
Abstract
Objectives:
To present the 6-month prevalence and sociodemographic correlates of mental disorders and mental health–related service contacts in a sample of children (4 to 11 years) and youth (12 to 17 years) in Ontario.
Methods:
The 2014 Ontario Child Health Study is a provincially representative survey of 6537 families with children aged 4 to 17 years in Ontario. DSM-IV-TR mental disorders were assessed using the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) and included mood (major depressive episode), anxiety (generalized anxiety, separation anxiety, social phobia, specific phobia), and behaviour disorders (attention-deficit/hyperactivity disorder, oppositional-defiant disorder, conduct disorder).The MINI-KID was administered independently to the primary caregiver and youth aged 12 to 17 years in the family’s home.
Results:
Past 6-month prevalence of any mental disorder ranged from 18.2% to 21.8% depending on age and informant. Behaviour disorders were the most common among children, and anxiety disorders were the most common among youth. Among children and youth with a parent-identified mental disorder, 25.6% of children and 33.7% of youth had contact with a mental health provider. However, 60% had contact with one or more of the providers or service settings assessed, most often through schools.
Conclusions:
Between 18% and 22% of children and youth in Ontario met criteria for a mental disorder but less than one-third had contact with a mental health provider. These findings provide support for strengthening prevention and early intervention efforts and enhancing service capacity to meet the mental health needs of children and youth in Ontario.
Introduction
Epidemiological studies of mental disorders among children and youth provide evidence on the level of disorder in the general population, its geographic distribution, and sociodemographic correlates and rates of mental health–related service contacts. This evidence can inform policy and program priorities for allocating resources to: children most at risk for experiencing mental disorder and/or service gaps, geographic areas, and service providers responsible for addressing mental health need in the community. In Canada, epidemiological studies explicitly designed to generate evidence on the prevalence and correlates of child and youth mental disorders and service contacts in the general population are limited to the 1983 Ontario Child Health Study (OCHS) 1 and 2 Quebec surveys conducted in the 1990s. 2,3 The 2014 OCHS—a sequel to the 1983 OCHS—was designed to address current evidence gaps.
A review of surveys conducted in populations comparable to Canadian children and youth 4 estimated the pooled prevalence of 1 or more mental disorders to be 14.3%, similar in magnitude to the worldwide estimate of 13.4% reported in a meta-analysis of 41 prevalence studies. 5 Important patterns in the distribution of child and youth mental disorders have also been documented. For example, disruptive behaviour disorders and attention-deficit/hyperactivity disorder are more common among boys compared to girls, while mood and anxiety disorders are more common among adolescent girls. 1,2,4,6,7 Consistent differences in prevalence by family socioeconomic circumstances and composition, immigrant background, and urbanicity have also been documented. 1,6,8 –13 The 1983 OCHS reported higher prevalence of disorder among children and youth living in urban versus rural areas, 1 lone- versus 2-parent families, 13 and households with low versus middle and high income. 11 In contrast, the 1983 OCHS reported similar prevalence of mental disorder between immigrant (i.e., foreign-born) and nonimmigrant (i.e., Canadian-born) children and youth. 14 Subsequent studies, however, in the United States 9,10 and Canada, 8 have consistently documented lower levels of mental disorder among children and youth from immigrant backgrounds.
Population-level evidence on the association between child and youth mental disorder and use of mental health services is very limited in Canada. The 1983 OCHS estimated that only 1 in 6 children and youth with a mental disorder received mental health or social services in the 6 months preceding the study. 1 Higher maternal education was positively associated with accessing mental health and social services, 15 while immigrant background was negatively associated. 14 Evidence from population-based studies in the United States consistently reveals underutilization of mental health services among females compared to males, younger children compared to adolescents, and those from ethnic minority and immigrant backgrounds. 10,12,16 –19 In contrast, living with 1 or no biological parent, compared to 2, has been positively associated with mental health service use. 16,20 Studies examining other socioeconomic and demographic correlates of service use, such as family poverty, parental education, and urbanicity, have been less consistent and generally reveal few or no differences. 1,16 –18,20,21 Data from the United States also indicate that school and speciality mental health settings are the most common sectors providing child mental health services, followed by general medical settings. 18,22 Admittedly, the unique demographic composition of Canadian society and its health care system raise questions about the applicability of health services research findings from the United States to the Canadian context.
The objectives of this study were to present the 6-month prevalence estimates and sociodemographic correlates of mental disorders and mental health–related service contacts among children (4 to 11 years) and youth (12 to 17 years) in Ontario.
