
Abstract
Objective:
Small clinical samples suggest that psychiatric inpatients report a lifetime history of interpersonal trauma. Since past experiences of trauma may complicate prognosis and treatment trajectories, population-level knowledge is needed about its prevalence and correlates among inpatients.
Methods:
Using health-administrative databases comprising all adult psychiatric inpatients in Ontario, Canada (2009 to 2016, n = 160,436, 49% women), we identified those who reported experiencing physical, sexual, and/or emotional trauma in their lifetime, 1 year, and 30 days preceding admission. We described the prevalence of each type of trauma, comparing women and men using modified Poisson regression, and identified individual-level characteristics associated with lifetime trauma history using multivariable logistic regression.
Results:
31.7% of inpatients reported experiencing trauma prior to admission. Lifetime prevalence was higher in women (39.6% vs. 24.1%; age-adjusted prevalence ratio [aPR] = 1.68; 95% CI, 1.65 to 1.71), including sexual (22.7% vs. 8.4%; aPR = 2.81; 95% CI, 2.73 to 2.89), emotional (33.3% vs. 19.4%; aPR = 1.76; 95% CI, 1.72 to 1.79), and physical trauma (24.2% vs. 14.8%; aPR = 1.68; 95% CI, 1.65 to 1.72). Factors most prominently associated with lifetime trauma were witnessing parental substance use (adjusted odds ratio [aOR] = 8.68; 95% CI, 8.39 to 8.99), female sex (aOR = 2.29; 95% CI, 2.23 to 2.35), and number of recent stressful life events (aOR = 1.62; 95% CI, 1.59 to 1.65).
Conclusions:
These results suggest that trauma-informed approaches are essential to consider in the design and delivery of inpatient psychiatric services for both women and men.
Introduction
Close to one in three individuals affected by mental illness—women more so than men—report having experienced interpersonal trauma of a sexual, physical, or emotional nature. 1 –3 Trauma is at least 2 to 3 times more common among individuals with mental illness than among those without. 1 In those with severe mental illness, including schizophrenia; trauma is even more common, with prevalence estimates approaching 37% for sexual and 47% for physical trauma. 4,5 While symptoms of trauma and stressor-related disorders such as post-traumatic stress disorder (PTSD) require treatment in and of themselves; interpersonal trauma, even in the absence of these conditions, can negatively affect mental illness treatment trajectories. 6 –8 A history of interpersonal trauma is associated with impaired engagement with clinical providers, 9 higher likelihood of substance use relapse, 10 and lower antidepressant response rates. 8 As such, recognition of trauma exposure and a trauma-informed approach to care are key to effective mental health and addictions (MHA) care. 11
Psychiatric inpatient units are where individuals with the most severe and complex mental illnesses receive treatment. Since interpersonal trauma can strongly impact mental illness presentations and treatment trajectories, it is important to consider it in the context of inpatient services. An inpatient population is only a subset of individuals with mental illness. Because it represents a subsample of individuals with considerable severity of illness, knowledge about the rates of, and factors associated with, trauma exposure in this group could optimize delivery of interventions. Research in small clinical inpatient samples, mostly in individuals diagnosed with substance use disorders 6,10,12 and major depression, 13 suggests that lifetime interpersonal trauma rates could be as high as 40% and reaching 70% in women. 9 Few studies have documented the timing of the trauma (i.e., recent vs. lifetime) or the type of trauma (i.e., sexual, physical, and emotional), which could inform care delivery for specific clinical presentations in inpatients. 12,14,15 Even fewer studies have examined differences in the nature and prevalence of trauma between men and women. 9,10,13,16 Further, there is limited information about other potential correlates of trauma in this population, including sociodemographic and psychosocial (e.g., homelessness and socioeconomic status), psychiatric and medical history, and/or clinical presentation factors. 17,18 Better characterization of the extent to which interpersonal trauma has occurred in the lives of men and women requiring psychiatric hospitalization would help with service planning and delivery.
In a large population-based sample of adult psychiatric inpatients in Ontario, Canada’s most populous province (approximately 13.5 million population), we examined the prevalence of sexual, physical, and emotional interpersonal trauma (lifetime, past year, and past month) among men and women. We expected that prevalence estimates would be similar to or higher than those observed in non-inpatient populations and that while there would be a greater burden of trauma among women, exposure would be high in men as well. To contextualize our findings, we examined the correlates of lifetime trauma history in the sample and hypothesized that associated factors would include indicators of sociodemographic marginalization and of medical and psychiatric complexity.
Methods
Study Design and Data Sources
This population-based, cross-sectional study used routinely collected health-administrative information. The Registered Person’s Database (RPDB), the central population registry file, which enables linkage across population-based health-administrative data sets, was used to identify age, sex, and residential postal code. Psychiatric hospitalization data were obtained via the Ontario Mental Health Reporting System (OMHRS), which contains detailed sociodemographic and clinical information for all adults admitted to designated psychiatric beds in Ontario. 19 Other datasets were used to identify past medical and psychiatric history including the Canadian Institute for Health Information’s Discharge Abstract Database (CIHI-DAD) for medical hospitalizations, the National Ambulatory Care Reporting System (NACRS) for emergency department visits, and the Ontario Health Insurance Plan (OHIP) for physician billing (Supplemental Table S1). Datasets were linked using unique encoded identifiers and analyzed at ICES.
Study Population
We considered all Ontario residents aged 18 to 105 years who were admitted to designated psychiatric inpatient beds between April 1, 2009, and March 31, 2016. Since multiple hospitalizations per person could be potential index events within the study period, we selected an eligible hospitalization at random. We excluded individuals residing outside of Ontario because their data could not be linked across datasets. Forensic patients were also excluded, as they represent a qualitatively different population. To attain complete data on the entire cohort, we further excluded inpatients with a missing discharge date or without diagnostic information.
