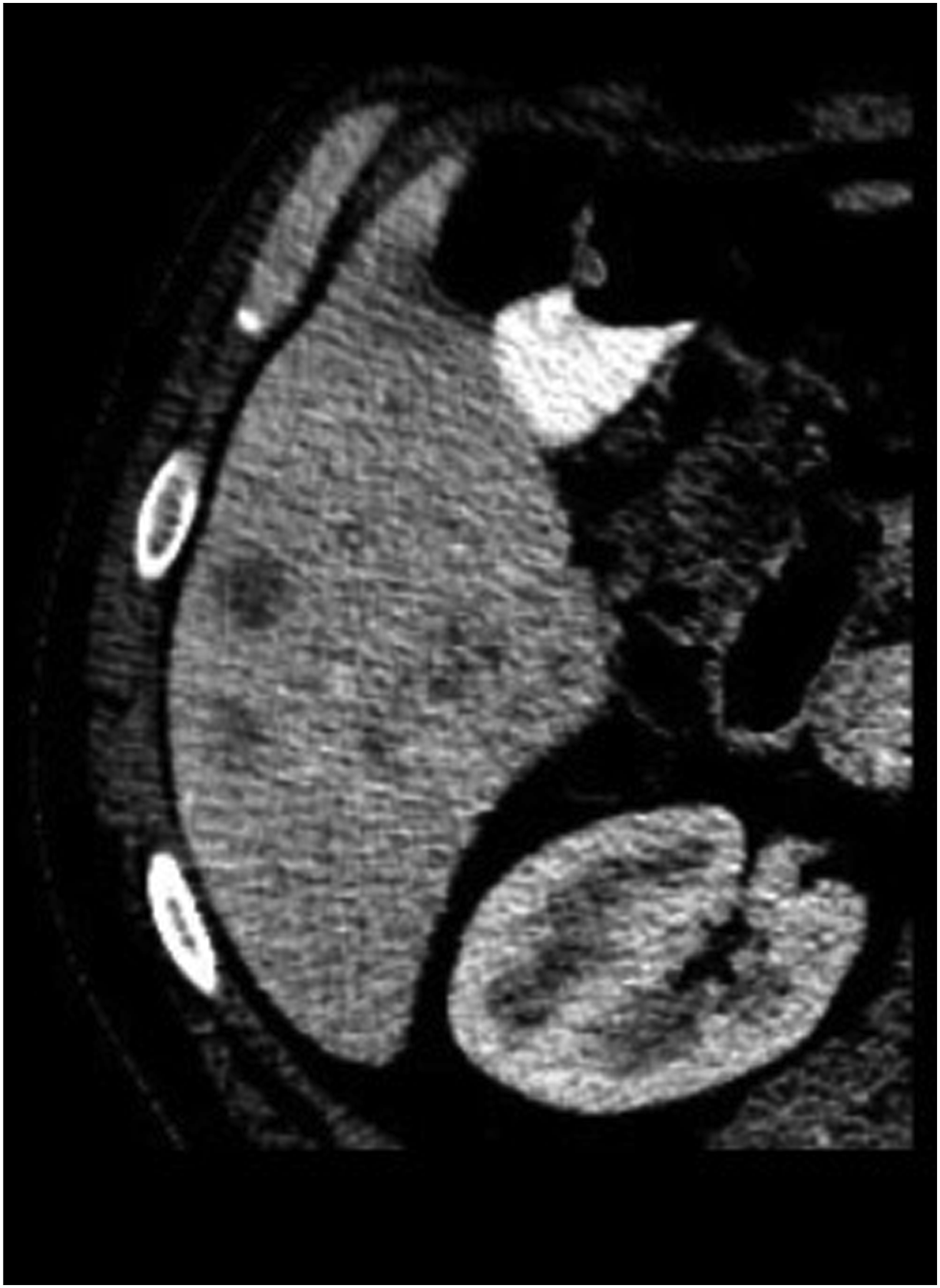
Steatosis and steatohepatitis are also commonly seen with chemotherapy agents, such as TKIs and tamoxifen, reportedly in 28–47% of patients. 34 US and CT can be used to diagnose hepatic steatosis; however, MRI remains the best non-invasive imaging modality to quantify intrahepatic fat. 34
Hepatic vascular complications include sinusoidal obstruction syndrome (SOS) (also known as veno-occlusive disease) which can be a life-threatening complication. 34 Several chemotherapeutic agents have been associated with SOS. It has been most commonly described with oxaliplatin which is used in the treatment of colon cancer. 34 Indirect signs of SOS include hepatosplenomegaly, ascites, a pulsatile portal vein, hepatofugal flow, loss of the triphasic hepatic venous waveforms, gallbladder wall thickening, portosystemic varices, and heterogeneous liver enhancement. 34 Gadoxetic acid-enhanced MRI has a sensitivity of 75% and specificity of 96–100% in the diagnosis of SOS which is evidenced by hypointense reticular hepatic parenchyma in the hepatobiliary phase. 35
Biliary Tree
Chemotherapy-induced cholecystitis, particularly as a complication of molecular targeted therapies, has been described.36,37 Findings on US or CT include gallbladder wall thickening/edema, gallbladder distension, wall hyperemia, and pericholecystic fluid. 38
Biliary tree inflammation can be caused by many chemotherapeutic agents such as asparaginase, doxorubicin, paclitaxel, sorafenib, and sunitin. 39 This injury is primarily due to irritation caused by medication excretion through the biliary system. Radiologically, this injury is detected as biliary/peribiliary tree enhancement with or without biliary strictures. Biliary sclerosis following initiation of hepatic arterial infusion of floxuridine for the treatment of metastatic colon cancer to liver is well-documented. 40
Pancreas
Chemotherapy-induced pancreatitis has been associated with asparaginase, cisplatin, cytarabine, and TKIs.41,42 Imaging findings such as pancreatic edema and surrounding fat stranding may suggest chemotherapy-associated pancreatitis, although these signs may not always be present, and correlating with serum lipase levels and epigastric pain may be required to reach this diagnosis. CT is the best modality for evaluation of acute pancreatitis and its potential complications. 43