Methods
The 2014 OCHS is a province-wide, cross-sectional, epidemiologic study of child and youth health and mental disorder. A probability sample of 6537 households (50.8% response) with 10,802 children aged 4 to 17 years participated. The sampling frame was the 2014 Canadian Child Tax Benefit file. Households were selected based on a 3-stage survey design that involved cluster sampling of residential areas and stratification by residency (urban, rural) and income (areas and households cross-classified by 3 levels of income: <20th, 20th to 80th, and >80th percentiles). In families with 2 or more eligible children, 1 was selected randomly to serve as the “selected child” (SC) for all assessments, and up to 3 remaining children 4 to 17 years old in the household were included in a subset of assessments. Data were collected in the home by trained Statistics Canada interviewers from the person most knowledgeable about all children (98.6% identified as parent of SC and therefore hereafter referred to as parent) and from youth aged 12 to 17 years. Data collection occurred from October 2014 to October 2015. Detailed accounts of the survey design, content, training, and data collection are available elsewhere. 23,24
Measures
Diagnostic interview
A modified version of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), a fully structured diagnostic interview, was administered by trained lay interviewers to the parent about the SC (MINI-KID-P) and separately to youth (12 to 17 years) (MINI-KID). 25,26 Modifications included: 1) the selection of a subset of the most commonly occurring mental disorders in children and youth; 2) an exclusive focus on past 6-month occurrence for all assessed disorders, with the exception of conduct disorder, which was assessed for the past 12 months, with at least 1 criterion present in the past 6 months; 3) adaptations to skip patterns to allow for the assessment of subthreshold conditions; and 4) the inclusion of distress or impairment criteria for the classification of each disorder. All modifications and translations into Canadian-French were approved by the developers of the MINI-KID.
Training of Statistics Canada interviewers on the administration of the MINI-KID included in-depth review of an interviewer manual and training videos with example interviews and practice assessments. Disorder classifications derived from the MINI-KID demonstrate adequate test-retest reliability across disorders, informants, and samples, as well as convergent and discriminant validity. 25,26
DSM-IV-TR disorders assessed include mood disorder (major depressive episode), anxiety disorders (generalized anxiety, separation anxiety, social phobia, specific phobia), and behaviour disorders (attention-deficit/hyperactivity disorder, oppositional-defiant disorder, conduct disorder). Children and youth who met criteria for at least 1 disorder were classified with any disorder. Classification of disorder was established separately for parent and youth (12 to 17 years), given low to moderate agreement between parent and youth reports of mental disorders 27,28 and informant-specific patterns of associated features of disorder. 29,30 In the present study, parent-youth agreement of disorder classification was low, with κ estimates ranging from 0.21 for social phobia to 0.38 for separation anxiety (see online supplemental table).
Service contact
Mental health–related service contact was assessed using questions administered to the parent about provider type and service setting. Provider type was assessed by asking the parent whether the SC had seen or talked to a medical doctor or other professional about mental health concerns in the past 6 months. Types of providers were aggregated to include general health care providers (family doctor, pediatrician, other regular health care provider, other type of physician or specialist, nurse, other health professional), mental health providers (psychiatrist, psychologist, social worker, other type of counsellor), and a combination of complementary/alternative medicine providers (religious or spiritual leader, alternative healers such as a naturopath or herbalist) and phone helpline or crisis hotline. These last 2 types of providers were combined because the level of endorsement did not meet Statistics Canada’s minimum cell count criteria for disclosure. 24
Service setting was assessed by asking the parent whether the SC had gone to specific settings for mental health concerns in the past 6 months. The settings included 1) specialized mental health or addictions agencies, supported by providing the parent with a geographically tailored list of community agencies within their census division 31 ; 2) a walk-in clinic, urgent care facility, and hospital emergency room; and 3) school-based setting accessed since the beginning of the school year. Participants could endorse speaking to more than 1 type of provider and/or going to more than 1 service setting. An indicator of any service contact was created that included endorsement of contact with at least 1 provider or in at least 1 service setting described above.
Sociodemographic characteristics
Standard Statistics Canada questions were administered to the parent about child age, sex, number of biological parents in the home, household income below the low-income measure (based on the 2013 before-tax cutoffs), 32 immigrant background (children and youth who were foreign-born or who had at least 1 foreign-born parent were classified as immigrant), and urban-rural residency (large urban, small-medium urban and rural) based on population density and size. 33
Statistical Analysis
The sample is based on the SC, chosen randomly in each household for a more detailed assessment of mental disorder (i.e., MINI-KID) and mental health–related service contacts (n = 3809 children aged 4 to 11 years; n = 2728 youth aged 12 to 17 years). About 10% of the sample was missing at least 1 parent-reported variable (n = 375 children aged 4 to 11 years; n = 309 youth aged 12 to 17 years). Children and youth with incomplete data were more likely to live with 1 or no biological parent and have a mental health–related service contact and a behaviour disorder. To address missed responses on study variables, multivariate, multiple imputation by chained equations (MICE) was performed in STATA 14.0. 34 Separate imputation models were developed for each informant (i.e., parent and youth reports) that included sampling design variables, all variables included in the present study, and auxiliary variables associated with missed responses. Primary analyses were based on 10 multiply imputed data sets, and results were combined using Rubin’s combination rules. 35,36 A comparison of the estimates from imputed and complete case analyses (available upon request) produced consistent results.
