
Abstract
Background
Despite well-known benefits of family involvement and interventions, gaps remain in their implementation in early intervention for psychosis. Guidelines have been developed for early psychosis services to bridge evidence-implementation gaps. Little attention has been paid to their nature, quality and recommendations regarding family involvement and interventions. We aimed to identify, describe, and appraise family-focused recommendations in Canadian early psychosis guidelines.
Methods
We conducted a systematic review (PROSPERO#CR042020208974), including Canadian guidelines/standards for first-episode psychosis/early intervention in psychosis, or for psychosis/schizophrenia with a section on first-episode psychosis/early intervention for psychosis. The search was conducted in Google and Google Advanced of 58 websites (April 2024). From each document, bibliographic information and family-focused recommendations were extracted. All family-focused recommendations were subject to content analysis and mapped against a patient and family engagement framework. All guidelines were appraised using Appraisal of Guidelines Research & Evaluation—Recommendation EXcellence (AGREE-REX), assessing rigor and implementability. Family-focused recommendations were rated on three AGREE-REX items. Findings were narratively synthesized.
Results
Seven documents were included, with five provincial early psychosis guidelines and two Canada-wide schizophrenia-spectrum guidelines. 96 family-focused recommendations were extracted covering 21 themes (19 appeared in ≤4 guidelines; two (family psychoeducation; involving families in treatment-planning) in five guidelines). No guidelines had recommendations regarding families in inpatient care; only two guidelines had recommendations for navigating consent vis-à-vis family involvement. 77.4% of recommendations were about direct care; 22.5% about involving families in organizational design/governance; and none about policymaking involvement. AGREE-REX ratings for relevant outcomes and local applicability were lower for family-focused recommendations than overall guidelines. Most guidelines fared poorly in eliciting families’ values/preferences.
Conclusion
Few family-focused recommendations featured consistently across early psychosis guidelines. There was little guidance on navigating barriers to family involvement. Our analysis revealed critical gaps, including in viewing families as partners in treatment decision-making and services/policy design. Future guidelines must integrate stakeholders’ values/preferences and guidance on real-world implementation.
Introduction
As most individuals are young at the onset of psychosis, 1 families play a critical role in the lives and treatment of persons with first-episode psychosis, initiating help-seeking, supporting and promoting service engagement and medication adherence, and liaising with treating teams particularly during crises.2,3 Numerous studies have linked family involvement with outcomes in first-episode psychosis such as reduced relapses and all-cause mortality, improved quality of life and functional and subjective recovery.4,5 Consistent with this evidence, early intervention services for psychosis typically involve family members in treatment. Unfortunately, however, such family involvement is higher at the outset of treatment, and then reduces and becomes inconsistent.6,7
In psychosis, family interventions, such as family psychoeducation and multiple family group therapy, are among those with the most consistent evidence for their benefits. 8 Despite these benefits, gaps remain in their implementation and uptake in early intervention services for psychosis. Implementation rates for family interventions in early intervention for psychosis range from 57% to 80%9,10 and uptake is even lower, with only 0.1–32% attending all family psychoeducation sessions.11,12 Disconcertingly, qualitative research points to families consistently feeling excluded, not regularly informed, their perspective not adequately considered, their needs not sufficiently assessed or met, 13 and their involvement obstructed by various barriers.11,14–18
A useful starting point to understand these challenges in involving families and implementing family interventions is to examine the nature and quality of clinical practice guidelines for early psychosis, particularly with respect to their recommendations for family involvement and interventions. Guidelines are used by service planners and providers to plan, monitor, and prioritize healthcare practices. Several provincial and Canada-level guidelines have been published to promote standardized, evidence-based service delivery across early intervention in psychosis programs.19–24
In Canada and globally, there have been growing arguments for seeing patients and families not merely as care recipients but as partners in care and in designing services, research, guidelines, and policies.18,25 Particularly in early intervention for psychosis, patient and family engagement are widely acknowledged as foundational.26,27 Whether and how these professed values are operationalized within guidelines and their recommendations remains unknown. We also do not know if and how evidence-based family interventions 3 feature as recommendations in guidelines.
Healthcare programs and providers need support to apply evidence-based recommendations in diverse real-world settings. Populations, contexts, and resources vary widely, and multiple factors can either facilitate or hinder uptake.28,29 Yet, Canadian psychosis guidelines have not been examined for how well they address implementability.
Addressing these knowledge gaps, this study's specific objectives were to (a) identify and systematically describe family-focused recommendations in Canadian guidelines for early intervention services for psychosis; (b) map family-focused recommendations against a well-known patient and family engagement framework to identify gaps in recommendations for family engagement; and (c) assess their quality and implementability.
Methods
Our study is a systematic review of Canadian clinical guidance documents on early psychosis, followed by their critical synthesis and quality appraisal. This is the Canadian-focused part of a larger knowledge synthesis registered with PROSPERO (#CR042020208974). We systematically searched for grey literature as clinical guidance documents are generally non peer-reviewed publications. 30 A search protocol was developed supported by a university librarian. Two independent reviewers conducted a Google and Google Advanced search of 58 websites (government, health, academic, networks such as the Canadian Consortium for Early Intervention in Early Psychosis [CCEIP, now called Early Psychosis Intervention Canada]) using 10 terms which combined psychosis or schizophrenia with early intervention, early detection, early identification, prevention, and coordinated speciality care. Where there were too many pages of results, searches were limited to the first five pages as recommended by the librarian. The larger review covered the period between 2000 and 2023. For this particular study, to ensure the inclusion of the latest early psychosis standards or guidelines from Canada, an additional Google search was conducted in April 2024 focused only on documents from Canada (which did not result in any new Canadian guidelines being included). The CCEIP (which includes members from across Canada) was also contacted and confirmed that the documents included in this paper are the most updated versions of each province's guidelines and that no other early psychosis guidelines or standards have been published other than the included ones. Pertinent peer-reviewed publications (e.g., a publication about guidelines for schizophrenia) from a comprehensive scoping review of early intervention for psychosis 31 were also considered.
Inclusion and Exclusion Criteria
Documents were included if they: i) were labeled as guidelines or standards (from here on, guidelines will be used for brevity); ii) exclusively focused on first-episode psychosis or early intervention in psychosis, or focused on psychosis/schizophrenia and had a dedicated section on first-episode psychosis or early intervention for psychosis; iii) focused on either a province within Canada or all of Canada; and iv) were in English or French. When multiple versions were found for the same jurisdiction, the most recently dated guideline was included.
Excluded documents were dissertations, informational reports, program descriptions or evaluations, and publications exclusively centered on pharmacotherapy.
Two reviewers screened titles and executive summaries; retained eligible documents; carried out deduplication; independently screened full texts; and made final selections. Decisions were based on consensus and discrepancies resolved by author SNI.
