
Abstract
Objective:
This paper reports on substance use, mental health problems, and mental health service utilisation in an early adolescent school-based sample.
Method:
Participants were 1,360 grade 7 and 8 students from 4 regions of Ontario, Canada. Students completed an in-class survey on mental health and substance use. The sampling strategy and survey items on demographics, substance use, service utilisation, and distress were adapted from the Ontario Student Drug Use and Health Survey. Internalising and externalising mental health problems were assessed using the Global Assessment of Individual Needs – Short Screener. Distress was defined as fair or poor self-rated mental health.
Results:
Rates of internalising and/or externalising problems above the threshold exceeded 30%; yet, fewer than half had received mental health services in the past 12 mo. Substance use was associated with increased odds of internalising and externalising problems above the threshold and distress. Youth using cannabis had 10-times the odds of exceeding the threshold for internalising or externalising problems. The use of substances other than alcohol or cannabis was associated with increased odds of fair or poor self-rated mental health among grade 8 students. Of the youth who confirmed at least a substance use problem, most also reported mental health problems; this association was stronger among girls than boys.
Conclusions:
Early adolescent substance use was associated with concurrent self-reported mental health problems in a non-clinical sample. The low levels of service utilisation reported highlight the need for improved access to early identification and intervention to prevent the development of concurrent disorders.
Concurrent mental health (MH) and substance use (SU) disorders (e.g., concurrent depression and cannabis use disorders) are associated with negative outcomes, 1 –3 including academic, vocational, health, and relationship problems, with there being an unmet need for services addressing SU and MH. 1,3 –9 Research on the co-occurrence of MH and SU problems has shown substantial overlap between MH and SU problems among mid to late adolescents. 10 –16 Less is known about concurrent SU and MH problems in early adolescents.
Early adolescence (age 11 to 14 y) is the typical age of onset for many MH disorders, including internalising (e.g., anxiety, depression) and externalising problems (e.g., attention deficit hyperactivity disorder, conduct disorder). 17 –19 Notably, dimensional factors, including internalising, externalising, and thought disorder symptoms, coexist with a general psychopathology or dysregulation factor to explain MH concerns among youth as a whole in clinical 20 and community 21 settings, possibly including SU concerns. 20 Although SU initiation typically occurs in mid-adolescence, some youth initiate SU in early adolescence. 22 Early SU initiation and use is a risk marker for SU disorders and other negative adult outcomes, 23 –25 even if not causally linked, because of its association with MH challenges, family SU problems, genetic risk, and other vulnerabilities. 26 –29 Associations between early adolescent SU and MH problems have been demonstrated but results have been mixed, showing, for example, SU associations with externalising and internalising problems, protective effects of internalising problems against specific types of SU, and interactions between specific internalising and externalising disorders and problematic SU. 27,30 –32,33 Similarly, gender effects have been mixed, with some studies showing stronger associations between internalising problems and SU for girls and others showing particular links between externalising problems and SU for boys; still others show no specific gender effects. 10,27,33 –35
Given that early adolescent MH and SU are associated with adult outcomes, effective early intervention is crucial to prevent emerging MH and SU problems from developing into more chronic, severe difficulties, including concurrent disorders (CDs). 19,34,36,37 It is important to sample youth from community, rather than clinics, to avoid referral bias and include youth with significant MH problems not engaged in treatment. Low specialised treatment rates among youth with MH and SU challenges have been identified provincially and nationally. 16,38 –42 Moreover, information about the adequacy of services received to meet treatment needs (e.g., intensity, quality, appropriateness) is lacking and many youth experience sustained unmet treatment needs. 42 –44 Although specialised treatment may not be needed among youth with subclinical difficulties, understanding the extent to which early adolescents with MH problems engage with counselling or other MH services is needed. In addition, attention to symptoms, including subclinical problems, rather than disorders, is needed to understand relationships between internalising and externalising difficulties and SU among early adolescents.
The current study examines the overlap between MH problems and SU based on survey results in an Ontario middle school sample. The study is 1 of 4 inter-related projects focused on youth CDs. 6 We aim to address the following questions: 1) What are the rates of internalising and externalising MH problems, SU, and SU problems among early adolescents from a non-clinical sample? 2) To what extent do MH problems overlap with SU and SU problems in this age group? and 3) What proportion of youth who report significant problems have received counselling or spoken with a health provider about their MH? We hypothesized that there would be significant overlap between SU and internalising and externalising MH problems. Although we make no specific hypotheses regarding proportions, reporting difficulties, and receiving treatment, given difficulties with youth service access and engagement, 6,9,39 we expected that there would be substantial unmet need (i.e., reporting significant MH problems and not speaking with a service provider).
Method
Sampling
Two school boards (one public and one publicly funded Catholic) were purposively selected within each of the 4 regional strata used in the Ontario Student Drug Use and Health (OSDUHS) province-wide, cross-sectional survey; boards were selected to include large urban, northern urban, suburban, and rural areas. 22 Consistent with OSDUHS, the sampling frame excluded military bases, First Nations reserves, youth justice facilities, and other non-mainstream school contexts. 22 Data were collected in 2 panels. In Panel 1 (2011), 7 of the 8 selected school boards agreed to participate; in Panel 2 (2013), 6 boards agreed to participate again.
