
Abstract
This cross-sectional study analyzed the association between physical activity (PA) and social jetlag (SJL) among shift workers. We evaluated 423 employees, aged between 18 and 60 years, who worked in a poultry-processing company in Brazil. Physical activity levels (PAL) were determined by the short form of the International Physical Activity Questionnaire (IPAQ-SF). SJL was calculated as the absolute difference between the time of mid-sleep on work and free days. The percentage of workers insufficiently active was high on all shifts, with no significant differences between the 3 shifts. The amount of time spent in sedentary behavior on workdays did not differ between shifts. Among night-shift workers, negative associations were observed between SJL and 1) the duration and weekly energy expenditure while walking; 2) the frequency of moderate and vigorous PA; and 3) the total energy expenditure related to PA. Even though PAL did not differ among workers on different shifts, we found a high prevalence of subjects who were insufficiently active or too sedentary among all groups. Also, SJL was negatively associated with PA in night-shift workers. These results suggest that PA should be encouraged among shift workers and that SJL may be an important factor in reducing PA in this cohort.
Shift work is extremely prevalent in modern societies around the world (Geliebter et al., 2000). Estimates indicate that approximately 20% of the economically active population worldwide engage in shift work (Barbadoro et al., 2013). In Brazil, approximately 10% of the population is engaged in this type of work (Moreno et al., 2003).
Current evidence clearly establishes that shift work is associated with a higher prevalence of disease, including obesity (Di Lorenzo et al., 2003), and comorbid conditions, e.g., type 2 diabetes mellitus, metabolic syndrome (Esquirol et al., 2009), and dyslipidemia (Monk and Buysse, 2013). Among the main causal factors of these diseases is poor diet (Mota et al., 2013; Balieiro et al., 2014), restricted sleep time, and poor sleep quality (Mota et al., 2014). In addition, other obesity-related lifestyle habits are common in these individuals, such as physical inactivity (Atkinson et al., 2008), and some studies show that shift workers are very likely to live a sedentary lifestyle (Garcez et al., 2015; Neil-Sztramko et al., 2016). Furthermore, an increase in their physical activity level (PAL) brings health benefits to the workers, including decreased body-mass index (BMI), blood pressure, and total cholesterol; reduced tobacco consumption; increased physical fitness, and sleep length; and reductions in work-dependent fatigue and musculoskeletal symptoms (Härmä et al., 1988; Shephard, 1996). These issues could be particularly relevant to shift workers.
Shift workers experience a form of circadian misalignment, especially on work days (Vetter et al., 2015). It is known that the degree of misalignment depends on the individual’s chronotype, their “morningness” or “eveningness” (Zavada et al., 2005; Roenneberg et al., 2012). Thus, evening-types have increased misalignment than do morning-types (Wittmann et al., 2006). This phenomenon has been termed “social jetlag” (SJL), a measure of the discrepancy between sleep times on work days and days off (Wittmann et al., 2006; Sallinen et al., 2005). This term is used to draw attention to its similarity to jetlag, induced by trans-meridian travel, which causes circadian desynchronization in an individual. However, unlike jetlag, SJL occurs chronically during an individual’s time spent at work. As with jetlag, SJL likely causes chronic effects on metabolism because of a misaligned circadian system (Parsons et al., 2014). In this context, some studies have suggested a relationship between SJL and obesity (Roenneberg et al., 2012), but any relationship between SJL and the causal factors of obesity, such as physical inactivity, is underexplored in the literature.
Accordingly, we hypothesized that SJL is negatively associated with the level and frequency of PA by shift workers. The objective of this study was to analyze any association between PA and SJL among workers on different shift-work schedules.
Methods
This cross-sectional study included 423 employees, aged between 18 and 60 years, working in a poultry-processing company in Brazil.
The shift-work schedule used by the company where the study was conducted had several start and end times for different shifts. However, regardless of the start time, all shifts lasted 10 h (8 h work, 1 h for a meal break and 3 intervals of 20 min; these intervals were required due to the nature of the work). The meal break occurred between the 4th and 5th hour after start time. The three 20-min interval breaks occurred during the 2nd, 7th and 9th hour after start time. All volunteers in the study worked from Monday to Friday, and always on the same shift. In this study, we have classified volunteers within the following categories:
Fixed early-morning worker: The individual should start work between 0301 h and 0659 h, as proposed by Sallinen et al. (2005). Example: the individual could start work at 0330 h and leave at 1330 h.
Fixed-day worker: The individual should work between 0700 h and 2000 h, as proposed by Huang et al. (2013). Example: the individual could start work at 0730 h and leave at 1730 h.
Fixed-night worker: The individual should work at least 3 hours after 2300 h, as proposed by Sallinen et al. (2005). Example: the individual could start work at 1700 h and leave at 0300 h.
Using these criteria, we enrolled 122 subjects who worked the early-morning shift, 133 who worked the day shift, and 168 who worked the night shift.
This study was approved by the Ethics Committee of the Federal University of Uberlândia (Protocol No. 981,343/2015). All workers provided written informed consent to participate in the study.
Socio-Demographic Evaluation
The volunteers included in the study answered a questionnaire that assessed demographic aspects such as age, sex, years of education, and work schedule.
Anthropometric Variables
Weight was measured with a scale to an accuracy of 0.1 kg (Welmy, São Paulo, Brazil). Height was measured to an accuracy of 0.1 cm using a stadiometer fixed to the wall (Welmy). Body mass index (BMI, kg/m²) was calculated as the weight (kg) divided by the height squared (m2). Waist circumference (WC) was measured with an inelastic measuring tape as the midpoint between the iliac crest and lower costal margin. These measurements were taken during the rest periods for each shift. A BMI >25 kg/m2 and waist circumference (WC) ≥94 cm for men and ≥80 cm for women were considered abnormal (WHO, 2000).