Pancreatic atrophy is another potential complication associated with chemotherapy treatment, specifically with TKIs. 44 It is important to document the degree of atrophy as the clinical significance depends on the treatment regimen. For example, pancreatic atrophy related to sunitinib is associated with shorter survival, while pancreatic atrophy due to sorafenib is associated with better tumor response and overall survival. 45 On imaging, pancreatic atrophy is demonstrated by parenchymal volume loss with fatty infiltration of the gland.46,47
Spleen
Chemotherapeutic toxicity can result in splenomegaly and has been described in colorectal cancer patients treated with oxaliplatin. 48 Chemotherapy-related splenomegaly is clinically significant as splenic enlargement is associated with an increased risk of thrombocytopenia. 48
Kidneys
Nephrotoxicity has been associated with many chemotherapeutic agents such as cisplatin, ifosfamide, vascular endothelial growth factor (VEGF) receptor-targeted molecular agents, and methotrexate. Imaging findings for various nephrotoxicities are non-specific and usually renal biopsy is required to make a definitive diagnosis. 49
Interstitial nephritis, which is associated with iplimumab and sorafenib, may be demonstrated on imaging by enlarged kidneys, a persistent nephrogram, renal edema, or a striated nephrogram sign. 49 Nedaplatin has been linked to papillary necrosis and is best diagnosed on CT urogram as excavation of the calyces, regression of the renal papillae, and blunting of the renal calyces. 49 Acute tubular necrosis, which can be caused by agents such as cisplatin, ifosfamide and imatinib, can manifest as increased cortical echogenicity on US or parenchymal contrast retention on CT. 49
Methotrexate and combination cisplatin and gemcitabine regimens are associated with an increased risk of renal infarct, best seen on CT as wedge shaped areas of non-enhancement or hypoenhancement of the renal cortex and the cortical rim sign. 49
Crizotinib, which is a TKI used in the treatment of metastatic non-small cell lung cancer, can result in the development of complex renal cysts which regress after cessation of therapy. 49 The clinical significance of this is not well understood at this time.