Schools were randomly selected from participating school boards using probability-proportional-to-size sampling. In strata where a board declined, additional schools were selected from the participating boards. Schools selected to participate in OSDUHS the same year were excluded. For Panel 1, 24 of 36 schools randomly selected (66.67%) participated, one (8.33%) was excluded due OSDUHS participation and 11 (30.56%) declined and were replaced by additional randomly selected schools. For Panel 2, Panel 1 schools were invited to participate in a second panel of data collection. Of the 22 schools re-invited at Panel 2, 17 (77.27%) participated, one (4.55%) was excluded due to ODUHS participation, 3 (13.63%) declined and one (4.55%) had closed; replacement schools were used for these 4 schools. For each school, one grade 7 and one grade 8 classroom (excluding special education classes) were randomly selected. Informed parental consent and participant assent was obtained. A pencil and paper survey (40 to 45 min) was administered during class. Surveys were anonymous to increase the validity of self-reports of stigmatized and/or illegal behaviors. 45
Participation rates (Panels 1 and 2 combined), for large urban, northern urban, suburban, and rural areas, respectively, were 58%, 58%, 69%, and 71%, respectively. OSDUHS participation rates (2013) for grade 7 and 8 students were 59%, 60%, 63%, and 57%, respectively, for corresponding regions. 22
Participants
Participants were 1,360 grade 7 and 8 students (Panel 1, n = 787; Panel 2, n = 573), from large urban (n = 372; 27.4%), northern urban (n = 326; 24.0%), suburban (n = 337; 24.7%), and rural (n = 325; 23.9%) regions. Overall, 48.9% identified as boys and 50.1% as girls. Fewer than 1% of participants did not specify sex/gender; however, trans, nonbinary or additional categories were not included as options. These participants were excluded from models that included sex/gender as a covariate/predictor but were included in totals/estimates. Participants’ mean ages, adjusted for sampling characteristics, were 12.25 y (SE, 0.02 y) for grade 7 and 13.25 y (0.03 y) for grade 8 students. There were no regional differences in sex/gender, age, or grade (see Table 1 for additional demographic characteristics).
Demographic Characteristics by Region.
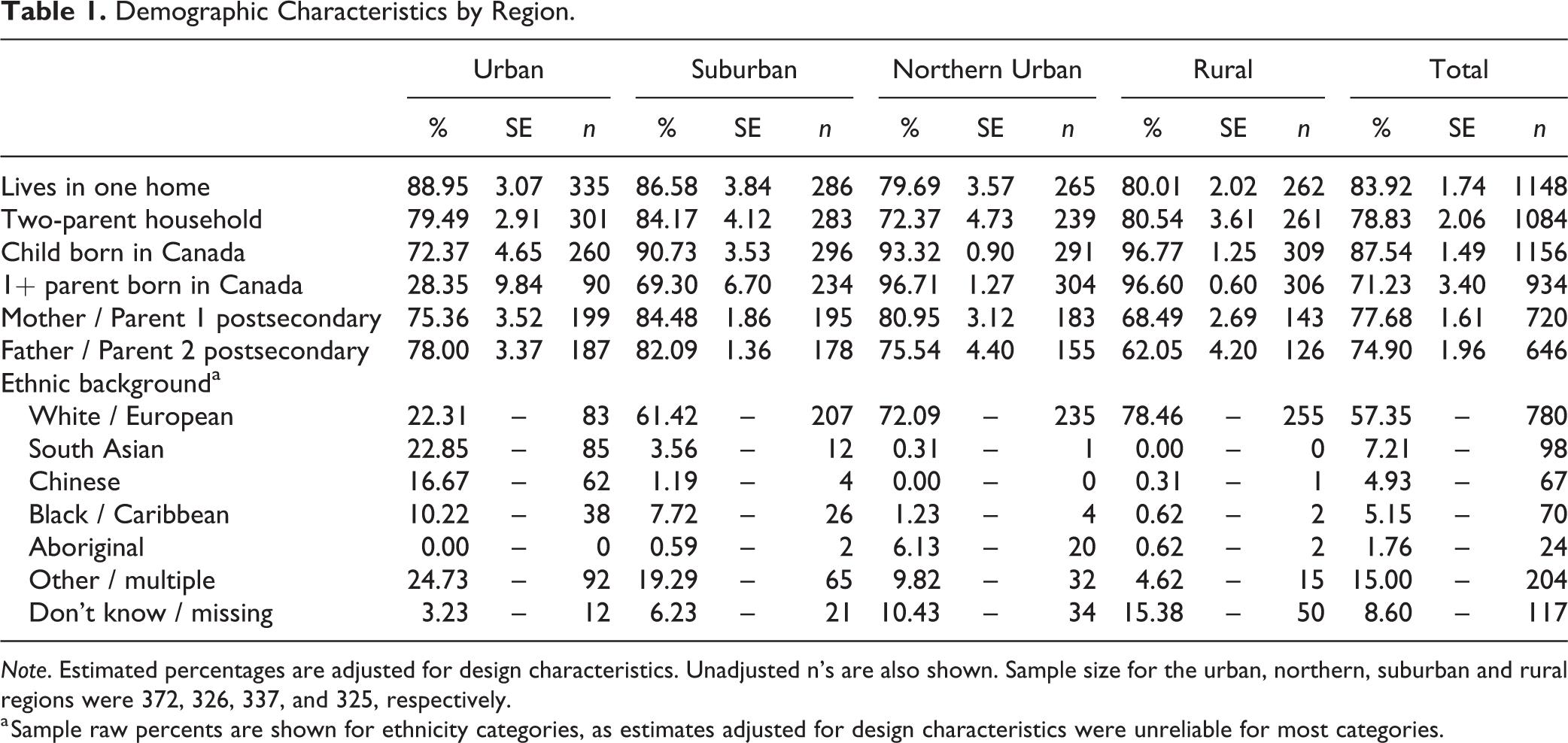
Note. Estimated percentages are adjusted for design characteristics. Unadjusted n’s are also shown. Sample size for the urban, northern, suburban and rural regions were 372, 326, 337, and 325, respectively.
