
Abstract
Background:
Comorbidities between Substance Use Disorder (SUD) and mental health disorders are highly prevalent, yet there remains a lack of information regarding how mental health conditions may affect addiction severity. Consequently, this study sought to investigate the relationship between internalizing disorders (anxiety and mood disorders) and addiction severity in patients hospitalized for SUD-related medical complications. Individual difference predictors and history of prior treatment for SUD were also examined.
Methods:
Participants (N = 200) were hospitalized patients who consented to receive peer-based recovery support services for their SUD. To be eligible for the study, participants needed to have a SUD diagnosis due to alcohol, opioids, methamphetamine, cocaine, or a combination of these substances (polysubstance use). Participants completed self-report questionnaires regarding demographics, mental health history, prior SUD treatment, and addiction severity (Drug and Alcohol Screening Test; DAST-10) during their hospitalization.
Results:
Results showed that patients with Generalized Anxiety Disorder (GAD) (M = 6.68, SD = 2.97) had greater addiction severity compared to those without GAD (M = 5.41, SD = 3.34), P = .016. Addiction severity results stratified by SUD type showed that the relationship was significant among patients with Alcohol Use Disorder (P = .014), but not among those with other SUD types (Ps > .27). Major Depressive Disorder (MDD) and Post-Traumatic Stress Disorder (PTSD) were not linked to addiction severity. Among those with GAD, 81.4% had previously been to treatment compared to only 53.1% of those without GAD, P = .010. The only participant characteristic linked with addiction severity was insurance status.
Conclusions:
GAD may represent a risk factor for advanced alcohol addiction trajectories, including greater addiction severity and severe health complications requiring inpatient hospitalization.
Substance Use Disorder (SUD) and co-occurring mental health disorders are highly prevalent in the general population. In 1996, the National Comorbidity Study data indicated that nearly half of those with SUD at some time in their lifetime also met criteria for one or more mental health disorders. 1 These findings remain consistent nearly 25 years later: the 2020 National Survey on Drug Use and Health found that 45% of individuals with SUD also had a mental health disorder. 2 One common framework for conceptualizing mental health disorders is the internalizing-externalizing model. 3 Internalizing disorders characterize symptoms that expressed inward and include anxiety and mood disorders. Externalizing disorders, on the other hand, reflect psychological distress that are manifested outwards, including SUDs, conduct disorder, and attention-deficit/hyperactivity disorder (ADHD 4 ). There is strong evidence that internalizing and externalizing symptoms have unique etiological underpinnings (eg, Krueger, 3 Cosgrove et al, 4 and Hatoum et al 5 ). Individuals can undoubtably experience symptoms of both internalizing and externalizing disorders; indeed, recent work has shown that certain genetic influences are linked with a general predisposition for psychopathology (eg, Murray et al 6 and Riglin et al 7 ). As such, it is important to understand the relationship between SUD and comorbid conditions, such as internalizing disorders, in individuals with severe SUD complications that require hospitalization.
Prior research estimates that about 15% to 17% of general hospital inpatients have a SUD diagnosis at time of discharge.8,9 Moreover, the rate of comorbid internalizing disorders in patients hospitalized with SUD is over double the rate of those hospitalized without a SUD diagnosis. 9 Thus, comorbidity rates between SUD and internalizing disorders are high, especially among SUD inpatient populations, and may pose heightened risk for hospitalizations. Indeed, inpatients with SUD are over twice as likely to have comorbid mental health conditions and have more serious SUD symptoms compared to those with SUD in outpatient treatment settings.10,11 SUD severity and barriers to recovery are likely to be exacerbated even further in inpatients hospitalized with medical complications from SUD. Individuals hospitalized with medical complications from SUD have an average length of SUD of 15 years, suggesting that this population has a long history of SUD. 12 Consequently, examining the relationship between SUD and comorbid mental health conditions among patients hospitalized with medical complications from SUD is important because this population is likely among the most complex and severe of individuals with SUD. They are medically complex patients with numerous layers of health barriers to their recovery. This population is at risk for a trifecta of serious health problems: having a long-term SUD, having serious medical comorbidities, and being at higher risk for mental health disorder comorbidities than outpatient populations. Despite this risk, the relationship between different substances causing SUD, addiction severity, and specific internalizing disorder manifestations remains a relatively under-explored area of research, particularly among hospitalized patients.