Prevalence estimates of mental disorders and service contact are presented for children (4 to 11 years) and youth (12 to 17 years) by informant (parent, youth), sex, number of biological parents in the home, household poverty, immigrant background, and urban-rural residency. Also presented are cross-tabulations of the association between service contact by provider type and setting and the following mutually exclusive classifications of disorder: 1) pure mood and/or anxiety, wherein the SC met criteria for mood and/or anxiety disorders but not behaviour disorders; 2) pure behaviour, wherein the SC met criteria for behaviour disorders but not mood and/or anxiety disorders; and 3) comorbid mood/anxiety and behaviour, wherein the SC met criteria for both mood and/or anxiety and behaviour disorders.
All analyses used sampling weights to generate prevalence estimates that are representative of the target population of children and youth in Ontario. To account for the complex survey design, mean bootstrap weights were applied with an adjustment factor to produce accurate standard errors in STATA 14.0. 34 To examine differences between groups in the prevalence of any mental disorder and mental health–related service contact, second-order Rao-Scott correction to χ2 tests (design-based F statistic) for complex survey design 37 was used to produce accurate test statistics and associated P values. The false discovery rate (FDR) method 38 was employed to account for multiple comparisons. Estimates were suppressed when unweighted cell counts were <10 and denoted with a “–.” 24
Results
Table 1 presents sample characteristics: the majority lived with 2 biological parents (71.2%), in large urban centres (70.3%), and in nonimmigrant families (64.4%).
Sociodemographic Characteristics of Study Sample, n = 6,537.
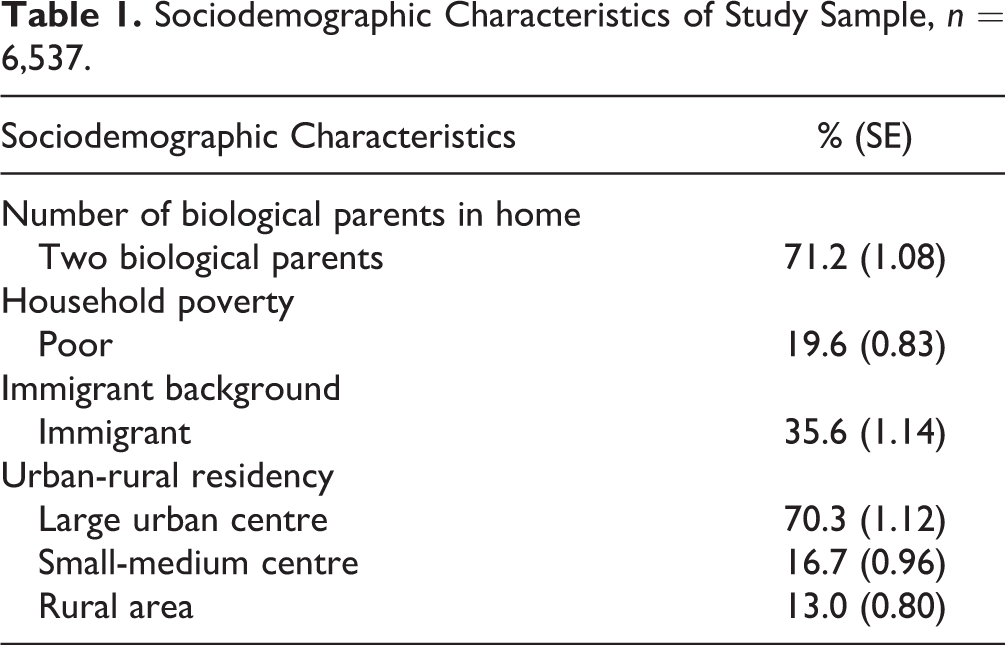
Table 2 presents 6-month prevalence estimates of disorder by age group, informant, and sex. The overall prevalence of any disorder was 18.1% for children (4 to 11 years) and 18.2% for youth (12 to 17 years) based on parent report and 21.8% based on youth report. Integrating parent and youth (12 to 17 years) reports of disorder yielded overall prevalence estimates of any disorder that ranged from 7.5% when the “and” rule and 26.0% when the “or” rule was applied at the disorder level (see online supplemental table).
Six-Month Prevalence of DSM-IV-TR Disorders by Age Group, Informant, and Sex.
