
Abstract
Objective:
This systematic review critically evaluated clinical practice guidelines (CPGs) for treating adults with major depressive disorder, dysthymia, or subthreshold or minor depression for recommendations following inadequate response to first-line treatment with selective serotonin reuptake inhibitors (SSRIs).
Method:
Searches for CPGs (January 2004 to November 2014) in English included 7 bibliographic databases and grey literature sources using CPG and depression as the keywords. Two raters selected CPGs on depression with a national scope. Data extraction included definitions of adequate response and recommended treatment options. Two raters assessed quality using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument.
Results:
From 46,908 citations, 3167 were screened at full text. From these 21 CPG were applicable to adults in primary care and outpatient settings. Five CPGs consider patients with dysthymia or subthreshold or minor depression. None provides recommendations for those who do not respond to first-line SSRI treatment. For adults with MDD, most CPGs do not define an “inadequate response” or provide specific suggestions regarding how to choose alternative medications when switching to an alternative antidepressant. There is variability between CPGs in recommending combination strategies. AGREE II ratings for stakeholder involvement in CPG development, editorial independence, and rigor of development are domains in which depression guidelines are often less robust.
Conclusions:
About half of patients with depression require second-line treatment to achieve remission. Consistency and clarity in guidelines for second-line treatment of depression are therefore important for clinicians but lacking in most current guidelines. This may reflect a paucity of primary studies upon which to base conclusions.
Depressive disorders, including major depressive disorder (MDD), subthreshold depression, and dysthymia, are complex illnesses associated with disability and reduced quality of life. Depressive disorders impose a substantial societal and economic burden, 1 –6 have a negative impact on overall health, 7 –11 and are linked with increased incidence of various illnesses and diseases. 12 –20 Although several modalities exist for treating depressive disorders, pharmacotherapy remains the most common first-line treatment strategy. The response to first-line treatment is moderate (40%-60%), 21 –23 while remission following antidepressant treatment is achieved in a minority of patients (from 30%-45% 21,22 to 53% 23 ). Evidence regarding the efficacy of antidepressants for treating dysthymia is sparse; approximately half of the trials indicate a superior response to antidepressant medications versus placebo. 24 –30 Few studies have focused on treating subthreshold (or minor) depression. 30 –32
Despite increases in prescribing of antidepressant medications, 33 discernible decreases in the prevalence of MDD have yet to be noted in countries where before-after comparisons have been feasible. 34,35 This may be because a substantial number of depressed individuals continue to receive inadequate treatment. 36 Clinical practice guidelines (CPGs) for depression treatment are intended to aid clinician decision making at various stages of treatment, including following an inadequate response to a first-line therapy as this is a common outcome of treatment. Little information exists, however, regarding the quality and consistency of current CPGs that address this clinical decision point.
To investigate consistency (or, alternatively, variability) in treatment recommendations for depression following inadequate antidepressant response, we systematically evaluated recent CPGs for MDD, dysthymia, and subthreshold/minor depression. To date, there has been limited formal evaluation of such guidelines. One group has previously assessed the quality of several national CPGs in treating depression in primary care settings specifically 37 using the initial version of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument. 38 The CPGs failed to “meet the criteria on rigor of development, applicability, and editorial independence.” This conclusion appears consistent with findings from another critical appraisal that used the AGREE to evaluate guidelines for treating psychotic depression. 39 Another group reported that of 29 CPGs for depression, only 10 indicated the level of evidence on which their recommendations were based. 40 Finally, in an evaluation of European CPGs for treating psychiatric illness, 8 of which addressed mood disorders specifically, 41 the domain of editorial independence was rated lowest, while stakeholder involvement, rigor of development, and CPG applicability were rated moderately.
Objective
Given the relatively poor response rates to first-line antidepressant treatment, as well as the negative consequences of untreated depression, clear guidance regarding treatment options for nonresponders is important for clinicians. The goals of this review are therefore 1) to review systematically the recommendations for second-line treatment of depression and 2) to critically appraise CPGs (using the AGREE II) that included any approach for patients who have not responded to at least one adequate course of antidepressant pharmacotherapy.
Methods
This study stems from a comparative effectiveness review sponsored by the Agency for Healthcare Research and Quality (AHRQ), US Department of Health and Human Services, 43 which provided copyright release for the publication of this article. The findings and conclusions presented in this article are those of the authors and do not necessarily represent the views of AHRQ. No statement in this report should be construed as an official position of AHRQ or of the US Department of Health and Human Services. The comparative effectiveness review focused on 4 research questions related to depression treatment following unsatisfactory response to selective serotonin reuptake inhibitors (SSRIs). 43 The current study reflects the findings pertaining to the evaluation of CPGs following response failure to an adequate course of antidepressant pharmacotherapy with a 4-year update (since 2011).
Search Strategy
The search strategy included CPGs published from 1980 to February 2015. We limited grey literature searches for CPGs published from January 1, 2004, to November 2014. The key search terms are outlined elsewhere. 43 The databases searched were MEDLINE, Cochrane Central, PsychINFO, Cochrane Database of Systematic Reviews, EMBASE, CINAHL, and AMED. The grey literature search (i.e., Internet) included systematic searches of relevant citations on the relevant websites (see online Appendix A). Members of a technical expert panel involved in preparation of the comparative effectiveness report were queried for any additional relevant sources. The reference lists of eligible citations and systematic reviews were also searched for potentially eligible citations.