Relationship between comorbid SUD and internalizing disorders
There is strong evidence that internalizing disorders have high comorbidity with SUD. In terms of SUD due to illicit substances in the general population, 23% also have generalized anxiety and 21% have depression. 13 Other work has shown that SUD and Post-Traumatic Stress Disorder (PTSD) are highly comorbid 14 ; indeed, treatment-seeking individuals with SUD have a 36% to 50% lifetime prevalence rate of PTSD. 15 Approximately half of individuals with Alcohol Use Disorder (AUD) also have anxiety or depression (eg, Alegría et al 16 -McGovern et al, 17 and Vasilieva et al 18 ). Those with SUD may use alcohol 19 or illicit substances15,20 in an effort to cope with their internalizing disorder symptoms. Although there has been significant research on the relationship between internalizing disorders and SUD prevalence in community and outpatient settings, there are few studies that have examined this relationship in the inpatient setting. Thus, the present research will explore the relationship between specific internalizing disorder symptoms and SUDs in inpatients hospitalized with complications from their SUD.
Predictors of SUD severity
Various predictors, such as prior treatment, have been associated with increasing SUD severity. Patients with greater SUD severity had better 6-month outcomes with inpatient treatment rather that outpatient treatment, and those with lower levels of SUD severity had better outcomes with outpatient treatment. 21 In addition, a recent study observed that feelings of low self-esteem and anxiety symptoms were predictive of substance use severity. 22 It is possible that if individuals experience temporary relief from their anxiety through substance use, then as one’s anxiety increases, their reliance on substances as an attempt to cope may also escalate. Similarly, other work has shown that individuals with internalizing disorders that have comorbid SUD experience greater disease and symptom severity than those without SUD. 23 Although prior research suggests that certain socioeconomic factors and anxiety may exacerbate SUD severity, there has been surprisingly little research aimed at systematically characterizing the relationship between different internalizing conditions and SUD severity. Moreover, to our knowledge, this relationship has not been examined in the hospital setting.
SUD severity, mental health, and treatment-seeking trends
Those with SUD and at least one comorbid mental health disorder may have an increased probability of obtaining treatment compared to those without comorbidities. Still, only 31% of those with a mental health disorder and SUD receive any substance use treatment. 24 Additionally, prior research shows that, among those with AUD, anxiety symptoms may be a driving factor to seek treatment for alcohol use disorder. 25 Further research has demonstrated that severity of mental illness may be a predictor for treatment. 24 A review of factors predicting substance use treatment outcomes concluded that one of the strongest predictors for substance use outcomes is mental health severity, over and above demographic factors. 26 However, only a small number of those that do receive treatment are provided with treatment for both SUD and mental health. 24 This is important because mental health treatment alone with co-occurring disorders may be ineffective. 27 Indeed, a recent qualitative study examined the unique factors of SUD treatment-seeking behavior among those with SUD compared to those with SUD and a comorbid anxiety disorder. Those with comorbid SUD and anxiety were more likely to minimize their SUD and reported not having sufficient information and SUD treatment options. 28 This work suggests that those with comorbid SUD and mental health conditions may have unique treatment needs and barriers.
Greater “recovery capital” may facilitate an individual’s ability to overcome such recovery barriers. Recovery capital refers to the amount of personal and environmental resources that an individual possesses in order to initiate and maintain recovery. 29 Recovery is defined as reductions in substance use, improvement in biopsychosocial functioning, and remission from SUD.30,31 Recovery capital includes such factors as social support, physical well-being, psychological well-being, housing, and employment.32,33 Greater recovery capital is associated with reduced addiction severity and better treatment outcomes, including sustained recovery.29,34 There are clear social inequalities in recovery capital resources. Recovery capital factors correlated with initiation and retention in SUD treatment include race, gender, and employment. 35 In fact, those that are Caucasian, male, and had a higher employment composite score attended more sessions and remained in treatment longer. 35 Furthermore, older age, higher levels of education, female gender, lower pretreatment substance use severity, and being Caucasian were linked with better outcomes. 26 This emphasizes the importance of transitioning SUD treatment to a more accessible, individualized approach that focuses on the patients’ comorbid conditions as well as their cultural, gender-specific, and vocational needs.