Adrenal Glands
Primary adrenal insufficiency secondary to ICIs has been reported, but is rare.50-52 Adrenal insufficiency cannot be diagnosed by imaging alone; however, it can be suggested by severe adrenal gland atrophy.
Gastrointestinal Tract
Gastrointestinal toxicity as a result of chemotherapy is common, hypothesized to be caused by reduced stem cell reserves, reduced cellular repair functionality, and protein loss. 53 Common causative chemotherapeutic agents include VEGF and VEGFR inhibitors and antiangiogenic TKIs.
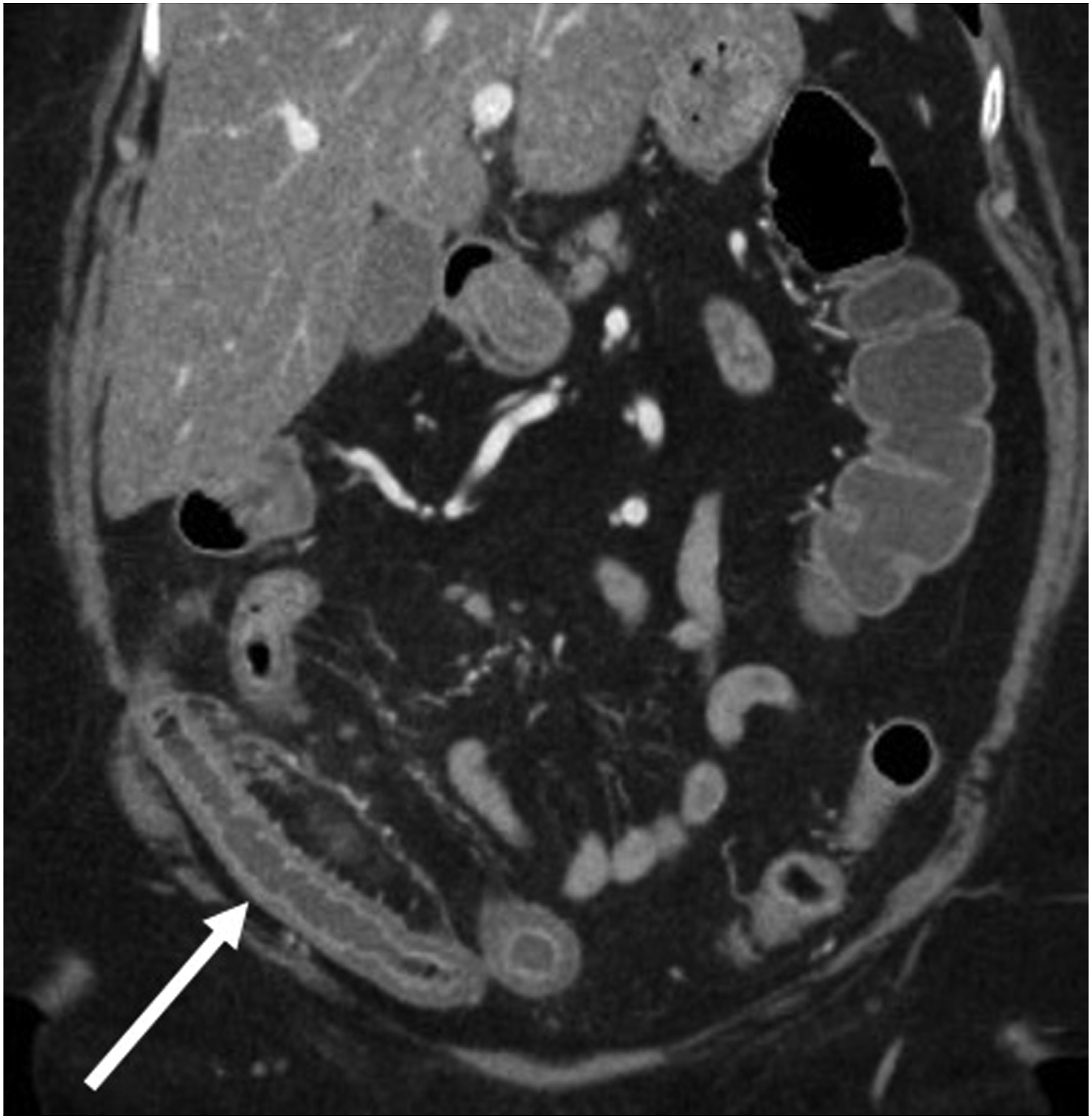
Enteritis, ileus and benign pneumatosis are well-recognized pathologies associated with chemotherapy.54-58 Typically, patients with chemotherapy-related pneumatosis, if clinically stable, are managed conservatively as this is a self-limiting condition (Figure 10). Neutropenic enterocolitis, which can be due to bacterial infection or related to chemotherapy, is characterized by bowel wall thickening with associated inflammatory changes, most commonly involving the cecum, ascending colon, and ileum (Figure 11).