Interpersonal Trauma Exposure
Information on interpersonal trauma experiences prior to the index inpatient admission was extracted from the Resident Assessment Instrument for Mental Health (RAI-MH), a comprehensive, standardized instrument with demonstrated reliability, 20,21 contained in the OMHRS dataset. 19 For all inpatients in designated psychiatric beds in Ontario, the RAI-MH is routinely completed by a member of the clinical team on admission, discharge, and every 3 months during the hospitalization. Several interpersonal trauma-related items are queried on the MH-RAI during the admission assessment. Patients are specifically asked whether they had experienced each of physical abuse or assault, sexual abuse or assault, or emotional abuse in their lifetime. If patients answer yes to the lifetime question, they are additionally queried about whether they had experienced interpersonal trauma at any time in the 1 year prior to hospitalization, including within the 30 days prior to hospitalization. For a detailed description of interpersonal trauma questions in the clinical assessment, see Supplemental Table S2. We examined each type of trauma separately as well as combinations of trauma types. 22,23
Analysis of Prevalence
We calculated the prevalence of lifetime interpersonal trauma exposure for trauma overall, each specific type (sexual, physical, and emotional), more than one type, and all three types of trauma. We compared the prevalence in women versus men using modified Poisson regressions with robust standard errors, generating age-adjusted prevalence ratios (aPR) with 95% confidence intervals (CI). With a relatively common outcome, the prevalence ratio is the most preferred and interpretable relative estimate. 24 We stratified the analysis for lifetime trauma exposure by the primary psychiatric diagnosis. Analyses were repeated for past 1-year and 30-day trauma exposure.
Analysis of Correlates
To contextualize our prevalence findings, we thematically organized potential correlates into three broad categories: sociodemographics; medical history; and clinical presentation on the index admission. Social and demographic variables included age, neighborhood income quintile, rural dwelling (RPDB), education level, marital status, accommodation, and income source (OMHRS). Using the RAI-MH, we also ascertained whether patients reported any lifetime history of witnessing parental alcohol or substance abuse, and the number of stressful life events reported 30 days prior to admission (OMHRS). Medical history variables included the number of medical comorbidities, identified using the Johns Hopkins Adjusted Clinical Groups® System (V10.0), 25 where individuals were assigned up to 29 aggregated diagnostic groups (ADGs) characterizing medical conditions based on health service use in the preceding 2 years (psychosocial conditions were excluded for this analysis), medical or MHA-related hospital admissions, emergency department visits, or outpatient physician visits to a psychiatrist or a primary care provider within the preceding 2 years (DAD, OMHRS, NACRS, and OHIP). Index admission characteristics included the primary discharge diagnosis using the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, information on the acuity of the hospitalization (e.g., concerns about harm to self; others; or inability to care for self, not mutually exclusive) and whether the admission was involuntary according to the Ontario Mental Health Act (OMHRS). 19,22
We described potential correlates overall and for women and men separately. We used standardized differences to illustrate the magnitude of sex-differences on covariates, which are preferable to use of P values for large data sets since they are independent of sample size. 26 A standardized difference of >0.10 is considered a clinically important difference. 27 Multivariable logistic regression models were then constructed to identify correlates independently associated with lifetime interpersonal trauma exposure, as they are most widely used for binary outcomes and are robust for handling sequential modeling procedures. 28,29 First, we examined covariates associated with interpersonal trauma exposure in bivariate models for women and men separately. If we observed similar effects across sex-specific strata, we planned to produce an overall multivariable model with sex as a covariate. Second, for each thematic block, we used the bivariate models to select nonredundant variables in order to minimize collinearity. Third, to create the multivariable model, we used a split sample (derivation and validation) method with sequential addition of variables in thematic blocks, starting with sociodemographics, then past history variables, and then characteristics of the inpatient admission. 30 Within each block, variables were added sequentially, with log likelihood (LL) tests used to determine whether adding/removing covariates improves model fit, compared to a simpler model. Once a variable was dropped, the effect of omitting or re-adding each of the remaining variables was examined; if a variable significantly changed the LL estimate (P < 0.05), it was retained. This process was repeated until no change was observed. Discrimination was assessed using the c-statistic. Statistical analyses were conducted using SAS statistical software (version 9.4). The use of data in this project was authorized under Section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Results
Cohort Description
Of 328,027 psychiatric hospitalization records, we excluded 272 due to data errors, 399 in non-Ontario residents, 7,350 in individuals aged <18 or >105 years, 4,129 without a discharge date or diagnostic information, and 8,001 in forensic patients. From the remaining 307,876 records (93.8%), all patients with only one admission were included; and one admission per person was randomly selected in individuals with multiple admissions, resulting in a cohort of 160,436 unique patients: 78,386 (48.9%) women and 82,050 (51.1%) men. Characteristics of the inpatients, broken down by sex, are presented in Table 1. The average age of inpatients was 42.0 (SD = 16.9). Most (89.9%) lived in urban regions, about one-third (28.1%) lived in the lowest-income neighborhoods, and 25.3% were employed. Almost half (45.9%) of all inpatients were never married, and about 14.5% reported having witnessed parental substance abuse in their lifetime. In the 2 years prior to the index hospitalization, 54.5% had an MHA-related emergency department visit, and 26.8% had been hospitalized for a psychiatric reason. At index hospitalization, about two thirds of inpatients were admitted involuntarily (65.4%), and a large proportion were admitted with concerns about self-harm (53.4%).
Characteristics of 160,436 Psychiatric Inpatients, Presented as N (%), Unless Otherwise Specified.