Current study
There is a lack of data regarding patient predictors for substance use severity, particularly among patients hospitalized with medical complications from SUD, who tend to have severe, long-term SUD. It is important to understand factors associated with severity of substance use so that clinicians can identify those at highest risk and take appropriate preventative measures. Moreover, prior research suggests that SUD patients with comorbid mental health conditions may have unique challenges and needs in treating their SUD, 28 so it is important to understand treatment seeking behavior among those with these comorbidities. The purpose of the present investigation was twofold. The primary objective was to characterize the relationship between specific internalizing disorders (Major Depressive Disorder [MDD], Generalized Anxiety Disorder [GAD], and PTSD) and addiction severity, including history of past SUD treatment, among patients admitted for medical complications related to SUD. The secondary purpose was to (1) examine associations between patient demographic characteristics and addiction severity in this population and (2) explore the relationship between specific internalizing disorders and SUDs caused by a particular substance, including alcohol, opioids, methamphetamine, and cocaine.
Methods
Participants
The sample was comprised of patients hospitalized due to SUD-related medical complications, such as endocarditis, cellulitis, alcoholic pancreatitis, and alcoholic cirrhosis, at a large tertiary care and teaching hospital in South Carolina, USA between April 2018 to February 2020. Patients were eligible for study participation if they were admitted as an inpatient to a general hospitalist, infectious disease, or medical teaching services team and were identified by their primary healthcare provider as having a SUD. Exclusion criteria included being less than 18 years of age, unable to provide informed consent (due to intubation, confusion, etc.), admitted for marijuana use only, unable to speak English, or pregnancy.
Participants (N = 200) ranged in age from 20 to 65 years (M = 41.97, SD = 10.23). The majority were Caucasian (80.5%) with 15% African American, 2.5% Hispanic, and 2% Other (Asian, American Indian, etc.). With regard to substance use, 26.5% were polysubstance users, 58.5% had Alcohol Use Disorder, and 34.5% had Opioid Use Disorder (OUD), 30% had a SUD due to methamphetamine, and 15.5% had Cocaine Use Disorder. Participants lived primarily in the Upstate (northwest) region of South Carolina. Additional participant characteristics are provided in Table 1.
Demographics and participant characteristics for the overall sample.

Measures
Demographic information
Information regarding participant age, gender, level of education (in years), marital status, and employment status were obtained through self-report.
Mental health and medical information
Duration of substance use and history of comorbid mental illness (MDD, GAD, and PTSD) based on the DSM-5 checklists were obtained through self-report. SUD diagnosis, substance(s) causing the patients’ SUD, and medical insurance status (insured vs. uninsured) were obtained through chart review. No patients in our sample had a history of schizophrenia.
Prior SUD treatment
Information regarding whether patients had ever been treated in an inpatient (residential or psychiatric facility) or outpatient setting (non-residential programs, clinic visits for SUD care, or regular SUD therapy) for SUD and whether they were actively involved in a recovery program was obtained through self-report.
Addiction severity
The 10-item Drug and Alcohol Screening Test (DAST-10 36 ), was employed to measure substance use severity over the past year. Higher scores represent greater severity. We note that for all questions in this measure, we asked participants about drug or alcohol use, rather than simply drug use. An example question would be “Have you neglected your family because of your drug or alcohol use?” Scores ranged from 0 to 10 with higher scores indicating greater addiction severity.
Procedure
The study was approved by the hospital’s institutional review board before procedures were implemented. Eight medical students were trained to administer informed consent, and 4 medical students were responsible for administering patient interviews for data collection across the study period. Informed consent training for medical students entailed the following: (1) reading through the study protocol and informed consent document; (2) viewing a National Institute of Mental Health (NIMH) video 37 on the elements of a successful informed consent; (3) observing the study PI administering informed consent to a study participant; (4) practicing mock informed consent session with the study PI and the study physician 3 times; (5) being observed giving informed consent by the study PI or study physician. Similarly, study interviews training entailed observing the study PI performing mock interviews with other medical students twice, followed by practicing mock interviews 3 times, and then being observed doing the interview with a study participant.