a Sample raw percents are shown for ethnicity categories, as estimates adjusted for design characteristics were unreliable for most categories.
Measures
Global appraisals of individual needs – short screener (GAIN-SS)
We used the GAIN-SS, 46 a short form of the Global Assessment of Individual Needs, previously validated with youth as young as 12 y. 46 Standard scoring was used. Sensitivity and specificity to detect diagnoses were 0.70 and 0.90, respectively. 46
Adapted survey items
Demographic, SU, and service utilisation items were adapted from the OSDUHS study instrument. 22 Sex/gender was ascertained with the question, ‘Are you (a) male (b) female’ with no additional options; therefore, missing data may represent trans or nonbinary youth. Participants reported past 12-mo alcohol use frequency and 9 additional substances used ‘to get high’: 1) cannabis (and alternate terms), 2) 3,4-methylenedioxy-methamphetamine MDMA or ‘ecstasy’, 3) cocaine, 4) glue or other solvents, 5) non-medical use of cough/cold medications, 6) other over-the counter-medications, 7) pain relief pills, 8) attention deficit hyperactivity disorder medication, and 9) other prescription medications. A fictitious substance was also queried as a validity check. All alcohol use except for ‘had a sip just to try it’ was defined as alcohol use. For other substances, ‘1 or 2 times’ or more often was defined as ‘use’. Service utilisation was defined as the number of visits with a counsellor or other professional to address MH. This variable was trichotomized (0, 1 to 5, and 6 or more visits) to differentiate minimal from more extended contact; a threshold of 6 was selected based on the literature on youth psychotherapy. 47,48
Data Analysis
All analyses were conducted using the Stata 12 survey module, weighted to adjust for probability-proportion-to-size sampling, and school-specific response rates within the grade, 22 and adjusted for clustering using Taylor linearisation. 22 Sample characteristics (sample size by region, grade, sex/gender) are shown unadjusted. Ethnicity (within regions) is also shown unadjusted, as survey estimates for many categories within regions were unreliable due to sample size.
Data validity rules were adapted from the OSDUHS; 22 indicators of a potential validity problem included 1) missing data on age or grade, 2) extreme responses on substance use (endorsement of 4+ illicit drugs used 40+ times in the past year), 3) less than 50% completed, 4) reported fictitious drug use, or 5) extreme responses on write-in answers. Twenty-five participants (1.71%) had one or more validity problem indicators and were excluded from the analyses. Estimates with a coefficient of variation greater than 0.33 are also shown but indicated as unreliable. For regional comparisons, the reference group was the large urban sample, because of challenges with service delivery in both Ontario’s rural and northern urban communities; this also allows for comparison with the largest community sampled.
Logistic regression models were fit for binary dependent variables (scoring above the threshold on GAIN-SS internalising and externalising subscales, any SU problems on GAIN-SS, endorsement of suicidal thoughts on GAIN-SS, and fair/poor self-rated MH). Multinomial logistic regression was used for the 3-level dependent variables service utilisation (none, 1 to 5 visits and 6+ visits). All potential 2-way interactions were tested with component main effects entered in the model; non-significant interactions were removed from the model. Three-way interactions (i.e., sex/gender by grade by region) were not included because of sample size limitations and interpretation challenges due to potential specificity of the selected sample.
Results
Mental Health and Substance Use Problems
Table 2 shows estimates for the proportion of participants who scored above the threshold on GAIN-SS subscales. Externalising and internalising problems overlapped; 59.42% (SE, 3.11%) of participants who scored above the threshold on externalising also scored above the threshold on internalising. Over 30% exceeded the threshold for either internalising or externalising MH problems: 12.66% (0.79%) met the criteria for internalising only, 8.34% (0.79%) for externalising only, and 12.21% (1.33%) for both internalising and externalising. Considerably fewer participants (7.47% [0.70%]) reported at least one SU problem on the GAIN-SS, and of these, most (71.80% [4.99%]) also met internalising and/or externalising criteria. Girls were more likely than boys to score above the threshold on internalising problems (OR = 1.87, SE = 0.29, t[25] = 4.12, P < 0.001). Grade 8 students were more likely than grade 7 students to report at least one SU concern (OR = 2.01, SE = 0.49, t[25] = 2.86, P < 0.008). In addition, participants were more likely to report at least one SU concern if they were from northern (OR = 4.57, SE = 1.29, t[25] = 5.39, P < 0.001) or rural (OR = 3.26, SE = 0.89, t[25] = 4.32, P < 0.001) regions, as compared with students in the large urban region.