Clinical Practice Guideline Selection
CPGs were defined as “systematically developed statements about specific clinical problems intended to assist practitioners and patients in making decisions about appropriate health care.” 44 We included full guidelines and consensus statements but excluded medical algorithms (i.e., decision-making tools) with no background or description of the process by which the algorithm was developed. CPGs were eligible for inclusion in the systematic review if they provided recommendations for treating adults (≥18 years of age) and adolescents (8 to 18 years) with a primary diagnosis of MDD, dysthymia, or subthreshold or minor depression who exhibited an “inadequate response” to pharmacological treatment with an antidepressant as the first line of treatment. CPGs for treating other forms of depression (e.g., postpartum depression, bipolar depression) were excluded, as were CPGs for treating depressive disorders in individuals with a primary neurological condition.
Standardized forms were pilot tested for study selection. Two reviewers independently screened citations; a third reviewer resolved conflicts.
Assessment of CPG Quality
The AGREE II is a validated checklist used to assess CPGs and compare across guidelines. 45 –47 Two raters used the AGREE II instrument to assess CPG quality. 42 The AGREE II consists of 6 domains used to evaluate the rigor and transparency with which a guideline is developed (i.e., the quality and clarity of a guideline). In brief, the domains consist of the following: 1) scope and purpose (items 1-3), 2) stakeholder involvement (items 4-6), 3) rigor of development (items 7-14), 4) clarity of presentation (items 15-17), 5) applicability (items 18-21), 6) editorial independence (items 22-23), and 7) an overall assessment (item 24).
Data Extraction from and Syntheses of the CGPs
Qualitative syntheses of data extracted using standardized and piloted forms from the CPGs included information on the following: 1) patient population (i.e., individuals with MDD, dysthymia, or subthreshold or minor depression), 2) definition of an adequate/inadequate response, 3) types of interventions and treatment specifications (e.g., monotherapy vs. combination therapy), and 4) basic information regarding each of the CPGs included in the systematic review (e.g., country of origin, intended setting for CPG application, and intended users).
Results
We captured a total of 30 (39 publications) CPGs (Suppl. Figure S1, online Appendix B). 48 –70 From the 30 CPGs, 18 (27 publications) were specific to adults, 48 –50,53,55 –58,60 –65,67,69 –76 9 specific to adolescents, 77 –85 and 3 applicable to both adults and adolescents. 51,54,59 Summary information for the adolescent CPGs is reported elsewhere. 43
From the 21 CPGs for adults, 4 were updated within our search interval, 49,51,53,68,69,86 –88 and we report only the most recent version of these updated guidelines. 49,51,53,69 Six CPGs published by the National Institute of Clinical Excellence (NICE) are interrelated 57,58,73 –76 ; from these we evaluated 2 unique CPGs. 57,58 Six publications 61 –63,89,90 are related to the Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines, 3 of these are recommendations, 61 –63 and the remaining 3 are publications providing supporting documentation for the methods used in the guidelines. 63,89,90 Finally, 1 publication is a summary companion paper 91 of another CPG from the American College of Physicians 67 ; the two were evaluated as a single CPG.
Seventy-three studies were excluded from this review because of the following: 1) publication prior to 2004 (n = 45), 2) exclusive focus on diagnosis or screening rather than treatment (n = 7), 3) not a population of interest (n = 15), and 4) a treatment algorithm was presented with no background or description of the process by which it was developed to confirm CPG status (n = 6).
Qualitative Syntheses of CPG Characteristics
Table 1 presents the characteristics of the CPGs for treating adults with MDD, dysthymia, and subsyndromal depression as a function of country of origin, setting, and intended users. Three CPGs were developed for specific populations, including elderly patients in the community 65 and in long-term care homes, 60 and inmates in federal prisoners. 53 One CPG included recommendations for patients with depression and cardiovascular disease. 64 The remaining CPGs were specific to adults with no specific comorbid conditions.
Characteristics of Evaluated Clinical Practice Guidelines Indicating Country, Disorder Type, Intended Setting, and Guideline Users.
