
Abstract
Objective:
To examine psychotropic medication prescription practices in federal Canadian penitentiaries.
Method:
468 files were drawn from a purposive sample of thirteen Canadian federal institutions representing the five regions, different security levels, and male and female designated facilities. Information on the names of all psychotropic medications prescribed, indications for use, dosage, frequency, and route of administration was retrieved. Designation of approved or off-label use of medications was determined by consulting: (1) the Health Canada (2016) Drug Product Database, (2) the Canadian Compendium of Pharmaceuticals and Specialties 2016, and (3) the American Hospital Formulary Service Drug Information 2016. Prescription rates were examined by gender, Indigenous ancestry, drug class, institutional infractions, and current offence.
Results:
36.2% of prescriptions for psychotropic medication were coded as ‘off-label’. Anxiolytic/hypnotics drugs were the psychotropic drugs most commonly used for off-label purposes. There were no differences in the prevalence of approved versus off-label prescriptions based on Indigenous ancestry or gender, and no pattern of elevated off-label prescription practices for offenders involved in institutional misconducts or those sentenced for the most serious crimes.
Conclusions:
The rates of prescribing ‘off-label’ psychotropic medication are not elevated relative to other correctional settings or to rates cited in Canadian surveys conducted in the community.
International research shows that the prevalence of psychotropic medication use is 2 to 6 times greater among prison inmates compared with the general population and highest among women offenders. 1 –3 In his Annual Report 2013–2014, the Correctional Investigator of Canada expressed concern over the frequency of psychotropic medication use in Correctional Service of Canada (CSC) institutional facilities, in particular, among women inmates. 4 Anecdotal and case reports about the unapproved, “off-label” use of psychotropic medications to control inmates’ behaviour have raised public concerns about the well-being of inmates and the ethical and legal ramifications of prescription practices for this vulnerable population. 5 –7 It has been noted that prescribing psychotropic medications in correctional settings that prioritize security and institutional control is subject to criticism that the medication could be used as a punitive or a control strategy rather than solely to address therapeutic goals. 6
Prevalence of Psychotropic Medication Use in Prisons
A 2015 survey conducted on the prevalence of psychotropic medication prescriptions in federal Canadian prisons found that about 30% of inmates had active prescriptions for psychotropic medication compared with about 8% in the general Canadian population. 8 The prevalence of active prescriptions for psychotropic medication was especially high among incarcerated women (45.7%) compared with incarcerated men (29.6%), and women were also more likely to have more than 1 active prescription for a psychotropic medication. There were no substantive differences in the prevalence of active prescriptions for psychotropic medication between Indigenous and non-Indigenous inmates.
International research reports a higher prevalence of psychotropic medication use among prison inmates. A 2014 national report on mental health care in U.S. jails and prisons found that between 25% and 60% of inmates received a psychotropic medication compared with 20% of the general population. 2,9 A study conducted in prisons in the east of England found that 19.6% of incarcerated men and 44.0% of incarcerated women had an active prescription for a psychotropic medication, a proportion that is 5 to 6 times greater than found in community samples. 5 In a Spanish study, 20.5% of inmates received psychotropic medication, compared with about 8% of the general population. 3 A 2012 census of prisoners in Western Australia reported that 21% were taking a psychotropic medication, double the proportion reported in the general population. 10 This high frequency of prescriptions for psychotropic drugs reflects the international findings of the elevated prevalence of serious mental disorders among incarcerated populations. A system review by Fazel et al. of surveys in Western countries, for example, determined that prisoners were 2 to 4 times more likely to suffer from a psychosis or major depression than the general population 11 ; his updated meta-analysis including surveys from low-income countries found a similarly higher prevalence of psychosis and depression among inmates. 12 In Canada, a recent comprehensive survey of incoming offenders found that 70% 13 of the men met criteria for a current mental disorder compared with 10% cited in the Canadian Community Survey, 14 although it should be noted that these estimates for offenders are inflated by high rates of substance use and personality disorders in correctional populations.