Mental Health and Substance Use Problems by Sex/Gender and Grade.
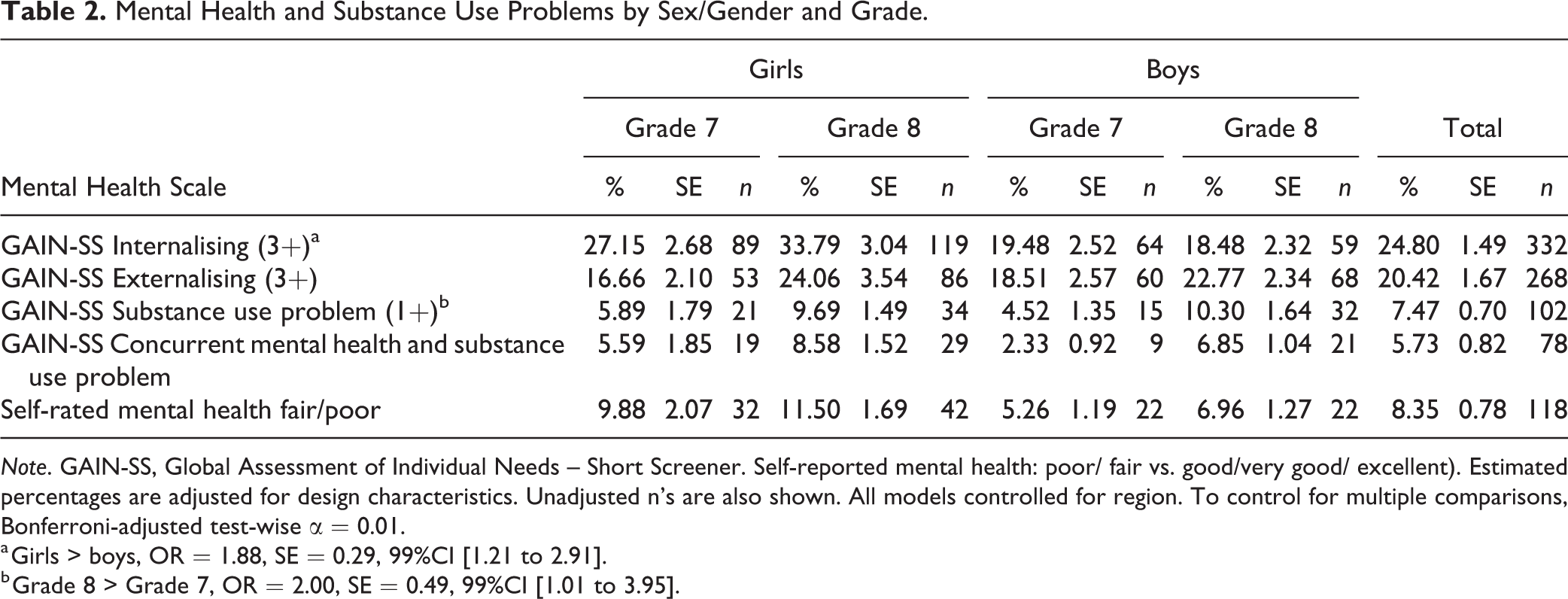
Note. GAIN-SS, Global Assessment of Individual Needs – Short Screener. Self-reported mental health: poor/ fair vs. good/very good/ excellent). Estimated percentages are adjusted for design characteristics. Unadjusted n’s are also shown. All models controlled for region. To control for multiple comparisons, Bonferroni-adjusted test-wise α = 0.01.
a Girls > boys, OR = 1.88, SE = 0.29, 99%CI [1.21 to 2.91].
b Grade 8 > Grade 7, OR = 2.00, SE = 0.49, 99%CI [1.01 to 3.95].
The estimated proportion of students reporting fair/poor MH is shown in Table 2. Girls were more likely to report fair/poor MH than boys (OR = 1.90, SE = 0.34, t[25] = 3.54, P = 0.0016). There were no differences by grade or region. Participants who reported fair/poor MH were more likely to exceed the threshold for internalising or externalising MH problems than those who did not (OR = 12.65, SE = 4.49, P < 0.001); these participants also reported more symptoms on the GAIN-SS (F[1,25] = 79.17, P < 0.001) when controlled for sex/gender, grade, and region. Only 1.97% (0.56%) of participants below the threshold on either internalising or externalising reported fair/poor MH. Thus, participants reporting fair/poor MH comprised a severe subset (21.16% [2.38%]) of those who met the criteria for internalising or externalising. Overall, the proportion who reported fair/poor MH and exceeded the threshold on the GAIN-SS was 6.87% (0.79%) for internalising and 4.59% (0.072%) for externalising problems.
Table 3 shows the proportion of students who reported past 12-mo use of alcohol, cannabis, or other substances by grade, sex/gender, and region. The proportion reporting alcohol use was greater among grade 8 than grade 7 participants (OR = 1.93, SE = 0.26, t[25] = 4.91, P < 0.001), and among participants from rural than large urban communities (OR = 2.80, SE = 0.85, t[25] = 3.37, P = 0.002), controlled for covariates. Most of the participants who confirmed alcohol use reported less than monthly use; 2.05% (0.34%) reported using alcohol monthly or more.