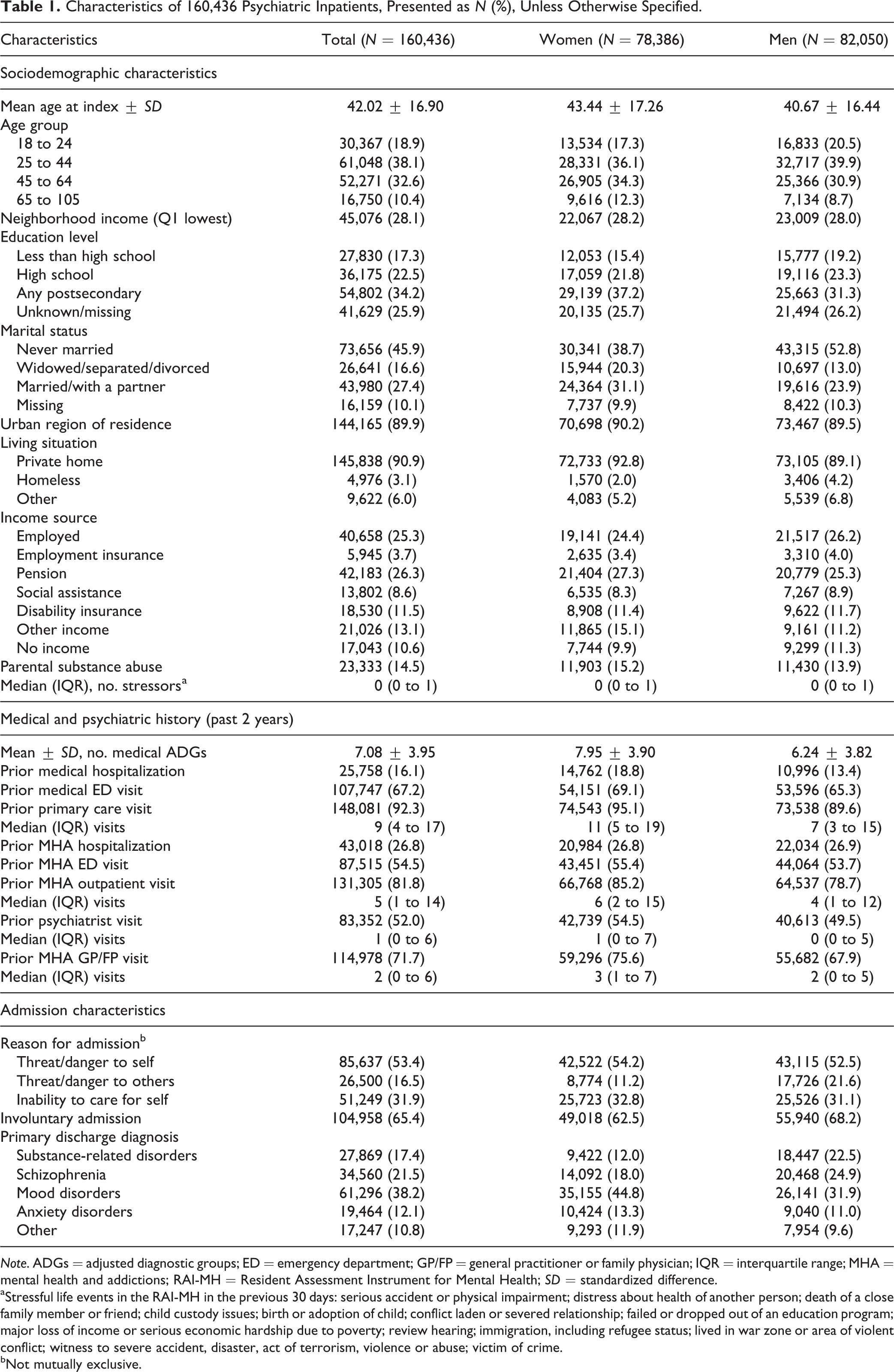
Note. ADGs = adjusted diagnostic groups; ED = emergency department; GP/FP = general practitioner or family physician; IQR = interquartile range; MHA = mental health and addictions; RAI-MH = Resident Assessment Instrument for Mental Health; SD = standardized difference.
aStressful life events in the RAI-MH in the previous 30 days: serious accident or physical impairment; distress about health of another person; death of a close family member or friend; child custody issues; birth or adoption of child; conflict laden or severed relationship; failed or dropped out of an education program; major loss of income or serious economic hardship due to poverty; review hearing; immigration, including refugee status; lived in war zone or area of violent conflict; witness to severe accident, disaster, act of terrorism, violence or abuse; victim of crime.
bNot mutually exclusive.
Interpersonal Trauma Prevalence
About 31.7% of inpatients (n = 50,832) reported experiencing lifetime interpersonal trauma, including physical (n = 31,111; 19.4%), sexual (n = 24,654; 15.4%), and emotional (n = 42,046; 26.2%). Lifetime history of trauma was significantly more common in women than in men (39.6% vs. 24.1%; aPR = 1.68; 95% CI, 1.65 to 1.71), with the largest relative difference for sexual trauma (aPR = 2.81; 95% CI, 2.73 to 2.89; Table 2). About 14.5% of women reported experiencing a lifetime history of all three types of trauma compared to 5.0% of men (aPR = 2.99; 95% CI, 2.89 to 3.10). Lifetime history of trauma was most common in those with substance use disorders and anxiety disorders and was more common in women than in men across all diagnoses (Figure 1; for additional detail, see Supplemental Table S3). Overall, and for each type of trauma, recent experiences (i.e., 1 year and 30 days prior to admission) were more commonly reported by women, in particular for sexual trauma in the 30 days preceding admission (aPR = 6.73; 95% CI, 5.45 to 8.32; Table 2).