59
Uncommon complications include intestinal perforation and gastrointestinal bleeding.60,61 52-year-old male with stage IV classical Hodgkin’s lymphoma who received the first cycle of a chemotherapy regimen that included doxorubicin, dacarbazine and brentuximab vedotin. Patient presented 2 days later with abdominal distention and elevated lactate. Coronal contrast-enhanced abdominal pelvic CT showed multiple loops of dilated small bowel with pneumatosis (arrow). The patient was managed conservatively, and CT findings resolved 8 days later. Case courtesy of Dr [Prasaanthan Gopee-Ramanan]. 76-year-old female with colorectal cancer presenting with nausea, vomiting and diarrhea. Coronal contrast-enhanced abdominal and pelvic CT revealed long segment thickening with surrounding inflammatory change involving the ileum that was attributed to capecitabine-induced enteritis.
Urinary Bladder
Hemorrhagic cystitis is a complication that can be seen following busulfan, doxorubicin, dacarbazine, fludarabine, and cabazitaxel treatment, but is most associated with cyclophosphamide and ifosfamide. 62 Imaging of hemorrhagic cystitis can show diffuse bladder wall thickening. To differentiate chemotherapy-related hemorrhagic cystitis from infection or graft-versus-host disease, it is important to know the treatment timeline, as chemotherapy-related hemorrhagic cystitis occurs early in the course of treatment.
Peritoneum
Ascites can be associated with chemotherapeutic agents, for example, as a part of capillary leak syndrome or treatment-related fluid overload. Imatinib, which is often used in the treatment of gastrointestinal stromal tumors and renal cell carcinomas, is one such example. 16
MSK
Muscles
The most common musculoskeletal chemotherapy toxicity is cachexia, defined as a reduction in lean body mass and muscle strength.63,64 These changes to body composition during chemotherapy, specifically an increased intramuscular fat to muscle tissue ratio, can be monitored using CT. 65 CT-derived parameters relating to body composition and myosteatosis are correlated to treatment success and may be more optimal biomarkers than body mass index.66,67 While the literature primarily reports on CT-derived parameters based primarily on mean radiodensity, similar measurements can be made based on proton density fat fraction MRI. 68 Monitoring muscular atrophy can provide important information to referring clinicians as cachexia is associated with a poor prognosis. 64
Bones
Osteoporosis causing insufficiency fractures can occur following long-term chemotherapy regimens, and in many cases these fractures are asymptomatic. 69 Additionally, osteonecrosis is a well-recognized complication of long-term corticosteroid use, a key component of many chemotherapy regimens. 70
Peripheral Nervous System
Platinum-based drugs, alkaloids, and proteasome inhibitors have been associated with peripheral neurotoxicity. 71 Recent evidence suggests a role for diffusion tensor imaging and imaging biomarkers for the detection of chemotherapy-induced peripheral neuropathy; however, nerve conduction studies remain the gold standard.72,73
Skin and Other Soft Tissues
Chemotherapy agents can result in sequelae of the skin and subcutaneous soft tissues. For example, imatinib and mitogen-activated protein kinase inhibitors have been associated with soft tissue edema. 45 Sunitinib is linked to the development of gynecomastia in men. 45 Finally, BRAF inhibitors, which are used in the treatment of metastatic melanoma, can result in cutaneous squamous cell carcinoma. 45
Systemic Manifestations of Chemotoxicity.