Substance Use by Region and Grade.
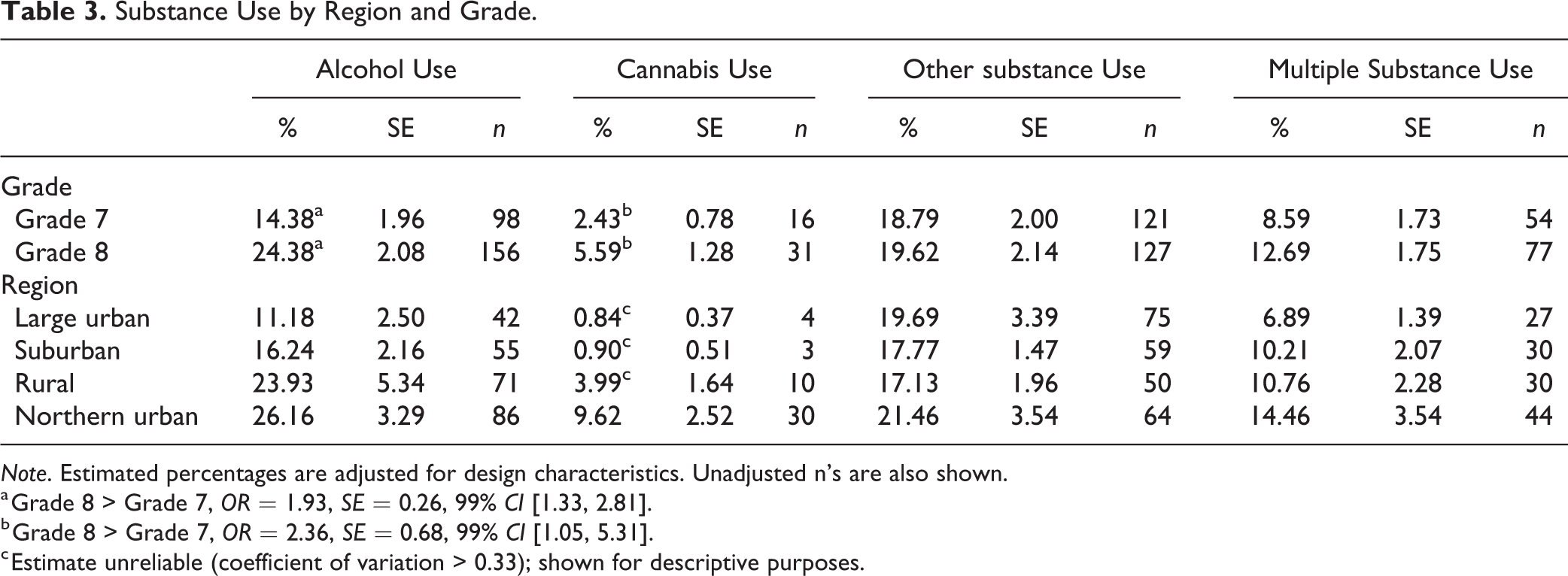
Note. Estimated percentages are adjusted for design characteristics. Unadjusted n’s are also shown.
a Grade 8 > Grade 7, OR = 1.93, SE = 0.26, 99% CI [1.33, 2.81].
b Grade 8 > Grade 7, OR = 2.36, SE = 0.68, 99% CI [1.05, 5.31].
c Estimate unreliable (coefficient of variation > 0.33); shown for descriptive purposes.
Relatively few participants reported any cannabis use in the past 12 mo. Grade 8 students were more likely to report cannabis use than grade 7 students (OR = 2.36, SE = 0.68, t[25] = 2.97, P = 0.006). The highest cannabis use rate was in the northern urban region; however, due to poor reliability and low use in other regions, regional comparisons were not possible. Approximately 1 in 5 participants reported using a substance other than alcohol or cannabis. There were no differences by sex/gender, grade, or region, and no interactions in the proportion of participants reporting other SU. The most common other substances ‘used to get high’ were glue or other inhalants (6.53% [0.79%]); cough medication (6.43% [0.86%]); pain medication (5.39% [0.68%]), and other prescription medications (4.26% [0.67%]).
Co-occurring Substance Use and Mental Health Problems
Table 4 shows the logistic regression models with SU (alcohol, cannabis, other substances, multiple substances) and SU problems predicting MH problems above the threshold on GAIN-SS internalising and externalising subscales. Models predicting fair/poor MH are also shown. All models are controlled for grade, sex/gender, and region.
Substance Use Predicting Mental Health Concerns: Logistic Regression Models.