Prevalence and aPR and 95% CI Comparing Women and Men Inpatients on Lifetime, Past-Year, and Past-Month Interpersonal Trauma.
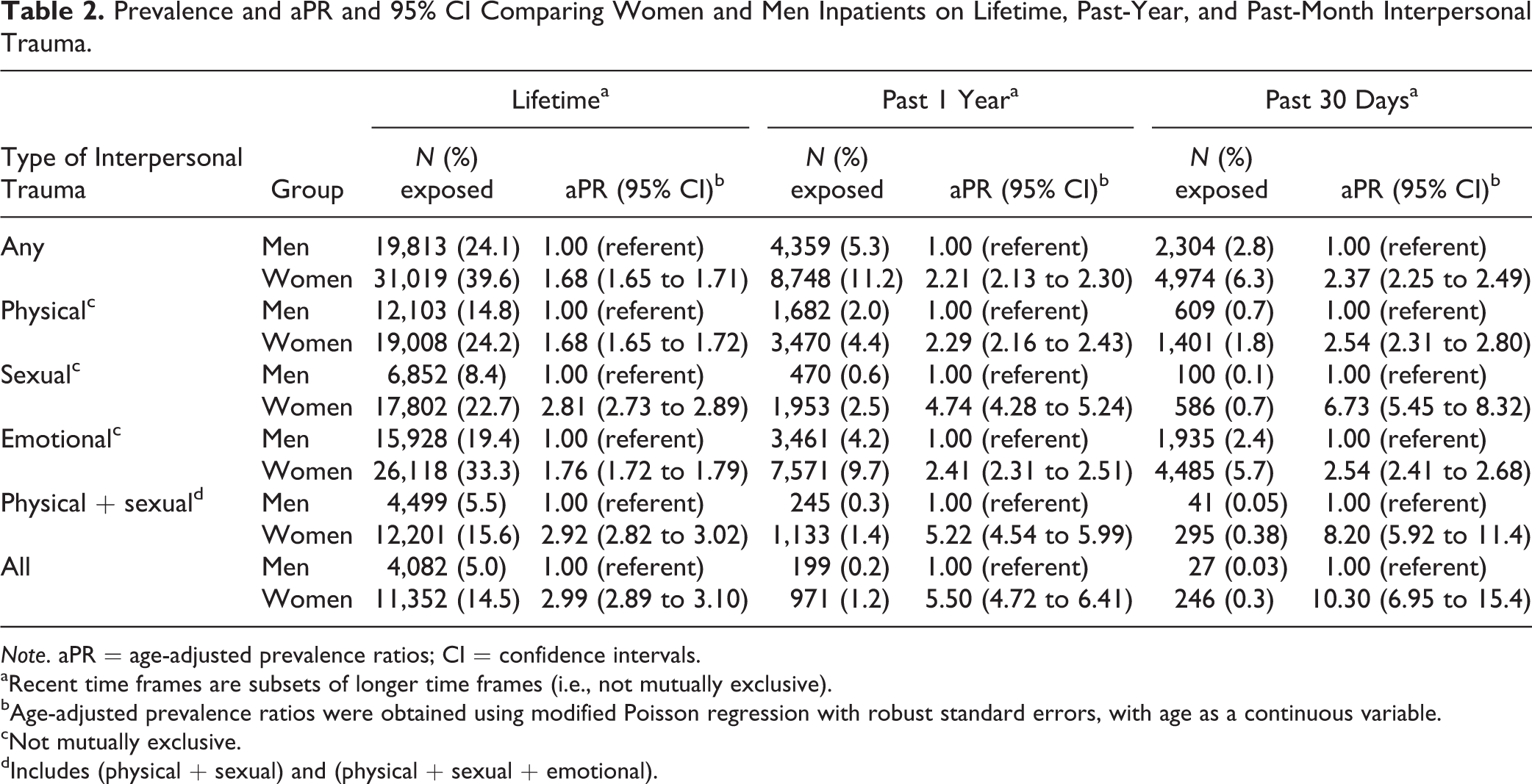
Note. aPR = age-adjusted prevalence ratios; CI = confidence intervals.
aRecent time frames are subsets of longer time frames (i.e., not mutually exclusive).
bAge-adjusted prevalence ratios were obtained using modified Poisson regression with robust standard errors, with age as a continuous variable.
cNot mutually exclusive.
dIncludes (physical + sexual) and (physical + sexual + emotional).
