
Abstract
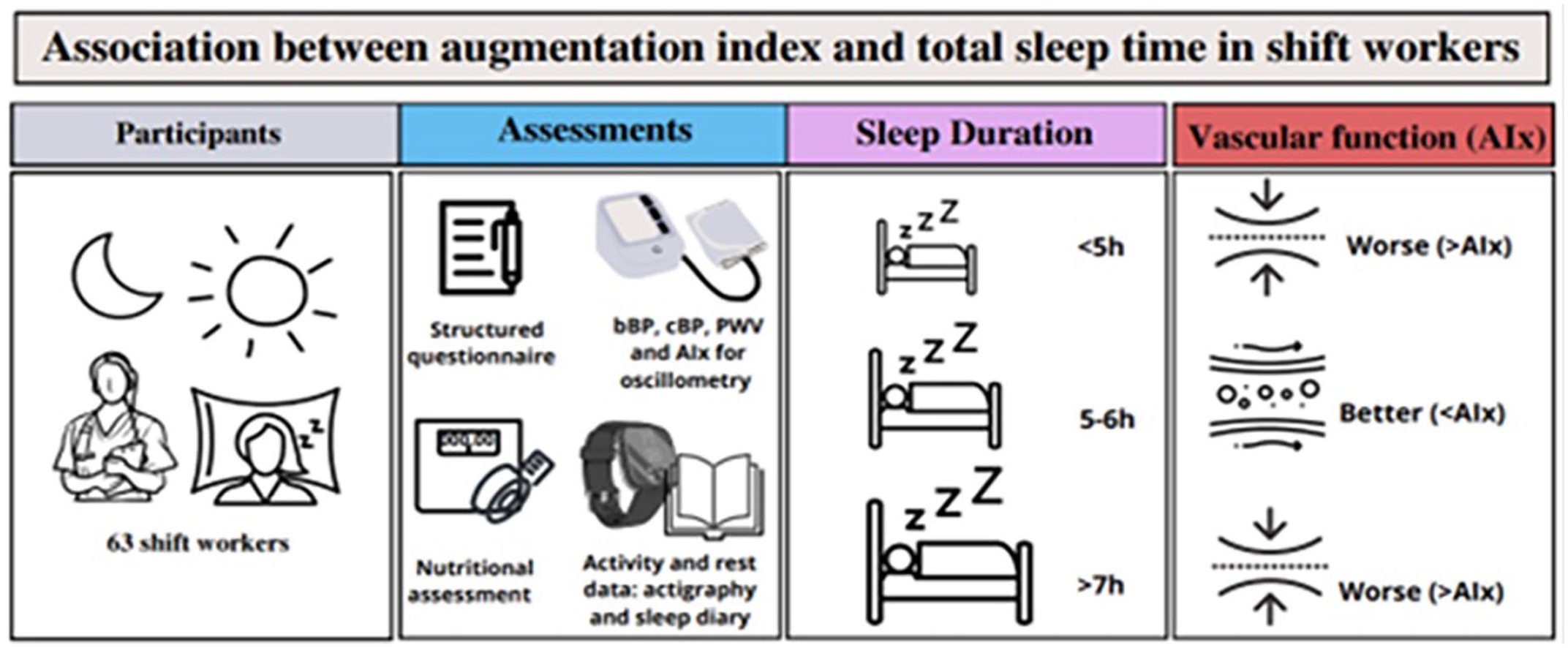
Augmentation index and pulse wave velocity are markers of vascular compromise and independent predictors of cardiovascular risk and mortality. While the link between shift work and heightened cardiovascular risk is established, the intricate genesis of early cardiovascular outcomes in shift workers remains incompletely understood. However, there is evidence that sleep duration plays a role in this regard. Here we evaluate the association of total sleep time with pulse wave velocity, augmentation index, and central blood pressure in night shift workers. This study cross-sectionally evaluated the association of total sleep time evaluated by 10-day monitoring actigraphy with augmentation index, pulse wave velocity, and brachial and central blood pressure evaluated by oscillometry in nursing professionals, 63 shift workers (89% women; age = 45.0 ± 10.5 years), and 17 (100% women; age = 41.8 ± 15.6) day workers. There were no differences in the studied variables between shift workers and day workers. Results of correlation analysis demonstrated that pulse wave velocity, central systolic blood pressure, central diastolic blood pressure, brachial systolic blood pressure, and brachial diastolic blood pressure tended to have significant correlation with each other, while these measures did not have a significant relationship with augmentation index in both groups. However, results of adjusted restricted cubic spline analysis showed a U-shaped-curve association between total sleep time and augmentation index (p < 0.001 for trend) with a nadir at 300-360 min of total sleep time in shift workers. The present study showed that total sleep time, assessed by actigraphy, had a U-shaped association with augmentation index in shift workers, which indicated better characteristics of vascular functionality when sleep time was 5-6 h in the workers studied.