Physical Activity (PA)
The short-form International Physical Activity Questionnaire (IPAQ-SF) was used to determine the PAL. The questionnaire was translated into Portuguese and validated for use by Brazilian participants (Matsudo et al., 2001). Questions related to the activities undertaken in the previous week. Volunteers answered 9 questions about walking frequency and duration, the frequency of taking moderate or vigorous PA, and estimates of the time spent sedentary during weekdays and the weekend.
The PAL was categorized using the recommendations established by the World Health Organization (Guilbert, 2003). Participants were considered physically active if they performed at least 150 minutes of PA per week (including time spent at work, transportation to/from work, household chores, and during leisure time). Participants who performed between 10 and 149 minutes of PA were considered moderately active, and those who performed less than 10 minutes per week were classified as insufficiently active.
The PAL from the IPAQ-SF was also converted into a metabolic equivalent (MET; min/wk) using the following formula:
Energy expenditure = Σ{duration (in min) × frequency (times/week) × MET level}, summing the values for each MET. These MET levels were calculated according to IPAQ guidelines (IPAQ, 2005): walking was 3.3 METs; moderate PAL, 4.0 METs; and vigorous PAL, 8 METs.
Sleep Patterns
Participants were asked to report their usual bedtimes and waking times on weekdays and weekends. Participants were asked: “What time did you go to sleep on weekdays (during the past two weeks)?”; “What time did you wake up on weekdays (during the past two weeks)?”; “What time did you go to sleep on weekends (during the past two weeks)?”; “What time did you wake up on weekends (during the past two weeks)?”. These evaluations were performed by a team trained and experienced in sleep studies; the team assessed sleep duration, discounting sleep latency from the estimated sleep period. (At the time of the interview, each participant was informed that it was necessary to assess the sleep time, excluding the time taken to fall asleep.).
Sleep duration was computed using the weighted average of Self-Reported Sleep Duration, which considers both weekdays and weekends, using the formula (Guilbert, 2003): [(Reported current weekday sleep duration × 5) + (Reported current weekend sleep duration × 2)]/7.
An average sleep time of less than 6 h was rated as inadequate, 6-7 h as marginal, and more than 7 h as adequate (ASA, 2007). A visual analog scale (0-10 cm) was also used for reported sleep quality on workdays and weekends.
Diurnal Preference
The Horne and Ostberg questionnaire explores preferred sleep time and aspects of daily performance (score range, 16-86) (Horne and Ostberg, 1976). It contains 19 questions, such as: “At what time would you like to get up?’’, “At what time do you feel tired?’’ and ‘‘What would be the best time to perform hard physical work?’’ Based on scores from this test, subjects were categorized as being either Evening (score, 16-41), Intermediate (42-58) or Morning (score: 59-86) Types.
Chronotype
For day workers, chronotype was derived from the time of mid-sleep time on free days at the weekend (MSF) with a further correction for calculated sleep debt (MSFsc), calculated as the difference between average sleep duration at the weekends and week days (Roenneberg et al., 2007). For early-morning and night workers, chronotype was calculated with a specific formula for shift workers (MSFEsc) proposed by Juda et al. (2013).
Social Jetlag (SJL)
SJL, a behavioral indicator of circadian misalignment, was calculated as the absolute difference between time of mid-sleep on work and free days, and it was also categorized dichotomously as >60 min (SJL present); or ≤60 min (SJL absent) (Wittmann et al., 2006).
Statistical Analyses
All statistical analyses were performed with the Statistica 7.0 software (StatSoft, Inc., Tilsa, OK). Initially, the normality of the data was tested using the Kolmogorov–Smirnov test. The values are presented as the means and standard deviation, or as median [interquartile range] for non-normally distributed data. To characterize participants according to shift, one-way ANOVA and Tukey post-hoc analyses were performed for normally distributed variables. When the variables were not normally distributed, the Kruskal–Wallis test was used. Variables with significant values in the Kruskal–Wallis test were tested by Dunn’s test with a correction of alpha via Bonferroni’s method. For determination of whether SJL was associated with PA or BMI in shift work, linear regression was performed while controlling for sex, age and mean total sleep time. To determine the risk of overweight (BMI ≥25 kg/m²) among those who had SJL and to eliminate potential confounders, a multivariate logistic regression analysis was performed, adjusting for sex and age.
Results
Table 1 shows the sociodemographic and anthropometric data, sleep patterns, chronotypes, and amount of SJL of the volunteers divided according to the shift worked. The night-shift workers were younger than those working the early-morning and day shifts (p < 0.001). There was a higher proportion of females in the early-morning shift (p < 0.001), with longer working times (p = 0.032). The night-shift workers had a significantly lower frequency of high WC and BMI compared with workers from other shifts (p = 0.006 and p = 0.02, respectively). The early-morning shift workers slept less on work days (p < 0.001) and more on rest days as compared with day- and night-shift workers (p = 0.003). The self-reported quality of sleep on work days for those working day shifts was higher than for those working early-morning and night shifts (p = 0.001). However, on rest days, the quality of sleep was considered better for those on early-morning and day shifts than those on night shifts (p = 0.003).
Sociodemographic Characteristics, Anthropometric Indices, Sleep Patterns, Diurnal Preference, Chronotype and Social Jetlag of Employees according to Shift Worked.