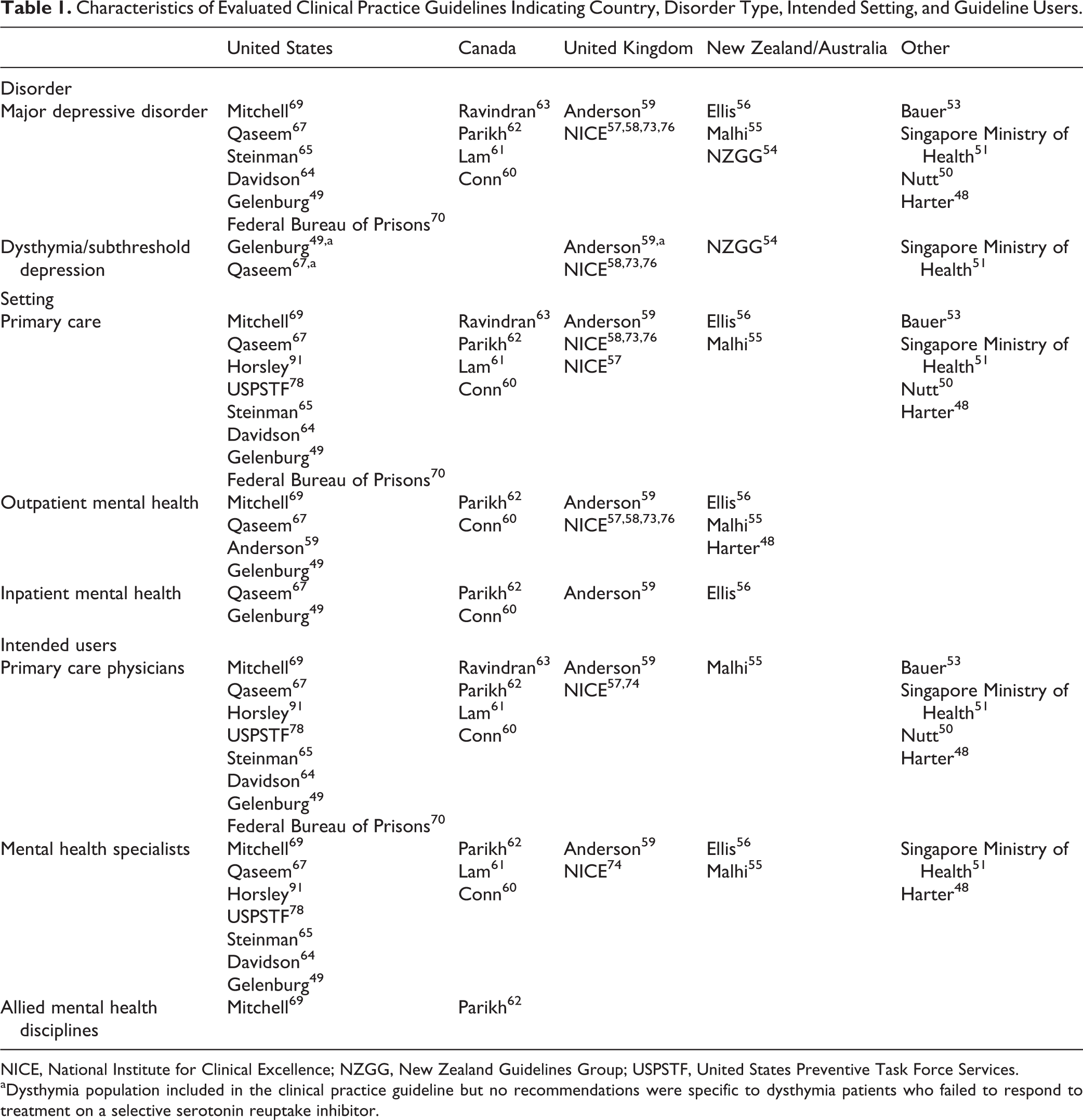
NICE, National Institute for Clinical Excellence; NZGG, New Zealand Guidelines Group; USPSTF, United States Preventive Task Force Services.
aDysthymia population included in the clinical practice guideline but no recommendations were specific to dysthymia patients who failed to respond to treatment on a selective serotonin reuptake inhibitor.
CPGs for Treating Patients with Dysthymia and Subsyndromal Depression
Six CPGs made specific note of dysthymia 49,51,54,59 or subthreshold depression. 58,67 Most CPGs do not provide an operational definition and/or distinction between these disorders, with 1 CPG including dysthymia under the label of subthreshold depression. 59 This definitional shortcoming was directly acknowledged in 1 CPG. 58
One CPG that did not distinguish dysthymia from minor/subthreshold depression did recommend second- and third-line interventions following insufficient response. 54 Another CPG 58 also notes the potential lack of discontinuity between subthreshold depressive symptoms and a MDD and provides recommendations for patients with subthreshold depression symptoms with inadequate response to first-line measures. The remaining guidelines 49,51,59,67 do not provide recommendations for treatment of patients with dysthymia and inadequate response.
CPGs for Treating Patients with MDD
All CPGs focused on treating adults with MDD are applicable to patients in primary care and outpatient settings; 6 49,56,59,60,62,67 are also applicable to inpatient settings (Table 1). All CPGs are primarily intended for primary care practitioners, with the exception of 1 CPG developed specifically for psychiatrists. 56 All but 2 of the guidelines consider various interventions for treating adult MDD; these 2 CPGs include only pharmacological interventions 67 or computerized cognitive behavioral therapy (CBT). 57 The remaining 19 CPGs recommend a variety of pharmacological, psychological, and complementary and alternative medicine interventions.