Arterial stiffness assessed by pulse wave velocity (PWV) and central wave reflection assessed by the augmentation index (AIx) are markers of vascular impairment and independent predictors of cardiovascular events (Vlachopoulos et al., 2010). In recent years, the development of novel devices has allowed the easy and non-invasive assessment of PWV and AIx (Omboni et al., 2016).
Previous studies have indicated that shift work is associated with a high risk of cardiovascular diseases (Wang et al., 2018). Even though the precise mechanisms underlying this association are not yet established (Wang et al., 2018; Gusmão et al., 2022), available evidence has suggested that the high cardiovascular risk related to shift work is influenced by sleep duration and quality (Yang et al., 2022). In particular, a U-shaped association between sleep duration and cardiovascular risk among shift workers (SW) (Yang et al., 2022) and in the general population (Cappuccio et al., 2011) has been reported. Nonetheless, the relationship between sleep duration and markers of arterial stiffness and central wave reflection in SW is still not fully known. The study was based on the hypothesis that shift work, and the consequent reduction in sleep duration, alters central blood pressure (BP), PWV, and the AIx of workers. The present study aimed to evaluate the association of total sleep duration (TST) with PWV, Aix, and central BP in night shift workers.
Methods
This cross-sectional study evaluated clinical characteristics, PWV, AIx, and sleep duration of convenience samples of 63 nurses who were SW and 17 nurses who were day workers (DW) from a psychiatric hospital located in Maceió, Brazil, enrolled from September to November 2021. Exclusion criteria were age under 18 years, chronic kidney disease, pregnancy, and breastfeeding. The protocol was approved by the Research Ethics Committee of the University of São Paulo.
All participants answered a structured questionnaire on sociodemographic data, health conditions (personal history and medication use), lifestyle (physical activity, alcohol consumption, smoking), and work schedule. Accumulated night shift work (ANSW) was calculated as the number of hours of night work per week multiplied by the total number of weeks worked during working life. Objective evaluation of weight and height was also performed in order to calculate body mass index (BMI). Obesity was defined as BMI ≥ 30 kg/m2 (World Health Organization, 2000).
Brachial BP, central BP, PWV, and AIx measurements were performed using the arm oscillometry technique using the Mobil-O-Graph PWA monitor™ device (IEM Healthcare, Stolberg, Germany) as previously reported (Benas et al., 2019; Paiva et al., 2020). The oscillometric device identified the peripheral pulse wave and projected the central pulse wave using a specific algorithm (ARCSolver) (Weber et al., 2011). Participants underwent 3 readings of peripheral BP, central BP, PWV, and AIx, with a 3-min interval between them. Measurements were acquired in the sitting position after 5 min of rest. Only those with 3 valid readings of all searched parameters were included in the study. The average of the 3 readings was used in the analysis. The preparation protocol established by the Brazilian Guidelines on Arterial Hypertension (BGAH)–2020 was used, and only after that the measurements were taken. The participant was instructed not to practice physical activity in the 60 min before, not to consume food, coffee, and alcoholic beverages, and not to smoke in the 30 min before the test. Upon arriving at the location for the measurements, they were asked to empty their bladder, rest comfortably seated for 5 min in a quiet place, and then an initial measurement was performed to enable the discarding of a possible alarm reaction. Finally, the other 3 measurements used to obtain the average of pressure values and stiffness parameters were performed. The normality classification of the obtained values was performed according to the reference values established by the BGAH–2020 (Barroso et al., 2021).
Individuals using antidiabetic medications, antihypertensive drug, and lipid lowering were labeled as having diabetes, hypertension, and dyslipidemia, respectively. Alcohol consumption was categorized in yes (at least twice a week) or no (less than twice a week). Smoking was categorized in yes to currently smokers and no to former smokers and no smokers. Individuals who performed regular physical activity at least 3 times a week were considered physically active.