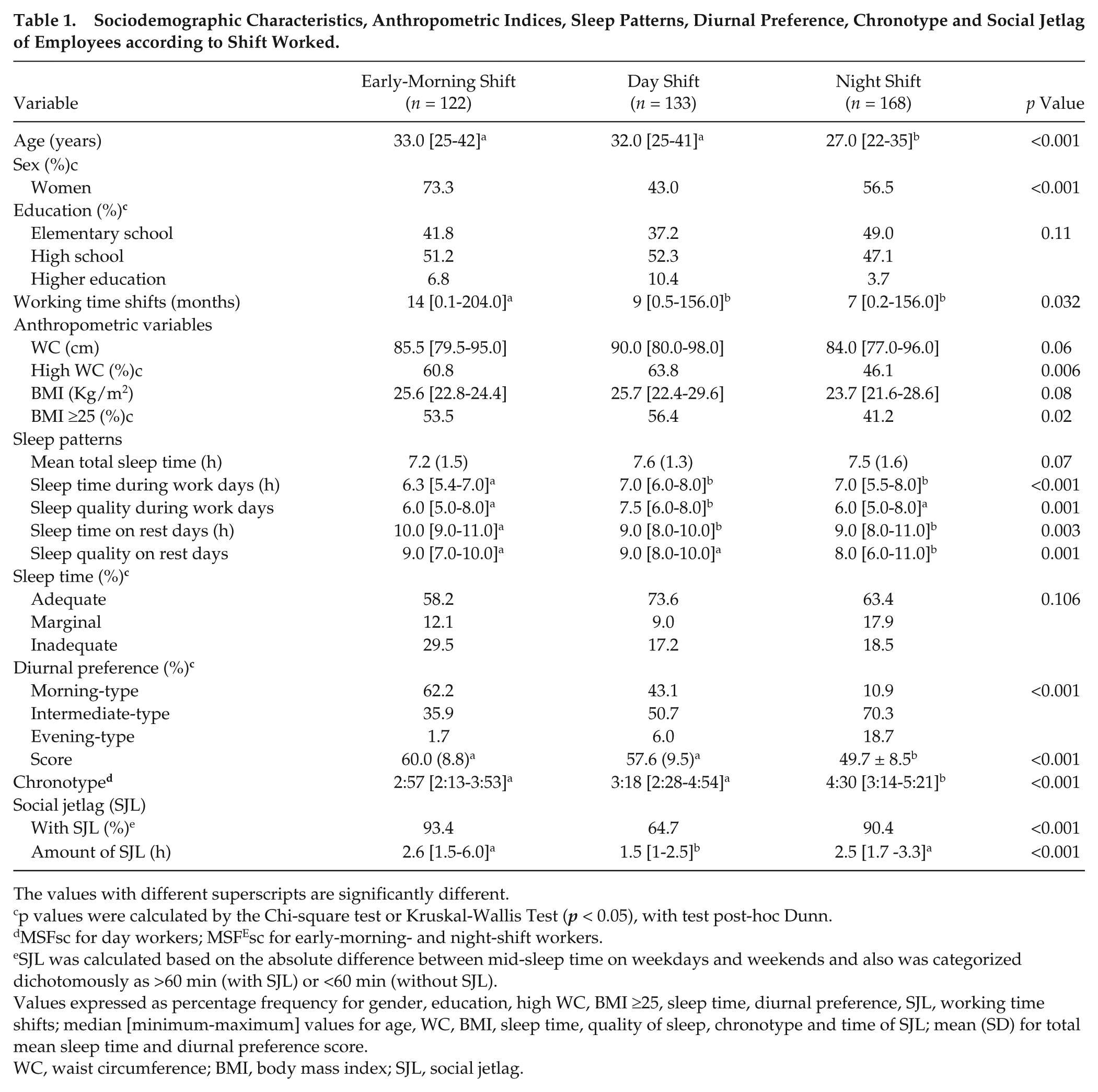
The values with different superscripts are significantly different.
p values were calculated by the Chi-square test or Kruskal-Wallis Test (p < 0.05), with test post-hoc Dunn.
MSFsc for day workers; MSFEsc for early-morning- and night-shift workers.
SJL was calculated based on the absolute difference between mid-sleep time on weekdays and weekends and also was categorized dichotomously as >60 min (with SJL) or <60 min (without SJL).
Values expressed as percentage frequency for gender, education, high WC, BMI ≥25, sleep time, diurnal preference, SJL, working time shifts; median [minimum-maximum] values for age, WC, BMI, sleep time, quality of sleep, chronotype and time of SJL; mean (SD) for total mean sleep time and diurnal preference score.
WC, waist circumference; BMI, body mass index; SJL, social jetlag.
We found that the diurnal preference distribution depended on the shift being worked: there were more morning-types in the early-morning shift workers and more intermediate-types in the night-shift workers (p < 0.001). The night-shift workers had the lowest average diurnal preference score (49.7 [8.5]) compared with day- (57.6 [9.5]) and early-morning shift workers (60.0 [8.8]) (p < 0.001). This is confirmed by the value of the chronotype (MSFEsc), which was also later over this shift (4:30 [range, 3:14-5:21]; p <0.001). It was found that both the proportion of workers with SJL and the amount of SJL depended on the shift being worked (p <0.001).
As chronotype tends to be influenced by age, we calculated the chronotype and diurnal preference based on different age groups (18-21, 22-29, 30-39, 40-50 and ≥51 years). Regarding the chronotype, we observed differences between groups when the MSFsc/MSFEsc was calculated. In general, lower age groups showed later scores when compared with the older age groups [(the group of subjects aged 18-21 years was later than that for the groups aged 30-39 years (p = 0.03), 40-50 years (p = 0.03), and >51 years (p = 0.02); the group aged 22-29 years was later than the groups for 30-39 years (p = 0.02), 40-50 years (p = 0.03); and >51 years (p = 0.01)]. Values of the MSFsc/MSFEsc were as follows: 18-21 years: 4:19 (3:12-5:46); 22-29 years: 4:03 (3:05-5:36); 30-39 years: 3:17 (2:53-4:27); 40-50 years: 3:00 (2:34-4:07); >51 years: 2:46 (2:09 - 4:17).
In relation to diurnal preference, we noted that lower age groups (18-21 and 22-29 years) showed lower scores when compared with older age groups (30-39, 40-50 and ≥ 51 years) (18-21 years: 50.7 [10.1], 22-29 years: 53.5 [9.8], 30-39: 56.8 [9.2], 40-50: 58.4 [9.8], e ≥ 51 years: 60 [7.5]; p < 0.01).
