
Abstract
Objective:
A current estimate of prevalence rates of mental disorder among Canadian federal offenders is required to facilitate treatment delivery and service planning.
Method:
The study determined prevalence rates of major mental disorders among newly admitted male offenders entering the federal correctional system in Canada. Data were collected at each regional reception site on consecutive admissions for a 6-month period (N = 1110). Lifetime and current prevalence rates were estimated using the Structured Clinical Interview for DSM Axis I Disorders (SCID-I) and the SCID Axis II Disorders (SCID-II). Degree of impairment was estimated using the Global Assessment of Functioning (GAF) scale. Results were disaggregated by Aboriginal ancestry.
Results:
The national prevalence rate for any current mental disorder was 73%. The highest rates were for alcohol and substance use disorders; however, over half of participants met the lifetime criteria for a major mental disorder other than alcohol or substance use disorders or antisocial personality disorder. Thirty-eight percent met the criteria for both a current mental disorder and one of the substance use disorders. Fifty-seven percent of offenders with a current Axis I mental disorder were rated as experiencing minimal to moderate functional impairment based on the GAF, indicating that most participants do not require intensive psychiatric services.
Conclusions:
These results underscore the challenge posed to Canadian federal corrections in providing the necessary mental health services to assist in the management and rehabilitation of a significant percentage of the offender population with mental health needs.
Clinical Implications
More than 40% of incoming federal male offenders meet the diagnostic criteria for a mental disorder other than personality or substance use disorders; about half of these have a significant degree of impairment associated with their diagnoses that requires specialized psychiatric services. Mental health professionals in Canadian prisons should be aware of the significant likelihood of comorbid substance use disorder and mental disorder. This is particularly striking among men of Aboriginal ancestry.
Limitations
The estimate of prevalence of mental diagnoses for incoming federal Canadian men may differ from rates for those who have been in custody for longer periods. Further research is required to determine the impact of specific diagnoses on institutional adjustment and outcomes on release.
There is well-established evidence that the rates of mental disorder in offender populations are higher than among the general public. 1,2 Estimates of the prevalence of mental disorders in prison samples have ranged from 15% to 81% 2 –9 depending on the assessment tools and the definition of mental disorder adopted. Some of the highest rates have been found in the Canadian correctional systems, 5,10 –12 where researchers and advocates have urged action to address the substantial mental health needs of these offenders. 13 –15 Studies uniformly find high rates of substance abuse disorders and antisocial personality disorder (APD) among individuals involved in the criminal justice system. 10 –12 Serious Axis I disorders are also more prevalent among offenders than in the nonoffender population. For example, a meta-analytic review of the research on rates of mental disorder among prisoners in several countries found that schizophrenia was 10 times more common in prisons than would be expected based on its prevalence in the general population. 16 In addition, an Australian national study estimated the prevalence of schizophrenia between 2% and 5% for prisoners, 17 whereas the rate in the general Australian population is around 1%, 18 similar to the estimates of 0.3% to 1% cited worldwide. 19
High rates of mental disorder among offender populations pose a challenge for correctional agencies responsible for addressing the offenders’ mental health needs. There is also literature, albeit inconsistent, that suggests that a diagnosis of a mental disorder or a co-occurring mental disorder and substance use disorder increases the likelihood of institutional adjustment problems and reoffending on release, 20 –23 requiring adapted interventions and strategies to address this risk. In the Correctional Service of Canada (CSC), Canada’s federal correctional agency, there is an indication that the prevalence of offenders with mental health problems may be increasing. 24 Between 1997 and 2008, the percentage of in-custody male offenders who self-reported at intake that they had received a current mental health diagnosis almost doubled from 7% to 13%, and the proportion prescribed medication for mental health issues increased from 9% to 21%. 24 These data are based on simple questions asked of offenders about their current and past mental health status when they are admitted into the federal correctional system. Although the results are useful for tracking general trends, they are not adequate for determining diagnoses or for guiding intervention strategies. As part of a comprehensive mental health strategy designed to assess and treat offenders with mental disorders, a self-report Computerized Mental Health Intake Screening System (CoMHISS), completed by all offenders entering the federal correctional system, was implemented nationally in 2009. 25 While these screening results flag offenders in need of follow-up from psychological staff, they do not provide the rates of diagnoses of mental disorder. 26 Complicating case management further is evidence that offenders with mental health problems often do not suffer from only one disorder but meet the criteria for multiple psychiatric diagnoses, most often a diagnosis for a major mental disorder in combination with a substance use disorder or APD. 12,27 –29 Indeed, Hodgins and Coté 30 determined that only 7.6% of offenders who met the diagnostic criteria for drug abuse or dependence experienced it in isolation. Various studies have shown that individuals with dual diagnoses are more likely to have criminal histories related to their substance abuse, to be homeless, to have more problems with institutional adjustment, and to fail after release from prison. 29,31