Defining an Inadequate Response
Eight CPGs define response as a 50% reduction in depression symptoms and partial response as a 25% to 50% reduction in symptoms. 49,53,54,59,61 –63,69,88 Of these, only 3 suggest different treatment strategies for those with a partial response compared to those with nonresponse to an antidepressant medication. 49,53,69 Only 1 CPG suggested a specific scale that clinicians should use to monitor symptom changes; that one recommended using the Patient Health Questionnaire-9 (PHQ-9). 54 One CPG emphasized that response should be assessed via a structured measure but provided no recommendation about what that measure should be or what threshold should be used for defining an adequate/inadequate response. 49 Two CPGs recommended evaluation of adherence to the medication as the first or early step before establishing inadequate response. 53,70 One CPG noted the inconsistencies in defining treatment nonresponders but opted to categorize patients in the context of next-step treatment options (i.e., tiered approach: if A does not work, proceed with B, etc.) rather than providing a specific definition of an inadequate/adequate treatment response. 58 The remaining CPGs did not provide a definition of inadequate response. 48,55,56,59,66,67,74
In addition, there is substantial variability regarding when an inadequate treatment response can be defined. CPGs suggest that an inadequate response can be defined at 2 to 4 weeks, 48,53,59,87,88 4 to 6 weeks, 54 and 4 to 8 weeks 49,70,86 after treatment initiation. One CPG defines an inadequate response as a partial improvement 6 to 8 weeks posttreatment. 67,87
Second-Line Treatment Recommendations
Four CPGs specific to treatment of MDD 57,60,64,65 do not provide recommendations for treating patients with an inadequate response to antidepressant interventions. Notably, no CPGs considered the specific type of first-line antidepressant when recommending second-line treatment. That is, the possibility of certain second-line treatments being more appropriate for certain first-line treatments is not reflected in current CPGs. Tables 2 and 3 present the recommended strategies for monotherapy and combination therapy following response failure to first-line treatment. Attempts were made to identify recommendations regarding specific medications. However, it is often unclear whether the information following the recommendation (e.g., “switch antidepressants”) is a selective summary of the available evidence or a recommended action. The CANMAT guidelines recommend a particular