Table 2 shows the PAL, sedentary behavior and the weekly energy expenditure in the 3 shifts. The percentage of subjects with different PAL ratings did not differ among the 3 shifts (p = 0.82). The amount of time engaged in sedentary behavior on work days and on rest days, and the total weekly energy expenditure, did not differ among the shifts (p = 0.10, 0.30 and 0.80, respectively).
Physical Activity Level, Sedentary Behavior and Weekly Energy Expenditure according to Shift.
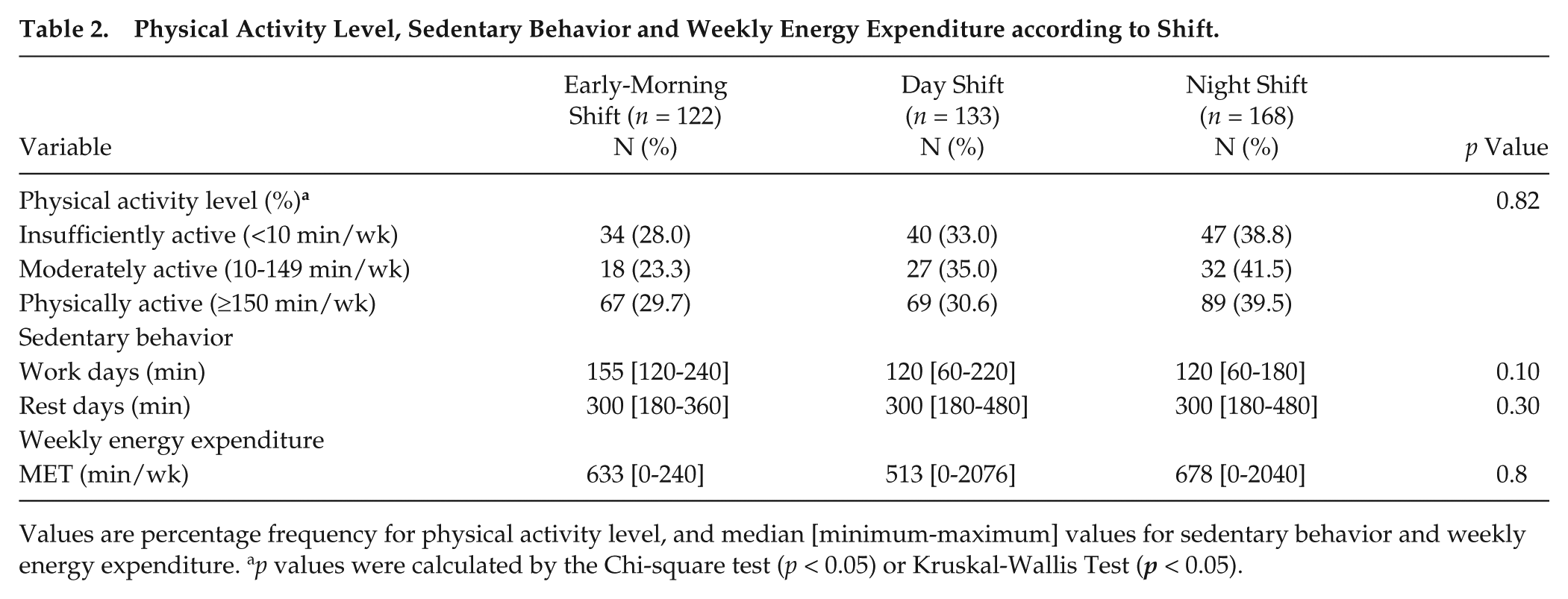
Values are percentage frequency for physical activity level, and median [minimum-maximum] values for sedentary behavior and weekly energy expenditure. ap values were calculated by the Chi-square test (p < 0.05) or Kruskal-Wallis Test (p < 0.05).
Table 3 shows the sleep patterns, diurnal preference and chronotype of the volunteers divided by the shift worked, according to the presence or absence of SJL. When evaluating workers from the night shift, there was a higher tendency to eveningness for subjects without SJL compared to with SJL (p = 0.04). In contrast, the tendency to eveningness was greater in the early-morning shift workers with SJL compared to without SJL (p < 0.001).
Sleep Patterns, Diurnal Preference and Chronotype of Employees according to Presence or Absence of Social Jetlag.
