
Abstract
Background:
Mental disorders constitute a significant public health problem worldwide. Ensuring that those who need mental health services access them in an appropriate and timely manner is thus an important public health priority. We used data from 4 cross-sectional, nationally representative population health surveys that employed nearly identical methods to compare MHSU trends in the Canadian military versus comparable civilians.
Method:
The surveys were all conducted by Statistics Canada, approximately a decade apart (Military-2002, Military-2013, Civilian-2002, and Civilian-2012). The sample size for the pooled data across the surveys was 35,984. Comparisons across the 4 surveys were adjusted for differences in need in the 2 populations at the 2 time points.
Results:
Our findings suggested that first, in the Canadian military, there was a clear and consistent pattern of improvement (i.e., increase) in MHSU over the past decade across a variety of provider types. The magnitudes of the changes were large, representing an absolute increase of 7.15% in those seeking any professional care, corresponding to an 84% relative increase. Second, in comparable Canadian civilians, MHSU remained either unchanged or increased only slightly. Third, the increases in MHSU over time were consistently greater in the military than in the comparable civilian sample.
Conclusions:
Our findings point to advantages with respect to MHSU of the military mental health system over the civilian system in Canada; these advantages have widened substantially over time. These findings speak strongly to the potential impact of analogous changes in other health systems, both military and civilian.
Over the past 2 decades, there has been increasing recognition that mental disorders constitute a significant public health problem worldwide. 1 As a result, researchers and international health organizations have called for “countries [to] make the…treatment of mental and substance use disorders a public health priority” 1 (p.1575). Many developed countries have heeded the call to improve mental health service use (MHSU) in their civilian populations. Civilian population health studies in these countries have subsequently shown increases in MHSU over the past decade. 2 –4
In contrast to the large civilian literature on trends in MHSU, to our knowledge only one study to date has used population health surveys to look at trends in MHSU in a military population in the past decade. 5 This U.S. study found increases in MHSU and decreases in perceived stigma from 2002 to 2011; nevertheless, it also found that in any given year, half of all military personnel with a mental health condition failed to receive mental health services.
The paucity of military population health research on MHSU trends over time is surprising. Military personnel are an important subset of the general population, and their unique mental health needs have come into sharp focus over the past 15 years of conflict in southwest Asia. Military populations have higher prevalence rates of certain mental disorders than their civilian counterparts. 6 Military personnel often access a separate mental health system, and military organizations have both special barriers that can hinder MHSU and unique opportunities that can facilitate it. 7 In the past couple of decades, a number of developed countries leveraged these opportunities and invested heavily in military mental health: In the U.S., U.K., Australia, and Canada, military organizations implemented public awareness, mental health education, and psychological resilience programs, and they expanded and strengthened their military mental health care systems. 8 –10 Yet, for most of these countries, whether MHSU has increased in their military populations as a result of these investments remains largely unknown.
Even more striking, no study to date has directly compared national trends in MHSU across military and comparable civilian populations over the same time period in a given country, making it uncertain as to whether the heavy investments in military mental health care have led, as intended, to greater gains in MHSU. This is an important gap in the mental health services literature, with implications for military and civilian policymakers alike. Until now, the principal impediment to comparing national trends in MHSU across military and civilian populations has been the lack of sufficiently comparable, high-quality data sources in both populations at 2 similar points in time.
In this study, we address this important gap in the scientific literature by using data from 4 cross-sectional, nationally representative population health surveys that employ nearly identical methods, in order to 1) explore trends in MHSU in the Canadian military over the period 2002 to 2013; 2) explore trends in MHSU in a comparable subsample of the Canadian civilian population over the same time period (2002-2012), and 3) compare trends in MHSU in the Canadian military to the trends in the subsample of comparable Canadian civilians. With these 3 comparisons, we hope to determine whether the substantial investments in the Canadian military mental health system have translated into greater improvements in MHSU relative to comparable civilians.
Method
Details of the method are provided in the Supplemental Materials.
Data and Sample
Data came from 4 cross-sectional population mental health surveys conducted by Statistics Canada and were collected in face-to-face interviews by trained lay interviewers using computer-assisted personal interviewing. The 2 civilian surveys included the Canadian Community Health Survey–Mental Health, 2012 (Civ-2012, n = 25,113, response rate of 68.9%), and 2002 (Civ-2002, n = 36,984, response rate of 77%). The sampling frame for both civilian surveys included those 15 years of age but excluded full-time members of the Canadian Armed Forces (CAF). The 2 military surveys included the Canadian Community Health Survey, Cycle 1.2–Canadian Forces Supplement, 2002 (Mil-2002), and the Canadian Forces Mental Health Survey, 2013 (Mil-2013). The sampling frame for the military surveys included both Regular Forces and Reservists.