Actigraphy was assessed using an actigraph device (ActTrust@, Condor Instruments, Brazil) over 10 consecutive days to cover the participant’s entire weekly work schedule, including weekends. Actigraphy records were extracted, exported, and analyzed using ActStudio software.
Participants simultaneously filled out an activity and rest diary on days when actigraphy was performed. Actigraphy records and the diary were compared to identify discrepancies and enhance the accuracy of parameters recorded by the actigraph. The onset and offset of sleep were recorded in the diary for comparison with the actigraph. For this reason, the event marker of the device was not used. The epoch was defined as 1 min, meaning that data were recorded every minute. Total sleep time (TST), expressed in hours, was defined as the daily average of sleep minutes measured by actigraphy.
Continuous data with normal or non-normal distribution are presented as mean ± standard deviation or median [25th percentile, 75th percentile], while categorical variables are presented as proportions. All analyses were performed splitting the sample into SW and DW. Student t test and chi-square test compared the variables between the studied groups. Pearson’s analysis was used to evaluate the correlation among all vascular and BP measures. Restricted cubic spline analysis with 3 knots adjusted for potential confounding factors (age, sex, body mass index, use of antihypertensive medications, diabetes, dyslipidemia, smoking status, alcohol use, physical activity, and hour of day when the vascular/BP measurements were