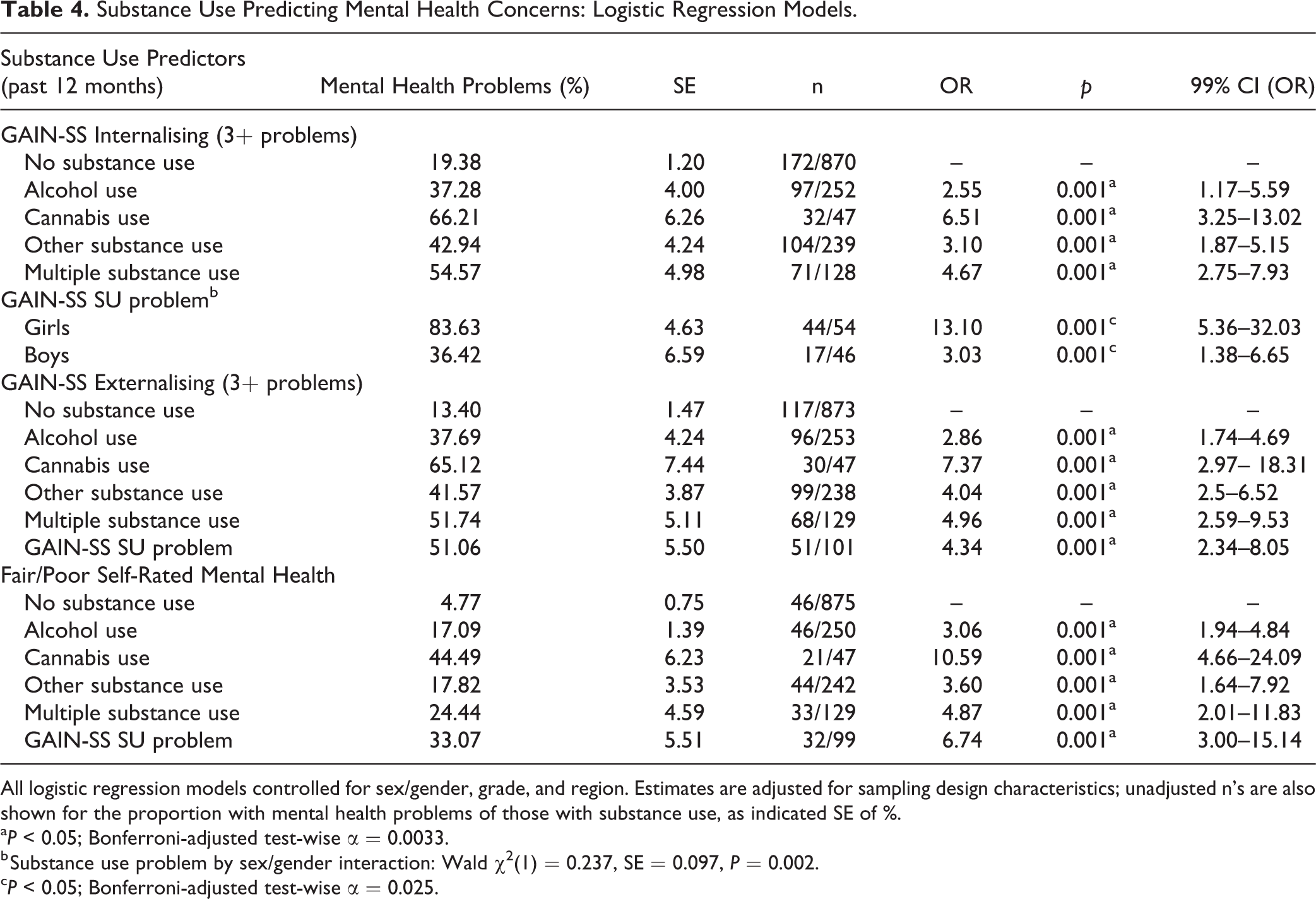
All logistic regression models controlled for sex/gender, grade, and region. Estimates are adjusted for sampling design characteristics; unadjusted n’s are also shown for the proportion with mental health problems of those with substance use, as indicated SE of %.
a P < 0.05; Bonferroni-adjusted test-wise α = 0.0033.
b Substance use problem by sex/gender interaction: Wald χ2(1) = 0.237, SE = 0.097, P = 0.002.
c P < 0.05; Bonferroni-adjusted test-wise α = 0.025.
Whereas an estimated 25.99% (0.016%) of students who did not use substances exceeded the criteria for a MH concern, participants using various substances were more likely to exceed the GAIN-SS internalising or externalising threshold and to report fair/poor MH. Cannabis use was strongly associated with both internalising problems (OR = 6.51, SE = 1.62, t[25] = 7.52, P < 0.001), externalising problems (OR = 7.37, SE = 2.41, t[25] = 6.12, P < 0.001), and self-reported fair/poor MH (OR = 10.59, SE = 3.12, t[25] = 8.00, P < 0.001). There was a significant interaction of sex/gender with endorsement of any SU problems on the GAIN-SS (t[25] = 3.42, P = 0.002), with higher odds ratios for girls (OR = 12.40, SE = 4.23, t[25] = 7.38, P < 0.001) than boys (OR = 3.47, SE = 0.82, t[25] = 5.28, P < 0.001).
To examine whether SU was associated with the severity of MH problems, additional analyses were conducted among participants who scored above the threshold on the GAIN-SS internalising or externalising subscales, comparing the number of symptoms on the internalising and externalising subscales combined. Among those participants, past 12-mo SU was associated with higher (square-root transformed) GAIN-SS MH symptom totals, controlled for sex/gender, grade, and region (coefficient = 0.16, 99%CI, 0.06 to 0.26, t(25) = 4.55, P < 0.001).