The majority of study participants were part of a longitudinal clinical trial examining recovery coaching. Therefore, all study participants had an interest in receiving help for their SUD from a peer recovery coach. However, the data for this study was collected solely to characterize the mental health and demographic characteristics of patients hospitalized with SUD. The study physician systematically screened inpatient unit charts weekly to identify potential study participants who had been diagnosed with a SUD by their primary provider. Patients identified through chart review were informed by the study physician or a trained medical student to gauge patient interest in participating in the study. Interested patients were approached by study physician who mad a SUD diagnosis through clinical determination. Trained medical students then verified SUD diagnosis by administering the 13-item Addiction Severity Index and then screened patients on all other inclusion/exclusion criteria (ASI-Lite).38,39 If necessary, the patient’s nurse was contacted to verify that the patient was cognitively able to provide informed consent in their professional opinion. Trained medical students administered informed consent and conducted the interviews, including survey measures. The medical students then recorded all relevant information from the patient’s chart into the study’s RedCap database.
Data analysis
Inter-rater reliability analyses were first computed to assess whether they were differences in addiction severity scores and mental health diagnosis proportion for patients interviewed by the 4 different medical students. A repeated measures analysis was first conducted to compare patients’ DAST-10 addiction severity scores between each interviewer. Results showed that there was no significant difference between interviewers (P = .99). To examine inter-rater reliability for mental health disorder diagnoses, we performed Multiple Proportions Test for each disorder. There were no significant differences between patients’ proportion of diagnoses obtained from each medical student for any of the 3 mental health conditions (MDD, GAD, PTSD; Ps > .30). The average addiction severity scores and proportions of diagnoses obtained by each medical student are shown in Supplemental Table S1.
For all analyses comparing mental health diagnoses, each diagnosis (MDD, GAD, and PTSD) was binary coded (Yes = 1, No = 0) and included as separate predictors. To address the relationship between the effect of specific internalizing mental health disorders on addiction severity, a multiple linear regression was performed with MDD (Yes vs No), GAD (Yes. vs No), and PTSD (Yes vs No) predicting DAST-10 scores. Based on prior research findings,21,26,35 the multiple linear regression controlled for the following factors that have been associated with SUD severity or treatment outcomes: age, gender, years of education, years of having a SUD, employment status (coded as Employed = 1, Unemployed/Disabled = 0), marital status (coded as 1 = married, 0 = single, divorced, or widowed), medical insurance status, history of mental illness, and history of prior in/outpatient treatment. It should be noted that one response for prior treatment and recovery and 5 marital status responses are missing from the data.
To compare the effects of each mental health diagnosis (MDD, GAD, PTSD) and SUD type (AUD, OUD, MUD, CUD) on prior history of inpatient or outpatient SUD treatment (coded as Yes vs No), a binary logistic regression was conducted. Separate regressions for inpatient and outpatient treatment were also performed to provide a more fine-grained analysis of the relationship between mental health, SUD type, and treatment history.
As an exploratory analysis, we further sought to understand whether a particular mental health disorder was more or less likely to be associated with a SUD caused by a particular substance. To examine these potential associations, we conducted 3 separate logistic regressions with each internalizing mental health diagnosis predicting AUD, OUD, or Methamphetamine Use Disorder (MUD). The sample size for Cocaine Use Disorder (n = 31) was too small to make comparisons. If the omnibus test was significant, planned comparisons among those with the mental health condition predicting the substance examined was then performed.
Results
Multiple linear regression with internalizing mental illness predicting addiction severity
The overall model of demographic factors predicting addiction severity was significant, R2 = .14, F(11, 185) = 2.71, P = .003. Results showed that MDD (P = .69) and PTSD (P = .69) were nonsignificant, but GAD was a significant predictor of DAST-10 scores (β = .21, P = .019). Results indicated that patients with GAD (M = 6.68, SD = 2.97) had greater addiction severity compared to those without GAD (M = 5.41, SD = 3.34). Further sub-analyses by SUD type suggested that this effect may be driven by those with an alcohol-related SUD. Within patients who had AUD, those with GAD (M = 4.93, SD = 3.15) had higher addiction severity scores than those with AUD but no GAD (M = 3.30, SD = 2.95), t(86) = −2.52, P = .014, d = 0.53. However, among patients with SUD due to other substances or polysubstance use, there was no significant difference in addiction severity scores between those with and without GAD (P = .27). In terms of the patient characteristics covariates, regression results indicated that Insurance status (β = −.20, P = .006) predicted addiction severity. Prior history of treatment was a marginally significant predictor (β = .14, P = .07). No other demographic predictors were significant (Ps >.20). Follow-up analyses showed that those who have medical insurance (M = 5.20, SD = 3.42) had lower addiction severity scores than participants without insurance (M = 6.74, SD = 2.88). Regression results are reported in Table 2.