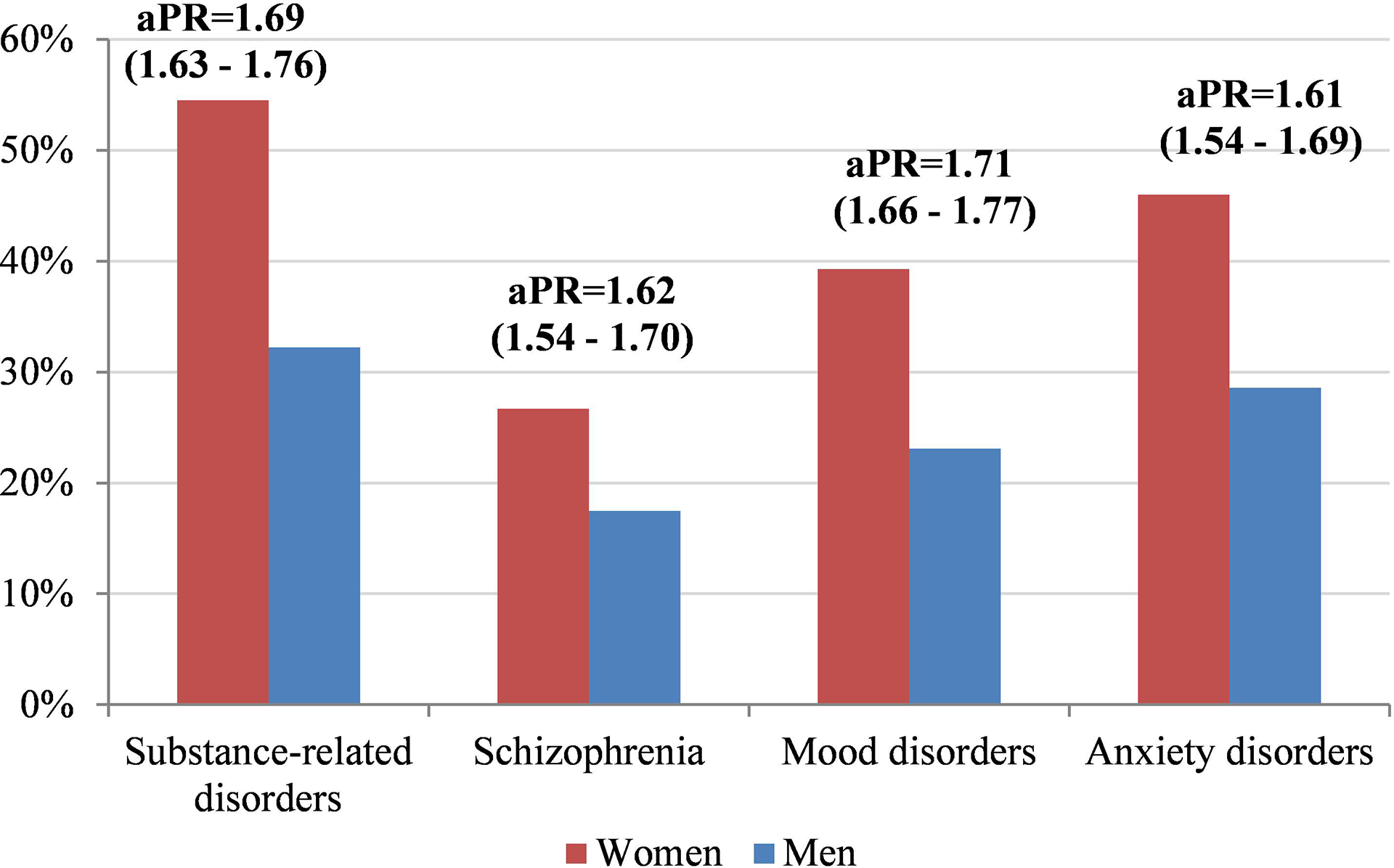
Any lifetime interpersonal trauma in men and women inpatients, shown in percentage of each sex, with age-adjusted prevalence ratio (aPR) and 95% confidence intervals, by diagnostic category. For diagnostic category definitions, refer to Supplemental Table S1. For single and multiple types of lifetime interpersonal trauma, stratified by diagnostic category, refer to Supplemental Table S2.
Interpersonal Trauma Correlates
In bivariate analyses, multiple covariates were associated with reporting experiences of interpersonal trauma any time prior to hospitalization, with minor differences in terms of which variables were significant for women and for men (Table 3). Sex-specific multivariable models were also similar, suggesting no major interactions with sex (Supplemental Table S4). Therefore, we generated an overall multivariable logistic model including sex as a covariate (Table 4), where interpersonal trauma history was positively associated with multiple sociodemographic characteristics (being a woman, younger, non-married, of low socioeconomic status, living in a rural area, and being homeless) and with having experienced more stressful life events 30 days prior to admission. The strongest risk factor in the model was having witnessed parental substance abuse (OR = 8.68; 95% CI, 8.39 to 8.99). Trauma history was associated with several health service use characteristics (having a prior medical emergency department visit, a psychiatric hospitalization, or an MHA-related outpatient visit). It was also positively associated with diagnoses of substance use disorders, anxiety disorders, and suicidality and negatively associated with being assessed as a threat to others or unable to care for self. The final multivariable model yielded a c-statistic of 0.769.
Characteristics of Psychiatric Inpatients Exposed and Unexposed to a Lifetime Experience of Any Interpersonal Trauma Considered for the Multivariable Models of Interpersonal Trauma Correlates; Presented as N (%), Unless Otherwise Specified, with SD Comparing Exposed and Unexposed Individuals.