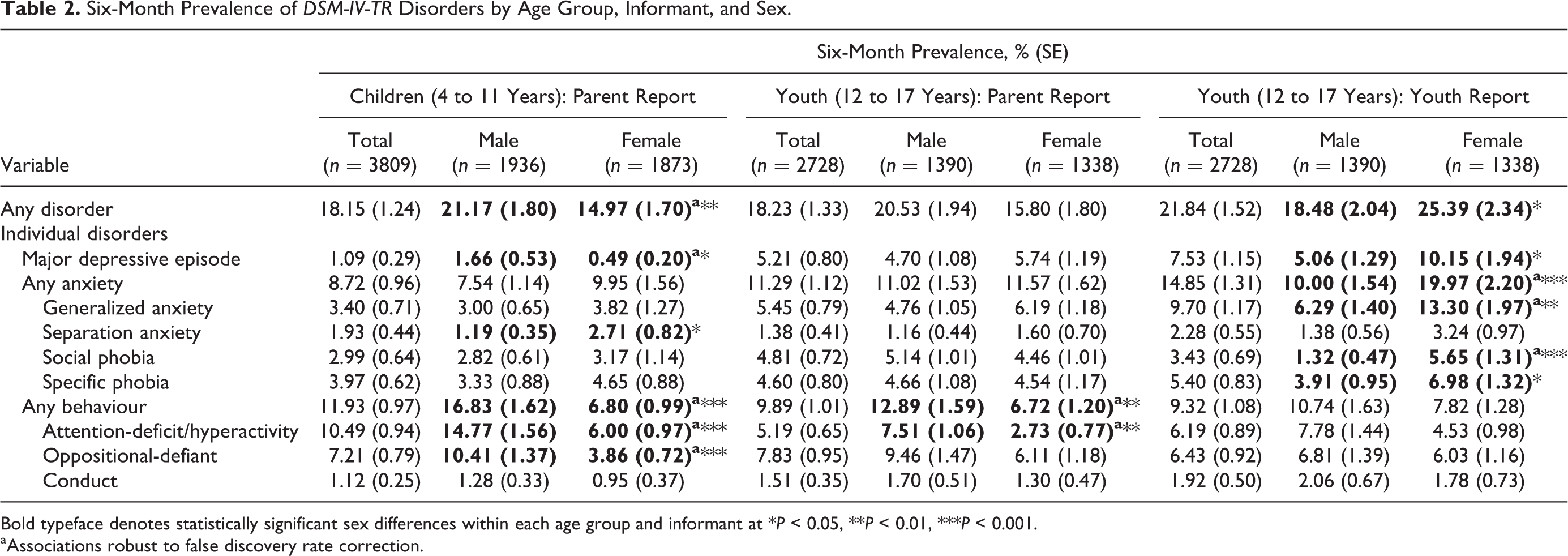
Bold typeface denotes statistically significant sex differences within each age group and informant at *P < 0.05, **P < 0.01, ***P < 0.001.
aAssociations robust to false discovery rate correction.
Among youth (12 to 17 years), the overall prevalence of any disorder was higher for females compared to males based on youth report (25.4% versus 18.5%) but generally higher in males compared to females based on parent report (20.5% versus 15.8%). The higher prevalence of any disorder in females identified by youth was attributable to major depressive episode (10.1% versus 5.1%) and generalized anxiety (13.3% versus 6.3%). There were no significant sex differences in the prevalence of anxiety disorders and major depressive episode, based on parent report on youth (12 to 17 years). The higher prevalence of any disorder in males identified by parents was largely attributable to elevated rates of attention-deficit/hyperactivity disorder (7.5% versus 2.7% in youth).
Table 3 presents the prevalence of any disorder by age group, informant, and sociodemographic characteristics. Correlates of any disorder were consistent across age groups and informants. Prevalence of disorder was consistently higher among children and youth living with 1 or no biological parent and consistently lower for those living in an immigrant family. Among youth (12 to 17 years), living in small to medium population centres was associated with higher prevalence (32.6% youth report) compared to large urban (19.1% youth report) and rural areas (23.0% youth report).
Six-Month Prevalence of Any DSM-IV-TR Disorder by Age Group, Informant, and Sociodemographic Groups.
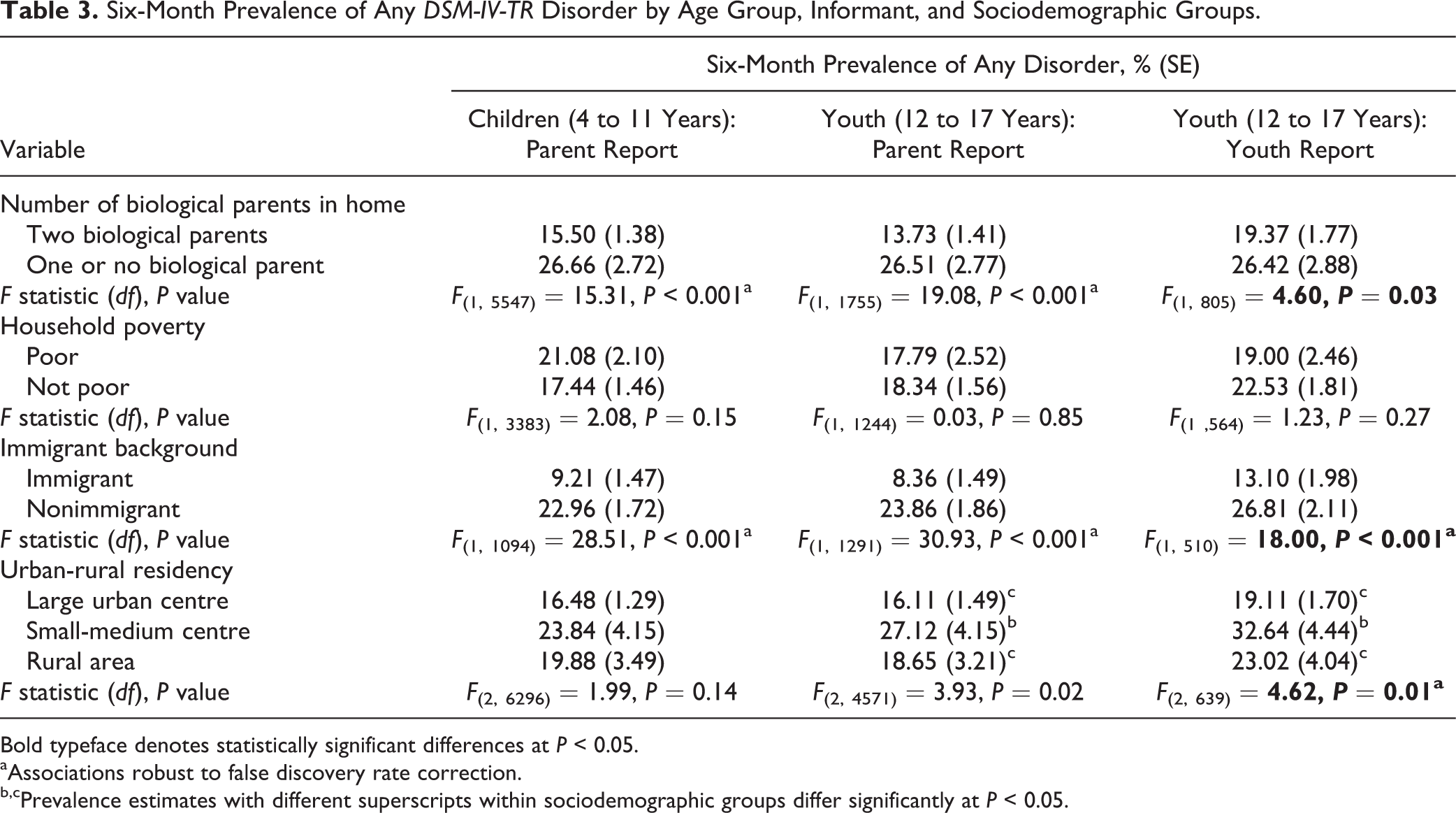
Bold typeface denotes statistically significant differences at P < 0.05.
aAssociations robust to false discovery rate correction.
b,cPrevalence estimates with different superscripts within sociodemographic groups differ significantly at P < 0.05.
Table 4 presents rates of mental health–related service contacts in the past 6 months by disorder class, age group, and informant. Among children and youth with an identified disorder, overall rates of any service contact were 61.5% for children (4 to 11 years) and 60.7% for youth (12 to 17 years) when disorder classification was based on parent report. In