Service Utilisation
Service utilisation by MH and SU problems is shown in Table 5. Overall, 24.6% (1.79%) reported 1 to 5 visits with an MH professional, and an additional 6.28% (0.62%) reported 6 or more visits. Youth who reported internalising problems above the threshold, one or more substance use problems, or suicidal thoughts were more likely to receive services either 1 to 5 times or 6 or more times. Participants who reported fair/poor MH were more likely than other youth to receive services 6 or more times. Externalising problems did not significantly predict service utilisation.
Mental Health Professional Visits in Past Year by Mental Health and Substance Use Concerns.
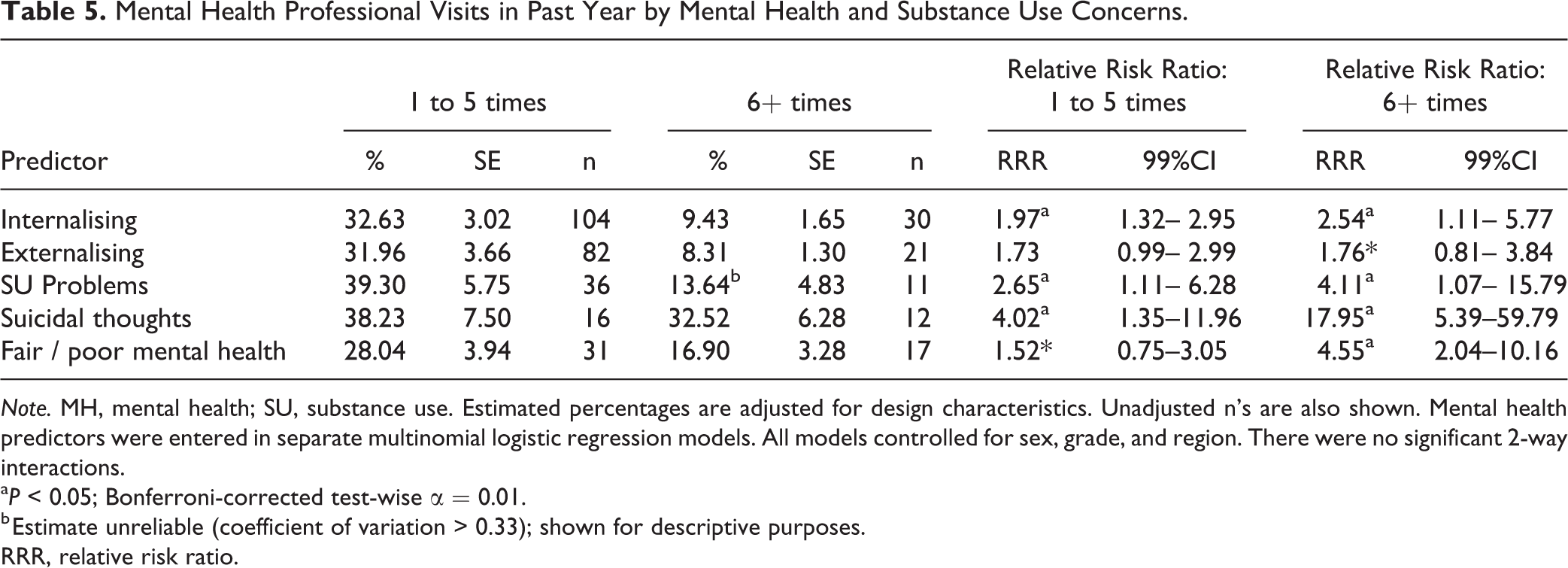
Note. MH, mental health; SU, substance use. Estimated percentages are adjusted for design characteristics. Unadjusted n’s are also shown. Mental health predictors were entered in separate multinomial logistic regression models. All models controlled for sex, grade, and region. There were no significant 2-way interactions.
a P < 0.05; Bonferroni-corrected test-wise α = 0.01.
b Estimate unreliable (coefficient of variation > 0.33); shown for descriptive purposes.
RRR, relative risk ratio.
Although most indicators of MH problems were associated with greater probability of having received services in the past year, the majority (59.45% [3.65%]) of those who exceeded the threshold on the GAIN-SS internalising or externalising scales reported receiving no MH services in the past year. Similarly, 47.06% (5.57%) of students with at least one SU problem, 53.91% (4.32%) of those who reported fair/poor MH, and 29.25% (8.03%) who reported suicidal thoughts reported receiving no professional MH services in the past year.
Discussion
This study is one of few reporting the overlap between MH and SU problems in early adolescence, assessed with validated screeners, in an Ontario non-clinical sample. 46 Although the overlap between SU and MH problems in mid-to-late adolescence is known, these data demonstrate this association in early adolescence, specifically with cannabis and additional substances other than alcohol. Even low levels of SU and SU problems were substantially associated with an increased risk for screening positive for internalising and externalising difficulties; youth with co-occurring SU or SU problems and MH problems reported greater severity of MH problems than youth without concurrent SU. Although these findings represent subclinical thresholds for SU disorder and symptom pattern screening rather than diagnoses, they demonstrate the importance of SU in understanding the emergence of co-occurring problems in a non-clinical middle school sample.