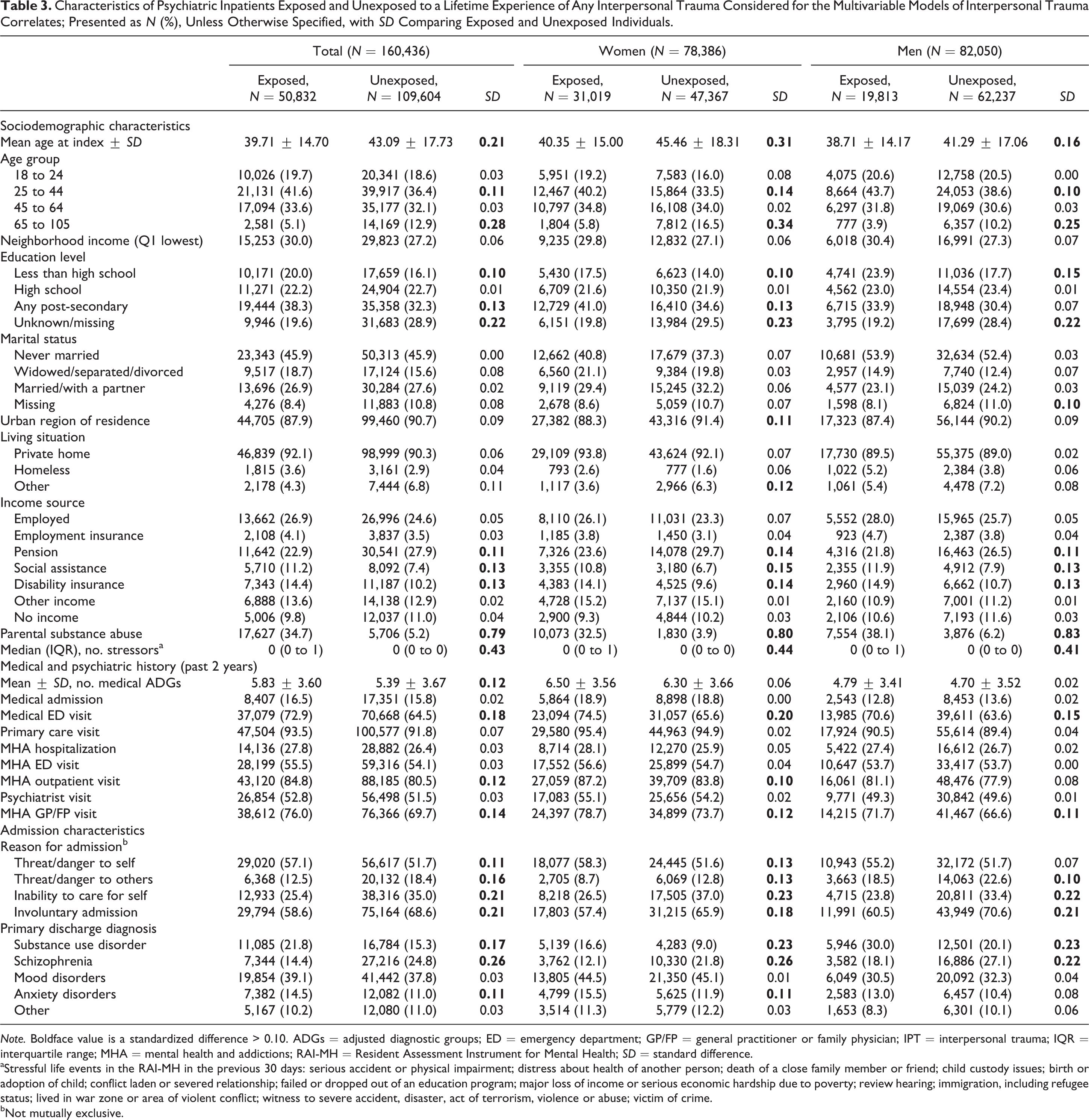
Note. Boldface value is a standardized difference > 0.10. ADGs = adjusted diagnostic groups; ED = emergency department; GP/FP = general practitioner or family physician; IPT = interpersonal trauma; IQR = interquartile range; MHA = mental health and addictions; RAI-MH = Resident Assessment Instrument for Mental Health; SD = standard difference.
aStressful life events in the RAI-MH in the previous 30 days: serious accident or physical impairment; distress about health of another person; death of a close family member or friend; child custody issues; birth or adoption of child; conflict laden or severed relationship; failed or dropped out of an education program; major loss of income or serious economic hardship due to poverty; review hearing; immigration, including refugee status; lived in war zone or area of violent conflict; witness to severe accident, disaster, act of terrorism, violence or abuse; victim of crime.
bNot mutually exclusive.
Multivariable Logistic Regression model of Covariates Independently Associated with Lifetime Interpersonal Trauma Exposure.
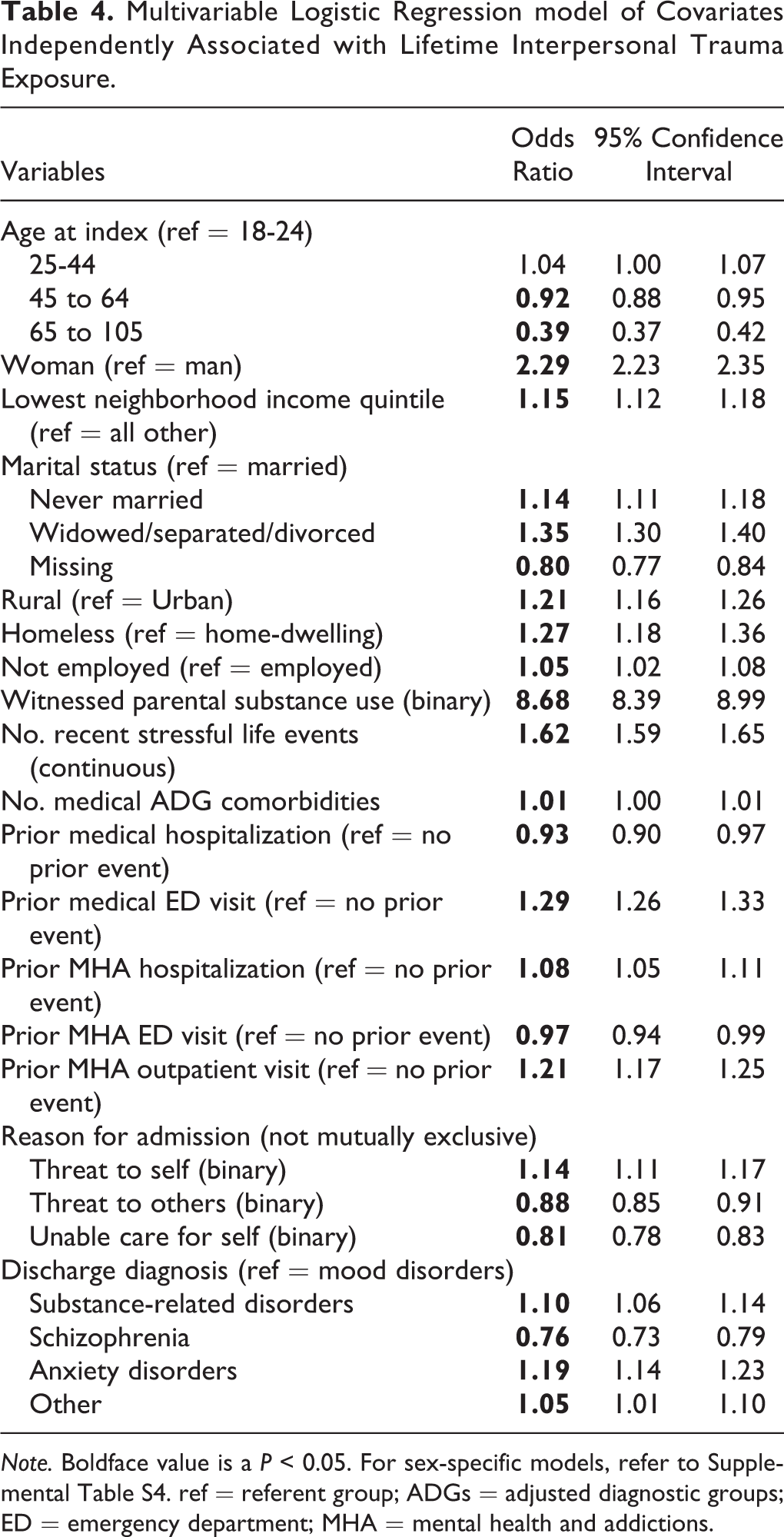
Note. Boldface value is a P < 0.05. For sex-specific models, refer to Supplemental Table S4. ref = referent group; ADGs = adjusted diagnostic groups; ED = emergency department; MHA = mental health and addictions.
Discussion
Summary of Findings
In this population-based study of adult psychiatric inpatients in Ontario, Canada, almost one in three individuals reported prior experiences of interpersonal trauma. Women were more likely to have experienced trauma than men but prevalence was high for both groups (40% and 24%, respectively). For recent experiences (i.e., within the 30 days preceding admission), gender differences were most pronounced for sexual trauma. Multiple variables were independently associated with trauma history in both men and women, including markers of significant vulnerability such as low socioeconomic status, stressful life events proximal to the admission, and high health service utilization. Together, these findings suggest that trauma is highly prevalent, and therefore must be part of the clinical assessment to ensure optimal inpatient and postdischarge outcomes.
Interpretation
Our prevalence estimate for lifetime trauma history among psychiatric inpatients (32%) is lower than what has been observed in individuals with mental illness and addictions more broadly. 1,4,31,32 However, our results may not be comparable to studies that utilized self-report surveys that may not have been as susceptible to under-reporting. 31 Specifically within inpatient populations, our estimate is also slightly lower than those observed in small clinical samples (44% to 61%). 