contrast, rates of any service contact were much lower when disorder classification was based on youth report (43.7%). Children with comorbid mood/anxiety and behaviour disorders were most likely to have service contacts. Although rates of any service contact were similar for pure mood/anxiety and pure behaviour disorders identified in youth (12 to 17 years) by parents or youth (49.6% versus 51.4% and 39.9% versus 39.7%), this was not the case among children (4 to 11 years). Rates of any service contact in this age group were 66.3% for pure behaviour and 44.6% for pure mood/anxiety. This difference was largely attributable to school-based services where rates of service contact were 59.3% for pure behaviour and 31.9% for pure mood/anxiety disorders.
Six-Month Prevalence of Mental Health–Related Service Contact among Children and Youth with DSM-IV-TR Disorders.
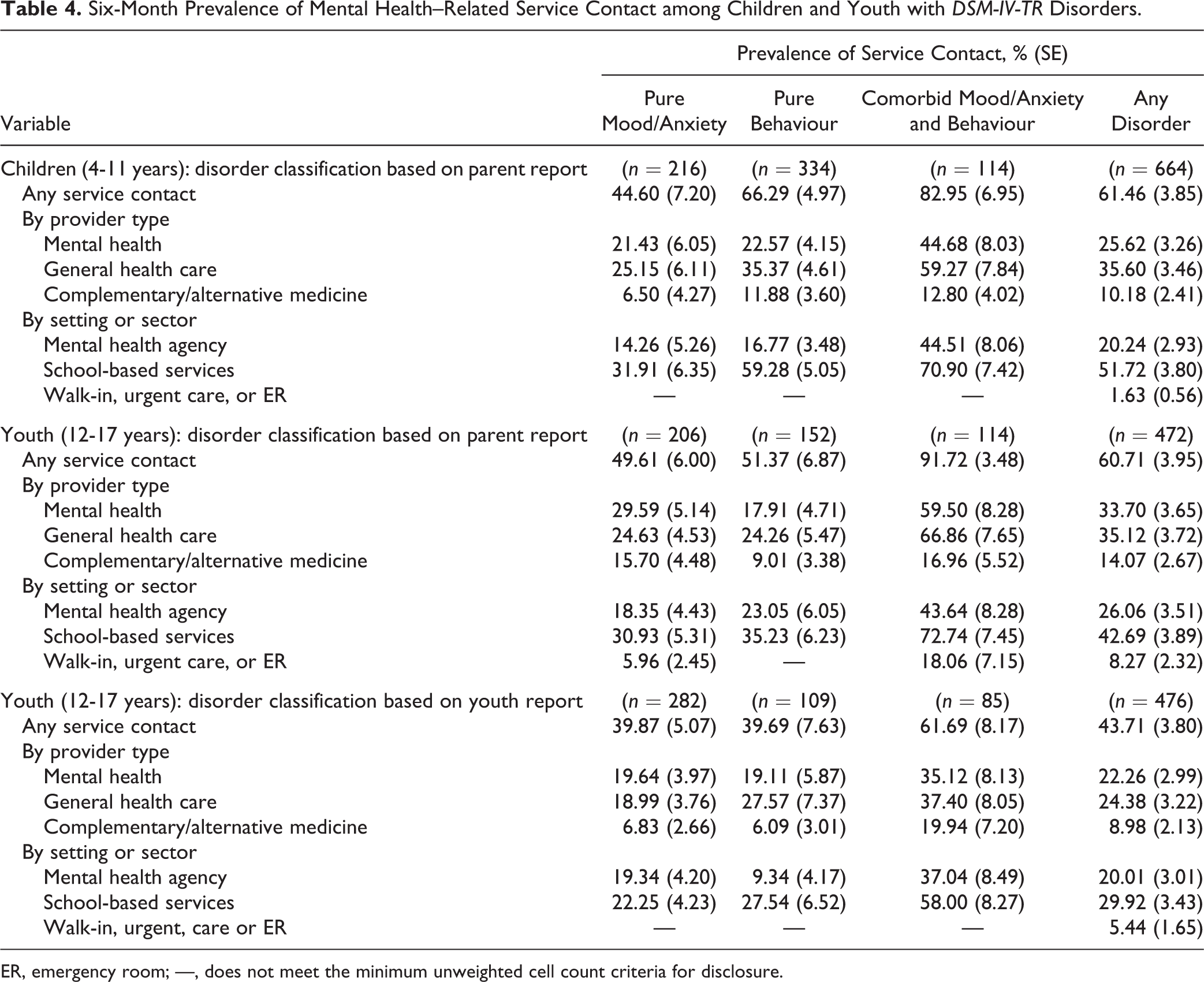
ER, emergency room; —, does not meet the minimum unweighted cell count criteria for disclosure.
Among youth, rates of service contact from mental health and general health care providers were similar (33.7% and 35.1% for parent-reported disorder and 22.3% and 24.4% for youth-reported disorder, respectively). Among children (4 to 11 years), 25.6% and 35.6% saw mental health and general health care providers for mental health concerns, respectively. The most common setting or sector for mental health–related service contacts was the school (Table 4).
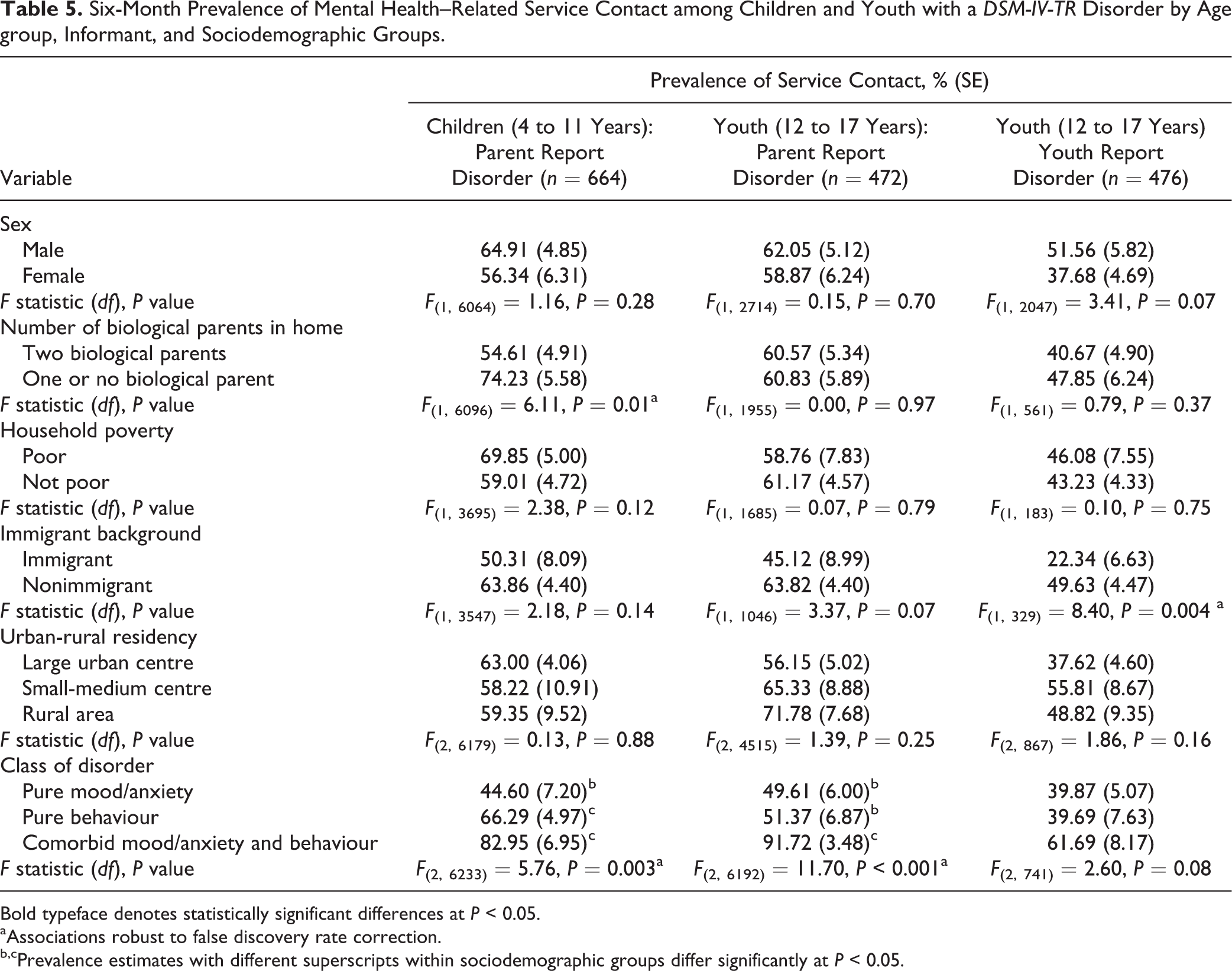
Table 5 presents the prevalence of service contact for those classified with a mental disorder by age group, informant, and sociodemographic groups. Immigrant children and youth were less likely to have a mental health–related service contact (22.3%-50.3%) compared to their nonimmigrant peers (49.6%-63.8%). Children and youth with comorbid mood/anxiety and behaviour disorders were most likely to have a mental health–related service contact (61.7%-91.7%) compared to those with pure behaviour (39.7%-66.3%) and pure mood/anxiety disorders (39.9%-49.6%). Children living with 1 or no biological parent were more likely to have a mental health–related service contact (74.2%) compared to those living with 2 biological parents (54.6%). When disorder classification was based on youth report, females were less likely to have a mental health–related service contact (37.7%) compared to males (51.6%).