Data Extraction and Management
Two authors independently extracted and discussed pertinent data from all included guidelines onto a predesigned MS Excel spreadsheet and received ongoing team feedback/guidance from senior author SNI. Document characteristics were extracted including authors, publication year and type (guideline or standards), targeted age group, geographic scope, funding source, focus (early intervention for psychosis-focused or not), length, and number of bibliographic references.
All family-focused recommendations (conceptualized broadly to include any family involvement in treatment and family interventions) were extracted separately into two categories (a) “Specific recommendations,” a specific recommendation or performance indicator (typically presented as a bullet point/box/numbered section) and (b) “General statements,” recommendations found in general sections but not explicitly labeled as a recommendation (e.g., a sentence such as “families should be considered key partners” in the introduction to the guidelines document). Clinical guideline developing bodies 32 typically focus on the first category of recommendations. There were few to almost no disagreements between raters with respect to their extraction of these objective descriptive elements.
Data Analysis and Synthesis
Quality Appraisal
The Appraisal of Guidelines Research & Evaluation—Recommendation EXcellence (AGREE-REX), a validated nine-item instrument developed in 2019, was used to assess the quality of recommendations in the included guidelines. 33 The AGREE-REX was chosen because it assesses rigor of evidence and methodology, as well as implementability of recommendations (e.g., were stakeholder preferences considered, adaptation to local context, etc.).
As recommended, 33 three scores were derived for (a) items on a 7-point scale (1 = lowest quality; 7 = highest quality) (b) domains by adding up scores for the three items each that fell under Clinical Applicability; Values and Preferences and Implementability; and (c) overall by adding up all item scores. Items 3 (Applicability to patients/populations), 5 (Values and Preferences of Patients/Populations) and 9 (Local Application and Adoption) were rated twice, for overall recommendations and for the cluster of family-focused recommendations. Domain and overall scores were converted into percentages and classified as >70% = high quality, <30% = low quality, and 30–70% = moderate quality, as per the AGREE-REX manual. 33
Four raters, with experience in early psychosis, independently appraised the guidelines using AGREE-REX and arrived at final scores via consensus. For documents not exclusively early psychosis-focused, appraisal involved reviewing the early intervention in psychosis, introductory, and methodology sections. During the consensus meeting, each rater first shared their individual scores; if the scores were identical or quite similar, then one rater presented their detailed justification for their scores and the other raters added any missing points; if the scores were different, each reviewer presented their justification without interruption followed by a group discussion to resolve disagreements; and final scores were arrived at by consensus. Senior author, SNI, was present during all consensus meetings.
Content Analysis to Derive Themes
A directed content analysis approach was used where each family-focused recommendation was assigned theme(s), that had been either defined before (using existing literature)18,34,35 or during (informed by data) analysis.36,37 Examples of some themes identified a priori were family psychoeducation, family role during hospitalizations or inpatient care, families involved in treatment and discharge discussions/decisions, etc. An example of a theme derived from the data is family involvement in community outreach. To do this, two raters independently categorized and refined key elements into codes (e.g., assess the satisfaction of families), code categories (e.g., questionnaires, record whether families were consulted during initial intake in clinical notes), and finally themes (e.g., assessment of family-focused domains), through iterative discussion and refinement. To ensure rigor, the two raters met regularly to discuss codes and themes, resolved disagreement by consensus and documented decisions. The raters were trained and supervised throughout by senior author SNI. The list of themes was finalized by the two raters and SNI.
Mapping Against an Engagement Framework
Specific family-focused recommendations were mapped using a patient and family codesigned multidimensional framework for patient and family engagement in healthcare. 38 Each recommendation was categorized as aligning with one of three options within the framework's “levels of engagement” (involvement in direct care; organizational design, and governance and policymaking) and “continuum for engagement” (consultation, involvement, and partnership and shared leadership). Engagement is seen as higher in partnership and shared leadership than in involvement, and higher in involvement than in consultation. The framework also recognizes individual, organizational and systemic factors that influence engagement. This categorization was done independently by authors HM and SNI, and disagreements (which were very few) were resolved by discussion.
Synthesis
As is common for literature reviews, including reviews of guidelines and interventions, a narrative synthesis approach was finally used to present and make sense of the findings.39–43 To ensure rigor and trustworthiness, all authors contributed to the final synthesis, with primary responsibility taken by authors HM and SNI, who refined synthesis and interpretation based on iterative discussion. Synthesis was done in various stages, starting with tabular presentation and description of findings from data extraction of document characteristics, content and mapping analysis of each document; followed by comparing results across documents, considering quality appraisal; and then synthesizing results within and across documents by pulling on relevant literature about early psychosis, family interventions, and involvement in psychosis and implementation science. Before preparing this manuscript, results were also presented to various stakeholders with experience in early intervention for psychosis during four meetings, and their feedback used to refine interpretation. These practices are consistent with good practices for synthesis in reviews.39,40
Results
Description of Included Guidelines
Seven guidelines (from 2009 to 2022) were included (Table 1, Figure S1). Five of these were from the grey literature search and two from our search of peer-reviewed literature. 31 Five were guidelines for specific provinces: New Brunswick (NB), 24 Nova Scotia (NS), 44 Quebec (QC), 19 Ontario (ON), 21 and British Columbia (BC). 20 These were developed and funded by their respective provincial health ministries. The provincial guidelines exclusively focused on early intervention in psychosis, except the NS guidelines which applied to mental health services in the province, with a specific section on early intervention in psychosis. The two peer-reviewed guidelines focused on schizophrenia-spectrum disorders, with specific sections on first-episode psychosis and early intervention (Canada2017a and Canada2017b).22,23 All guidelines covered recommendations for pharmacological and psychosocial interventions. All early intervention in psychosis guidelines targeted adolescence and early adulthood, but no two stipulated the same age range. Five were only in English; one was only in French (QC) and one was in both languages (NB). Only one guideline (QC) had a previous version, which was considered but excluded.
Description of Included Documents in Chronological Order.