A mental health survey of CSC offenders conducted in 1988 used the Diagnostic Interview Schedule (DIS) to estimate rates of major mental disorder among a representative cross section of offenders. Using broad criteria, the authors reported high rates of serious disorders, including estimates of 56% for anxiety, 30% for depression, and 10% for psychotic disorders. 12 Given the previously noted indication that the rates of mental disorder may be increasing, the CSC requires an updated survey of the current prevalence of mental disorders among this vulnerable population. Knowledge of the rate of various major mental disorders in a prison population and the extent of impairment experienced related to these disorders allows for more detailed planning and delivery of services. Addressing the mental health needs of offenders promotes their improved quality of life, reduces suffering, respects basic human rights, and meets legislative requirements to provide essential health care services. 25
Method
Participants
All men admitted to the CSC on new warrants of committal were approached within the first 4 weeks following their admission to obtain their consent to participate. The national consent rate was 78%. To determine the representativeness of the sample, the profiles of study participants and refusers were compared. Participants were more likely to be lower risk (both as assessed by criminogenic need and static risk) and also more likely to be convicted of a sexual offence (χ2 = 9.18, df = 1, P < 0.01). There was no difference in the mean age between the participants and decliners (35.56 vs. 35.21 years, respectively). The demographic profile of participants and the sample size of each region was representative of the distribution of offenders in the CSC. All offenders included in this study provided informed consent to participate. Under the Privacy Act, paragraph 8(2)(j), the CSC is permitted to compile health data for statistical use as long as the presentation of the information guarantees confidentiality and the information is used in a manner consistent with the purpose for which the data were collected. Research within the CSC is conducted under the provisions of the Tri-Council policy on research ethics but is exempt from the requirement for an ethics review board.
Measures/Material
Structured Clinical Interview for DSM Axis I Disorders
The Structured Clinical Interview for DSM Axis I Disorders (SCID-I) 32 is a semistructured interview designed to determine major DSM-IV Axis I diagnoses. 32 The Research Version of the SCID, used here, allows the researcher to modify the interview to fit the specific needs of a particular study. 33 The following categories of Axis I disorders were assessed for this study: 1) mood, 2) psychotic, 3) substance use, 4) anxiety, and 5) eating. Pathological gambling was also included as an optional module. The SCID-I is widely considered the “gold standard” for assessing psychiatric diagnoses 34,35 and has been used with men and women in the community, as well as psychiatric and offender samples. 36 –38
Research suggests that the reliability for the SCID-I is good to excellent for most modules. 38 –43 Its validity is also good to excellent, comparing favourably to diagnoses made by psychiatrists in terms of sensitivity (0.50-1.00), specificity (0.94-1.00), and agreement (κ = 0.66-0.90). 44
Structured Clinical Interview for DSM Axis II Disorders
The Structured Clinical Interview for DSM Axis II Disorders (SCID-II) 45 is a semistructured interview that was developed for the assessment of DSM Axis II personality disorders. It is considered a valid tool for assessing personality disorders and has been used with offenders. 46 –48 Only the portions of the SCID-II that assess borderline personality disorder (BPD) and APD were administered in this study.
Reliability is reported as excellent for the BPD assessment, with kappa scores between .87 and 1.0 for measures of baseline interrater, test-retest, follow-up interrater, and follow-up longitudinal reliabilities. 38,48 –50 The interrater reliability of the APD assessment of the SCID-II is fair to excellent (.41-.95). 39,50 –52 Compared to other measures and psychiatric diagnoses, it has strong sensitivity (0.74-0.84), specificity (0.82), and convergent validity (r = 0.80) in men and women psychiatric patients. 53 –55 One study that compared the SCID diagnoses to longitudinal diagnoses found strong validity for the APD module for male psychiatric patients, with an agreement at 0.95 diagnostic power. 55
Modified Global Assessment of Functioning–Revised
The Modified Global Assessment of Functioning–Revised (GAF) is included in the DSM-IV-TR as the measurement for Axis V and is the most widely used measure of global functioning in psychiatric patients. 56,57 Ratings on the GAF range from 90 (absent or minimal symptoms and no impairment) to 0 (immediate danger from serious neglect or self-injurious behaviour). The tool contains descriptors for each 10-point bracket, making the distinction between criteria easier for raters. Although limited research on the reliability and validity of the revised tool has been conducted, the GAF has been used by the World Health Organization (WHO) to estimate degree of impairment across their large-scale international studies 58 and is regarded as a useful tool that can be easily administered with little training or clinical expertise. 59 While the psychometric properties of the tool have been criticized when it is used in clinical settings, excellent reliability and validity are reported when the instrument is applied with a structured assessment protocol such as the SCID and when raters receive brief training. 60
Procedure/Analytic Approach
The study employed a continuous intake method, meaning that all eligible offenders were approached to participate in the order in which they were admitted to the institution over a 6-month period. Due to logistical difficulties and lower than usual admission rates in some regions, data collection exceeded 6 months in some regions if a larger sample size was required. All interviews that comprise the data for the study were conducted between March 2012 and September 2014. The CSC requires that research results be disaggregated by Aboriginal ancestry if the numbers allow for meaningful analysis. For this study, the number of offenders in other ethnic groups was too small for analysis by subgroup.