Six-Month Prevalence of Mental Health–Related Service Contact among Children and Youth with a DSM-IV-TR Disorder by Age group, Informant, and Sociodemographic Groups.
Bold typeface denotes statistically significant differences at P < 0.05.
aAssociations robust to false discovery rate correction.
b,cPrevalence estimates with different superscripts within sociodemographic groups differ significantly at P < 0.05.
Discussion
From 2014 to 2015, 18% to 22% of children and youth aged 4 to 17 years in Ontario met criteria for at least 1 DSM-IV-TR mental disorder assessed in the Ontario Child Health Study. Among children and youth with a parent-identified mental disorder, only 26% of children (4 to 11 years) and 34% of youth (12 to 17 years) had contact with a mental health care provider, although a much larger proportion had mental health–related service contacts with other providers and in other settings.
Rates of service contact were consistently lower when disorder classification was based on youth report. Children and youth with comorbid mood/anxiety and behaviour disorders had higher rates of service contact with a mental health care provider compared to those with pure mood/anxiety or pure behaviour disorders. Schools were the most common setting for mental health–related contacts with various professionals. Across settings, general health and mental health care practitioners were the most common providers. The high prevalence of disorder and service gaps underscores the continued public health importance of child and youth mental health in Ontario.
Sex differences in the prevalence of disorder were largely consistent with previous studies, 1,2,6,7 with 1 noteworthy exception. Among youth (12 to 17 years), there was a reversal in the pattern of sex differences based on parent versus youth reports. The major classes of disorder contributing to this reversal were mood and anxiety disorders. While prevalence estimates were similar for males and females based on parent report, youth report revealed rates that were 2 to 3 times higher for females compared to males.