sequence of interventions following response failure to first-line treatment (second- and third-line therapies—i.e., stepped approach); however, there are several options within each intervention step. 61 –63 Other guidelines specify a stepped approach 58 or utilization of second- and third-line antidepressant medications after failure to respond to initial treatment 53,54 but are less explicit about which agents to consider. 67 Two others make a distinction between a partial response and treatment nonresponse and specified different approaches in each instance. 49,61
Treatment Recommendations in Clinical Practice Guidelines That Identified Strategies for Those That Failed Response in North America (United States and Canada).
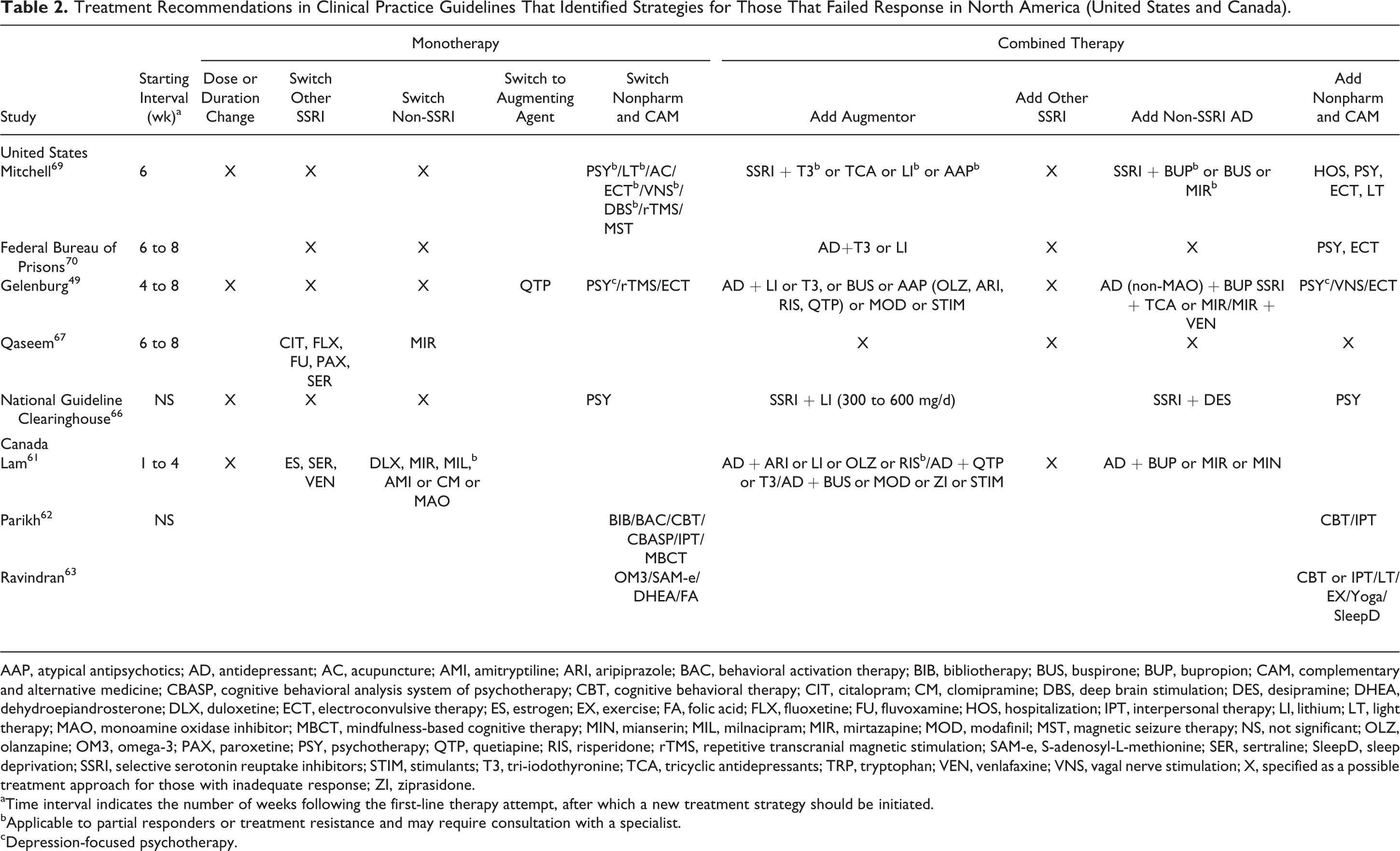
AAP, atypical antipsychotics; AD, antidepressant; AC, acupuncture; AMI, amitryptiline; ARI, aripiprazole; BAC, behavioral activation therapy; BIB, bibliotherapy; BUS, buspirone; BUP, bupropion; CAM, complementary and alternative medicine; CBASP, cognitive behavioral analysis system of psychotherapy; CBT, cognitive behavioral therapy; CIT, citalopram; CM, clomipramine; DBS, deep brain stimulation; DES, desipramine; DHEA, dehydroepiandrosterone; DLX, duloxetine; ECT, electroconvulsive therapy; ES, estrogen; EX, exercise; FA, folic acid; FLX, fluoxetine; FU, fluvoxamine; HOS, hospitalization; IPT, interpersonal therapy; LI, lithium; LT, light therapy; MAO, monoamine oxidase inhibitor; MBCT, mindfulness-based cognitive therapy; MIN, mianserin; MIL, milnacipram; MIR, mirtazapine; MOD, modafinil; MST, magnetic seizure therapy; NS, not significant; OLZ, olanzapine; OM3, omega-3; PAX, paroxetine; PSY, psychotherapy; QTP, quetiapine; RIS, risperidone; rTMS, repetitive transcranial magnetic stimulation; SAM-e, S-adenosyl-L-methionine; SER, sertraline; SleepD, sleep deprivation; SSRI, selective serotonin reuptake inhibitors; STIM, stimulants; T3, tri-iodothyronine; TCA, tricyclic antidepressants; TRP, tryptophan; VEN, venlafaxine; VNS, vagal nerve stimulation; X, specified as a possible treatment approach for those with inadequate response; ZI, ziprasidone.
aTime interval indicates the number of weeks following the first-line therapy attempt, after which a new treatment strategy should be initiated.
bApplicable to partial responders or treatment resistance and may require consultation with a specialist.
cDepression-focused psychotherapy.
Treatment Recommendations in Clinical Practice Guidelines That Identified Strategies for Those That Failed Response in Europe and Other Countries.