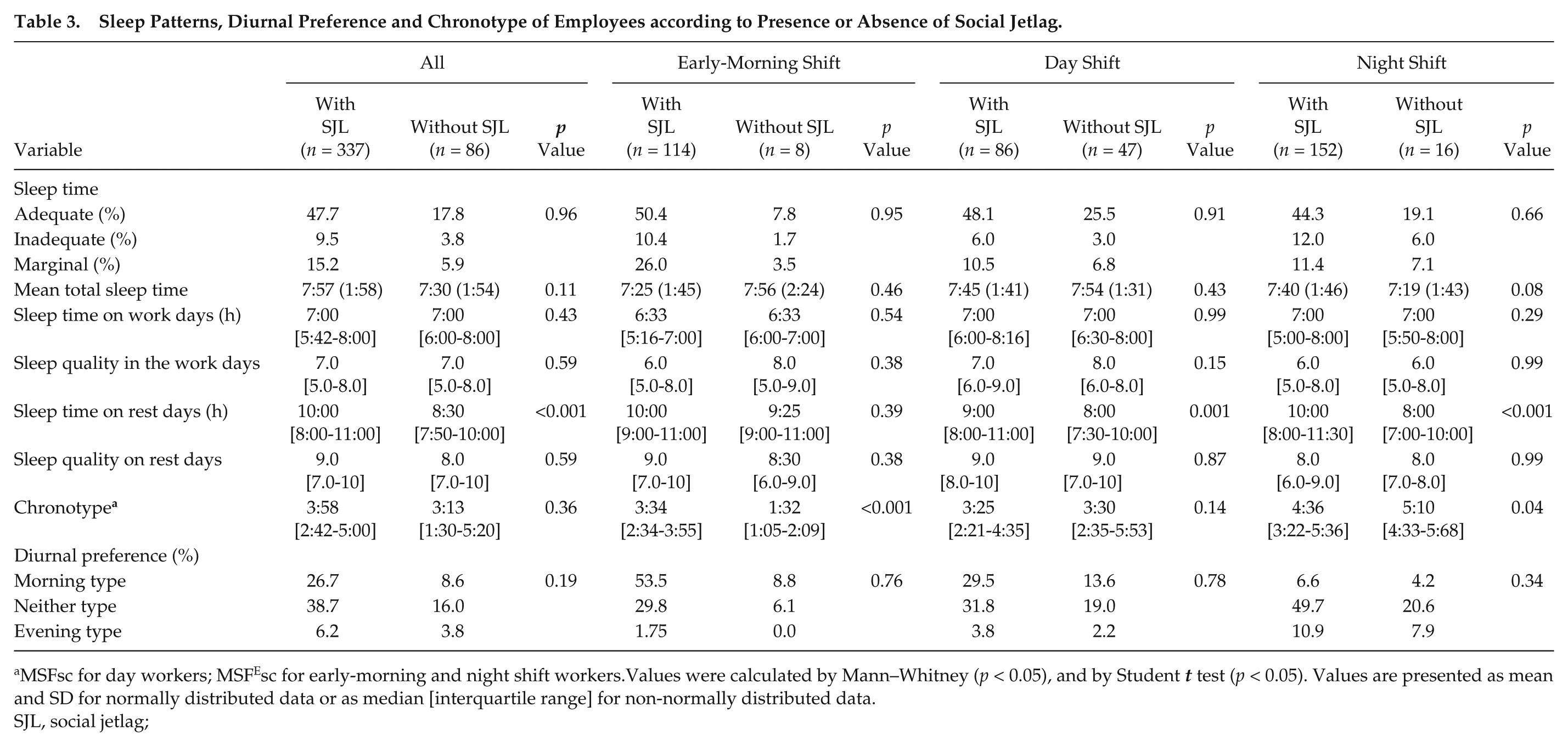
MSFsc for day workers; MSFEsc for early-morning and night shift workers.Values were calculated by Mann–Whitney (p < 0.05), and by Student t test (p < 0.05). Values are presented as mean and SD for normally distributed data or as median [interquartile range] for non-normally distributed data.
SJL, social jetlag;
Table 4 shows the beta-coefficients from linear regression analyses of SJL upon the frequency, duration, and energy expenditure of different types of PA in the different shifts, adjusted for age and BMI. Among night-shift workers, negative associations were observed between SJL and duration, along with weekly energy expenditure on walking (MET, min/week) (β = −0.15, p = 0.04; and β = −0.15, p = 0.03, respectively). There was a negative association between SJL and weekly frequency of moderate-intensity PA (β = -0.14, p = 0.04) and vigorous-intensity PA (β = −0.17, p = 0.03) among night-shift workers. Also, a negative association was found between SJL and total energy expenditure related to PA (MET, min/wk) (β = −0.19, p = 0.01) among night-shift workers.