Regression results with internalizing mental illness predicting addiction severity.

Abbreviations: GAD, generalized anxiety disorder; MDD, major depressive disorder; PTSD, post-traumatic stress disorder.
History of treatment includes both inpatient and outpatient treatment.
Logistic regression with internalizing mental illness and SUD type predicting prior treatment
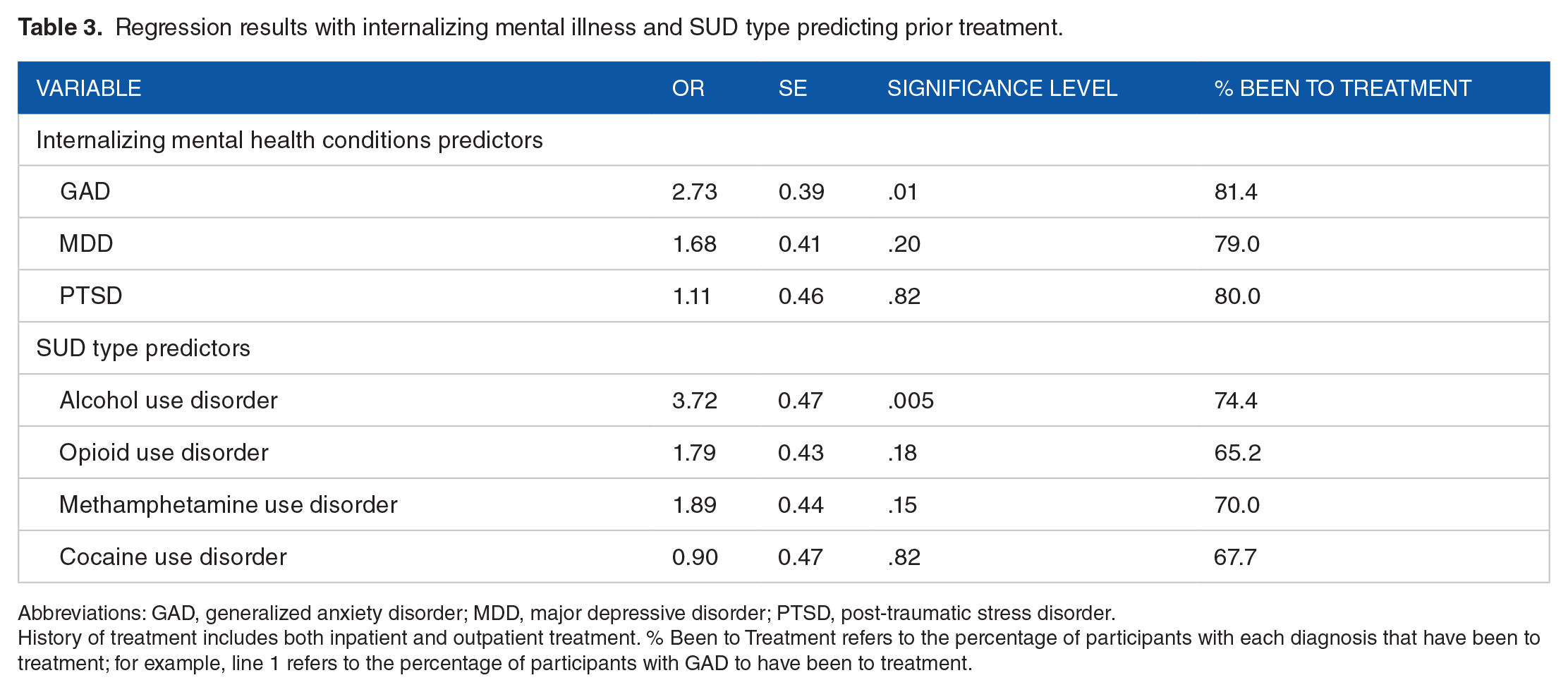
The logistic regression model with internalizing mental health conditions and SUD types predicting combined treatment (either outpatient or inpatient) was significant (χ2 = 28.76, P < .001). Results revealed that GAD (odds ratio [OR] = 2.73, P = .01) but not MDD (P = .20) or PTSD (P =.82) predicted past history of either inpatient or outpatient treatment. Among those with GAD, 81.4% had previously been to treatment compared to only 53.1% of those without GAD. For SUD type, those with AUD were less likely to have been to treatment (OR = 3.72, P = .005). Among those with AUD, 74.4% had previously been to treatment compared to 58.8% of those without AUD who had been to treatment. None of the other individual SUD types predicted past history of treatment (Ps > .10).