Past studies have documented more pronounced sex differences in ratings of emotional problems based on youth compared to parent reports. 2,29 Given the critical role of parents in initiating access to mental health services, 20 parental underidentification of anxiety and depression among adolescent girls may be contributing to gender-related treatment gaps. Consistent with past studies, 15,18,19 children with mood and/or anxiety disorders and females were generally less likely to have mental health–related service contacts compared to children with other classes of disorder and males. These differences highlight the need to identify and address gender-related barriers to the recognition of mental disorders and use of mental health services. The prominent role that parents and school-based and general health care providers play in initiating access to services suggests that such efforts should include a focus on improving identification and care pathways for girls, particularly those with mood and/or anxiety disorders. 20
In terms of residency, prevalence of disorder among youth was highest in small to medium centres compared to large urban centres and rural areas. This contrasts with epidemiological studies reporting higher prevalence in urban compared to rural areas. 1,6 Our companion article documents larger increases in the prevalence of mental disorders and perceived need for professional help between 1983 and 2014 in small to medium centres and rural areas compared to large urban centres. 39
Differences between urban versus rural areas in the percentage of children (4 to 11 years) and youth (12 to 17 years) with a mental disorder having mental health–related service contacts did not reach statistical significance. These findings contrast sharply with those reported in the 2017 Scorecard for the Mental Health of Children and Youth in Ontario, 40 which document increased access and use of specialized physician-based mental health care in urban compared to rural and remote communities, drawing attention to conflicting results attributable to sample and data source differences. It is important to note that past US studies 16,18 and the 1983 OCHS 1 did not report urban-rural differences in mental health service use for children and youth. Further analyses of the 2014 OCHS will be useful in refining our understanding of geographical variation in access to child and youth mental health services, the nature of services received, and barriers to care.