Assessor training
Research assistants (RAs) were hired to work at the reception centres in each of the CSC’s 5 geographical regions (i.e., Atlantic, Quebec, Ontario, Prairies, and Pacific) and were trained on the administration of the SCID-I and SCID-II. Assessor training comprised 5 days of self-directed learning using the training materials provided by the authors of the SCID (i.e., 2 user’s manuals, 2 written case examples, 8 instructional DVDs). Upon completion of the training, a session with the first author was held to discuss any issues or questions that arose and to practice cases to ensure consistency. In instances where the RAs were unsure of a rating for an offender, they would consult the SCID manual and the first author before coming to a consensus. Coding decisions were kept in a living document and were shared with all RAs.
Participant recruitment
All incoming offenders on new warrants of committal were recruited at the reception units on a continuous basis. Offenders who were admitted because of revocations, breaches, or suspensions of a previous release were not included. It should be noted that a small percentage of offenders who would have met the referral criteria were not approached to participate for various reasons (e.g., they were immediately placed in segregation, were receiving treatment in hospital, were assessed as a security risk, or were a high-profile offender). Their information was documented and notes were taken indicating the reason they were not approached to participate. If an offender was approached and declined for personal reasons, the RA documented the reason. All interviews were conducted in a private room to ensure confidentiality. If an offender had been violent with staff or displayed behaviours that were considered unsafe, the interview was postponed or cancelled.
Informed consent and data management
No compensation or incentive was provided to participants. A verbal summary of the informed consent form was provided to the participant, followed by an opportunity to ask questions about the procedure and the consent form. A hardcopy of the signed informed consent form was required for the interview to proceed. A debriefing form was given to the participant following the completion of the interview. All interviews were conducted in English or in French. In the event an offender stated that he was concerned about his mental health or the RA felt the offender required follow-up services, he was referred to the psychology department at the institution.
After the interview was completed, data were entered into an electronic spreadsheet in a protected file on a secure network, and the hardcopy SCIDs were locked in a cabinet in a secure room at the institution. Offender names were kept separate from their participant numbers as a measure to further protect their identity. As a quality control measure, data on the electronic spreadsheet were periodically compared to the results recorded on the hardcopy SCID files.
Statistical techniques
Chi-square analyses were conducted to determine whether any statistically significant differences existed between the men who agreed to participate and those who did not, as well as to compare rates of mental disorder between Aboriginal and non-Aboriginal offenders. Student’s t tests were also performed to establish if any mean differences existed among the groups.
Results
National Prevalence
The overall rates of diagnoses for each category of mental disorder are presented, followed by rates for each individual diagnosis within that category. Table 1 displays the findings from the national sample (N = 1110). Current alcohol and substance abuse or dependence disorders were the most common (49.6%; n = 551), closely followed by rates of APD (44.1%; n = 490) and anxiety disorders (29.5%; n = 328). Eighty-one percent of offenders (n = 899) met the diagnostic criteria for at least 1 mental health disorder in their lifetime; 73% of participants (n = 808) met the criteria for a current disorder (i.e., within the past month).
Prevalence Rates of Mental Disorders in Newly Admitted Offenders (N = 1110).