Approved and “Off-Label” Use of Psychotropic Medication
Health Canada is responsible for authorizing all drugs marketed for sale in Canada. The “label” (a detailed product monograph, as well as product packaging) identifies the population group for which the drug is to be used, the indication(s) the drug is used to treat, the recommended dosages, and the route of administration. 15 Once approved by Health Canada, the drug is officially approved for use only according to its label. “Off-label” is the use of a drug in a population for an indication or at a dosage or method of administration for which it has not been approved and which is not described by the drug label. 16 Nevertheless, off-label prescription practice is common, especially in paediatrics, psychiatry, among the elderly, in transplant medicine, in HIV/AIDS treatment, and in cancer treatment. International studies report that as many of 30% to 50% of prescriptions for psychotropic medications are for off-label use. 17 For example, in Canada, a Quebec study found that psychotropic medications were prescribed off-label by primary care physicians between 26% and 67% of the time. 18 A report published by the Royal College of Psychiatrists (in the United Kingdom) based on a review of published research concluded that as many as 50% of adult psychiatric patients are prescribed at least 1 off-label medication. 19 In a French study, 39.8% of prescriptions for psychotropic medications issued in a psychiatric hospital were for off-label uses. 20 A study of Medicaid prescriptions in the state of Georgia in the United States found that more than two-thirds of psychotropic medication prescriptions were off-label. 21
Reason for Current Study
There is anecdotal evidence of the off-label use of psychotropic medication among prison inmates, including the use of quetiapine (Seroquel) as a sedative to control inmates, buprenorphine, and the selective serotonin reuptake inhibitor class of drugs used in the treatment of addictions and divalproex sodium and oxcarbazepine to treat aggression. 22 –25 A systematic review of studies of psychometric medication prescribing practices in prison settings reported that polypharmacy was common, along with high doses, long duration of medication use, poor documentation, and infrequent monitoring of patients. 26
This study investigated concerns about the prescription of psychotropic medications for federal inmates in a sample of CSC institutions. The study assesses the proportion of medications prescribed by physicians for “approved” uses to treat mental health problems and compares it to the proportion of medications prescribed by physicians for “off-label” use among men and women offenders. The research includes an analysis of demographic, criminal history, substance abuse, and institutional behaviour correlates of approved and off-label psychotropic medication prescriptions and a comparison of the prevalence of approved and off-label psychotropic medication prescriptions in the study sample compared with estimated prevalence in the general Canadian population. Identifying patterns in the prescription of off-label psychotropic medications for Canadian federal offenders would point to where steps need to be taken to reduce the reliance on psychotropic medication, particularly off-label use, and enhance the evidence base currently supplied by qualitative research that has relied on offender interviews. 6
Method
Ethical Review
Under the Privacy Act, paragraph 8(2)(j), CSC is permitted to compile health data for statistical use as long as the presentation of the information guarantees confidentiality and the information is used in a manner consistent with the purpose for which the data were collected. An anonymized data set was prepared and provided to the lead researcher by CSC. As advised by the lead researcher’s university ethics administrator, under Sec. 2.4 of the Tri-Council Policy Statement Ethical Conduct for Research Involving Humans (2014), 27 REB review is not required for research that relies exclusively on secondary use of anonymous information as long as any data linkage or dissemination of results does not result in generating identifiable information.
Participants
The CSC administers the sentences of all offenders sentenced by the courts to 2 or more years. Beginning in March 2016, a mixed-methods sampling design was employed to ensure representation of each of the major administrative features and inmate groups in the federal prison system. 28 In the first stage, a purposive sample of 13 of 43 federal institutions encompassing 28% of the total inmate population was drawn, representing each of the 5 regions in the CSC, different security levels, and men’s and women’s facilities, with all 5 women’s institutions included to ensure a sufficient number of cases for comparative analysis. In the second stage, a list of all inmates at each selected institution with 1 or more active prescriptions for a psychotropic medication was provided by each of the 5 regional pharmacies. From this list, a systematic probability sample was drawn by selecting by random start every fifth name, and the health care file for each name selected was retrieved and reviewed. 29,30 All information on the name of the psychotropic medication(s) used, indication(s) for use, dosage, frequency, and route of administration was recorded on a spreadsheet. Where a selected file was not available, or where the number of files selected at an institution was too few, additional files were systematically selected until a sufficient number of files (between 30 and 40) containing the required information was obtained at each institution. Data collection was completed on March 14, 2016.
The anonymized data on psychotropic medication prescriptions were provided by CSC to the principle researcher (first author) and were merged with additional data provided through the Offender Management System, the comprehensive electronic database on all federal offenders.
Administrative information linked to prescription practices included offenders’ date of birth, Indigenous ancestry, sentence length, admission date, major admitting offence, substance abuse assessment, and the Dynamic Factors Identification and Analysis–Revised Substance Abuse (DFIA-R) domain ratings, along with the number of charges for institutional misconducts.
The DFIA-R is a well-validated assessment of offender dynamic risk factors completed on all incoming offenders. Each need domain is rated on a 4-point scale, ranging from none to considerable. 31 Institutional misconducts are charges for behaviours within institutions that result in formal charges. Examples of major charges are fighting or possession of drugs, whereas a minor charge could be for disobeying an order or possession of unauthorized items. The final data set contained information for 468 individual inmate cases (295 men and 173 women, representing 12% of the total number of inmates included in the first-stage purposive sample selection and 3.5% of the total federal inmate population). Post hoc calculation of statistical power of the sample was 99.5% 32,33 based on an estimated population proportion of off-label use of pp = 0.30, inmate sample proportion ps = 0.40, α = 0.05, and n = 468.
Across the 13 institutions, 144 (30.8%) inmates self-identified as being of Indigenous ancestry (First Nations/Métis/Inuit), and 324 (69.2%) self-identified as non-Indigenous (white or otherwise).