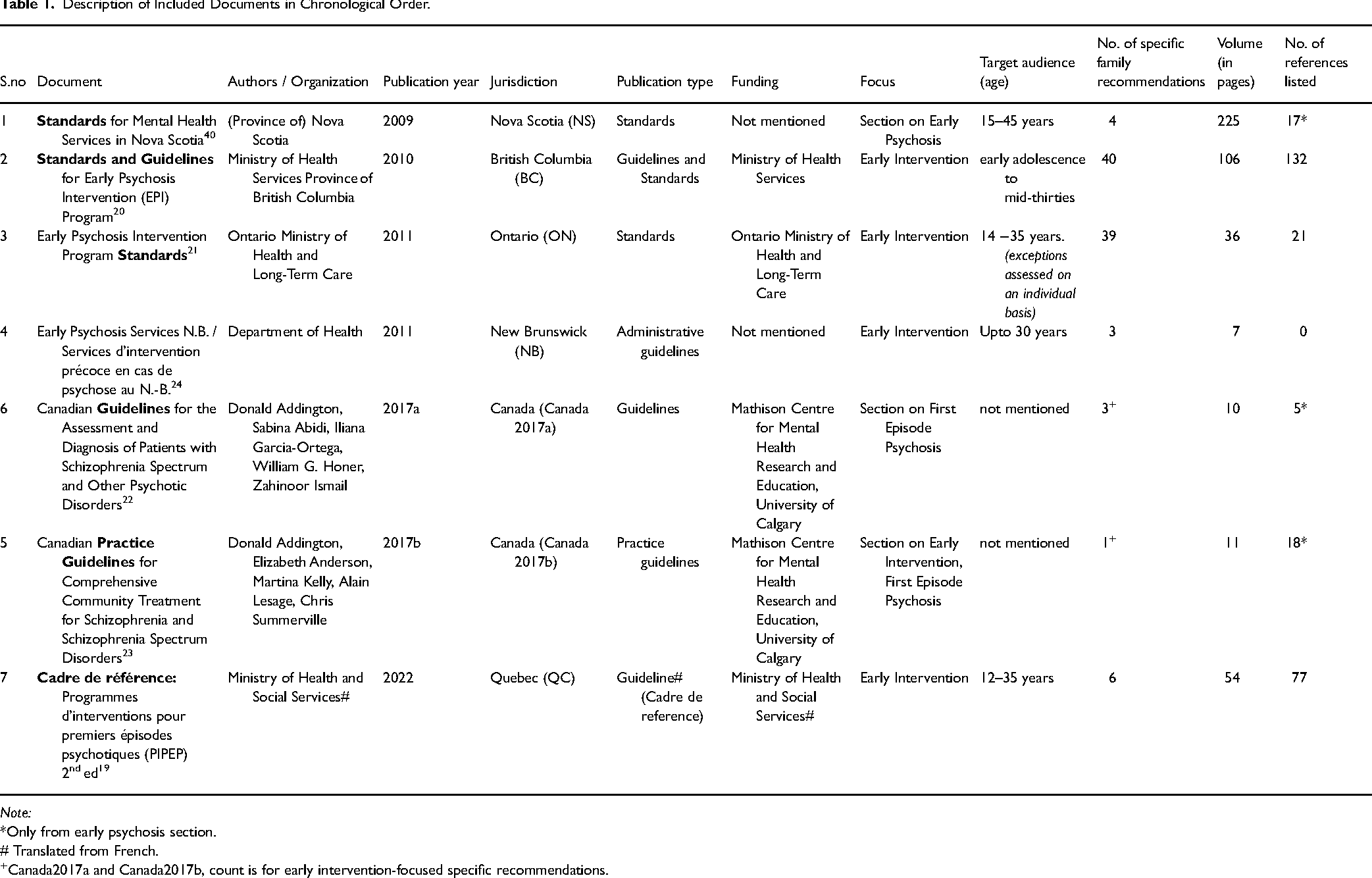
Note:
*Only from early psychosis section.
# Translated from French.
Canada2017a and Canada2017b, count is for early intervention-focused specific recommendations.
Supplemental information was also used in extraction and quality appraisal where this was provided. Specifically, we reviewed and extracted information about the detailed methodology for the two Canadian guidelines which was outlined in an additional publication. 45 The QC guidelines referenced the government's overall mental health action plan, 46 which was considered in extraction and appraisal.
Involvement of Families in Guideline Development
The development of the two Canadian guidelines involved two named family caregivers as members of their national multidisciplinary team. The ON standards named one family member from a named family organization as having been involved. The BC guideline referred to an advisory council including members from family organizations (numbers and names not provided). The NS guideline referenced seeking consumer opinions, although it is unclear if this included families. The NB and QC documents had no information on whether families were involved (the QC document had a list of names with no additional details).
Quality Appraisal
As can be seen in Table 2, only one document (BC) scored high quality overall and for its three domains. One document (NB) scored low quality in all three domains and overall. This was a brief guideline (seven pages with includes both English and French version) which may have resulted in low scores. The remaining five guidelines were of moderate overall quality, with individual domains also ranked moderate in quality. The two Canadian guidelines, however, were ranked high quality in the clinical applicability domain, scoring high on items relating to integrating “evidence” and “applicability to target users” given the use of detailed, rigorous methodology. 45
Heatmap Showing an Overview of AGREE-REX Scores in Chronological Order.
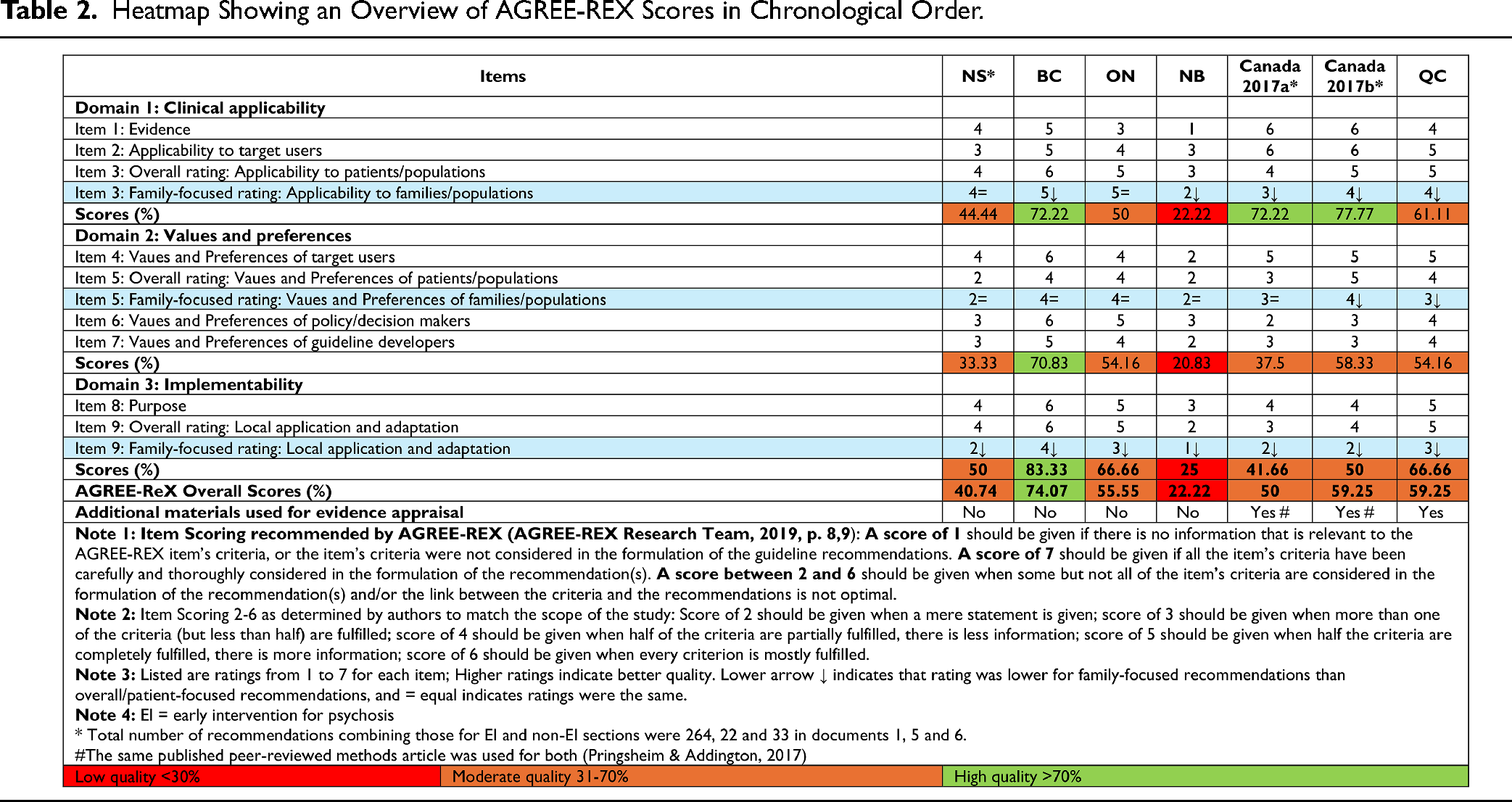