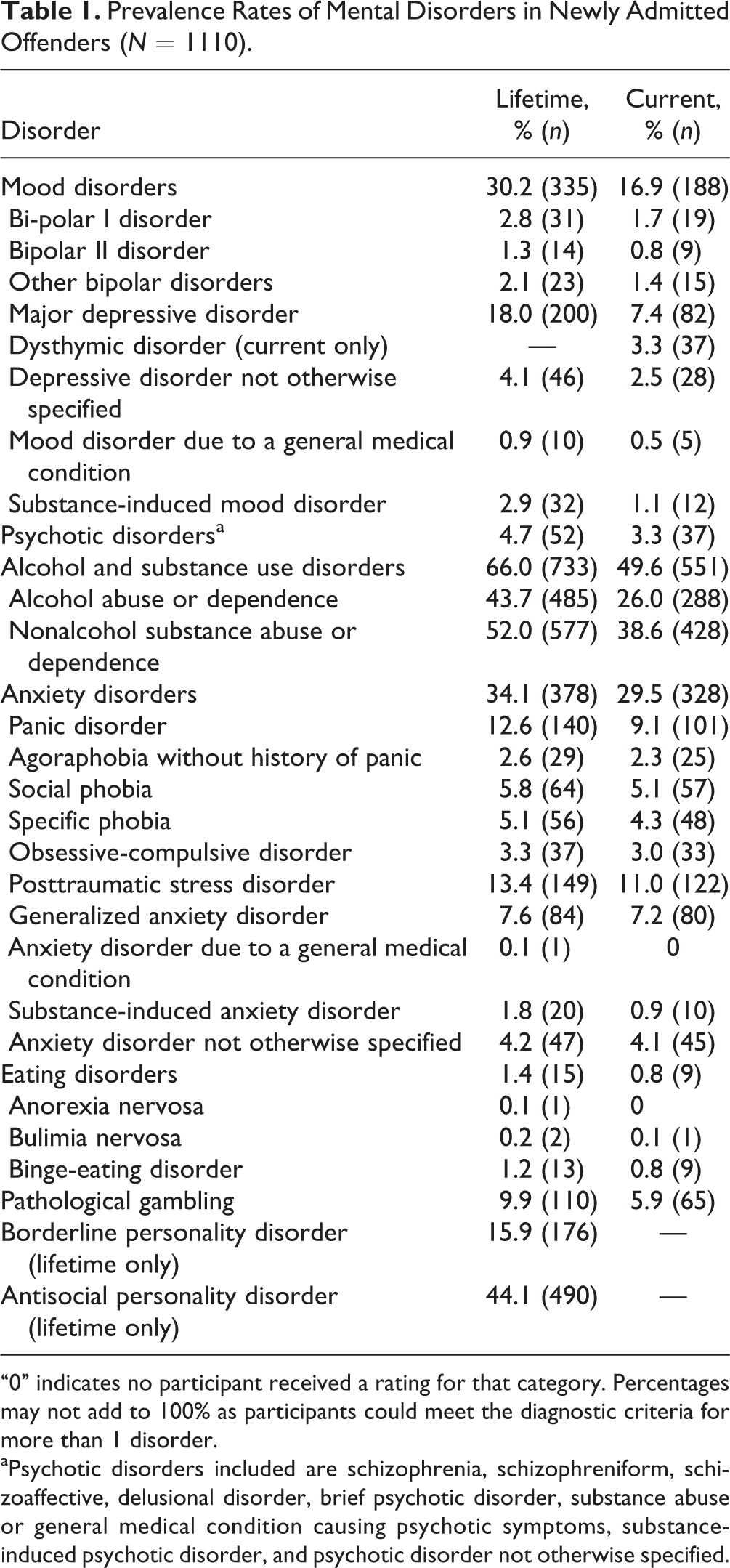
“0” indicates no participant received a rating for that category. Percentages may not add to 100% as participants could meet the diagnostic criteria for more than 1 disorder.
aPsychotic disorders included are schizophrenia, schizophreniform, schizoaffective, delusional disorder, brief psychotic disorder, substance abuse or general medical condition causing psychotic symptoms, substance-induced psychotic disorder, and psychotic disorder not otherwise specified.
Aboriginal Offenders
A breakdown of the national results by Aboriginal and non-Aboriginal ancestry is provided in Table 2. Differences in rates should be interpreted with caution given the smaller number of Aboriginal participants and low base rates of some conditions. The most striking findings are a considerably higher rate of alcohol and substance use disorders, as well as pathological gambling and personality disorders in the Aboriginal group. Although numbers are low, it appears that the rates of psychotic disorders and mood disorders are not significantly different between Aboriginal and non-Aboriginal offenders.
Prevalence Rates of Mental Disorders for Aboriginal and Non-Aboriginal Offenders (N = 1110).