6,9,12,14,16,33 However, these studies were mainly conducted in individuals with substance-related disorders, whose rates were some of the highest in our sample (55% for women and 32% for men). Moreover, high rates of interpersonal trauma have been shown in forensic patients. 15 Their exclusion from our sample, as they represent a qualitatively different patient population, may have lowered the prevalence estimates we observed. The observation that physical abuse was more common than sexual abuse is consistent with estimates from the general population 2,34,35 and some clinical samples. 4,9,12 Most studies in inpatient populations have also found higher reported rates of trauma in women than in men, 6,9,12,14 as we observed, though most show a more modest gender split. While only a handful of prior studies disaggregated different types of trauma by sex in psychiatric inpatients, our findings are consistent with these showing that each of sexual, physical, emotional, 14 and multiple types of trauma 9,14 were more common in women.
Many characteristics we identified as being associated with interpersonal trauma exposure have been documented as such outside the inpatient setting. For example, a recent systematic review showed that low socioeconomic status, homelessness, and high mental health service utilization were associated with PTSD. 17,18 For psychiatric inpatients, the few available studies are consistent with our findings with regard to both the magnitude and nature of associations, highlighting that those with a history of abuse are less likely to be admitted involuntarily 9 but more likely to have a family history of alcoholism, 14 deliberate self-harm, or suicide attempts 12 –14,16 ; to have a diagnosis of anxiety (in women) 12,14 ; and more prior medical and psychiatric service utilization. 6,16
Longitudinal research suggests a causal relationship between trauma exposure and the development of mental illness. 36 However, the prevalence estimates we observed in inpatients approximate general estimates in individuals with mental illness. 37 So, it is not necessarily the case that those with a history of trauma are more likely to require psychiatric admission. Higher relative rates of trauma in women, compared to men, have also been frequently observed. 9,38 While only about 5% of inpatients reported recent trauma, women were more than twice as likely as men to report trauma of some kind in the month preceding admission—and more than 6 times as likely to report recent sexual trauma. Since recent abuse may exacerbate existing mental illness, 39 trauma experiences may be a precipitating factor for psychiatric hospitalizations in women more than previously recognized.