Separate regressions for inpatient and outpatient treatment were performed next. Results showed that GAD was associated with increased likelihood of past inpatient (OR = 3.47, P = .001) but not past outpatient (OR = 1.34, P = .41) treatment. AUD was associated with increased likelihood of both past inpatient OR = 3.53, P = .003) and outpatient OR = 2.90, P = .01) treatment. Table 3 shows the logistic regression results.
Regression results with internalizing mental illness and SUD type predicting prior treatment.
Abbreviations: GAD, generalized anxiety disorder; MDD, major depressive disorder; PTSD, post-traumatic stress disorder.
History of treatment includes both inpatient and outpatient treatment. % Been to Treatment refers to the percentage of participants with each diagnosis that have been to treatment; for example, line 1 refers to the percentage of participants with GAD to have been to treatment.
Logistic regression analyses examining the relationship between SUDs and mental health
The omnibus test from the logistic regression indicated that a significant likelihood difference between PTSD (Yes vs No) and OUD (Yes vs No) groups was present. The follow-up planned contrast examining whether those with PTSD were more or less likely to have OUD indicated that the likelihood of having both PTSD and OUD was 30% and the likelihood of having PTSD but not having OUD was 22%; this difference did not reach the level of significance, however (P = .258). Instead, another planned contrast showed that 70% of patients with OUD did not have PTSD, while 30% of those with OUD also had PTSD (X 2 (1, N = 69) = 10.57, P = .001). All other omnibus tests comparing Mental Health Diagnosis with each of the SUD types were nonsignificant.
Discussion
This study sought to examine the relationship between (1) internalizing disorders and (2) patient characteristics on addiction severity in hospitalized SUD patients. The results demonstrated that individuals with GAD had greater addiction severity and were more likely to have been to prior inpatient treatment. The relationship between GAD and addiction severity was specific to those with AUD; among AUD-only patients, those with GAD had higher addiction severity scores than those without GAD, but there was no significant relationship between addiction severity scores and GAD for other SUD types. These finding suggest that GAD may exacerbate AUD severity.
A second key finding was that specific internalizing disorders and SUD types are associated with prior history of addiction treatment. In terms of internalizing disorders, results showed that those with GAD were more likely to have been to inpatient addiction treatment previously. Similarly, those with AUD were more likely to have been to treatment—both inpatient and outpatient—compared to those with SUD types other than AUD. It is possible that those with GAD have a strong need for intensive inpatient treatment services because they have greater addiction severity. Thus, GAD represents a predictor of both heightened addiction severity, particularly among those with AUD, and greater likelihood of seeking intensive recovery treatment services.
In terms of participant characteristics, lack of medical insurance was associated with greater addiction severity. This may be due to early intervention and recognition of those with SUD for those with medical insurance, and thus highlights the importance of community support and outreach programs. It is also possible that those with medical insurance may fall into a higher socioeconomic status bracket, which has been associate with better recovery outcomes, but this information was not obtained as part of this study. However, we note that employment status was not associated with addiction severity in this sample. No other factors, including marital status, years of SUD, years of education, and gender, were significantly predictive of addiction severity in this sample. It is also possible that those with less severe addiction are more likely to be higher functioning enough to seek out health insurance.
As an exploratory analysis, we examined whether certain mental health conditions were more or less likely to co-occur with specific SUD types. A significant association between PTSD and OUD was observed such that a greater proportion of patients with OUD did not have PTSD compared OUD patients with PTSD. Other estimates have shown that 41% of individuals with OUD have a lifetime history of PTSD.40,41 Thus, it is possible that rates of OUD and PTSD were lower in the inpatient sample in the present study than in the general population. Overall, however, the present study does not find strong evidence for an association between any particular internalizing mental health condition and increased likelihood of comorbidity with specific SUD types. In other words, the proportion of patients with MDD, GAD, and PTSD, was not higher in a SUD caused by any one particular substance.