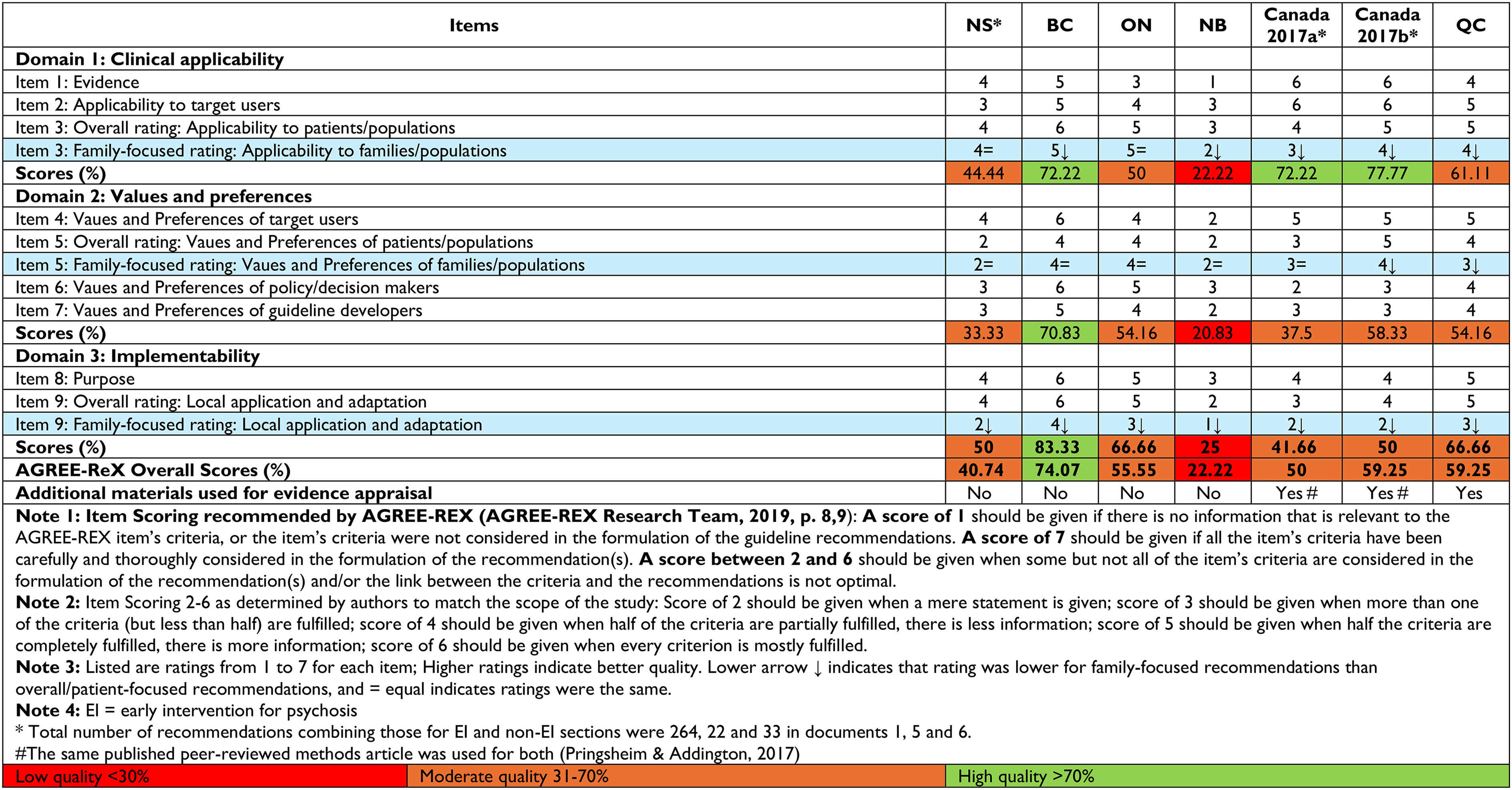
On the three pertinent items, family-focused recommendations were never rated higher than overall recommendations. On item 3, which assesses the extent to which relevant outcomes were considered in developing recommendations, how these were ascertained as relevant, and whether recommendations were tailored to particular populations, five of seven documents scored lower for family recommendations than overall, with scores mostly in the low to low-moderate range, except for BC and ON which scored higher.
On item 5, all guidelines performed in the low to low-moderate range for overall and family-focused recommendations, indicating that most had not elicited the values and preferences of families (and patients) in developing guidelines (or in reporting this if these were elicited), and in considering the acceptability of recommendations. BC, ON, NS, NB, and Canada2017a had identical ratings, for overall and family-focused recommendations. Ratings were one point lower for family-focused compared to overall recommendations in the case of QC and Canada2017b guidelines.
On Item 9, which focuses on local implementability covering aspects like how recommendations can be tailored to local contexts/settings, costs, resources, training/competencies, etc., all guidelines consistently performed lower on family-focused recommendations than on overall recommendations, with low scores for the applicability of family-focused recommendations across all guidelines except BC which had a moderate rating.
Themes
Twenty-seven themes were identified from the literature and analysis of the extracted recommendations (Table 3). One theme identified as salient in the literature, “families involved during their ill family member's inpatient care” was not identified in any of the included guidelines. Supplementary Tables a-g present each recommendation against its corresponding theme for each guideline.
Family Work Themes from Specific Recommendations and General Statements, Arranged in Order of Frequency of Endorsement across Guidelines (n = 27).