Beta-Coefficients from Linear Regression Analyses of Social Jetlag upon Physical Activity Levels according to Shift and Adjusted for BMI and Age.
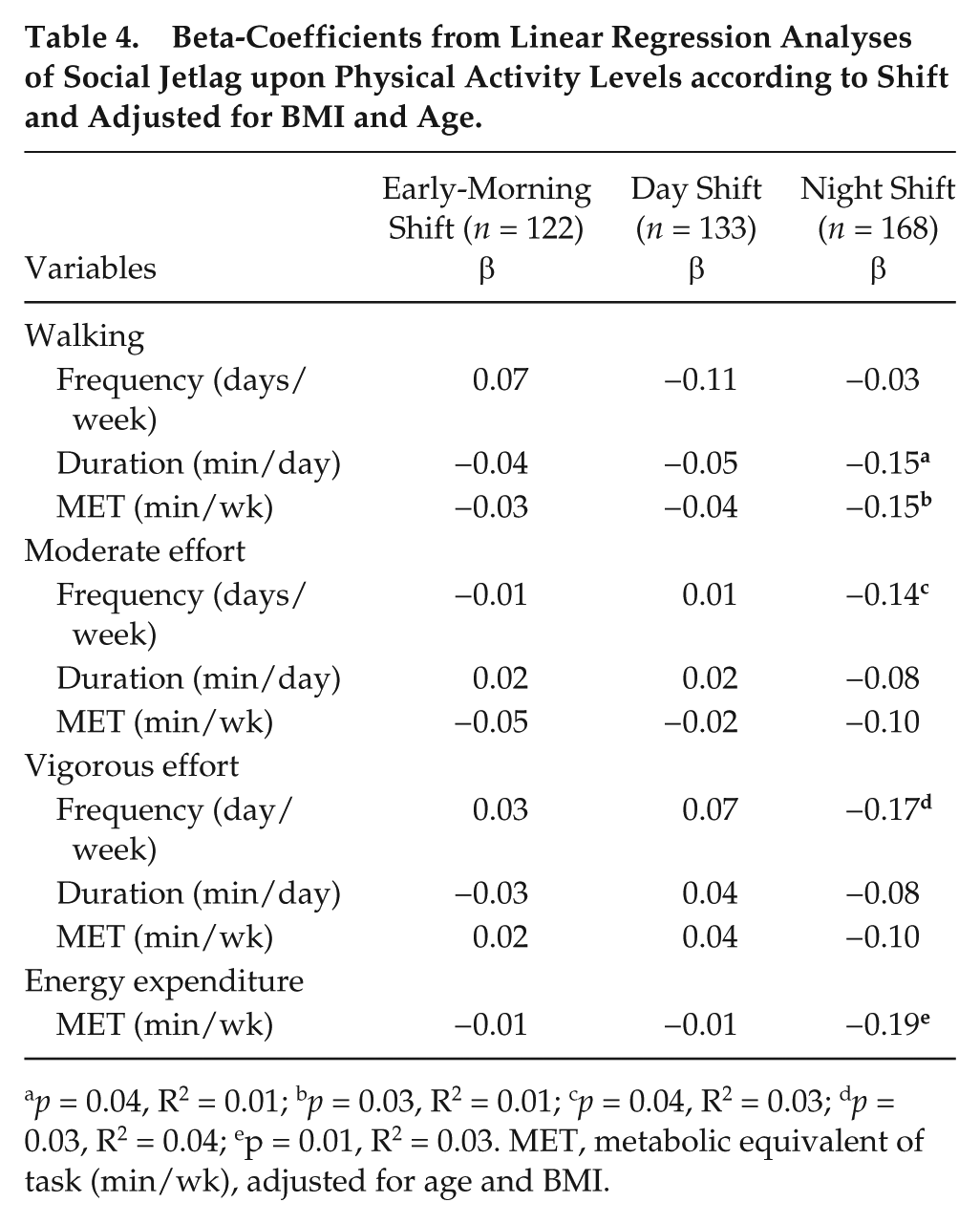
p = 0.04, R2 = 0.01; bp = 0.03, R2 = 0.01; cp = 0.04, R2 = 0.03; dp = 0.03, R2 = 0.04; ep = 0.01, R2 = 0.03. MET, metabolic equivalent of task (min/wk), adjusted for age and BMI.
Table 5 shows the beta-coefficients from linear regression analyses of SJL upon the frequency, duration and energy expenditure of different types of PA across the different BMI groups (<25 kg/m² and ≥25 kg/m²), adjusted for age and sex. There was no association between SJL and different variables of PA in subjects with BMI <25 kg/m² and BMI ≥25 kg/m².
Beta-Coefficients from Linear Regression Analyses of Social Jetlag upon Physical Activity Levels according to BMI and Adjusted for Age and Sex.
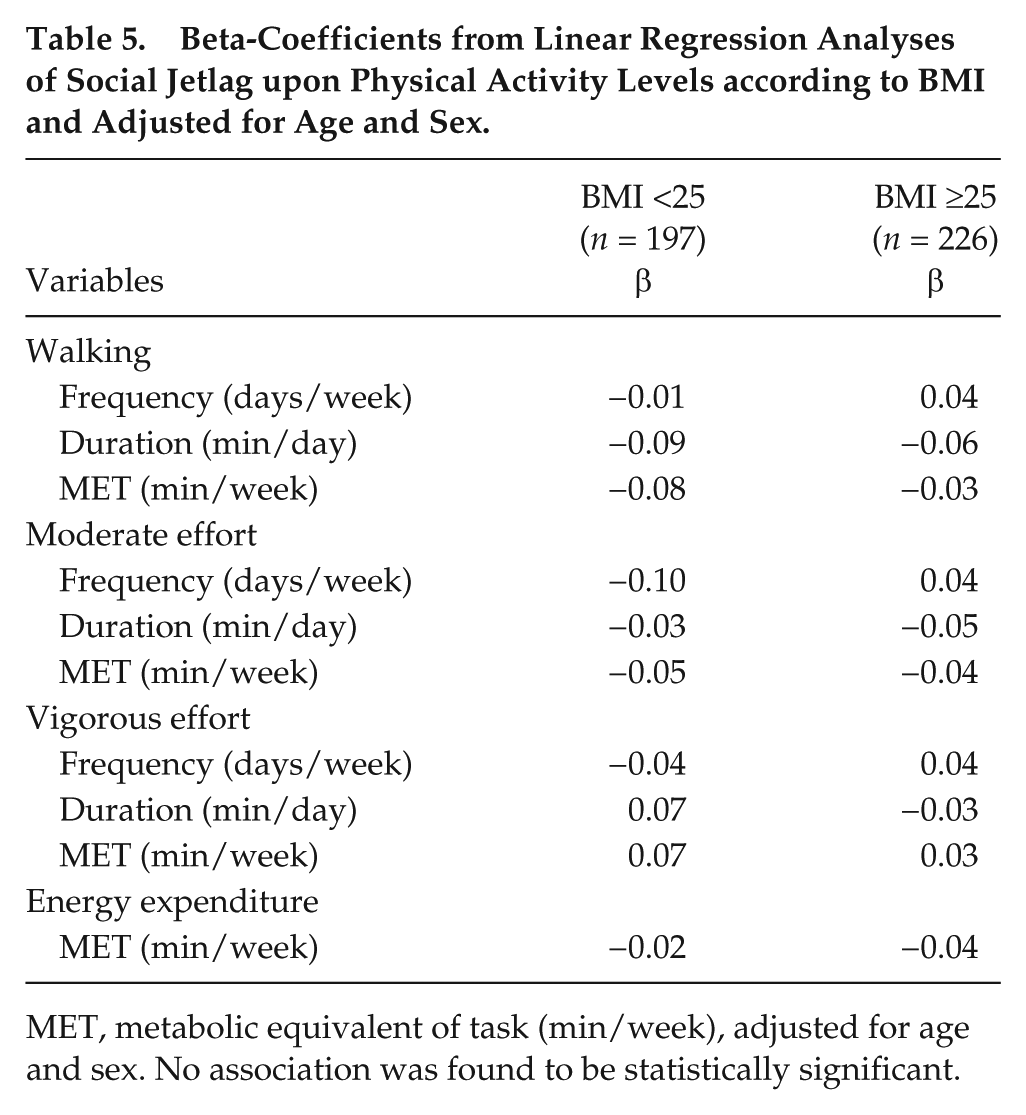
MET, metabolic equivalent of task (min/week), adjusted for age and sex. No association was found to be statistically significant.