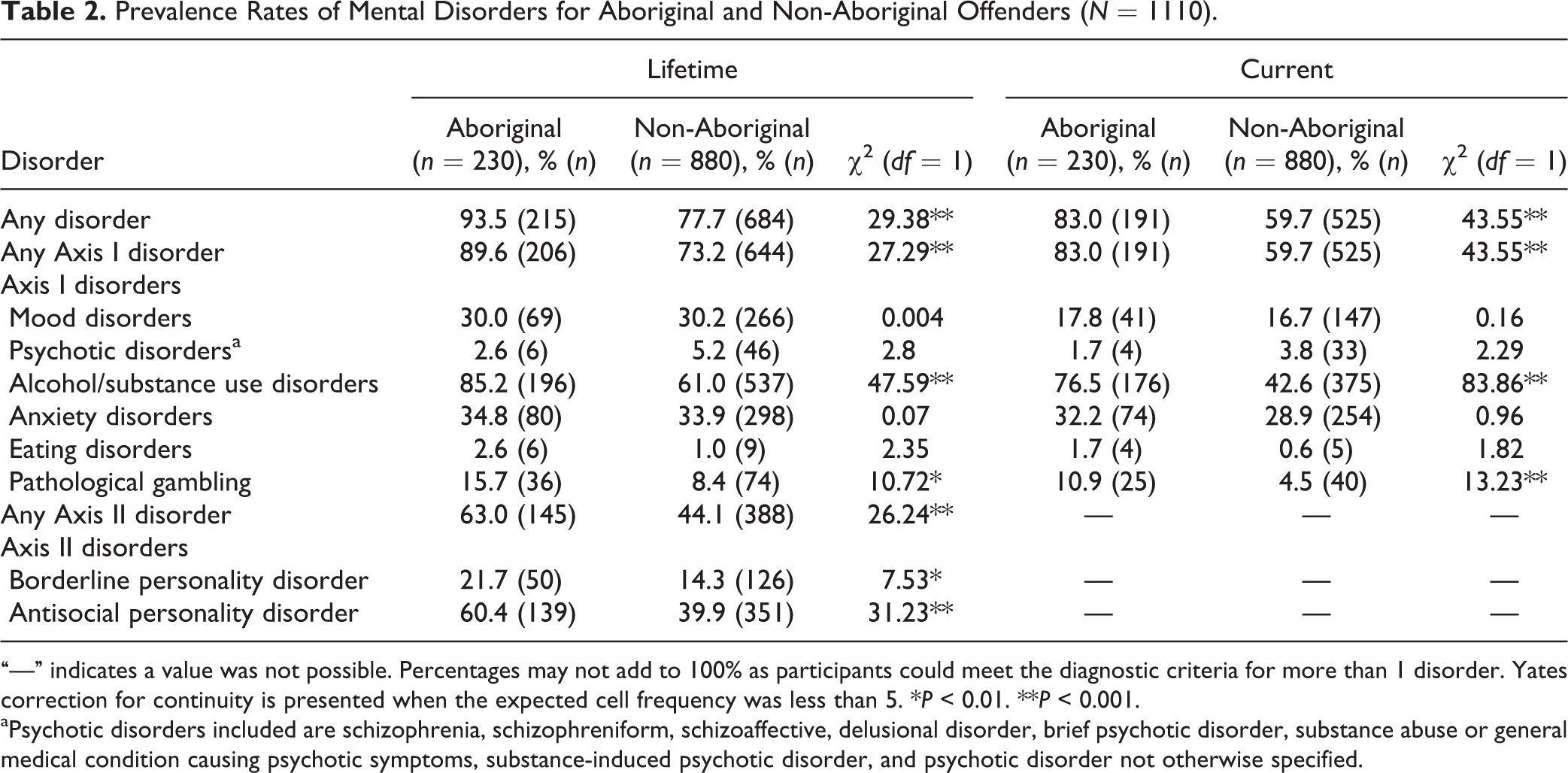
“—” indicates a value was not possible. Percentages may not add to 100% as participants could meet the diagnostic criteria for more than 1 disorder. Yates correction for continuity is presented when the expected cell frequency was less than 5. *P < 0.01. **P < 0.001.
aPsychotic disorders included are schizophrenia, schizophreniform, schizoaffective, delusional disorder, brief psychotic disorder, substance abuse or general medical condition causing psychotic symptoms, substance-induced psychotic disorder, and psychotic disorder not otherwise specified.
Rates of Comorbidity
Given the high prevalence of alcohol and substance use disorders and APD in offender samples, additional analyses were conducted, removing offenders who only had these disorders (see Table 3). Forty-four percent of participants (n = 483) met the diagnostic criteria for a current mental disorder other than APD or alcohol or substance use.
Prevalence Rates of Mental Disorders Excluding Alcohol and Substance Use Disorders and APD (N = 1110).