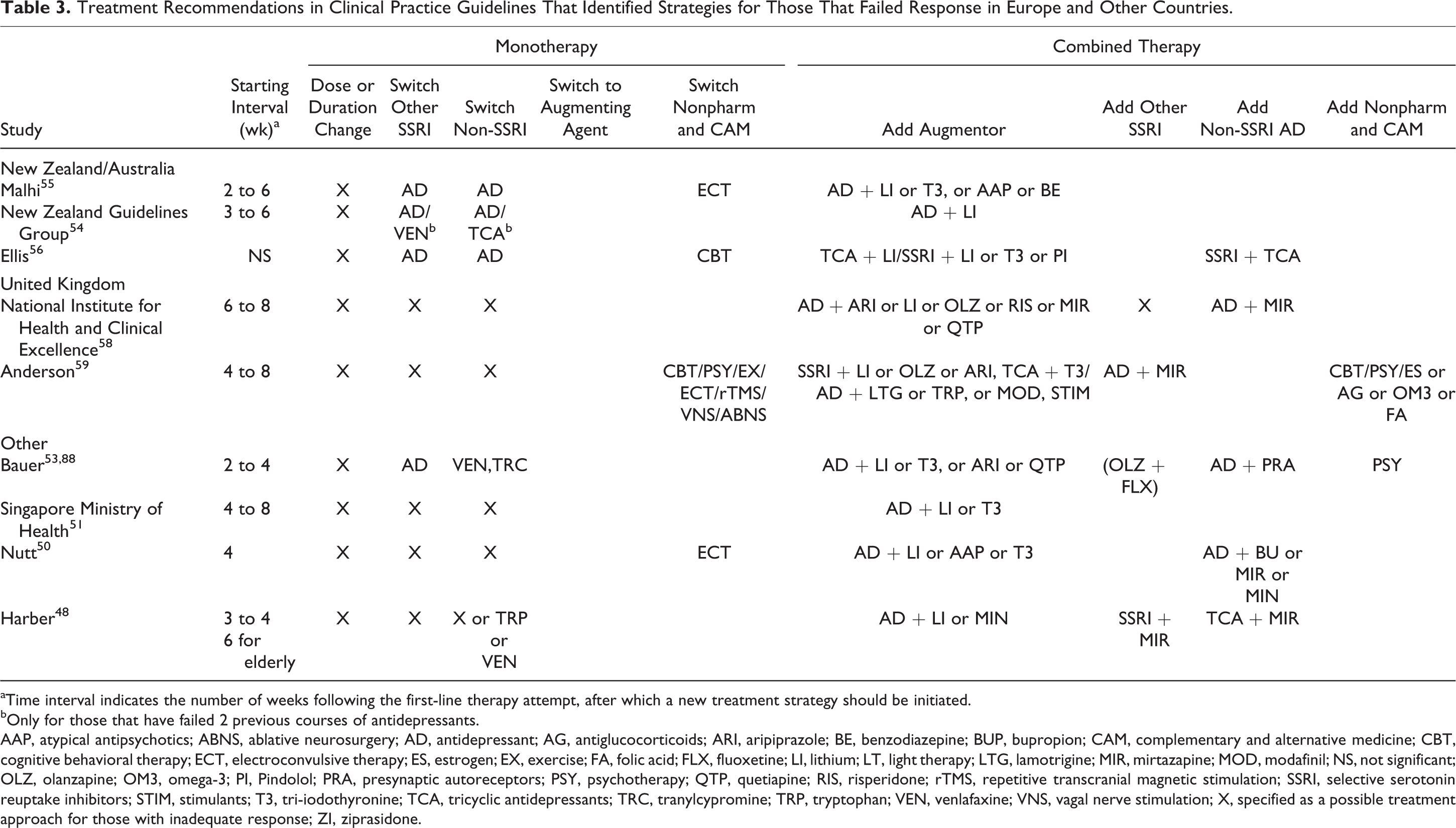
aTime interval indicates the number of weeks following the first-line therapy attempt, after which a new treatment strategy should be initiated.
bOnly for those that have failed 2 previous courses of antidepressants.
AAP, atypical antipsychotics; ABNS, ablative neurosurgery; AD, antidepressant; AG, antiglucocorticoids; ARI, aripiprazole; BE, benzodiazepine; BUP, bupropion; CAM, complementary and alternative medicine; CBT, cognitive behavioral therapy; ECT, electroconvulsive therapy; ES, estrogen; EX, exercise; FA, folic acid; FLX, fluoxetine; LI, lithium; LT, light therapy; LTG, lamotrigine; MIR, mirtazapine; MOD, modafinil; NS, not significant; OLZ, olanzapine; OM3, omega-3; PI, Pindolol; PRA, presynaptic autoreceptors; PSY, psychotherapy; QTP, quetiapine; RIS, risperidone; rTMS, repetitive transcranial magnetic stimulation; SSRI, selective serotonin reuptake inhibitors; STIM, stimulants; T3, tri-iodothyronine; TCA, tricyclic antidepressants; TRC, tranylcypromine; TRP, tryptophan; VEN, venlafaxine; VNS, vagal nerve stimulation; X, specified as a possible treatment approach for those with inadequate response; ZI, ziprasidone.
Quality Assessment of CPGs Using the AGREE II Instrument
Table 4 includes the domain scores for the AGREE II ratings of the 21 unique CPGs. All CPGs score high on scope and purpose (domain 1: 69%-100%). Scores on stakeholder involvement vary from 17% to 97%. 61 –63,63,89,90 Five of the 21 CPGs indicate that patients’ views and preferences had been sought (i.e., an item in domain 2). 48,56 –58,69 On the rigor of development (domain 3) element, scores vary from 12% to 84%. Scores are high for clarity of presentation (domain 4) (61%-94%), based on recommendations within the CPG overall, and not specific to recommendations regarding second-line treatments. When considering applicability (domain 5), scores are variable, ranging from 0% to 90%. The majority of CPGs score poorly on 2 items in this domain: 1) consideration of potential resource implications of applying recommendations and 2) presenting monitoring or auditing criteria. For editorial independence (domain 6), scores are again variable (12%-100%). In terms of raters’ overall assessment and recommendation of the CPGs for clinical use, only the NICE guideline 58 was strongly recommended by both raters. Two CPGs were not recommended, 63,64 while the remainder were recommended with provisos alterations by at least 1 of the 2 raters.
Scores from the AGREE II for Clinical Practice Guidelines for Adults.