Procedure
Approved or off-label use of psychotropic medication prescriptions was determined by consulting and comparing information from 3 main sources: (1) the 2016 American Hospital Formulary Service Drug Information (AHFS), 34 considered to be an evidence-based standard for drug information in institutional formulary environments, which also contains up-to-date information on scientifically supported off-label uses of medications. The AHFS is the formulary framework employed by the CSC. (2) Health Canada’s Drug Product Database, 35 which contains label and other information on all drugs approved for use in Canada. (3) The 2016 Canadian Compendium of Pharmaceuticals and Specialties (CCPS), 36 which contains detailed drug product monographs (labels) approved by Health Canada, along with additional clinical drug information. In addition, off-label uses of psychotropic medications were also checked against published research in PubMed 37 and MEDLINE 38 search engines and other web-based search engines, including WebMD. 39 For each prescribed medication, including dosage, route of administration, frequency, and indication for use, the lead researcher compared the information documented in the inmate’s health record with the approved or off-label use of the medication documented in the AHFS, Health Canada’s Drug Product Database, and the CCPS.
The published academic research literature was examined as an additional check on whether the prescribed medication, dosage, route of administration, frequency, and indication for use was identified as an accepted or off-label use. Where a discrepancy occurred between sources on whether a medication was used in an approved or off-label manner, the CCPS was taken to be the final authority on Canadian approved prescribing practices. Data were coded (0 = approved, 1 = off-label) for each individual inmate (N = 468) with a psychotropic medication prescription and for each prescription (range = 1-6). IBM-SPSS 24© was used to perform the statistical analysis. 40
Interrater reliability was assessed by comparing the coding of psychotropic medications by the lead research with that made by the psychiatrist member of the research team. A random sample of 40 cases already coded by the lead researcher was drawn from the final data set, and the psychiatrist member independently coded a total of 73 prescriptions for psychotropic medication as (0 = approved, 1 = off-label). The Kappa ( ) statistic
41
was computed for all prescriptions issued to the 40 inmates, with an overall percentage agreement between the 2 raters of 84.9%, and a Kappa statistic of (n = 73) = 0.63, P < 0.001, demonstrating a “substantial” level of agreement between the raters.
42
) statistic
41
was computed for all prescriptions issued to the 40 inmates, with an overall percentage agreement between the 2 raters of 84.9%, and a Kappa statistic of (n = 73) = 0.63, P < 0.001, demonstrating a “substantial” level of agreement between the raters.
42
Statistical Analysis
Tabular analysis of approved versus off-label prescriptions of psychotropic medications by subgroup comparisons based on gender, age, Indigenous ancestry, AHFS-defined pharmaceutical categories, indication for use, and criminal history variables including most serious offence on sentence, time served, institutional charges, and substance abuse need level (DFIA-R) was conducted, and the chi-square test was used to identify statistically significant subgroup differences in the distribution of approved versus off-label prescriptions. 43
Results
The distribution of approved and off-label prescriptions for psychotropic medication, by gender, age group, and Indigenous ancestry, is presented in Table 1. Data were missing for 49 prescriptions for which no indication for use was recorded. Missing data analysis (49/829 = 5.9%) demonstrated no significant association with the number and distribution of prescriptions used, χ2(10, N = 42) = 8.679, P = 0.563. Interrater reliability was substantial at 84.9%, agreement between the 2 rates, with a Kappa statistic of (n = 73) = 0.63, P < 0.001. We found that slightly more than one-third (36.2%) of psychotropic medication prescriptions were indicated for off-label use. There were no statistically significant differences in the distribution of approved versus off-label prescriptions for psychotropic medication by gender, age, or Indigenous ancestry. Similarly, no statistically significant differences were observed in the distribution of the number of prescriptions for psychotropic medications issued to individual inmates based on gender or Indigenous ancestry (Table 2). Rates of off-label prescriptions by offender indicated that about 50% of men and women and Indigenous and non-Indigenous offenders were prescribed an off-label psychotropic medication during the period examined in this study.
Approved and off-label prescriptions for psychotropic medication.