MH problems—as identified by the GAIN-SS, suicidal ideation and fair-to-poor self-rated MH—predicted engagement with MH services, as did SU problems, particularly for longer-term treatment (6 or more sessions). This association was especially strong for youth reporting suicidal thoughts, suggesting appropriate targeting of more intensive resources. However, consistent with previous findings of the high levels of unmet need in youth, 16,38 –42 a substantial proportion of early adolescents with above-threshold MH problems and almost one-third of those reporting suicidal thoughts had not received MH services within the past 12 mo. Most of the youth who engaged with services received fewer than 6 sessions, suggesting possible unmet need even among those who did speak with a professional. It is unknown, however, the extent to which participants who scored above the threshold were interested in services and unable to access them. 48,49 Fewer than one-quarter of participants who scored above the threshold on a GAIN-SS MH subscale self-reported fair or poor MH; thus, many who endorsed 3 or more internalising or externalising symptoms may not perceive a need for intervention. This issue could be clarified by a more direct assessment of youths’ perceptions of unmet need and expectations regarding services, and caregivers’ perspectives of treatment need.
Almost half of the participants scored above the threshold on internalising problems (past 12 mo); many also exceeded the threshold for externalising problems. Although the GAIN-SS has been validated with clinical samples, including early to mid-adolescents, the specificity of the GAIN-SS among non-clinical samples of early adolescents is unknown. The difference in context for youth completing the GAIN-SS in a classroom rather than with service providers may also have affected responses. Unlike clinical contexts, where youth indicate areas for which they are seeking assistance, in the classroom context, youth may be reporting more transitory problems, especially when reporting over a 12-mo timeframe. Alternatively, results may accurately reflect the high rates of MH problems among early adolescents. Consistent with the literature, girls reported higher rates of internalising problems than boys. 50 In addition, the SU–MH overlap was stronger in girls than boys. Studies have been mixed on sex/gender differences in the relation between MH and SU, with some studies reporting greater association for girls and others showing no differences. 27,34,35 Previous studies have also noted, however, that mixed findings may have resulted, at least in part, from age and gender confounding. 10 In this study, age was constrained, perhaps allowing a more careful examination of gender effects.
The pattern of regional differences—with greater rates of SU and MH problems in rural and northern communities compared with large urban communities, which is consistent with OSDUHS findings 22 —is compounded by poorer access to services in those regions. 39
The cross-sectional data do not provide information on the direction of the association between SU and MH problems, including environmental or other factors, increasing the risk for both difficulties. Response rates for this study were comparable to the OSDUHS for grade 7 and 8 students. Nevertheless, participants may differ from nonparticipants in relevant ways. For example, despite the relatively large percentage of youth who reported MH problems, the extent of MH problems among early adolescent students may have been underestimated, as some absences from school may have been related to MH or SU problems. Students in special education classes, youth justice and other out-of-home placements, which were excluded from the sampling frame, are known to have higher rates of MH problems. 4,7,51,52 In addition, the class time allotted for the survey limited the measures that could be administered and, although surveys were anonymous, youth may have hesitated to report illicit drug activity; our results are consistent with the Ontario-wide OSDUHS findings that grade 7 and 8 students prefer misusing substances that can be obtained legally. Furthermore, due to low rates, estimates of cannabis use were unreliable; therefore cannabis-related results must be interpreted with caution. Finally, the study was limited to self-report measures; no triangulation by additional raters was possible.
Despite these limitations, the findings of this study have important school, service, and policy implications. Historically, MH and SU problems have been considered and addressed separately, as exemplified by separate national policy initiatives, such as the ‘Mental Health Commission of Canada 53 and Canadian Centre on Substance Use and Addiction’. 54 School-based SU prevention efforts have typically been distinct from MH initiatives 55,56 and the integration of SU services into MH services has been inadequate. 57 More recently at the policy level, integrated strategies to address MH and SU have gained prominence, for example, in Ontario, 58 and some school-based health promotion/SU prevention initiatives have demonstrated integrated approaches and impact across MH and SU, such as that developed by Conrod. 59 Similarly, service delivery models that focus on the early identification and intervention for youth MH and SU problems in one-stop-shop models of care are expanding in Canada, including attention to the needs of early adolescents. 60 –62 The findings from this study support the need for continued development, evaluation, and implementation of these integrated approaches, particularly in terms of developing and evaluating developmentally specific prevention and early intervention approaches that are tailored to the needs of youth at differing developmental stages, of different genders, and with different MH and SU presentations. 60 –62
Conclusions
Our results demonstrate that even low levels of SU co-occur with MH problems in early adolescents living in Ontario, Canada. Our results underscore the need for the implementation of effective school-based prevention models that integrate SU and MH considerations, as well as integrated community-based models of service delivery that enhance the early identification of MH and SU needs, and facilitate access to early intervention to meet those needs and prevent the development of concurrent disorders.
Footnotes
Acknowledgements
We thank the Institute for Social Research at York University for conducting the data collection for this study. We also thank participating school boards, schools, students, and families for making this research possible.
Data Access
Data access available upon request, with appropriate ethics approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Institutes of Health Research, FRN 101832, the Rx and D Health Research Fund, and the Ontario Centre of Excellence for Child and Youth Mental Health.