The multivariable models in this study aimed to identify associations with interpersonal trauma, rather than causally related variables, in order to provide context to our prevalence estimates. It is unclear whether the effect of age is a true association, or whether it reflects potential underreporting by older adults, due to age-cohort differences in the use of language, conceptual understanding of experiences, or cognitive limitations. 37,40 The effects of marital and socioeconomic status may be bi-directional, with victims of interpersonal trauma more likely to become homeless and unemployed as a result of fewer social supports, or an unstable living environment increasing exposure to trauma. 18 The effect of additional life stressors as well as parental substance use is unsurprising, 17 with some authors suggesting that abuse in the context of parental alcoholism may play a role in the development of substance-related disorders. 14 The positive associations with anxiety (including PTSD) and substance-related disorders, as well as with self-harm, are logical in the context of what is known about the complex sequela of trauma. A recent systematic review, for example, showed that childhood trauma was among the most prominent predictors of nonsuicidal self-injury across a variety of psychiatric conditions. 41
Strengths and Limitations
To our knowledge, this is the largest population-based study to examine the prevalence of interpersonal trauma history in psychiatric inpatients. Since the RAI-MH routinely collects information on interpersonal trauma in all designated psychiatric beds in Ontario, 22,23 we were able to examine multiple types and multiple time frames of interpersonal trauma and to disaggregate the findings by sex. Moreover, a multitude of sociodemographic and clinical characteristics helped contextualize our findings and together were able to discriminate well between those with and without a history of experiencing interpersonal trauma (c-statistic close to 80%).
This study was conducted in a subsample of inpatients, who are a high-severity group, and so the findings were not intended to generalize to the broader population of individuals experiencing mental illness and addictions. Even within the sample, however, measures of trauma history may be subject to underreporting. On a psychiatric inpatient unit, there may not be sufficient time to establish the type of trust to enable a patient to disclose a trauma history. There could also be underreporting by sex (e.g., due to stigma surrounding sexual abuse in men) 42 or by age, as discussed previously. A recent review also found evidence of abuse occurring in inpatient units 5 ; while another found that some recipients of psychiatric care report their disclosures not being taken seriously by clinical staff, 43 suggesting that trauma history may not be properly reported or recorded in a clinical setting. Due to the way questions about interpersonal trauma exposure were asked in the RAI-MH, we could not determine the timing of the first exposure to interpersonal trauma (i.e., whether there was childhood trauma exposure) nor the severity or chronicity of the trauma. However, we did have a measure of whether trauma exposure was recent. Further, the cross-sectional nature of this study presented a profile of psychiatric inpatients with a history of interpersonal trauma, which precluded making causal statements. Future studies will aim to examine the functioning and symptomology, and discharge disposition in inpatients who have experienced interpersonal trauma, as well as long-term outcomes and treatment trajectories post-discharge.
Conclusions
This study highlights a need to consider individuals’ history of interpersonal trauma exposure in the psychiatric inpatient setting. A small minority of inpatients, particularly women, report interpersonal trauma exposure quite proximal to the inpatient admission. This suggests that initiation of trauma-focused interventions might be warranted on the inpatient unit in some cases and necessitates discussion about ensuring that capacity for delivery of such interventions is available therein. However, it is not likely to be feasible nor necessary for every patient to engage in specialized trauma therapy on the inpatient unit. Instead, the high reported rates of lifetime trauma exposure for both men and women inpatients point to a need for a systematic trauma-informed approach to care, as distinct from trauma-specific interventions. 11 Trauma-informed approaches realize the widespread impact of trauma, recognize its signs and symptoms, and promote recovery and resilience while resisting retraumatization. 11,44 On an inpatient unit, and especially in the case of an involuntary hospitalization, there is a large potential for retraumatization. 45 Minimizing the use of restraints, ensuring practices that seek to correct power imbalances that disadvantage vulnerable groups, increased attention to the therapeutic relationship and boundaries, and inclusion of patient advisors who have trauma experience is warranted. 45
In summary, this study highlights the high prevalence of both lifetime and recent interpersonal trauma in men and women psychiatric inpatients, as well as the social and clinical complexities that need to be addressed in this vulnerable population. The results support action toward incorporating a trauma-informed approach to care for all inpatients to improve response to treatment, optimize transition back to the community postdischarge, and improve well-being and quality of life. Future research can explore the correlates of specific types of trauma exposure, as well as outcomes both during the inpatient stay and in the time after discharge from hospital.
Supplemental Material
Supplemental Material, 07_Epidemiology_of_Interpersonal_Trauma_Supplements_2019-02-06 - Epidemiology of Interpersonal Trauma among Women and Men Psychiatric Inpatients: A Population-Based Study: Épidémiologie du traumatisme interpersonnel chez des femmes et des hommes hospitalisés en psychiatrie : une étude dans la population
Supplemental Material, 07_Epidemiology_of_Interpersonal_Trauma_Supplements_2019-02-06 for Epidemiology of Interpersonal Trauma among Women and Men Psychiatric Inpatients: A Population-Based Study: Épidémiologie du traumatisme interpersonnel chez des femmes et des hommes hospitalisés en psychiatrie : une étude dans la population by Evgenia Gatov, Nicole Koziel, Paul Kurdyak, Natasha R. Saunders, Maria Chiu, Michael Lebenbaum, Simon Chen and Simone N. Vigod in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We thank Kinwah Fung, MSc (ICES, Toronto, ON, Canada), for her contributions to methodological oversight. We thank the Ontario Ministry of Health and Long-Term Care (MOHLTC) for their data. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the authors and not necessarily those of CIHI.
Data Access
The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the programs may rely upon coding templates or macros that are unique to ICES.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the ICES, which is funded by an annual grant from the MOHLTC. It was also supported by the Mental Health and Addictions Scorecard and Evaluation Framework grant from the MOHLTC (04601A14-19). The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Dr Vigod is supported by Women’s College Hospital, the University Of Toronto Department Of Psychiatry and by a New Investigator Award from the Canadian Institutes for Health Research. Dr Kurdyak received operational grant funding from the MOHLTC Health Services Research Fund Capacity Award and is supported in part by the Medical Psychiatry Alliance, a collaborative health partnership of the University of Toronto, the Centre for Addiction and Mental Health, the Hospital for Sick Children, Trillium Health Partners, the MOHLTC, and an anonymous donor. Michael Lebenbaum is supported by a Vanier Canadian Graduate Scholarship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.