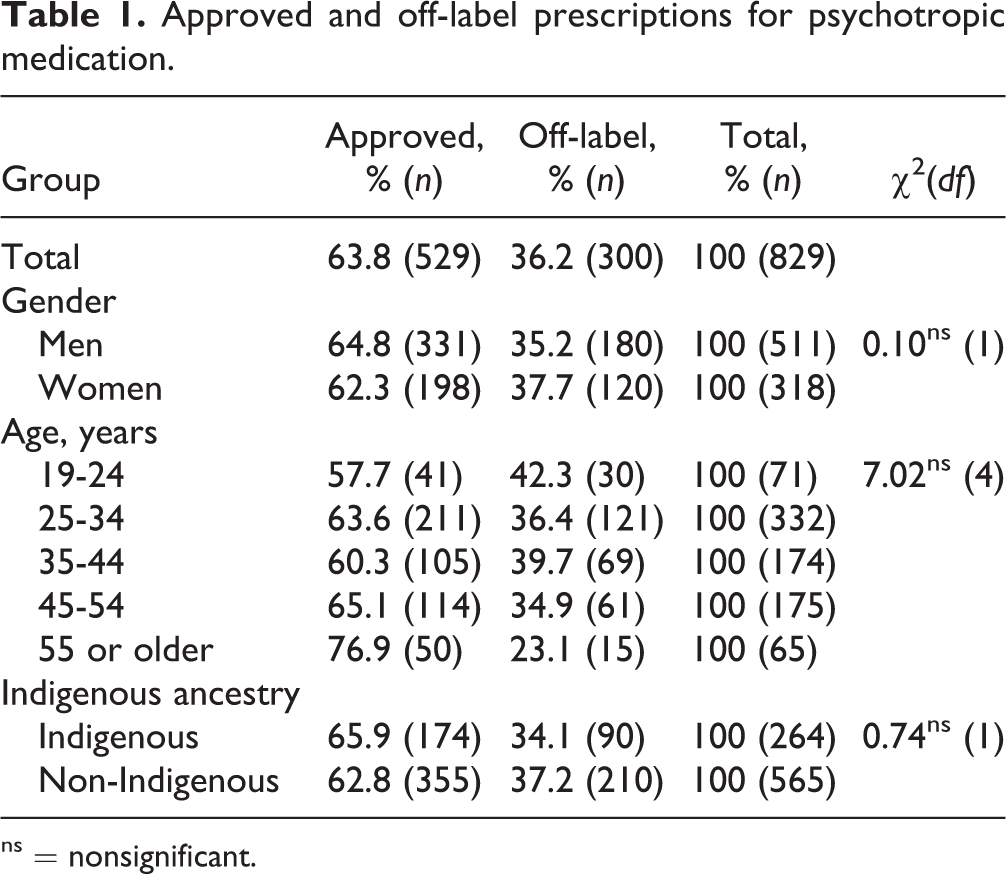
ns = nonsignificant.
Number of prescriptions issued for psychotropic medication by gender and ancestry.
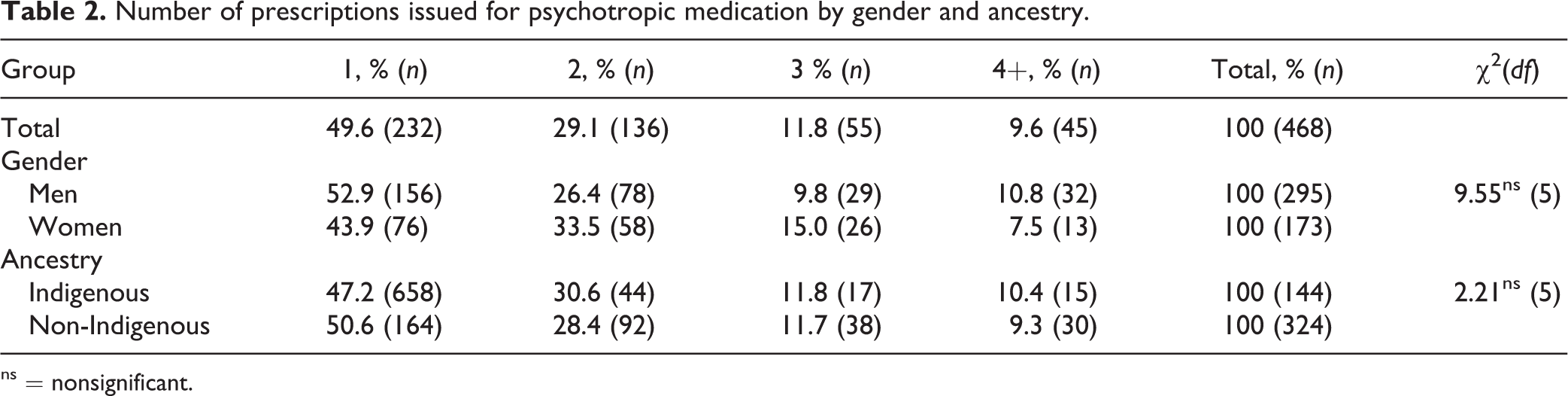
ns = nonsignificant.
The distribution of approved and off-label prescriptions for psychotropic medication according to the American Hospital Formulary Service (AHFS) 33 –defined drug class is presented in Table 3. There was a statistically significant difference, χ2(4, n = 827) = 55.49, P < 0.001, in the distribution of psychotropic medications by AHFS-defined drug class. More than one-half of prescriptions for antidepressant agents (62.2%) and antipsychotic agents (61.8%) were for approved uses. Similarly, central nervous system (CNS) stimulants prescribed to treat attention-deficit hyperactivity disorder (90.1%) and antimanic drugs used to treat bipolar disorder (71.0%) were prescribed predominantly for approved purposes. On the other hand, most prescriptions for anxiety/insomnia agents were for off-label use. The most commonly prescribed psychotropic medications were the antidepressants.
Rates of approved and off-label prescriptions for psychotropic medication, AHFS-defined categories (N = 827).