After adjustments for sex, age, mean total sleep time, and energy expenditure, no significant associations were found between SJL and BMI (β = 0.01; p = 0.69), with all subjects grouped together. Also, for the same adjustment, no association between SJL and BMI was found for each shift separately (early-morning: β = −0.05, p = 0.58; day: β = 0.05, p = 0.54; and night: β = −0.03, p = 0.66).
In addition, no association was found between BMI and total energy expenditure related to PA (METs, min/wk) after adjusting for sex, age, mean total sleep time (β = −0.04; p = 0.65), or when analyzing the association for each shift separately (early-morning: β = −0.01, p = 0.99; day: β = −0.02, p = 0.82; night: β = −0.04, p = 0.67).
When all workers were grouped together, the results of the multivariate logistic regression adjusted for sex and age demonstrated that SJL was not a risk for overweight subjects [OR = 0.79, 95%CI = 0.46-1.34, p = 0.39].
Discussion
This study analyzed the associations between the PA pattern and SJL in subjects working different shifts at a poultry-processing company in Brazil. Although we found no differences in the PAL among workers working different shifts, the results indicate that SJL is negatively associated with the frequency of taking moderate or vigorous PA, as well as with the energy expenditure related to PA. These data suggest that the SJL of these workers could negatively influence the amount of PA. Furthermore, from the results, we can infer that night-shift workers with desynchronized social and biological clocks may undertake less PA. For these reasons, it is suggested that attempts to reduce SJL should be used as part of an educational strategy to increase PA in shift workers.
Evidence from the current study and from the literature (Petru et al., 2005; Roenneberg et al., 2012; Wennman et al., 2014) indicate that SJL is a generalized phenomenon, including among the shift-working population. A European epidemiological study conducted by Roenneberg and colleagues (2012) found that 69% of the cohort had at least 1 h of SJL. Rutters and colleagues (2014) also identified that, among 147 healthy European subjects, 63% had SJL of at least 1 h. An epidemiological study by Wennman and colleagues (2014) of over 4,000 Finnish men and women found that subjects slept less on work days and more on rest days. Vetter et al. (2015) found more than 75% of employees from all shifts had at least 30 min of SJL. In our study, if we consider the same classification for SJL (at least 30 min, as by Vetter et al., 2015), 86.4% of all workers would have SJL (data not shown), indicative of the growing concern. Juda and colleagues (2013) showed that SJL was dependent on the work shift (p < 0.001). Unlike the findings in the current study (which found the highest SJL in those working the early-morning shift, p = 0.01), Juda et al. (2013) found the highest association for SJL with the night shift (p < 0.05). Collectively, such evidence suggests that SJL is very common in workers from different shifts, and that strategies are needed to minimize SJL and protect the health of these individuals.
The influence of chronotype in developing SJL is important and has been the subject of several studies (Jansen et al., 2003; Vetter et al., 2015). Vetter et al. (2015) observed that SJL was minimal in subjects whose chronotypes were aligned to their working hours. In their intervention study, the authors adjusted subjects’ diurnal preference to their work shift. They found mean reduction in SJL of 1 h 20 min (p = 0.002), and improvement in the duration and quality of sleep (Vetter et al., 2015). The results of Petru et al. (2005) also support the need to adapt working hours to chronotype. In the present study, early-morning shift workers with SJL had a later chronotype when compared with those without SJL (MSFEsc: 3:34 [2:34-3:55] vs. 1:32 [1:05-2:09], respectively; p < 0.001), which means that SJL can be due to a mismatch between the chronotype and working hours. Furthermore, night workers without SJL showed a later chronotype (more suggestive of an evening-type individual) compared with subjects with SJL. This may reflect better tolerance to work during the night in an individual with a tendency to eveningness (Vetter et al., 2015). According to Juda et al. (2013), it would be ideal for shift workers to minimize the difference in their biological and social clocks.
The relationship between PAL and SJL is poorly described in the literature. Recently, Rutters et al. (2014) were the first to demonstrate that individuals with SJL were physically less active than those without SJL. These authors found, in a group of 145 apparently healthy participants aged 18-55 years, that participants with ≥2 h SJL were less physically active compared with those with ≤1 h SJL (p = 0.05). Importantly, here we show that SJL seems to impair the frequency of taking moderate and vigorous PA, and is associated with a decreased energy expenditure related to PA in night-shift workers. Both moderate and vigorous physical activities are postulated to promote cardiovascular benefits and prevent diseases, such as obesity and hypertension (Warburton et al., 2006).
The mechanism explaining the relationship between SJL and lower PAL remains elusive. However, studies have shown that shift workers have chronic fatigue and excessive sleepiness (Folkard et al., 2003; Jansen et al. 2003), which is associated with higher SJL (Juda et al., 2013). Thus, we speculate that fatigued and sleep-restricted workers, and thus, those with higher SJL, prefer to use their free time to rest and recover from the lack of sleep and fatigue rather than participate in PA. In addition, shift work can restrict the opportunities for participating in physical activities due to limited options and free time resulting from the work schedule (Atkinson et al., 2008).
Interestingly, studies have also found that SJL can be associated with being overweight (Roenneberg et al., 2012), increased glycated hemoglobin levels in diabetes patients (Reutrakul et al., 2013), increased resting heart and cortisol levels (Rutters et al., 2014), and increased symptoms of depression (Levandovski et al., 2011). In the present study, we conducted a linear regression analysis of SJL upon PAL according to BMI, adjusting for age and sex. However, we found no association between SJL and different variables of PA in subjects separated according to BMI (<25 kg/m² and BMI ≥25 kg/m²). A multivariate logistic regression analysis was performed, adjusting for sex and age, to determine the risk of being overweight (BMI ≥25 kg/m²) among those who had SJL and to eliminate potential confounders.