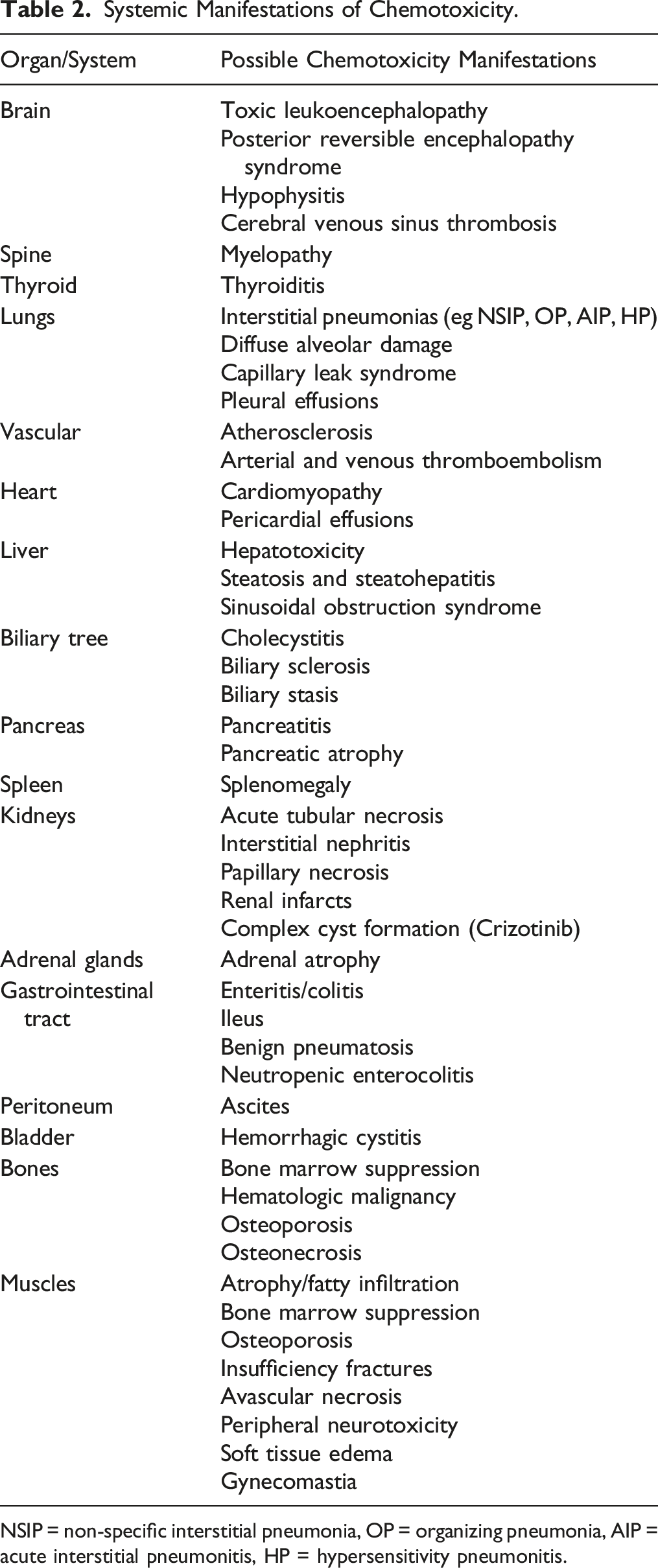
NSIP = non-specific interstitial pneumonia, OP = organizing pneumonia, AIP = acute interstitial pneumonitis, HP = hypersensitivity pneumonitis.
Conclusion
Chemotherapy-related toxicities have manifestations across many organ systems. As we return to a new normal following the COVID-19 pandemic, many patients will be diagnosed with, and begin treatment for, a variety of malignancies and some will develop chemotherapy-related toxicities. It is important for radiologists to be familiar with their imaging manifestations to best care for these patients.
Footnotes
Acknowledgments
Thank you to Dr. Prasaanthan Gopee-Ramanan for contributing cases to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.