Because the sampling design for Reservists differed across the 2 military surveys, for Mil-2002 and Mil-2013, we restricted the samples to the Regular Forces, with sample sizes of 5155 (response rate of 79.5%) and 6696 (response rate of 79.8%), respectively. For the civilian surveys, we restricted the samples to those who were full-time employed, aged 17 to 60, and we excluded respondents who would likely be ineligible for military service, 6 to create civilian groups comparable to the Regular Forces (n = 8538 and n = 15,595 from Civ-2012 and Civ-2002, respectively). The pooled data across the 4 surveys had a sample size of 35,984.
Measurement
Past-Year Mental Health Service Utilization
Past-year MHSU for “emotions, mental health, or use of alcohol or drugs” was assessed for a variety of health care providers: 1) psychiatrist, 2) family doctor or general practitioner, 3) psychologist, 4) social worker, counselor, or psychotherapist, and 5) nurse. An aggregate category of “any professional” was also created. Military respondents were asked not to include “visits for routine pre- or postdeployment screening.”
Sociodemographic and Clinical Covariates
Military personnel and civilians differ substantially in terms of their sociodemographic characteristics and in terms of their clinical needs, 6 factors that need to be considered in comparing MHSU across these populations. Sociodemographic covariates (age, sex, education, marital status, ethnicity/cultural origin, and household income) were drawn from the nondiagnostic sections of the surveys. Clinical covariates (self-reported physical and mental health status, past 12-month major depressive disorder [MDD], and past 12-month suicide ideation and attempt) were drawn from the diagnostic sections of the surveys, based partly on the World Health Organization version of the Composite International Diagnostic Interview (WHO-CIDI) 11 , a reliable and valid 12,13 lay-administered psychiatric interview that generates diagnoses based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV). 14
Statistical Analysis
We assessed differences in MHSU between 1) the two military surveys; 2) the two civilian surveys; and 3) the two contemporary military and civilian surveys. To fully assess differences, we first estimated the absolute difference and then the relative difference in the prevalence of MHSU across the surveys. Absolute and relative differences capture unique and complementary information (details in Supplemental Materials).
Absolute Differences in MHSU
Since the 4 surveys differed in sociodemographic and clinical characteristics (see Table 1), we used iterative proportional fitting—a sample matching approach that adjusts the survey weights in one population to yield an identically sized population with the same marginal distribution of covariates as the reference population. 15,16
Selected Characteristic of the Study Samples from the Four Surveys (95% CI).a
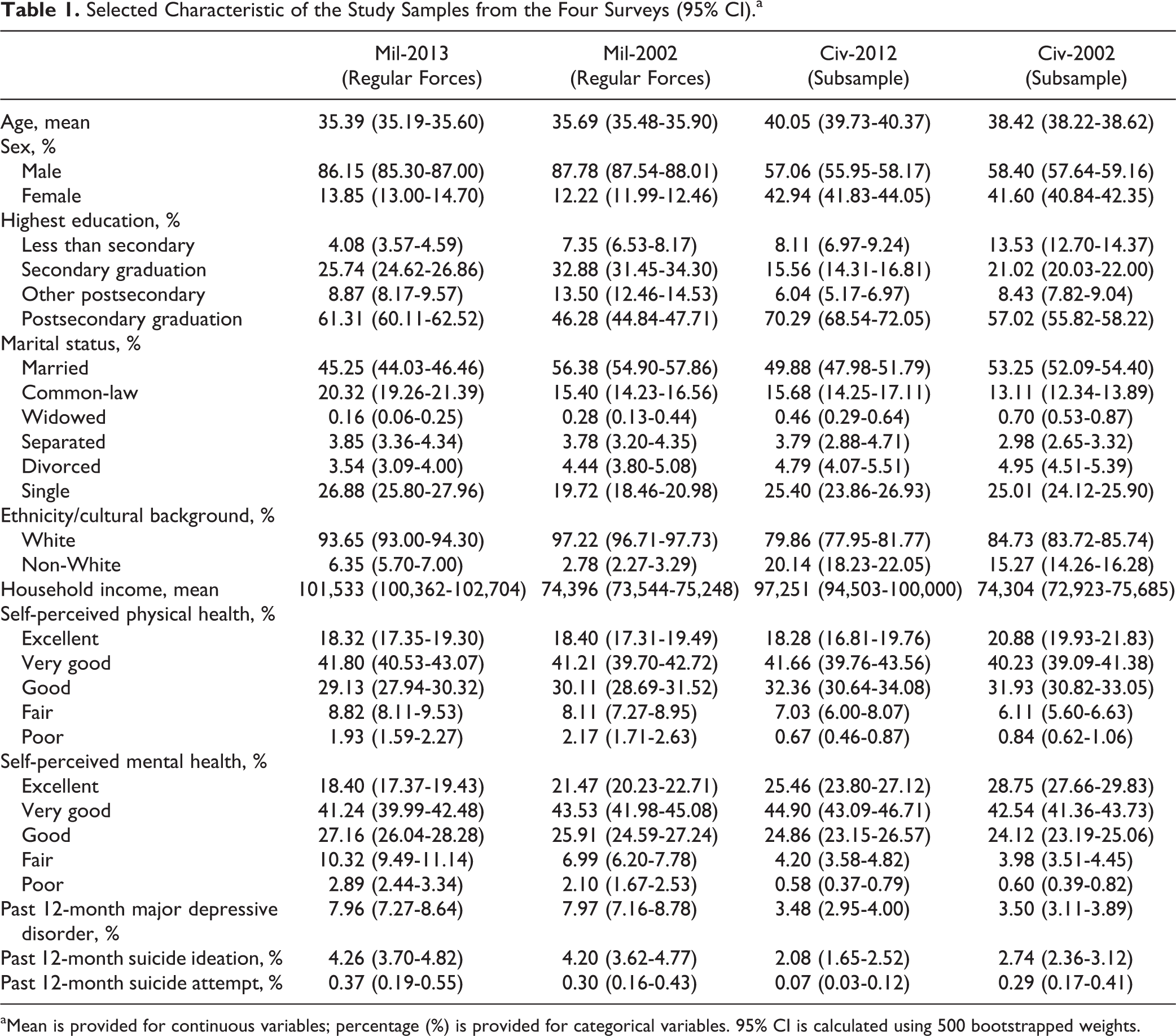
aMean is provided for continuous variables; percentage (%) is provided for categorical variables. 95% CI is calculated using 500 bootstrapped weights.