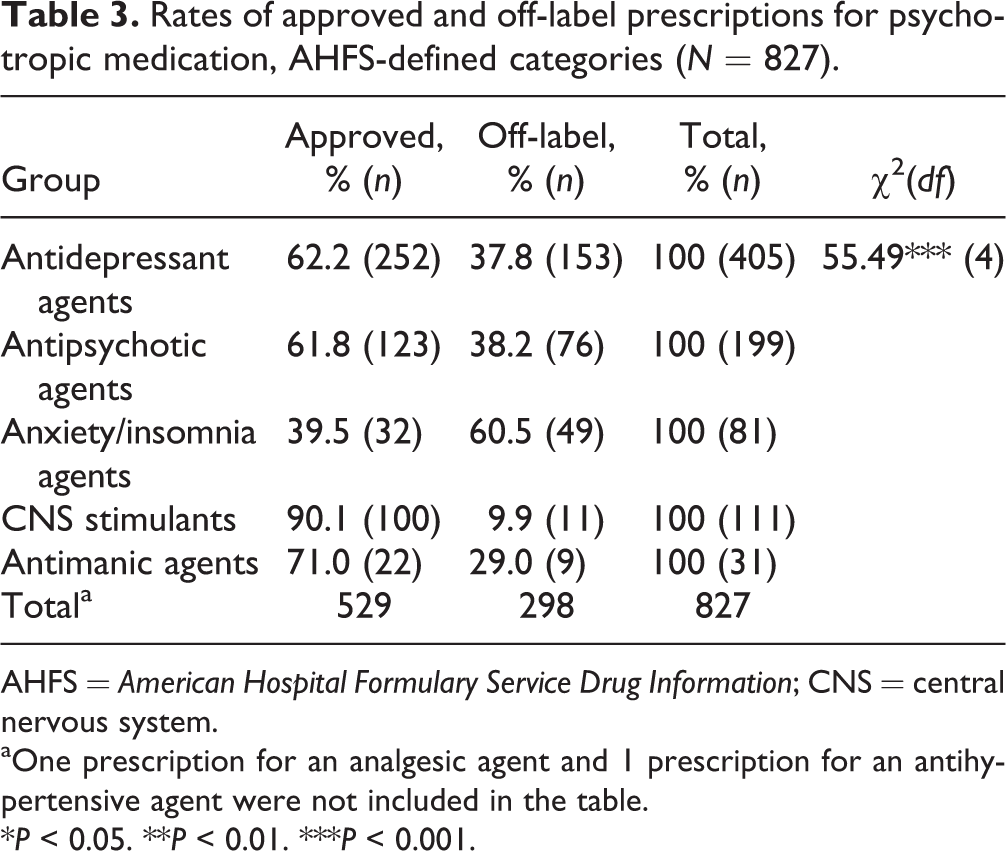
AHFS = American Hospital Formulary Service Drug Information; CNS = central nervous system.
aOne prescription for an analgesic agent and 1 prescription for an antihypertensive agent were not included in the table.
*P < 0.05. **P < 0.01. ***P < 0.001.
Approved and off-label prescriptions for psychotropic medication are broken down by indication for use, based on the Diagnostic and Statistical Manual of Mental Disorders (DSM)–5 classification categories, 44 in Table 4. Psychotropic medications prescribed for schizophrenia spectrum and other psychotic disorders, bipolar and related disorders, depressive disorders, and disruptive, impulse-control, and conduct disorders were used largely according to approved prescription guidelines. Sleep-wake disorders, however, have a very high rate of off-label prescription use (73.7%). Higher rates of off-label prescribing were also found in relation to anxiety disorders, trauma, and stressor-related disorders, substance-related and addictive disorders, and other mental disorders.
Approved and off-label prescription of psychotropic medication, by indication for use based on DSM-V classification.
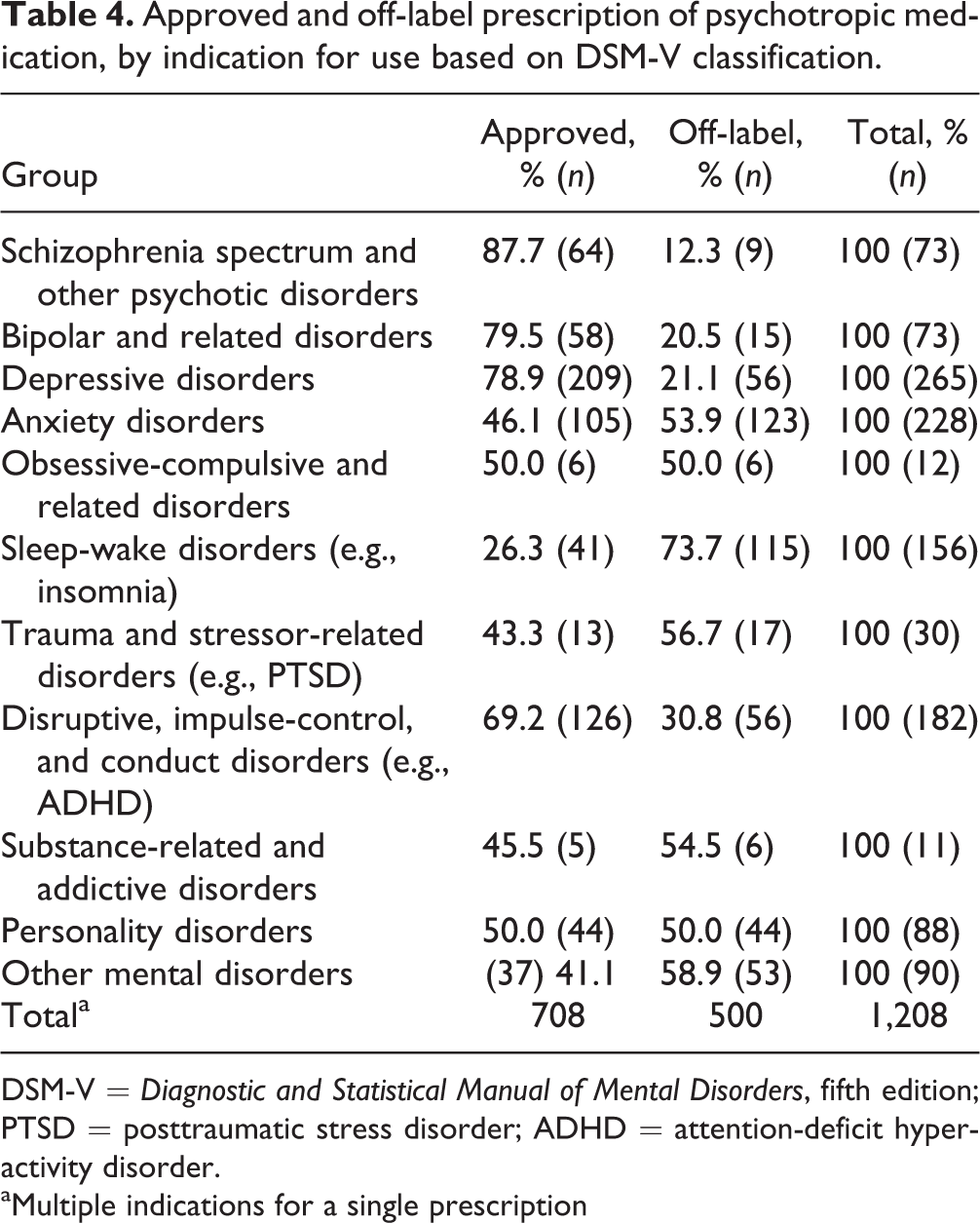
DSM-V = Diagnostic and Statistical Manual of Mental Disorders, fifth edition; PTSD = posttraumatic stress disorder; ADHD = attention-deficit hyperactivity disorder.
aMultiple indications for a single prescription