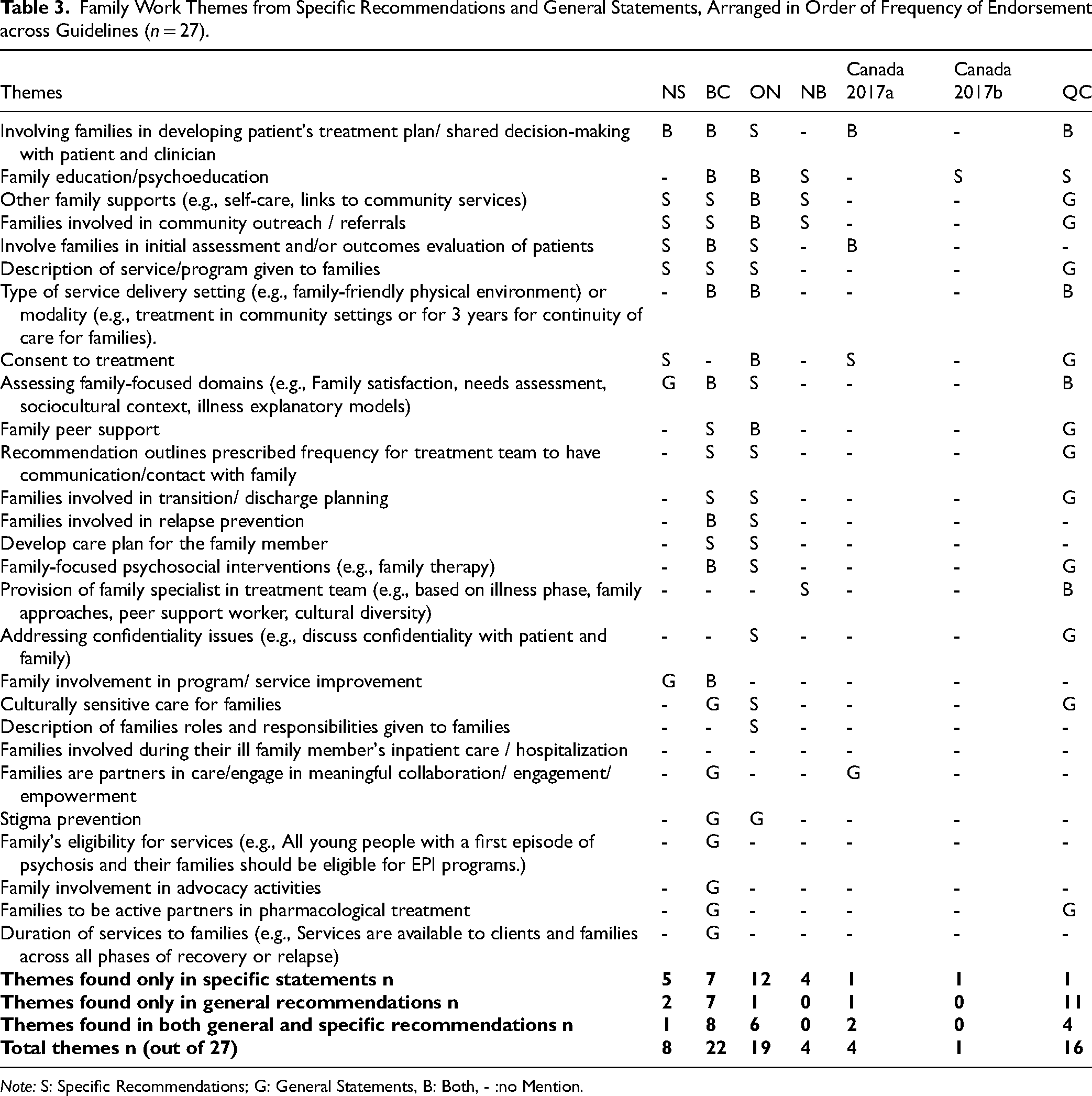
Note: S: Specific Recommendations; G: General Statements, B: Both, - :no Mention.
Specific Family-Focused Recommendations
Ninety-six specific family-focused recommendations were identified from all seven guidelines, The number of specific family-focused recommendations, as well as the proportion of total recommendations they comprised, varied widely; BC: 40 (26%); ON: 39 (47%), QC: 6 (17%); NS: 4 (15%); NB: 3 (18%); Canada2017a: 3 (43%); and Canada2017b: 1(33%). These 96 specific recommendations touched on 21 themes, as seen in Table 3.
The two most commonly endorsed themes by specific recommendations (five of seven guidelines) pertained to involving families in developing patients’ treatment plan (BC, Canada2017a, ON, NS, QC), and provision of family education or psychoeducation (BC, Canada2017b, ON, NB, QC). Four guidelines each made specific recommendations regarding families’ involvement in community outreach (BC, ON, NS, NB); providing other family supports such as community resources and self-care management (BC, ON NB, NS); and involving families in patients’ assessments (NS, BC, ON, Canada2017a).
The remaining themes (e.g., involving families in navigating consent issues or discharge planning, making description of services available to families, family peer support, culturally sensitive care for families) only featured in specific recommendations in three or fewer of the seven guidelines.
General Family-Focused Statements
Five of seven guidelines (BC, Canada2017a, ON, NS, QC) contained 43 general family-focused statements, some of which were broad (“Services include crisis and emergency response service, and individual/group/family assessments and treatment services” 24 (p.19)), whereas others referred to concrete practices (“In rural areas, peer linking may require creative and diverse strategies (e.g., family-to-family newsletters, secure web-based discussion groups, etc.)”) 20 (p.48). These general statements spanned 24 themes, as can be seen in Table 3. General statements in the QC guideline covered more themes than specific recommendations and, although not presented in a box such as their specific recommendations were, they were still worded as recommendations, for example, under “addressing confidentiality,” a general statement was “a young person whose family is already aware that he or she is being followed at PPEP may refuse to allow his or her parents to be met and involved in his or her follow-up, but these parents could still receive general psychological education about psychosis and its treatment[transl].” 19 (p.29) However, this theme was not covered in their specific recommendations.