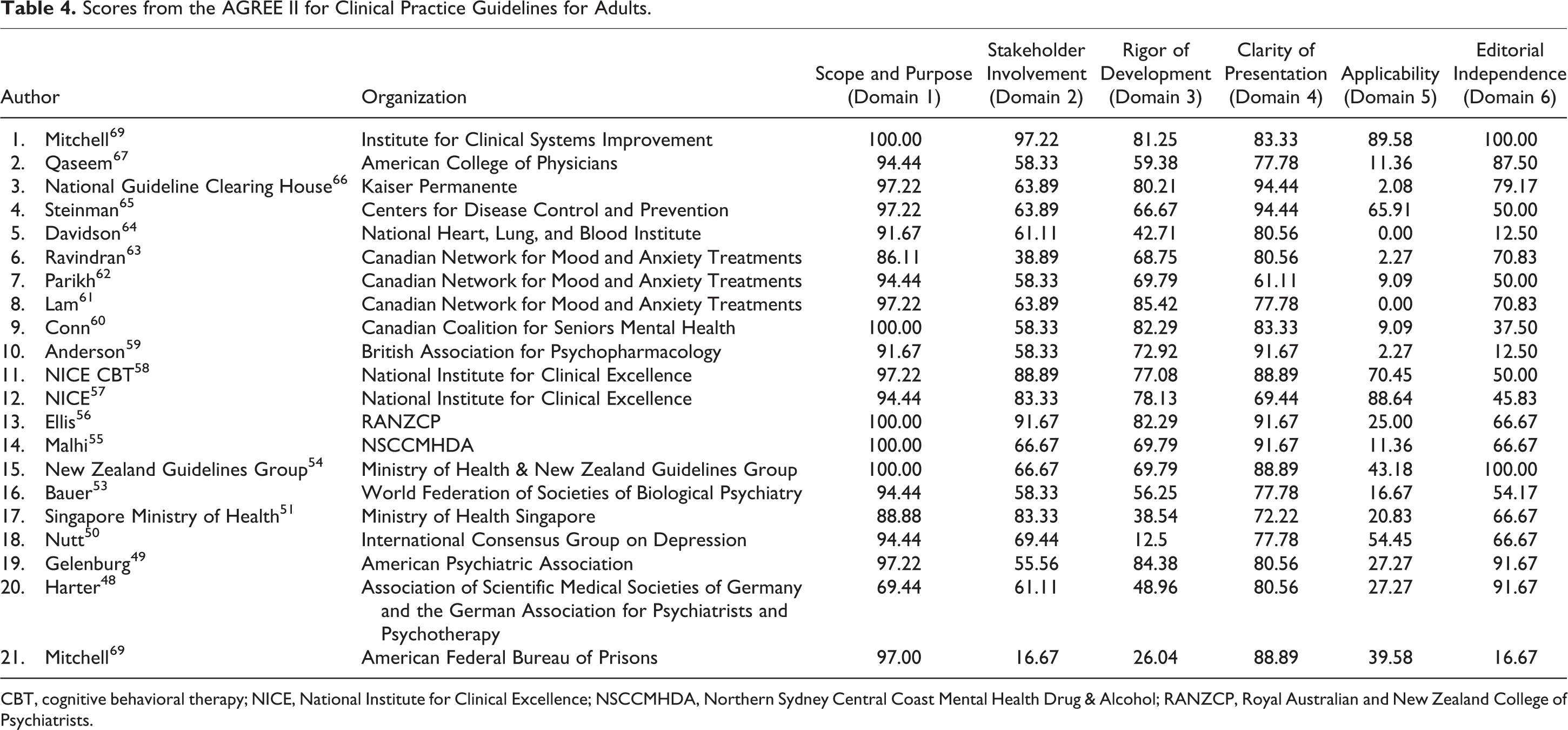
CBT, cognitive behavioral therapy; NICE, National Institute for Clinical Excellence; NSCCMHDA, Northern Sydney Central Coast Mental Health Drug & Alcohol; RANZCP, Royal Australian and New Zealand College of Psychiatrists.
Discussion
This systematic review evaluated 21 CPGs for treating adults with MDD or dysthymia/subsyndromal depression, limited to those that were published in English and applicable in a national context or developed by large national professional associations. Most guidelines address the issue of choosing second-line treatment strategies. None provides second-line treatment recommendations that considered the specific nature of the first-line treatment. The quality of the guidelines was highly variable, particularly in certain domains.
Quality of Current CPGs for Treating Depressive Disorders
The AGREE II instrument indicates that most guidelines provide good clarity regarding the aims and structure of the CPGs. Variation exists, however, in the guidelines for rigor of development, applicability, and editorial independence, which is consistent with other summaries of CPGs for depression. 37,39,41 The variability in these quality domains is amplified when the recommendations for treating individuals with an inadequate response to initial treatment are examined, perhaps because of the relative insufficiency of extant studies of second-line treatment strategies. Although some CPGs clearly state the limitations of the evidence from which they are developed, others did not. The uncertainty of the evidence therefore needs to be better highlighted in these and future CPGs. Transparency on the processes used to derive recommendations is key for future CPGs.
Although the CPGs generally rate in the moderate to high range for attempting to link available evidence with the recommendations, the AGREE II does not address the clinical sensibility (or ecological validity) of treatment strategies. The AGREE II also cannot confirm whether the best evidence is selected from which to draw conclusions. A variety of grading systems for evaluating the strength of the evidence used across guidelines contributes to this inconsistency. Future CPGs should evaluate the strength of their evidence using standardized evaluation approaches, such as the widely adopted Grading of Recommendations Assessment, Development, and Evaluation (GRADE), 92 which assesses the quality of evidence. The GRADE approach provides transparent criteria for assessing the quality of the evidence as well as separate criteria for the strength of recommendations.