performed) evaluated the association of TST with brachial BP, central BP, PWV, and AIx in SW and DW. ANSW was further included as a confounding variable when evaluating shift workers. Restricted cubic spline analysis with 3 knots (adjusted for age, sex, body mass index, use of antihypertensive medications, diabetes, dyslipidemia, smoking status, alcohol use, physical activity, TST, and hour of day when the vascular/BP measurements were performed) evaluated the relationship between ANSW and vascular/BP measures among SW. Statistical analyses were performed using Stata v.14.2 (Stata Corp LP, College Station, TX, USA) and p values <0.05 were considered significant.
Results
There were no differences in the studied variables between SW and DW workers (Table 1). Notably, most participants were female, non-smokers, middle-aged, and more than half were sedentary and consumed alcoholic beverages (Table 1). AI was not correlated with any measure (PWV, central systolic BP, central diastolic BP, brachial systolic BP, and brachial diastolic BP) in both groups (Table 2). In addition, no significant association of AI with any other vascular/BP measure was detected by restricted cubic analysis. However, other measures (with the exception of brachial diastolic blood pressure [DBP] and central DBP that are not correlated to PWV) are significantly correlated at a p < 0.05 (Table 2).
Characteristics of the participants.
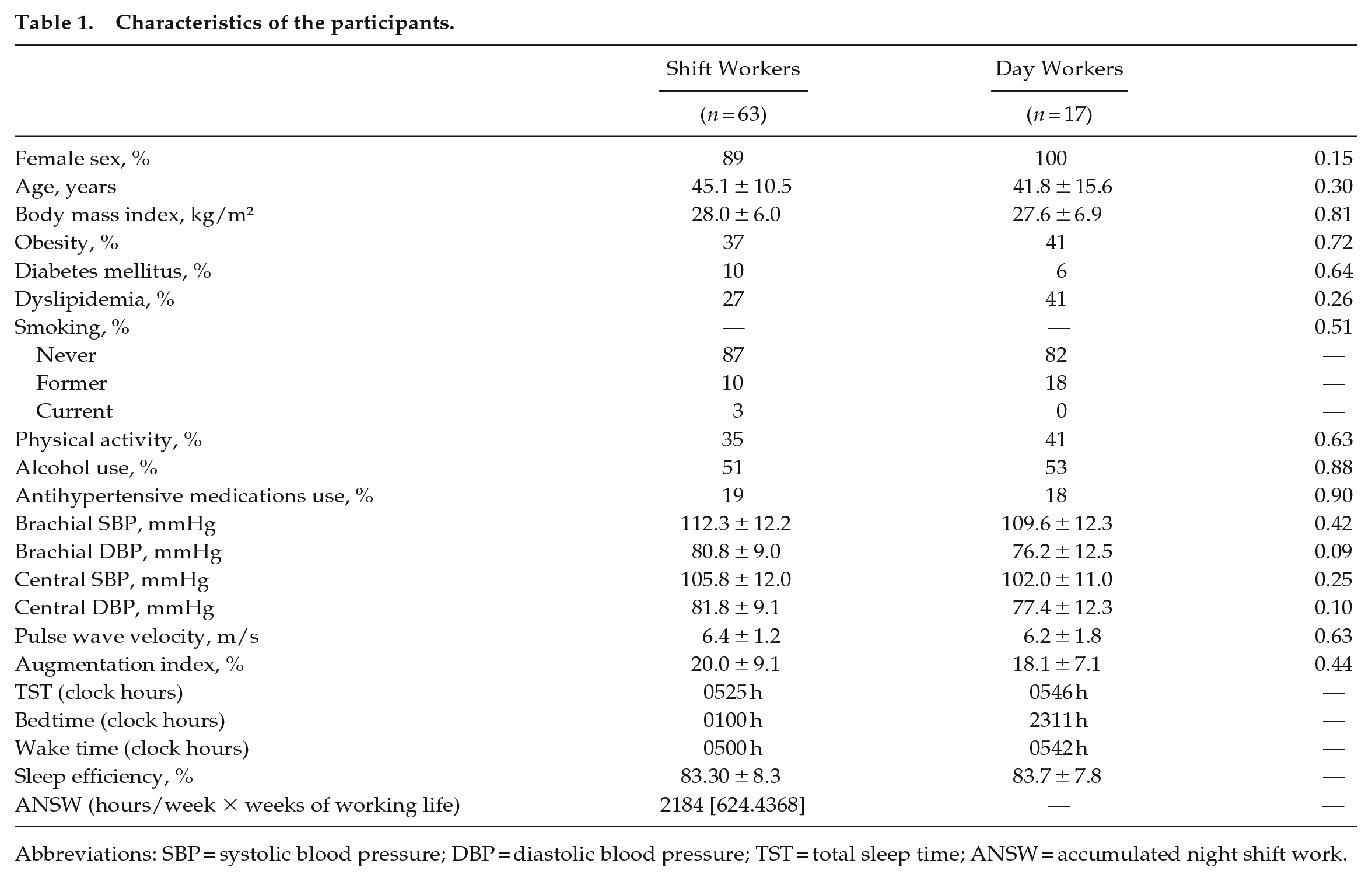
Abbreviations: SBP = systolic blood pressure; DBP = diastolic blood pressure; TST = total sleep time; ANSW = accumulated night shift work.