Engagement Framework
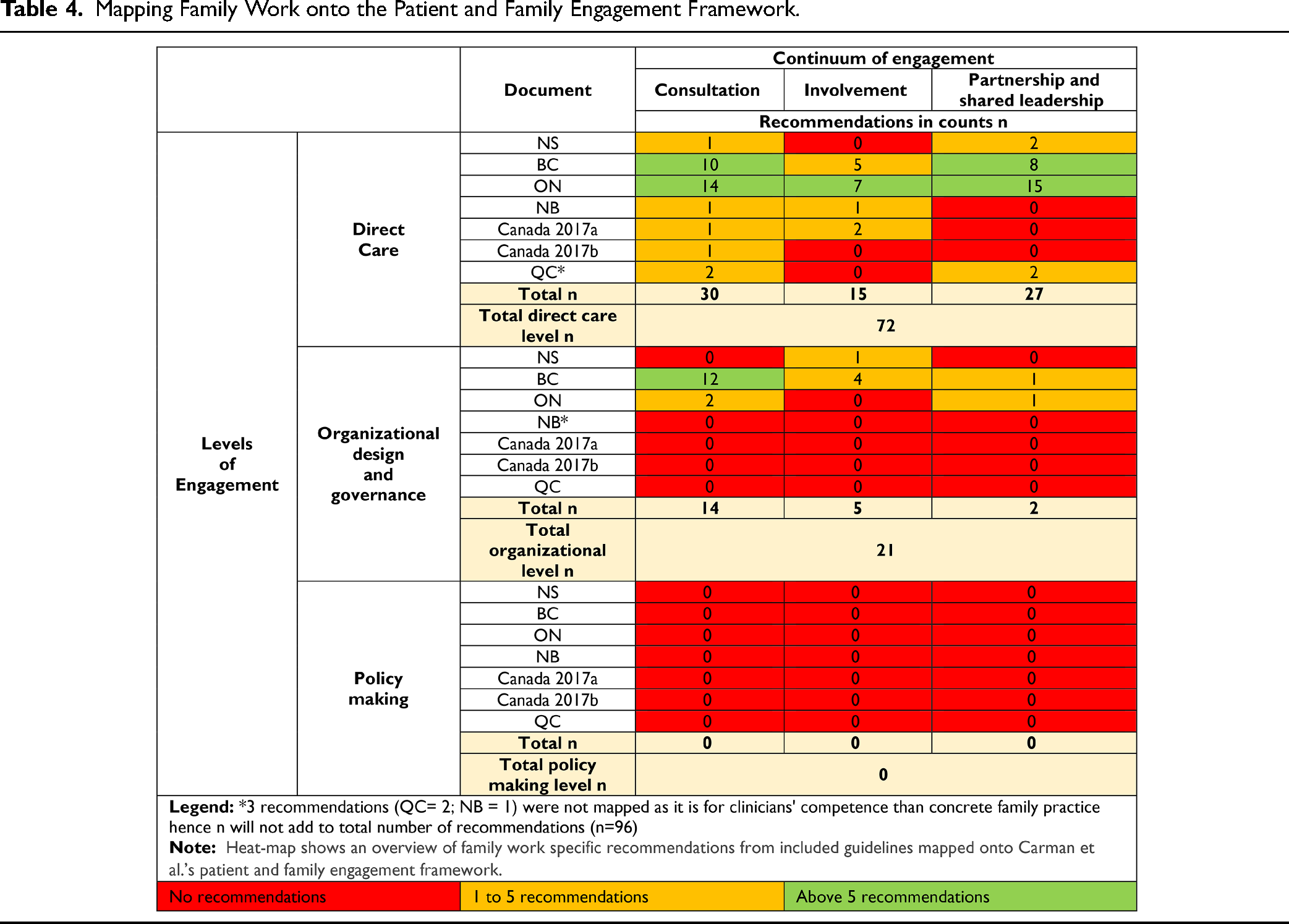
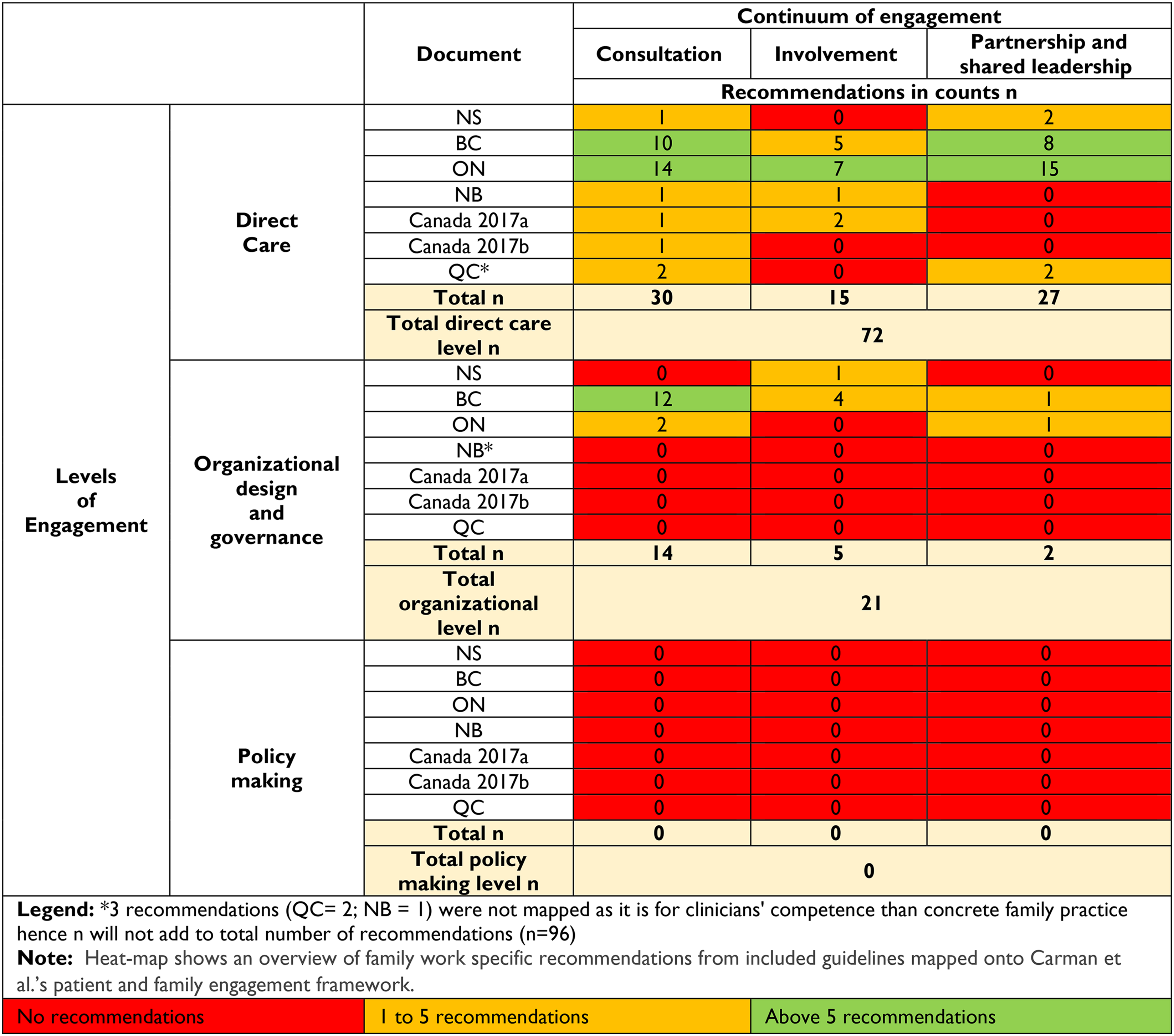
Three out of 96 recommendations focused on clinicians’ skillsets rather than tangible practices for families and were therefore not mapped against the engagement framework. As seen in Table 4, most recommendations (n = 72/93, 77.4%) fell under the “direct care” level of engagement, within which the highest number of recommendations reflected the lowest degree of the continuum of engagement, that is, consultation (30/72, 41.6%), followed by partnership and shared leadership (27/72, 37.5%) and then involvement (15/72, 20.8%). Only 21 recommendations from three jurisdictions (BC, ON, NS) had recommendations for involving families in organizational design and governance (n = 21/93, 22.5%) that reflected lower degrees of the continuum of engagement (consultation = 14; involvement = 5; partnership and shared leadership = 2). There were no recommendations about involving families in policymaking. Supplement a-g presents each recommendation by level and continuum of engagement.