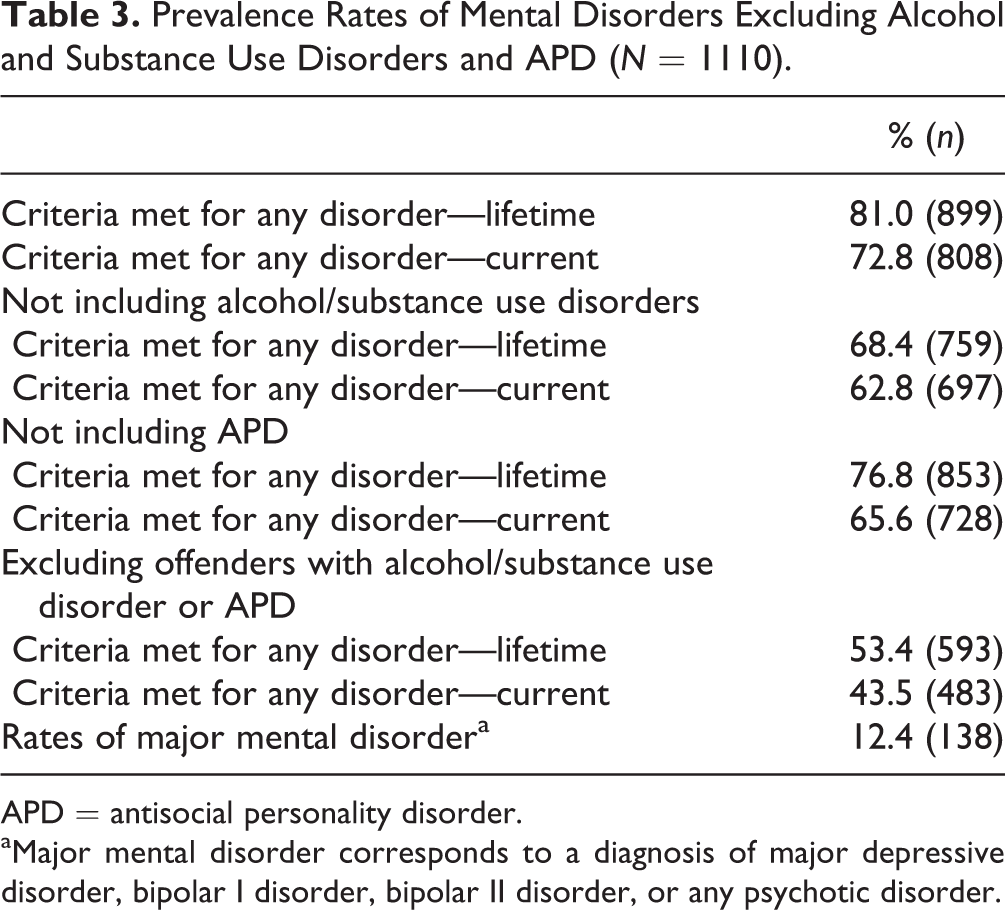
APD = antisocial personality disorder.
aMajor mental disorder corresponds to a diagnosis of major depressive disorder, bipolar I disorder, bipolar II disorder, or any psychotic disorder.
To establish the rates of common comorbid disorders among newly admitted offenders using results of the SCIDs, a cross-tabulation analysis was conducted (see Table 4). Thirty-eight percent of participants (n = 306) have a comorbid diagnosis of a mental disorder (other than APD) and a current alcohol or substance use disorder. The percentage of offenders with a current mental disorder who also have current diagnosis of APD is 34% (n = 276).
Co-occurring Disorders: Alcohol and Substance Use Disorders and APD.
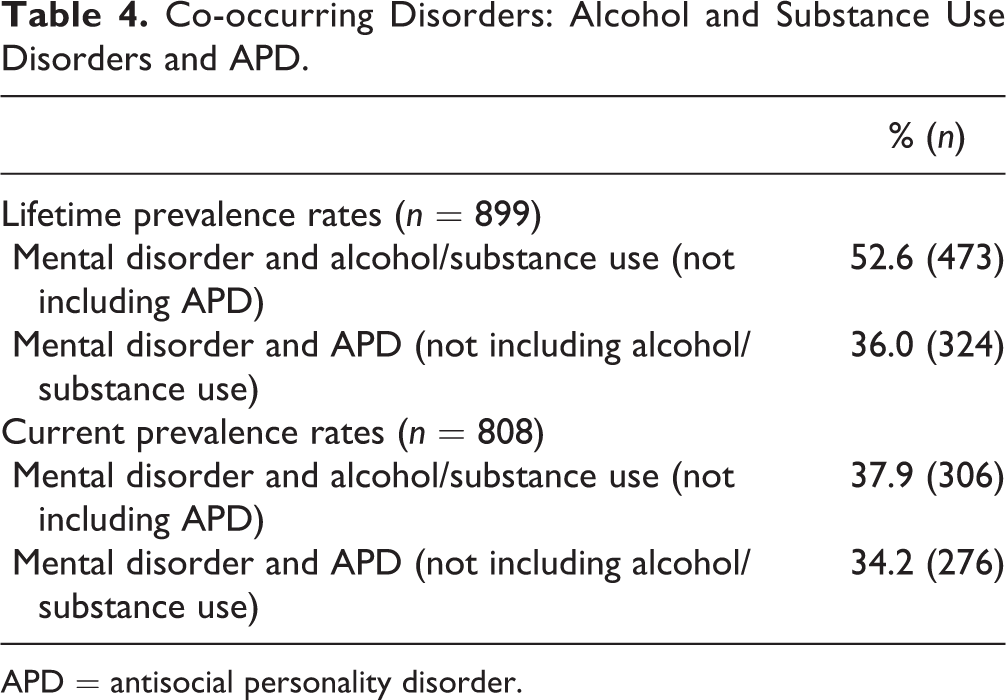
APD = antisocial personality disorder.