Comparisons of approved and off-label prescriptions for psychotropic medication by most serious offence and time served are presented in Table 5. We examined patterns related to time served because we considered that offenders may be particularly vulnerable to psychological distress during the early part of their sentence as they adjust to incarceration and that physicians could therefore prescribe medication to alleviate their distress. We did not, however, find a pattern related to time served. We did find a statistically significant relationship, χ2(7, n = 814) = 37.39, P < 0.001, between the current offence and the prevalence of approved or off-label prescriptions for medication, with offenders with the most serious and violent offences being more likely to have been prescribed psychotropic medication prescriptions for approved uses, while there was a higher prevalence of off-label prescriptions for offenders with nonviolent offences.
Approved and off-label prescriptions for psychotropic medication, by most serious offence, time served, institutional charges, and substance misuse need level on the DFIA-R.
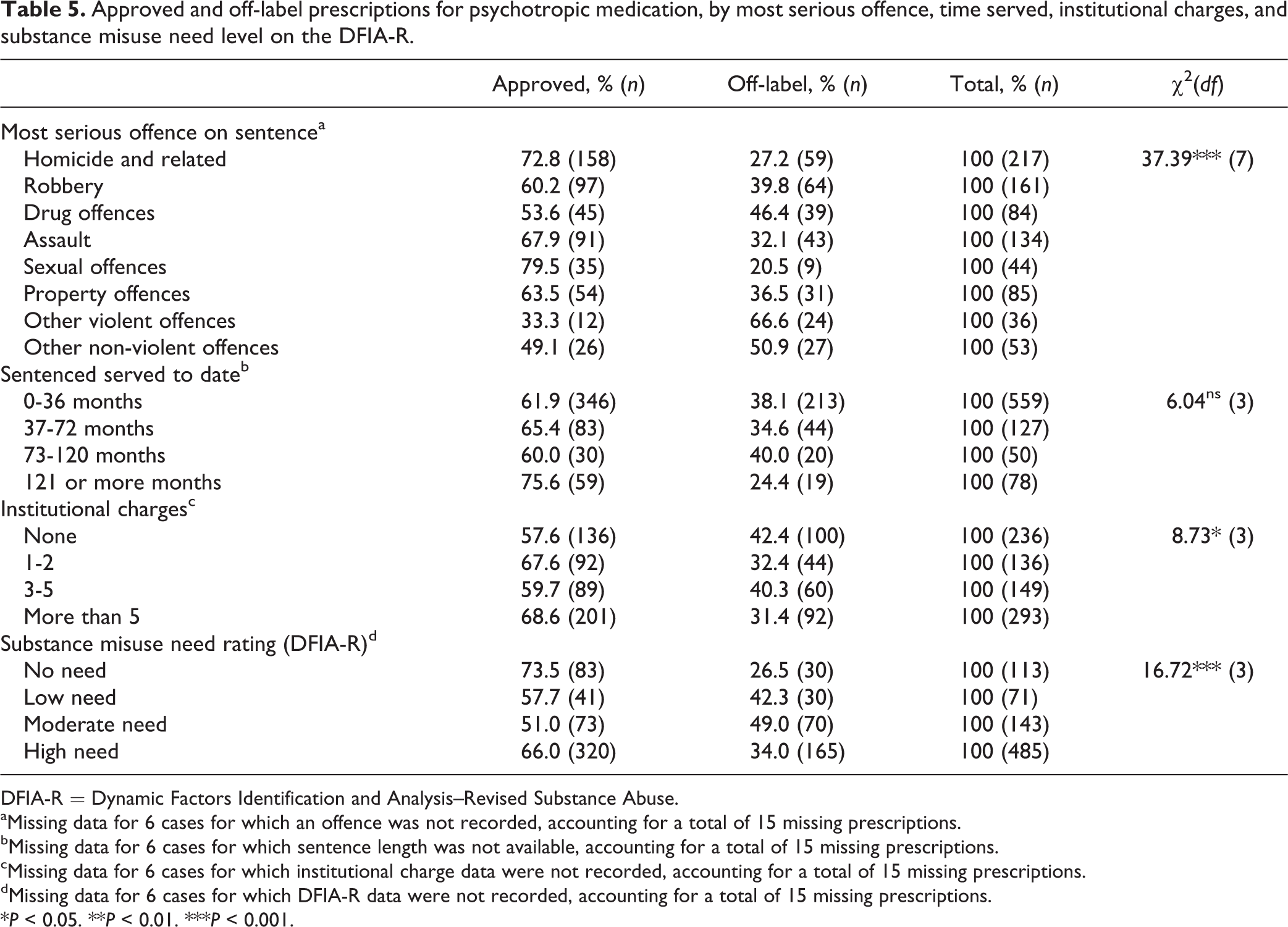
DFIA-R = Dynamic Factors Identification and Analysis–Revised Substance Abuse.
aMissing data for 6 cases for which an offence was not recorded, accounting for a total of 15 missing prescriptions.
bMissing data for 6 cases for which sentence length was not available, accounting for a total of 15 missing prescriptions.
cMissing data for 6 cases for which institutional charge data were not recorded, accounting for a total of 15 missing prescriptions.
dMissing data for 6 cases for which DFIA-R data were not recorded, accounting for a total of 15 missing prescriptions.
*P < 0.05. **P < 0.01. ***P < 0.001.
Approved and off-label prescriptions for psychotropic medication, by total number of institutional charges during the sentence and degree of substance abuse problems (DFIA-R substance abuse domain ratings), are shown in Table 5. There was a statistically significant difference, χ2(3, n = 814) = 8.73, P < 0.05, in the distribution of approved versus off-label prescriptions for psychotropic medication based on the number of institutional charges, with inmates with 1 to 2 charges or more than 5 charges having the highest rates of prescriptions for psychotropic medication for approved purposes. This finding does not suggest a consistent pattern of off-label prescribing for psychotropic drugs for offenders who evidence problematic behaviour while incarcerated, although prescription levels for psychotropic drugs, in general, were higher for this group. There was a statistically significant, although inconsistent, relationship, χ2(3, n = 814) = 16.717, P < 0.001, between inmates’ need level on the substance abuse domain and prescriptions for psychotropic medication; those with no need and those with the highest level of need were most likely to be prescribed psychotropic medications for an approved use, while those with low to moderate need ratings were somewhat more likely to be prescribed these medications off-label.