Other linear and logistic analyzes in the present study found that the relationship between SJL and PAL cannot account for a relationship between SJL and obesity. Our results are in concordance with those of Rutters et al. (2014), with there being no association between BMI and SJL in a group of subjects of similar age and nutritional status to those in our study. Yet, contrary to our study, Roenneberg et al. (2012) found a significant positive association between BMI and SJL in a study with overweight individuals. It is possible that we did not find this relationship because subjects in our cohort were not obese; most of the subjects with excessive weight presented a BMI up to 30 kg/m² (see variability in BMI in Table 1). Longitudinal studies with subjects who are overweight and obese are needed to study the associations among SJL, nutritional status and PAL.
In our study, over 49% of the employees were considered inactive. This is a very high proportion, considering that the Brazilian population is lower (46%) but already regarded as problematic (Malta et al. 2015). This finding implies that shift workers are exposed to greater health risks than the general population, particularly since most shift workers perform less than 150 min of exercise per week, the value recommended by the World Health Organization as necessary a protection from chronic disease (WHO, 2000). Similar findings have been obtained in other studies (Marqueze et al., 2014, Garcez et al., 2015). Whereas Garcez et al. (2015) found a higher prevalence of PA among night-shift workers compared with day-shift workers (39.0% vs. 30.8%; p = 0.006), Marqueze et al. (2014) showed that irregular shift workers had higher average times of moderate PA during their leisure time as compared with day-shift workers (98.5 [166.2] vs. 23.1 [76.0] min/week; p < 0.01). We did not find differences among the shift work groups in relation to the frequency of PAL, but our findings did highlight the high prevalence of insufficiently (<10 min/wk) and moderately (10-149 min/wk) active individuals, and the long periods of time in which they were engaged in sedentary behavior (Table 2). In another study, where the focus was not on assessing PAL, the authors found that longer working hours was associated with decreased PAL during leisure time (Bushnell et al., 2010).
The questionnaire used to assess PAL (IPAQ) provides us the data of sedentary behavior on work days and rest days, which was not statistically different between shifts. Although this is not an exact measure of how much PA is performed on each day (work and rest)—the questionnaire does not specifically measure this—we do know that more time sitting (analyzed as a “sedentary behavior”) is indicative of less PA (Wennman et al., 2014). These results lead us to believe that subjects do not undertake PA on work days because they are fatigued, restricted sleep and misaligned, factors that impede PAL (Schneider et al., 2005; Kouvonen et al., 2013). On the other hand, on the rest day, subjects most likely use this time to rest and compensate for any lack of sleep; and it is important to note that the sleep time on rest days is higher than on working days (10.0 h vs. 6.3 h, respectively; Table 1). Intervention strategies that encourage the practice of PA in shift workers should be conducted and based on the implementation of changes in the workplace. According to the American College of Occupational and Environmental Medicine (2004), these strategies should publicize the benefits of maintaining an active life, provide opportunities for PA in the workplace, set goals that motivate employees to increase their PAL, and include assessments of physical fitness and regular examinations for these shift workers. Moreover, the presence of a professional physical education area in the workplace would be very important, because this could encourage changes related to PAL in shift workers, which, in turn, could change behavioral patterns (Torquati et al., 2016).
We found a high prevalence of problems in sleep patterns among shift workers, with a poorer self-reported quality of sleep among subjects who worked “atypical” hours (early-morning and night shifts) as compared with those who worked the day shift (p = 0.001). Indeed, those who worked the early-morning shift showed less sleep time on work days (6.3 h) as compared with those on other shifts (p < 0.001). These results agree with those from a study conducted in Germany by Vetter et al. (2015), where early-morning shift workers slept less (6 h 23 min [29 min]) than those working the night shift (7 h 11 min [56 min]) (p = 0.003). On the other hand, we observed longer sleep times (10 h; p = 0.003) on rest days in those working the early-morning shift.
In addition, there was a high prevalence of overweight/obesity and high values for WC among all groups in the present study. Subjects in the day and early-morning shifts carried slightly higher excess weight than the Brazilian population (50.8%; Portal Brazil, 2014). However, higher WC values among shift workers were also found in the study by Balieiro et al. (2014) (night shift, 86.4% vs. day shift, 72.4%; p = 0.03). The current literature clearly indicates that a high WC is an independent predictor of cardiovascular risk and metabolic syndrome (Macagnan et al., 2012), and is prevalent among shift workers (Biggi et al., 2008). It is noteworthy that the different proportions found in our study between being overweight/obese and having high WC values (less for night workers than for other shift workers) are contrary to those from many published studies, which generally show a higher proportion of problems among night-shift workers (Di Lorenzo et al., 2003; Biggi et al., 2008; Antunes et al., 2010; Macagnan et al., 2012). Variables such as age, amount of time working in shift work, and job function could explain such differences.
This study has some limitations. First, it is a cross-sectional design, which does not establish causal relationships. Some evaluations were carried out using questionnaires which, although validated in other studies, are subjective in nature and depend on an individual’s memory and motivation. The study was also conducted upon a convenience sample, and this may have led to selection bias.
Conclusion
We conclude that SJL is negatively related to the duration and weekly energy expenditure on walking, frequency of moderate and vigorous PA, and total energy expenditure related to PA in night workers. Although no difference in PAL was found for those working different shifts, it is important to emphasize the high prevalence of individuals who were insufficiently active and engaged in sedentary behaviors among all groups of workers. These results suggest that SJL may adversely affect PA and other health variables among shift workers. Longitudinal research is needed to elucidate the relationship between PA, SJL and shift work.
Footnotes
Acknowledgements
The authors thank Jim Waterhouse.
Conflict Of Interest Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.