Correlation coefficients for the studied vascular and blood pressure parameters.
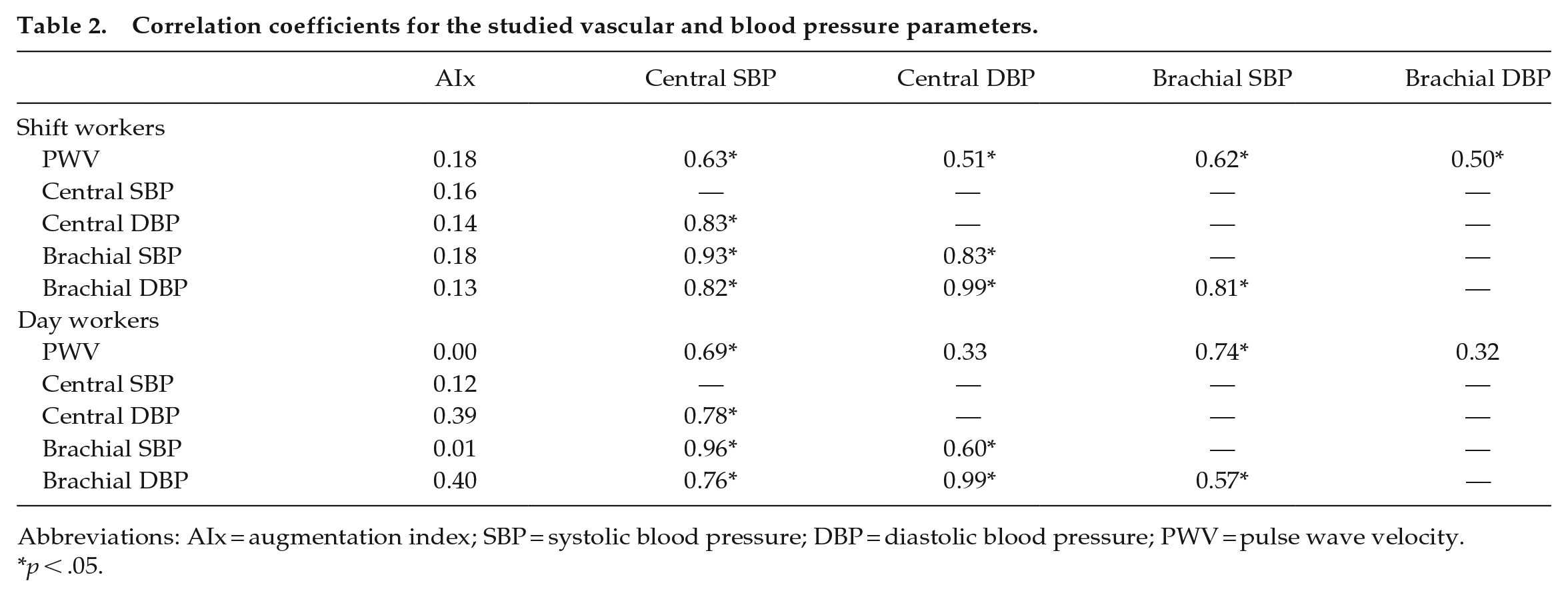
Abbreviations: AIx = augmentation index; SBP = systolic blood pressure; DBP = diastolic blood pressure; PWV = pulse wave velocity.
p < .05.
Results of adjusted restricted cubic spline analysis showed a U-shaped association between AIx and TST (Figure 1a; p < 0.001 for trend) in SW. Notably, the nadir was at 300-360 min (5-6 h) of TST. Conversely, no significant association between TST and brachial BP, central BP, and PWV was detected in SW (Figure 1b-1e), while no significant association between TST and any vascular or BP measure was observed in DW (Suppl. Fig. 1). In addition, no significant relationship was observed between ANSW and brachial BP, central BP, PWV, and AIx in SW (Figure 2).
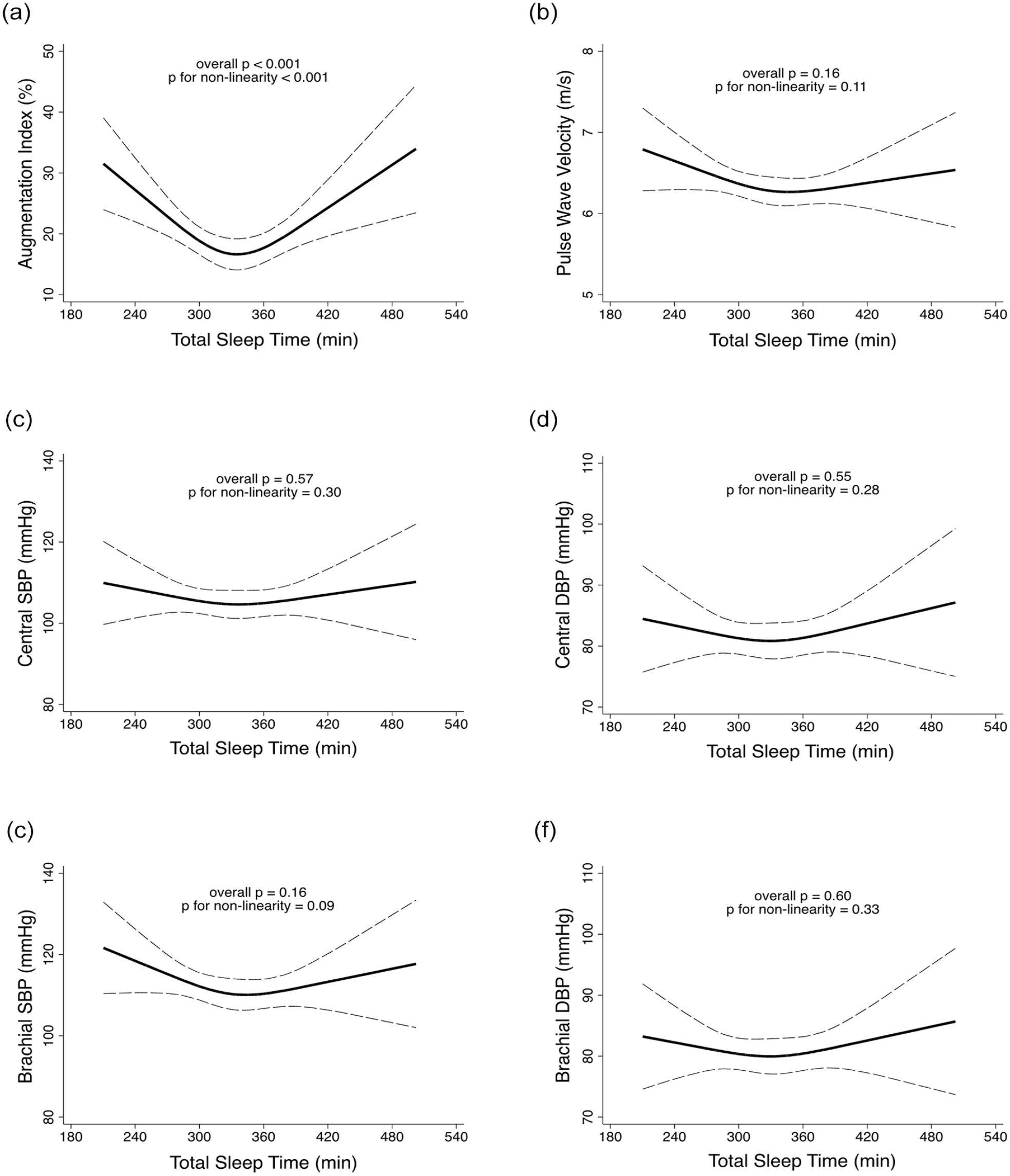
Restricted cubic analysis for the relationship between total sleep time and (a) augmentation index, (b) pulse wave velocity, (c) central SBP, (d) central DBP, (e) brachial SBP, and (f) brachial DBP in shift workers. All analyses were adjusted for age, sex, body mass index, use of antihypertensive medications, diabetes, dyslipidemia, smoking status, alcohol use, physical activity, accumulated night shift work, and hour of day when the vascular/blood pressure measurements were performed. Abbreviations: SBP = systolic blood pressure; DBP = diastolic blood pressure.
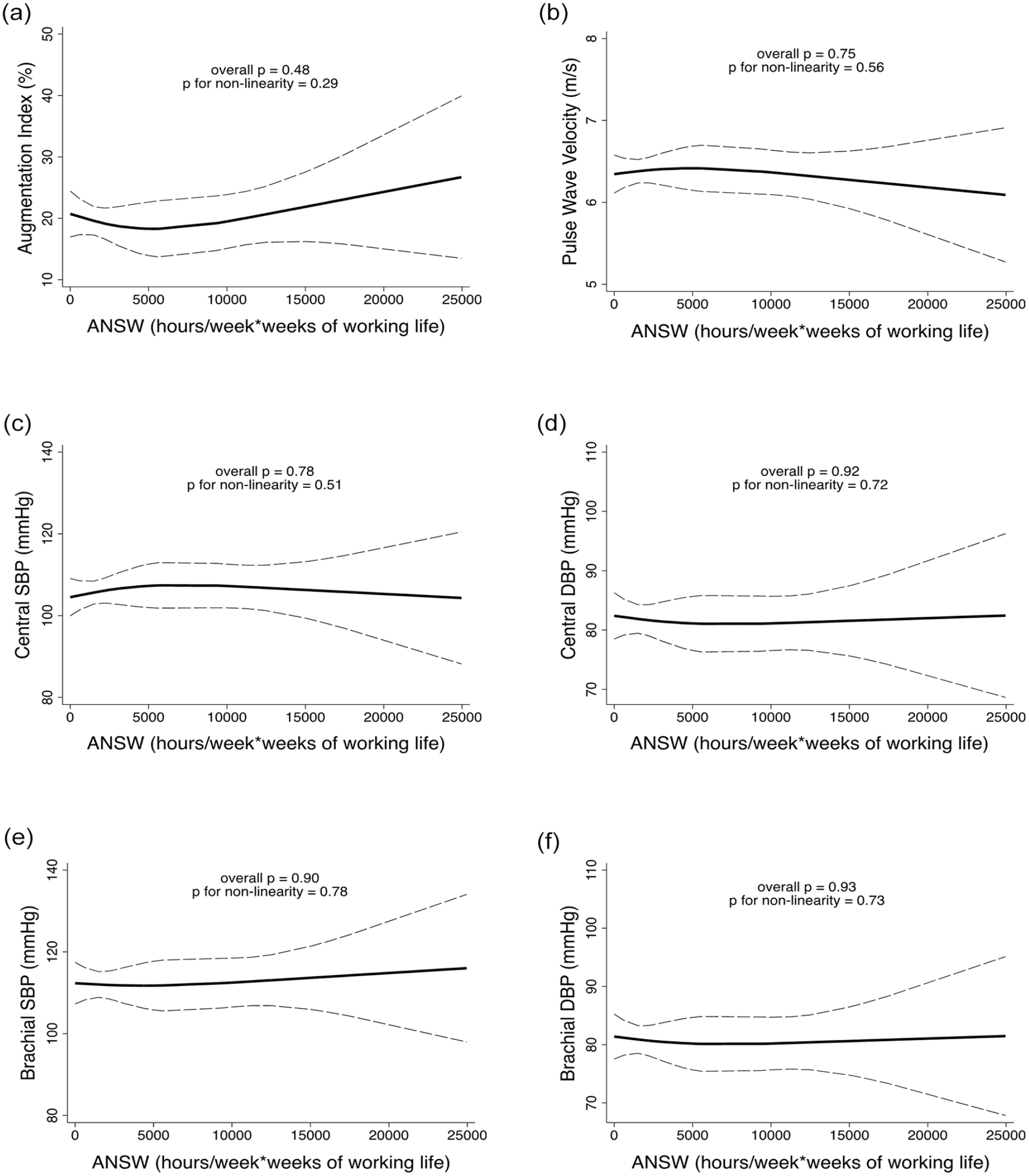