Mapping Family Work onto the Patient and Family Engagement Framework.
Discussion
Content of Family-Focused Recommendations
All extant Canadian guidelines for early intervention for psychosis have family work-focused recommendations covering a variety of themes, reflecting their acknowledgement of “families” as a key stakeholder group in the treatment of psychosis. Disconcertingly, only few of the same recommendations featured consistently across all or most guidance documents.
Most guidelines had recommendation(s) around involving families in their loved one's assessment and treatment planning, although these varied in number and level of detail. Most guidelines also emphasized family education or psychoeducation, aligning with the meta-analytic evidence for its benefits. 47 Beyond psychoeducation, most guidelines had relatively sparse recommendations about specific family-focused interventions (e.g., multiple family group therapy) and patient-focused interventions that involve families (e.g., cognitive-behavior therapy for psychosis), despite their rich body of evidence.48–50
Most explicit recommendations were about involving families in “direct care” with less than a quarter recommending their involvement in organizational design and governance and none recommending their involvement in policymaking. The few recommendations about involving families in design and governance rarely saw them as partners with shared leadership. This may partially be attributable to increased breadth and depth of patient and family engagement becoming more prominently encouraged relatively recently in Canadian healthcare. 51
Three of the seven guidelines made explicit recommendations about assessing families’ needs and satisfaction with services. The BC guideline provided 12 additional measurable family-focused indicators (e.g., number of care plans signed by families and number of families engaged) and the ON guideline additionally recommended assessing families’ goals and aspirations.20,21 These domains could be considered as candidates by measurement-based care and learning health systems in early psychosis. 29
Consent, Confidentiality, and Family Involvement
With two exceptions (ON with an explicit recommendation, QC with general statements), there was no advice for navigating patients’ consent and confidentiality vis-à-vis involving families in treatment. Consent and confidentiality can significantly deter family engagement in early psychosis intervention and mental healthcare.18,52 While strategies to navigate disagreements around decision-making and confidentiality among patients, caregivers, and families have been proposed in the literature,27,52,53 these did not feature in the recommendations.
Encouragingly, both ON and QC provide clear, converging recommendations for when patients refuse consent for involving families, namely, that treating teams discuss the benefits of family involvement with the patient and if the patient still refuses, treating teams can listen to the family's concerns and provide them psychosocial support and education (while respecting patient's choice by not disclosing details about their care). Using these as exemplars and being guided by literature and stakeholder inputs, future guidelines must make recommendations for involving families when patients refuse consent, that acknowledge consent as fluid (e.g., patients may consent but not want all information to be shared with families) and evolving (e.g., patients may refuse consent to involve families initially but agree later during treatment).18,27,52,53
Quality and Implementability of Family-Focused Recommendations
Our analysis highlighted significant gaps in the quality of recommendations within Canadian early psychosis guidelines. The first pertains to the little attention paid to implementability and applicability considerations such as training, resources, and adaptations to local contexts, which may help explain the gaps between evidence and standards on the one hand and practice on the other hand in early psychosis programs, and their poor and inconsistent implementation of family-focused recommendations.28,35,54 Generally, there has been limited implementation science work in early psychosis.55,56 Family work recommendations were much more likely to be formulated in ways that did not support their implementability, with generic statements or statements lacking operationalizable detail (e.g., “This [referring to treatment in early interventions services for psychosis] should be multidisciplinary and encompass the following: …Family involvement and family interventions…”) 23 (p. 667).
The second gap pertains to many guidelines not having actively and systematically elicited the values and preferences of families; specified outcomes relevant for families; or clarified how listed outcomes were chosen as relevant. Families were mentioned as having been involved in developing only two early psychosis-specific and the two Canada-wide guidelines. Most documents and evidence informing them were created prior to the patient-oriented research push in Canada. 51 Low(er) ratings on this (and other AGREE-REX) item(s) may have also arisen because sufficient information (e.g., if families were included, how their opinions were considered) was not reported in the guidelines. Given that “engagement” is at the heart of early psychosis intervention, 57 it is incumbent upon those developing guidelines that recommendations reflect the values and preferences of families (and patients) and that the strategies used to gather these are clearly outlined. Strategies could range from involving family members (with diverse lived experiences) during guideline development to integrating literature on the values and preferences of families. These may be helpful in identifying practices that may not yet have the highest levels of strength and consistency of evidence 58 but may be consistently valued by lived experience stakeholders (e.g., peer support).
The third gap pertains to most guidelines not detailing how and when recommendations should be tailored to particular subsets of families based on age, ethnicity, religion, and family member type (e.g., sibling/spouse/parent), and their intersectionalities. Equity considerations have increasingly become central in healthcare, but most guidelines were published over eight years ago. Definitions of “family” and familial values and views about mental illnesses and caregiving are influenced by social-cultural dimensions.59–61 Factors like ethnicity have also been shown to impact uptake of family interventions 62 along with being associated with risk for psychosis and pathways to care.63,64
Limitations and Strengths
Our review focused on family-focused recommendations in early psychosis guidelines, but the extent to which early psychosis programs are actually guided by jurisdictional guidelines (and/or Canadian guidelines) is not clear. Nonetheless, because these guidelines enjoy the support of relevant ministries, they could be argued to be credible representations of minimally acceptable standards of early psychosis care in their respective jurisdictions. Only five among Canada's 10 provinces and three territories have published early psychosis guidelines, despite early psychosis services also operating in at least four other provinces.
On the AGREE-REX, 33 a score of 1 (lowest quality) could either reflect the poorest quality or that guideline developers failed to describe their methodology. Our protocol did not allow us to distinguish these unless we contacted all developers, which we did not do. While the AGREE-REX provides thresholds for high, moderate, and low quality for overall scores, it does not provide similar thresholds for individual items and domains. We used similar cutoffs for individual items and domains, along with detailed descriptions of their quality. Notwithstanding these limitations, AGREE-REX permits a comprehensive evaluation of recommendations in terms of their implementability and rigor and should be used when developing future guidelines.