This work emphasizes the high rate of the comorbidity between mental health conditions and SUD. Indeed, two-thirds of participants in our inpatient sample had an internalizing mental health condition, which is a higher rate than reported from community samples. 13 Hierarchical models of psychopathology suggest that this association between internalizing disorders and Substance Use Disorders may be explained by one’s general factor of psychopathology (“p factor”), or the shared variance among internalizing and externalizing disorders. 42 Certain neurocognitive, impulsivity, distress, and social adversity risk factors are associated with the p factor and contribute to overlap in internalizing and externalizing symptoms. Other models, such as the secondary psychopathology model, suggest that anxiety symptoms arise in response to withdrawal symptoms; repeated substance use triggers the onset of anxiety in predisposed individuals, such as those with a high p factor. Moreover, as a consequence of repeated substance use, negative affect symptoms can occur also, leading to depressive symptoms. 43 Indeed, one of the primary study findings is that those with comorbid AUD and GAD showed greater addiction severity than those with AUD but no GAD. Thus, GAD may be a risk factor for advanced alcohol-related complications. One explanation for this association may be that those with anxiety symptoms may be more likely to self-medicate with depressants, increasing their reliance on alcohol. 44 Paradoxically, however, substance use as self-medicating or coping strategy tends to worsen mental health symptoms in the long-run. 45 This finding is in line with past research suggesting that GAD management is a key issue that needs to be addressed in SUD treatment or other healthcare settings. 22 Prior work suggests that those with comorbid SUD and internalizing mental health conditions report feeling more committed to their recovery efforts when they receive treatment that is tailored to addressing both their addiction and internalizing symptoms. 28 Therefore, screening for symptoms of depression and anxiety and referral to treatments or programs that can effectively address both comorbidities may be vital for improving patient health in this population.
Limitations
Though the study findings demonstrate a strong relationship between internalizing mental health conditions and AUD severity, the conclusions about internalizing mental health conditions and SUD due to other substances should be generalized with caution. Though overall sample sizes were reasonable, the sample size for SUD due to methamphetamine and cocaine users in the population was very low. Therefore, more research on the relationship between mental health conditions and methamphetamine and cocaine users hospitalized with SUD complications is needed. It should be noted that it is possible that some patients were still experiencing mild withdrawal and were feeling acutely ill, which has potential to bias self-report responses. While it is possible that withdrawal may also account for some anxiety-related symptoms, DSM-5 diagnosis for GAD assesses symptoms over the past 6 months, and thus, it is unlikely that results for GAD were significantly impacted by withdrawal symptoms.
Furthermore, all patients in our sample were interested in receiving help with recovery services for their SUD. Hospitalized SUD patients who are not interested in recovery assistance may present differently. A further limitation to the study conclusions is that socioeconomic factors and homelessness status were not measured in this study, and these factors may be associated with SUD severity. Future work should consider incorporating these factors and approaches into the study design.
Conclusion
Inpatients hospitalized for SUD-related complications experience significant physical health consequences from long-term substance use. This study showed that GAD, over and above other internalizing conditions, may be a factor that is particularly predictive of greater addiction severity in patients hospitalized for SUD complications, particularly those with AUD. In this patient population, two-thirds of patients with SUD were not only coping with physical health complications but also the burden of internalizing mental health problems as well—a substantial challenge that could be aided by tailored recovery service or treatment resources. This study also demonstrated that being insured may provide individuals with greater “recovery capital”—or resources to find recovery. In contrast, comorbid anxiety may be a particularly prevalent indicator of severe SUD problems. Thus, screening for and addressing anxiety symptoms in this population may potentially be beneficial for improving SUD outcomes in this population.
Supplemental Material
sj-docx-1-sat-10.1177_11782218221115583 – Supplemental material for Examining Internalizing Mental Health Correlates of Addiction Severity in Patients Hospitalized With Medical Complications From Substance Use Disorder
Supplemental material, sj-docx-1-sat-10.1177_11782218221115583 for Examining Internalizing Mental Health Correlates of Addiction Severity in Patients Hospitalized With Medical Complications From Substance Use Disorder by Bryana N Baginski, Kaileigh A Byrne, Lauren Demosthenes and Prerana J Roth in Substance Abuse: Research and Treatment
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through the Health Sciences Center at Prisma Health Transformative Research Seed Grant Award and the Prisma Health-Upstate Addiction Research Collaborative.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KAB, LD, and PJR led funding acquisition for the study. All authors conceptualized the study. BNB and PJR were responsible for data collection. KAB. oversaw the study. BNB and KAB performed data analysis and wrote the manuscript.
Informed Consent
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000. Written informed consent was obtained from all patients for being included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.