Restricted cubic analysis for the relationship between ANSW and (a) augmentation index, (b) pulse wave velocity, (c) central SBP, (d) central DBP, (e) brachial SBP, and (f) brachial DBP in shift workers. All analyses were adjusted for age, sex, body mass index, use of antihypertensive medications, diabetes, dyslipidemia, smoking status, alcohol use, physical activity, total sleep time, and hour of day when the vascular/blood pressure measurements were performed. Abbreviations: ANSW = accumulated night shift work; SBP = systolic blood pressure; DBP = diastolic blood pressure.
Discussion
The major finding of the present report was that TST had a U-shaped association with AIx in SW. Our findings align with the notion that sleep duration exhibits a U-shaped association with adverse cardiovascular outcomes and risk, given the correlation between higher AIx and increased cardiovascular event risk (Cappuccio et al., 2011; Yang et al., 2022). Furthermore, they may provide novel explanations for the greater risk related to sleep duration among SW. AIx is considered an indirect measure of arterial stiffness (Vlachopoulos et al., 2010) but is also influenced by greater systemic vascular resistance (Wilenius et al., 2016). Even though short and long sleep durations have been related to adverse cardiometabolic characteristics among SW (Cappuccio et al., 2011), our results showed that the relationship between AIx and TST was independent of traditional cardiovascular risk factors, considering that these were used as adjustment variables in the analyses, suggesting that alternative mechanisms might be contributing to vascular damage related to sleep duration in SW. In this regard, the increase in sympathetic activity that occurs in sleep restriction and hypersomnia may alter vessel functionality as previously demonstrated by changes in peripheral vascular resistance (Gupta, 2017). Therefore, AIx may be a potential candidate to explain the current findings. However, further studies are necessary to confirm this assumption.
Although AIx had an independent association with TST, no other vascular or BP measurement showed significant association with TST in SW. The reasons for these discrepancies are not clear in our analysis. However, it was noteworthy that PWV, central BP, and brachial BP measurements had significant correlation with each other, while these measures did not have a significant relationship with AI. These data support the notion that AI is a measure with distinct features compared to the other vascular and BP measures, which could justify its sole independent association with TST.
Several epidemiological studies and meta-analysis have demonstrated that sleep duration of 6-8 h is associated with lower cardiovascular risk and mortality (Cappuccio et al., 2011; Yang et al., 2022). By contrast, we found that 5-6 h of sleep was related to better vascular characteristics, which seems to disagree with the aforementioned studies. However, it is noteworthy that sleep duration in large sample studies is typically estimated from subjective reports, which is biased by systematic over-reporting (Cespedes et al., 2016). Indeed, sleep duration estimated by subjective reports is in average more than 1 h greater than sleep duration calculated by actigraphy (Cespedes et al., 2016).