Our review also has noteworthy strengths. Our critical analysis using multiple methods—bottom-up content analysis, top-down mapping against an engagement framework and quality appraisal—yielded a first-ever, thorough portrait of the state of family-focused recommendations in Canadian early psychosis guidelines and helped identify substantive (e.g., family involvement in policymaking, specific family interventions) and process (e.g., involving families as partners rather than only consulting them) gaps.
Implications
Our systematic synthesis of family-focused recommendations across Canadian guidelines for early intervention in psychosis provides all jurisdictions and early intervention programs a menu of strategies for family involvement and interventions and a list of convergent practices (e.g., psychoeducation) to be prioritized.
Given our focus on Canadian guidelines, we cannot determine whether findings generalize to other regions where early psychosis services are more widely implemented. National guidelines may exert stronger influence in the UK 65 and Australia 66 than in Canada's provincially driven system. Nonetheless, evidence of inconsistent implementation of family engagement elsewhere35,67,68 underscores the need to examine the quality of family-focused recommendations in guidelines across jurisdictions.
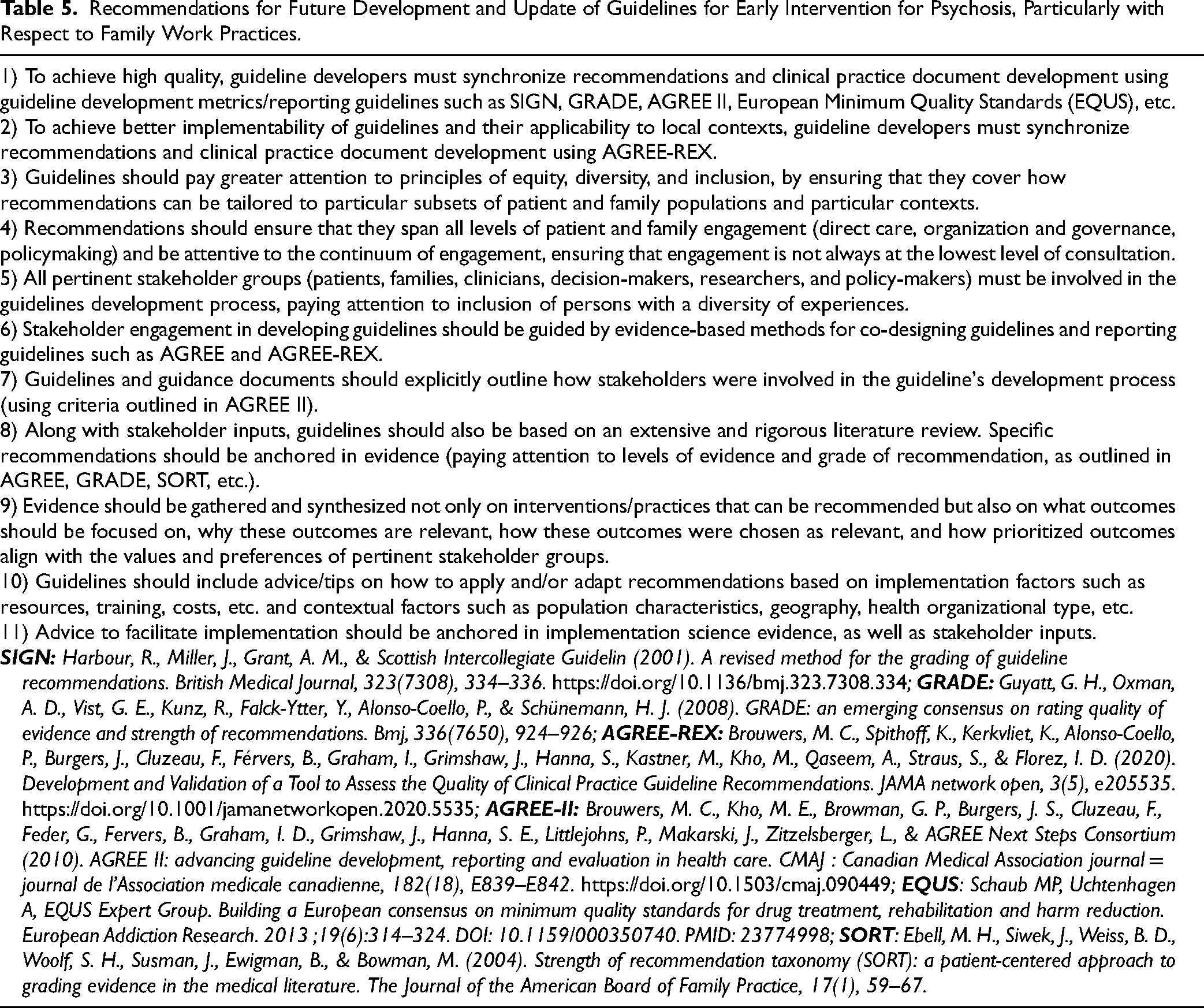
Given that guidelines inform delivery and optimization of patient and family care, it is critical that they are implementable in routine practice and provide the best possible evidence- and values-informed recommendations for direct care and for involving families (and patients) in services and policy design. Based on identified strengths and gaps, we propose concrete recommendations for practice and future guideline development in early intervention services for psychosis (Table 5). Since AGREE-REX could be used as a methodological checklist to formulate and report the quality of recommendations, our results serve as a benchmark against which future early psychosis guidelines and recommendations can be measured.
Recommendations for Future Development and Update of Guidelines for Early Intervention for Psychosis, Particularly with Respect to Family Work Practices.
Data Access
All source data (“guidelines”) used in this publication are already available to all. All other data has been reported in main and supplemental tables and figures.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251393981 - Supplemental material for Family-Focused Recommendations in Canadian Guidelines for Early Intervention Services for Psychosis: A Systematic Review: Recommandations axées sur la famille dans les Lignes directrices canadiennes relatives aux services d’intervention précoce en cas de psychose : Une revue systématique
Supplemental material, sj-docx-1-cpa-10.1177_07067437251393981 for Family-Focused Recommendations in Canadian Guidelines for Early Intervention Services for Psychosis: A Systematic Review: Recommandations axées sur la famille dans les Lignes directrices canadiennes relatives aux services d’intervention précoce en cas de psychose : Une revue systématique by Helen Martin, Ruben Valle, Nicole Pawliuk and Srividya N. Iyer in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors acknowledge Kevin MacDonald for his support with the project. The authors also thank Dr. Navdeep Kaur and Dr. Kathleen MacDonald for their valuable feedback on the initial manuscript draft. Special thanks to Dr. Aarati Taksal for her contributions in reviewing the manuscript and compiling the reference list.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Srividya N. Iyer received salary support from Fonds de recherche du Québec–Santé (FRQS) and the Canada Research Chairs program. This project was funded by the Canadian Institutes of Health Research (FDN 143333); Principal Investigator: Iyer.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.