Discussion
Although there may be good reasons for the off-label use of psychotropic medications, there are also risks, including unknown adverse effects and potential legal liability coupled with concerns that medical practitioners may be pressured to prescribe psychotropic medications to maintain institutional peace and control. 45 There is, therefore, a strong need to undertake empirical research to determine the prevalence of approved and off-label medication use in the prison environment. The current study found that estimates of the prevalence of prescriptions for off-label uses of psychotropic medications were in the same order (36.2%) as were found in a Quebec study of primary care physician prescription practices in the general population 18 and somewhat lower than international estimates of off-label prescribing in general populations. This finding may reflect the increased scrutiny of prescribing practices that is observed in institutional environments (hospitals, institutions with psychiatric staff) compared with clinics and private medical practices. 46 An analysis by offender indicted that about 50% of men, women, and Indigenous offenders had been prescribed an off-label psychotropic drug; this rate is comparable to those cited in a review of published studies compiled by the Royal College of Psychiatrists in the United Kingdom. 19
We found no significant differences by gender, age, or Indigenous ancestry in the use of approved versus off-label prescriptions for psychotropic medication. However, a statistically significant difference was found in the distribution of approved versus off-label psychotropic medication prescriptions by AHFS-defined drug class, with antidepressant and antipsychotic agents and CNS stimulants and antimanic agents more likely to be prescribed for approved purposes only. The 5 most common indications for use of a prescribed psychotropic medication are (1) depressive disorders; (2) anxiety disorders; (3) disruptive, impulse control, and conduct disorders; (4) sleep-wake disorders; and (5) personality disorders. All these diagnoses are found at high prevalence rates among offender populations in both international 47 –50 and Canadian studies. 13,51,52
On the other hand, most prescriptions for anxiety/insomnia agents were for off-label uses, perhaps a reflection of the high prevalence of off-label prescribing observed for the DSM-5 diagnosis of sleep-wake disorders, echoing findings from other research. 6,53 Treatment protocols for individuals with histories of substance misuse caution about the potential detrimental pharmacologic effects related to the abuse and addiction potential of certain classes of drugs for this population. 54 Prescriptions for antianxiety medication, for example, with their potential sedating or euphorigenic effects, risk promoting the use of the medication higher doses than prescribed. 55,56 Physicians within CSC, therefore, may have applied alternative “off-label” protocols for the treatment of anxiety/insomnia to offset the risk of dependency and sedation.
We found no evidence that off-label prescription practices were being used to manage offenders involved in institutional misconducts or who had more serious offence histories. A statistically significant relationship was observed between the most serious offence on the sentence and the prevalence of approved or off-label prescriptions for medication, with those with the most serious and violent offences most likely to be prescribed medications for approved uses, compared with higher rates of off-label prescription use for less serious, less violent offences. Both the number of institutional charges and the DFIA-R substance abuse domain ratings demonstrated a statistically significant relationship with the distribution of approved versus off-label prescriptions for psychotropic medication, but the pattern was not consistent. Likewise, there is not a clear trend in the pattern of substance abuse and prescription practices. Prescription of off-label psychotropic medications was not related to the portion of offenders’ sentence served, suggesting that physicians adhered to the formularies as consistently during the early period of adjustment to incarceration as they did when the offenders were later in their sentence.
Limitations
The present study was restricted to a sample of 13 of 43 institutions operated by the CSC. The sample was selected to ensure representation of each of the major administrative features and inmate groups in the federal prison system, including women, indigenous offenders, and inmates at a variety of security levels.
Comparison of the frequency of off-label use of psychotropic medications among federal inmates with that of the Canadian community was limited to one available study of prescribing practices among primary care physicians in Quebec, although the results did show that the levels of off-label medication use in this Canadian federal inmate study are not inconsistent with the results of other international studies.
We did not complete an agreement on reliability and validity of psychiatric diagnosis associated with the medication. It is possible that the designation of a medication as “off-label” may have been affected by a failure to accurately detect or diagnose a mental disorder.
Conclusions
The prevalence rate of off-label prescriptions for psychotropic medication within Canadian federal institutions fell within estimates found in studies of prescription practices in the community and in other studies completed in correctional settings. There were no significant differences by gender, age, or indigenous ancestry in the prevalence of approved versus off-label prescriptions for psychotropic medication. Among the different classes of psychotropic drugs, anxiolytic/hypnotics were the most likely medications to be prescribed off-label. No clear pattern associating a history of problems with substance misuse and prescription practices was detected. The condition found to have the highest rate of off-label prescriptions was insomnia. The findings suggest that rates of off-label prescribing in Canadian federal correctional facilities could be reduced if offenders had access to alternative nonmedical interventions to help them cope with sleep and anxiety problems.
Footnotes
Access to Data
Researchers seeking access to the data used in this study may make application to the CSC in the form of a request to the Commissioner.
Acknowledgments
The authors would like to acknowledge the cooperation of the Research Branch and Mental Health Branch of the Correctional Service of Canada in providing the data set for this study. The study was completed with funds awarded to Nipissing University. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the policies and perspectives of the Correctional Service of Canada.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Gregory P. Brown and Professor Terry Rabinowitz received funding to conduct the research through a Memorandum of Understanding between the Correctional Service of Canada and the Institute for Applied Social Research, School of Criminology and Criminal Justice at Nipissing University. As independent, academic researchers, Professor Brown and Professor Rabinowitz retain the right to make presentations about and publish the results of their research. Consequently, there is no conflict of interest declared. Dr. Lynn Stewart, Mr. Harold Boudreau, and Ms. Angela Wright are staff at the Correctional Service of Canada. Staff are encouraged to publish their work in peer-reviewed journals, but the content of the articles is not necessarily endorsed by the Correctional Service of Canada. No conflict of interest is declared.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was completed with funds awarded to the Institute for Applied Social Research, School of Criminology and Criminal Justice at Nipissing University, under the terms of a Memorandum of Understanding between the Correctional Service of Canada (CSC) and Nipissing University. In undertaking and completing research studies on behalf of and funded by CSC, the Nipissing University researchers and their academic associates retain the right to make presentations about and publish the results of their research.