On the other hand, even studies with objective measures of sleep have shown during the last decades an association between short sleep duration and cardiometabolic diseases. The Coronary Artery Risk Development in Young Adults (CARDIA) cohort study, for instance, showed that participants sleeping 5 h or less (measured by actigraphy) had an increased risk of developing coronary calcifications (King et al., 2008). In addition, 20 years ago, it was demonstrated that chronic restriction of sleep to 6 h or less strongly impairs waking neurobehavioral functions (van Dongen et al., 2003).
A cohort of Brazilian adults that aimed to assess the association of obstructive sleep apnea (OSA), short sleep duration (SSD), daytime sleepiness, and cardiometabolic risk factors observed, through actigraphy, that short sleep duration around 5-6 h was associated with OSA. However, SSD was not independently associated with obesity, hypertension, and dyslipidemia, that is, cardiovascular risks (Drager et al., 2019). Thus, our findings are surprising since the negative and diverse effects of short sleep duration have been well documented.
Nevertheless, some results of the present study deserve further comments. First, we found no association between the burden of shift working and measures of arterial stiffness and central hemodynamics, which is in agreement with data obtained from other populations (Gusmão et al., 2022). Second, to our knowledge, our report is the first to provide an association between AIx and sleep duration, since a previous study evaluating 1687 post-menopausal women failed to find a significant association in the whole sample (Lee et al., 2021). Although differences in the protocols and characteristics of the samples might have played a role in such discrepancies, our findings suggest that evaluation of central hemodynamics might be an interesting target for further studies evaluating the relationship between sleep duration and cardiovascular risk. Third, it should be noted that AIx, despite being influenced by pathophysiological conditions, medication use, heart rate, age, and gender (Townsend et al., 2015; van Sloten et al., 2015; Prodel et al., 2018), is still indicated as capable of predicting the functional capacity of vascular elasticity, as long as the previous aspects are controlled in the analyses (Salvi et al., 2022).
This study has some limitations. First, mainly female and only nursing workers were included, which does not allow extrapolation of the results to the general population. Second, causality cannot be established due to the cross-sectional design of the study. Third, the sample size, particularly of DW, was relatively small. Conversely, the evaluation of TST in our analysis was performed using actigraphy, which provides a more accurate measure of sleep duration than subjective reports (Cespedes et al., 2016).
In conclusion, the present study demonstrated that TST assessed by actigraphy had a U-shaped association with AIx in SW with a nadir at 5-6 h of sleep, indicating that sleep duration lower and higher than this range might be related to vascular impairment and possibly greater cardiovascular risk in this population.
Supplemental Material
sj-docx-1-jbr-10.1177_07487304241229180 – Supplemental material for Association Between Augmentation Index and Total Sleep Time in Night Shift Workers
Supplemental material, sj-docx-1-jbr-10.1177_07487304241229180 for Association Between Augmentation Index and Total Sleep Time in Night Shift Workers by Waléria D. P. Gusmão, Victor M. Silva, Annelise M. G. Paiva, Marco Antonio Mota-Gomes, Wilson Nadruz and Claudia R. C. Moreno in Journal of Biological Rhythms
Footnotes
Acknowledgements
This article is part of the Doctoral thesis of the first author; therefore, the University of São Paulo (USP) financed the acquisition of inputs and organization of office material for collection in the research field. The Research Support Foundation of the State of Alagoas (FAPEAL) provided funding for the researcher’s internship on the Campus of the Public Faculty of the University of São Paulo (USP).
Author Contributions
Waléria D. P. Gusmão: Conceptualization, Study design, Methodology, Data collection, Data curation, Writing – original draft and review. Victor M. Silva: Data collection, Data curation. Annelise M. G. Paiva: Methodology, Writing – review, Marco Antonio Mota-Gomes: Methodology, Writing – review. Wilson Nadruz: Formal analysis, Writing – review & editing. Claudia R. C. Moreno: Conceptualization, Study design, Methodology, Data curation, Writing – review & editing, Supervision. All authors have read and agreed to the published version of the manuscript.
Conflict Of Interest Statement
The authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Note
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.