Most CPGs do not include patient representation in the guideline development process; a majority of CPG panel members are physicians. Although the range of scores for editorial independence suggests that there could be improvement on this measure, there are limitations to the AGREE II approach to assessing this domain. For example, potential conflicts of interest in one CPG 49 were assessed in greater detail and showed that 100% of the CPG panel members disclosed financial relationships with industry (predominately pharmaceutical) and each member had ties with several different companies. 94
Scores for editorial independence were markedly heterogeneous, ranging from 12% to 100%, and only 8 from 21 CPGs scored at least 70% in the AGREE II domain, suggesting problems with lack of independence of guideline developers to funding body or lack of reporting of any potential conflict of interests of panel members. There are a number of studies suggesting links with guideline panel members and the quality and direction of reporting. 93 –95 There is the suggestion that even when disclosure of financial conflict of interest is transparent, this may not be sufficient to prevent potential biases. 96 Others suggest that bias is intractable, and so too is the problem of nondisclosure. 97 Groups that ensure greater safeguards to minimize competing interests of panel members may make different recommendations. 94,98 Future CPGs for MDD should consider the panel composition and manage competing interests of panel members.
Scores for the applicability domain tended to be the lowest. This domain evaluates the extent to which 1) facilitators/barriers for implementing the CPGs are recognized and discussed, 2) advice/tools on how the CPGs should be incorporated into practice are included, and 3) resource implications associated with implementing CPGs are acknowledged. As such, future CPGs should consider the feasibility of implementing the recommendations and discuss the potential barriers to this goal explicitly within the document.
Second-Line Treatment Strategies
No recommendations were identified specific for individuals with dysthymia or subthreshold or minor depression who had failed previous treatment. This may reflect a lack of current consensus regarding how to define a failed or inadequate response in patients with fewer or less severe baseline symptoms than those with MDD.
Recommendations for treatment following a failure of the first-line medication included dosing or treatment interval changes, switching to a different medication, or adopting an alternative therapy. These recommendations were generally nonspecific regarding optimal dosing, which alternative treatments should be considered, or the duration of treatment prior to initiating a change. Combination therapy recommendations generally identified the types of antidepressants and augmenting agents that should be considered following a first-line antidepressant nonresponse. There was high inconsistency across CPGs with regard to the types of augmenting agents to use, however.
There is also little attention given to the appropriateness of second-line strategies in the context of the first-line treatment. Dose increases may be a preferable strategy for some but not other antidepressant medications. Choosing a second antidepressant following the failure of a first might—or might not—be guided by the specific properties of the first failed antidepressant. Some augmentation agents might preferentially augment certain antidepressant medications in comparison to others. This lack of attention to the potential for second-line strategies to be guided by the first-line treatment may reflect a paucity of extant primary studies addressing these critical clinical questions.
Limitations
There are several limitations in this systematic CPG review. Our search was limited to guidelines published in English. We excluded guidelines that specifically focused on populations with other primary health conditions (i.e., cancer, diabetes). We also excluded CPGs that were not national in scope. We do not believe, however, that publication bias is an issue for CPGs whose aim is to be widely disseminated and adopted.
Additionally, the operational definition of CPGs adopted in the current systematic review excludes treatment algorithms, which aim to provide guidance with regard to treatment strategies, methods of implementation, and treatment steps. 99 Algorithms are often included in CPGs but in isolation do not constitute a guideline. Nevertheless, their use in clinical practice may be as relevant as the use of CPGs. 100 Future CPGs may wish to develop and incorporate algorithms within the guidelines that are evidence based or at the least identify that they represent best practices.
Conclusions and Future Recommendations
This review assessed CPGs from 2004 to 2014 for treating adults with depression (including dysthymia, subthreshold/minor depression, and MDD), with a focus on recommendations following failed response to first-line antidepressant pharmacotherapy. While there are many first-line treatment strategies for patients with depressive disorders, there is, in comparison, a paucity of information regarding the best approaches to adopt when that first-line treatment is inadequate. Given that approximately half of treated patients will require more than 1 treatment to achieve remission, better information regarding optimal second-line approaches is critical for reducing the burden of illness associated with this condition.
Consistent with previous studies, 39 –41 assessment of the CPGs using the AGREE II instrument revealed deficiencies in the domains of stakeholder involvement, rigor of development, and editorial independence. The evidence on which the guidelines are based is problematic with respect to the sufficiency of the evidence, its ecological validity, and its balanced representation in the guidelines.
Groups that wish to develop CPGs for depressive disorders might consider several factors in the future. First, a clear definition of inadequate response is required. Standardized methods for establishing adequacy of response (i.e., cutoff values using specific depression scales) in real-world settings should be included. Second, the representation of various stakeholders (including patients and payers) in the CPG development process should be prioritized in the future. Third, greater clarity with regard to the recommended clinical actions following a failed treatment response is critical. These recommended actions should emerge directly from the best available evidence. When existing evidence is lacking, CPGs should indicate that the evidence for a specific recommendation is insufficient. Finally, the impact of contextual factors on the applicability and feasibility of the CPG, such as practice setting (inpatient, outpatient) and type of clinician (e.g., primary care practitioner, psychiatrist), should also be highlighted.
Footnotes
Author Note
The authors are solely responsible for the content of the review. The opinions expressed herein do not necessarily reflect the opinions of the Agency for Healthcare Research and Quality. Parminder Raina holds a Tier 1 Canada Research Chair in Geroscience and the Raymond and Margaret Labarge Chair in Research and Knowledge Application for Optimal Aging.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original systematic review was funded by the Agency for Healthcare Research and Quality, United States Department of Health and Human Services (HHSA 290 2007 10060 I). The AHRQ provided peer review and approval of the final report for the original review.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.