Global Assessment of Functioning
Scores from the GAF scale were analyzed to determine the level of impairment experienced by offenders for Axis I disorder and BPD (see Table 5). Fifty-seven percent of offenders (n = 249) with a current Axis I mental diagnosis were rated as having no or minimal impairment to moderate impairment on the GAF, indicating a reasonably good level of functioning in daily life. Offenders with BPD or a current diagnosis of primary psychotic symptoms fell within the lower levels of functioning on the GAF more frequently than did offenders with other diagnoses (with the exception of those with eating disorders), but these numbers are very low and therefore should be interpreted with caution.
Frequency and Scores from the GAF Scale by Mental Disorder Axis for Current Diagnoses.
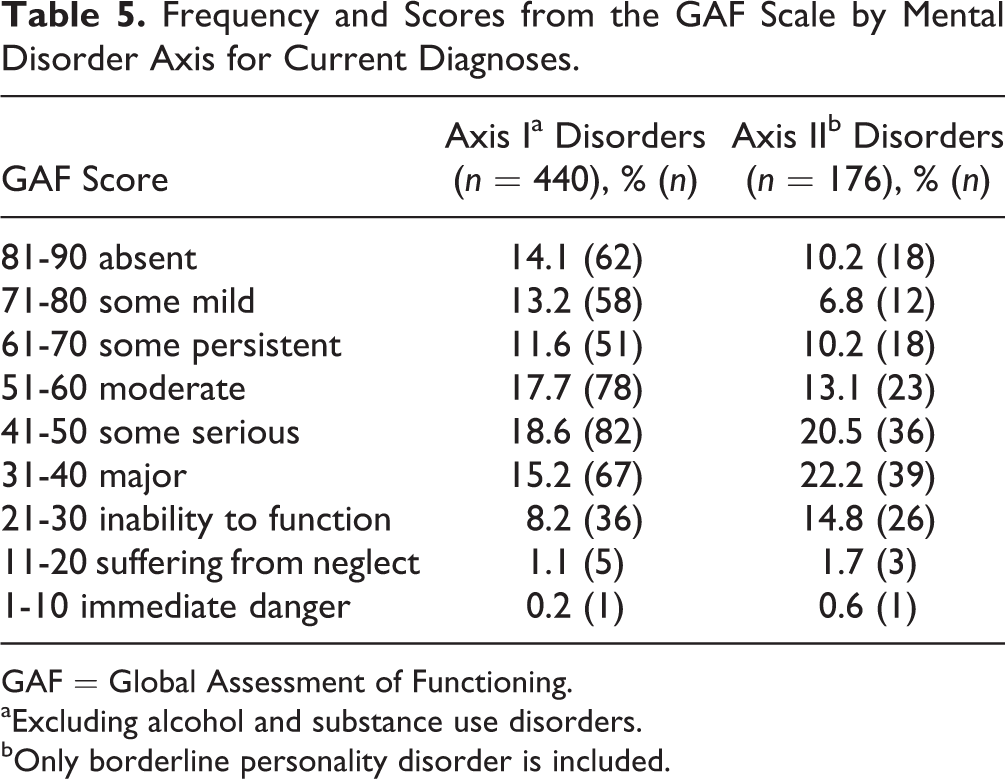
GAF = Global Assessment of Functioning.
aExcluding alcohol and substance use disorders.
bOnly borderline personality disorder is included.
Discussion
Prior to the 1980s, very few studies provided estimates of the rates of mental health disorders in prison populations. 4,61 In recent years, however, the need to determine these rates has become well recognized by correctional administrators. Establishing rates of mental disorders in incoming populations serves an important function in informing decisions regarding the allocation of resources and improving the standard of care to address the diverse needs of the offender population.