Consistent with past studies, prevalence of mental disorder was higher among children and youth living in nonintact families 6,13 and lower among those living in immigrant families. 8 –10 In contrast, household poverty was not associated with prevalence of disorder. Similar findings have been reported using data from a national survey of US adolescents that documented consistent associations between parental education and mental disorder but no consistent poverty effect. 6,12 Past studies have demonstrated stronger associations between poverty and mental disorder in children compared to adolescents 41,42 and for behaviour compared to mood and anxiety disorders. 42 –45 Further analysis of joint education-income effects by disorder class (i.e., behaviour versus mood/anxiety), age groups, and informants is needed to enhance our understanding of associations between family socioeconomic circumstances and child and youth mental disorder.
Proportionately fewer immigrant children and youth with a mental disorder had a mental health–related service contact compared to those living in nonimmigrant families. Despite their lower overall prevalence of disorder, these findings point to important disparities in mental health–related service contacts among children and youth from immigrant backgrounds that need to be addressed. 10
Children (4 to 11 years) living with 1 or no biological parent were more likely to have a mental health–related service contact compared to those living with 2 biological parents. The higher prevalence of mental disorder among children and youth living in nonintact families and their increased likelihood of having mental health–related service contacts reinforce the importance of family context in shaping mental health and treatment pathways. The mechanisms underlying these associations, including the presence and timing of relationship disruptions among caregivers, single parenthood, parental psychopathology, and family stressors, warrant further study.
Strengths of the study include the large and representative sample of children and their families, the use of a validated diagnostic interview administered independently to parent and youth that incorporated distress and/or an impairment criterion in the classification of mental disorders, and comprehensive assessment of mental health–related service contacts. Study limitations include our inability to document the temporal ordering of study variables in relation to disorder onset and persistence, low response rate, exclusions of high-risk samples (i.e., youth living on reserves and in institutions), and specific disorders (i.e., substance use disorders). In addition, our approach to classifying mental health–related service contact relied solely on parental report and should not be equated with receipt of mental health treatment. Our goal was to establish the percentage of children and youth who received some form of recognition for mental health concerns, as an index of service contact within our systems of care. Future studies will systematically examine the nature and level of satisfaction of care received and perceived barriers to accessing care.
Conclusion
Without renewed attention to innovative service delivery models, 20,46,47 the gap between child and youth mental health need in the population and the availability of specialized mental health care is too large to bridge. Schools and general health care providers represent settings and professionals that can help facilitate the implementation of a stepped collaborative care model to child and youth mental health, playing a pivotal role in the identification and management of mental health problems and referral to specialized services for those children and youth most in need. Such approaches will require significant training and supervision of nonspecialist providers and the establishment of close partnerships across sectors of care, including mental health, health, and education. Specific subgroups of children and youth may also benefit from targeted prevention efforts and outreach to facilitate access to mental health care, including children from nonintact families, immigrant backgrounds, and females with mood and/or anxiety disorders.
Despite significant growth in the field of child psychiatric epidemiology, we continue to lack harmonized methods of data collection on the magnitude, correlates, and associated burden of mental disorders, rendering comparisons across studies and contexts impossible. The high prevalence of child and youth mental disorders and significant service gaps provide a strong rationale for continuing to prioritize research and policies aimed at preventing mental disorders and facilitating access to evidence-based care amongst those in need.
Supplemental Material
Supplemental Material, 830024_supplemental_table - Six-Month Prevalence of Mental Disorders and Service Contacts among Children and Youth in Ontario: Evidence from the 2014 Ontario Child Health Study
Supplemental Material, 830024_supplemental_table for Six-Month Prevalence of Mental Disorders and Service Contacts among Children and Youth in Ontario: Evidence from the 2014 Ontario Child Health Study by Katholiki Georgiades, Laura Duncan, Li Wang, Jinette Comeau, Michael H. Boyle and 2014 Ontario Child Health Study Team in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We thank Dr. Kathleen R. Merikangas for her critical review of the manuscript, Dr. James Carpenter and Dr. Paul Allison for advice regarding handling missing data, and Steven Ma and Nancy Pyette for technical assistance with editing and proofreading the manuscript.
Data Access
Data access available through Statistics Canada Research Data Centres.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The primary authors (KG, LD, LW, JC, and MB) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by research operating grant 125941 from the Canadian Institutes of Health Research (CIHR), Health Services Research Grant 8-42298 from the Ontario Ministry of Health and Long-Term Care (MOHLTC), and funding from MOHLTC, the Ontario Ministry of Children and Youth Services, and the Ontario Ministry of Education. Dr. Boyle is supported by the CIHR Canada Research Chair in the Social Determinants of Child Health and Dr. Georgiades by the David R. (Dan) Offord Chair in Child Studies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.