Results indicated that rates of mental disorders among federal male offenders do not appear to have increased markedly from the previous national survey completed in 1988. Rates of current psychotic disorders and depressive disorders obtained in this study and in the previous CSC survey are quite similar. 12 Rates reported by Brink and colleagues, 5 using the SCID to assess 207 incoming federal offenders in 1 Canadian region, reported similar lifetime rates for mood disorders (22% vs. 30% in our survey), psychotic disorders (5% vs. 4.7%), and substance use disorders (70% vs. 66%). Nevertheless, current rates are high, considerably higher than those found among the Canadian public. Using a self-report tool that mapped symptoms onto the DSM, the recent Community Mental Health Survey of Canadians aged 15 years and older noted that three-quarters of Canadians have “flourishing mental health,” that is, high positive emotions and high positive functioning. 1 Rates of mental illness including at least 1 diagnosis for depression, bipolar disorder, generalized anxiety disorder, alcohol abuse and dependence, cannabis abuse and dependence, and other substance abuse and dependence hover around 10%. 1 The comparable rate for federal offenders including the same conditions is more than 70%. It should be noted, however, that the reported rates in our study were not age adjusted. In addition, estimates in both surveys include substance use disorders, which are typically much higher in correctional samples.
Complicating treatment planning for this population are high rates of comorbidity with over half of male offenders having at least 1 mental disorder other than APD and at least 1 substance use disorder. Past community surveys have established a much higher rate of suicide for Aboriginal Canadians than the Canadian population as a whole, as well as higher rates of depression. 62 Our results suggests that while the rates of mood and psychotic disorders in the federal offender population are elevated relative to the general population, these rates do not differ between Aboriginal and non-Aboriginal offenders. Aboriginal offenders do, however, have markedly higher rates of alcohol and substance use disorders and personality disorders. Treatment providers should be aware that many Aboriginal offenders with a mental disorder also have a comorbid alcohol or substance use disorder.
While the SCID provided reliable estimates of major mental disorder among this offender population, our study also afforded unique information on the degree of impairment related to a mental disorder through the assessment on the GAF. Many individuals with mental disorders lead productive lives and may not require extensive psychiatric services or may not require them on an ongoing basis. Our analysis indicates that among offenders who met criteria for a current Axis I disorder, approximately 43% were rated as experiencing serious to severe impairment. Consistent with the literature, greater impairment was found for offenders in our study who met the criteria for BPD (60% with serious to severe impairment) than those with Axis I disorders only. 63 These scores are difficult to compare to clinical community samples, but 1 study found that 47% of those with BPD had GAF scores below 50, suggesting higher rates of impairment in the correctional sample for offenders with BPD. 64
Limitations
The present study was restricted to only those offenders recently admitted to federal custody under new warrants of committal. The prevalence rates may differ from those of offenders in the provincial system. Indeed, they may also differ from those in the federal system who are in the general CSC population. For individual offenders, adjustment to the stress of recent incarceration could increase the likelihood of experiencing a current disorder while in reception centres. On the other hand, when rates are examined across incarcerated samples, offenders who have more mental health needs typically have longer sentences and may face challenges earning discretionary release. Offenders who return to custody on a current sentence also tend to have higher risk and need profiles and may therefore have higher rates of mental disorder. 65 A previous study analyzing mental health indicators used by the CSC found that offenders in the general population self-reported higher rates of psychiatric problems than offenders who were assessed upon admission. 66 In addition, some offenders deferred from assessment may have been among those most likely to have a diagnosis (i.e., those immediately sent to treatment centres or those who were segregated upon admission). The number of offenders lost to the sample for these reasons was very low, however, and unlikely to have substantially affected the overall estimates. But together, these considerations suggest that the rates of mental disorder provided here may actually underestimate the rates in the incarcerated federal population.
Another limitation of the research was that interrater reliability among RAs was not determined. However, the reliability for the SCID-I and SCID-II is well established. What is more, all RAs were trained in the same manner, following a strict training protocol, and the trainer checked assessment results regularly. These provisions typically ensure good interrater reliability.
Conclusions
It was anticipated that many offenders sentenced to a federal penitentiary would present with mental health issues. Their histories indicate that they are among the most marginalized members of society, experiencing multiple social determinants associated with adverse health and mental health outcomes such as limited education, poverty, and early histories of abuse. 67 The results of this study illustrate the challenges posed to Canadian federal corrections to provide the required interventions and mental health services to assist in the management and rehabilitation of a significant percentage of the correctional population.
Footnotes
Acknowledgments
We thank the contribution of the Research Branch and Mental Health Branch of the Correctional Service of Canada for providing the funding and resources for this study. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the policies and perspectives of the Correctional Service of Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.