Estimating model-adjusted prevalence rate differences in the complex sample survey setting is challenging. Several approaches have been proposed 17 to test the robustness of the results. We used 2 approaches in this study: ordinary least-squares linear regression models with a robust variance estimate 18 and logistic regression models using SUDAAN, 19 software designed specifically for analyzing data from complex surveys. The absolute difference was denoted as the MHSU prevalence rate difference (PRD) between 2 surveys.
Relative Differences in MHSU
The relative difference was denoted as the MHSU prevalence rate ratio (PRR) of one survey to another. Given that the prevalence of past-year MHSU in the 4 surveys was relatively low for each provider type (<20%), we approximated PRR with prevalence odds ratio for the association between MHSU and being included in different surveys, which we calculated from binary logistic regressions. 20 We used logistic regression standardization and propensity score matching approaches to adjust for survey differences in sociodemographic and clinical variables.
Temporal Changes in MHSU in Military versus Comparable Civilian Populations
To assess whether the temporal change in MHSU for each provider is unique to the military, (i.e., that no such change has taken place, or that a smaller or a larger change has taken place in comparable civilians over the same period of time), we estimated the interaction between survey type (military vs. civilian) and survey time (2013/2012 vs. 2002) for the prevalence of MHSU, first for absolute and then for relative differences.
Weighting
For each of the 4 surveys, Statistics Canada created a survey weight to ensure that the survey samples were representative of the target population. We used survey weights in all our analyses. We performed bootstrapping, a variance estimation technique, to account for the complex survey design for calculating 95% confidence interval (CI) of all estimates. All analyses were conducted in SAS version 9.4. 21
Results
As expected, the military and comparable civilian samples showed considerable differences in sociodemographic and clinical characteristics. Compared with the 2 civilian samples, the 2 military samples were younger and more likely to be male and White. They reported worse self-reported mental health status as well as higher prevalence of past 12-month major depression, suicide ideation, and attempt. Differences were also observed between the older and more contemporary samples. For example, the 2 contemporary samples (Mil-2013 and Civ-2012) reported higher proportions finishing postsecondary education and lower proportions being married than the older samples (Mil-2002 and Civ-2002), respectively (see Table 1).
For all providers, the 2013 military sample reported the highest raw prevalence of past-year MHSU, followed by the military sample in 2002, the comparable civilian sample in 2012, and the comparable civilian sample in 2002 (Supplemental Table 1). An almost identical pattern of results emerged when the adjusted prevalence of past-year MHSU was calculated using iterative proportional fitting weights (Figure 1).
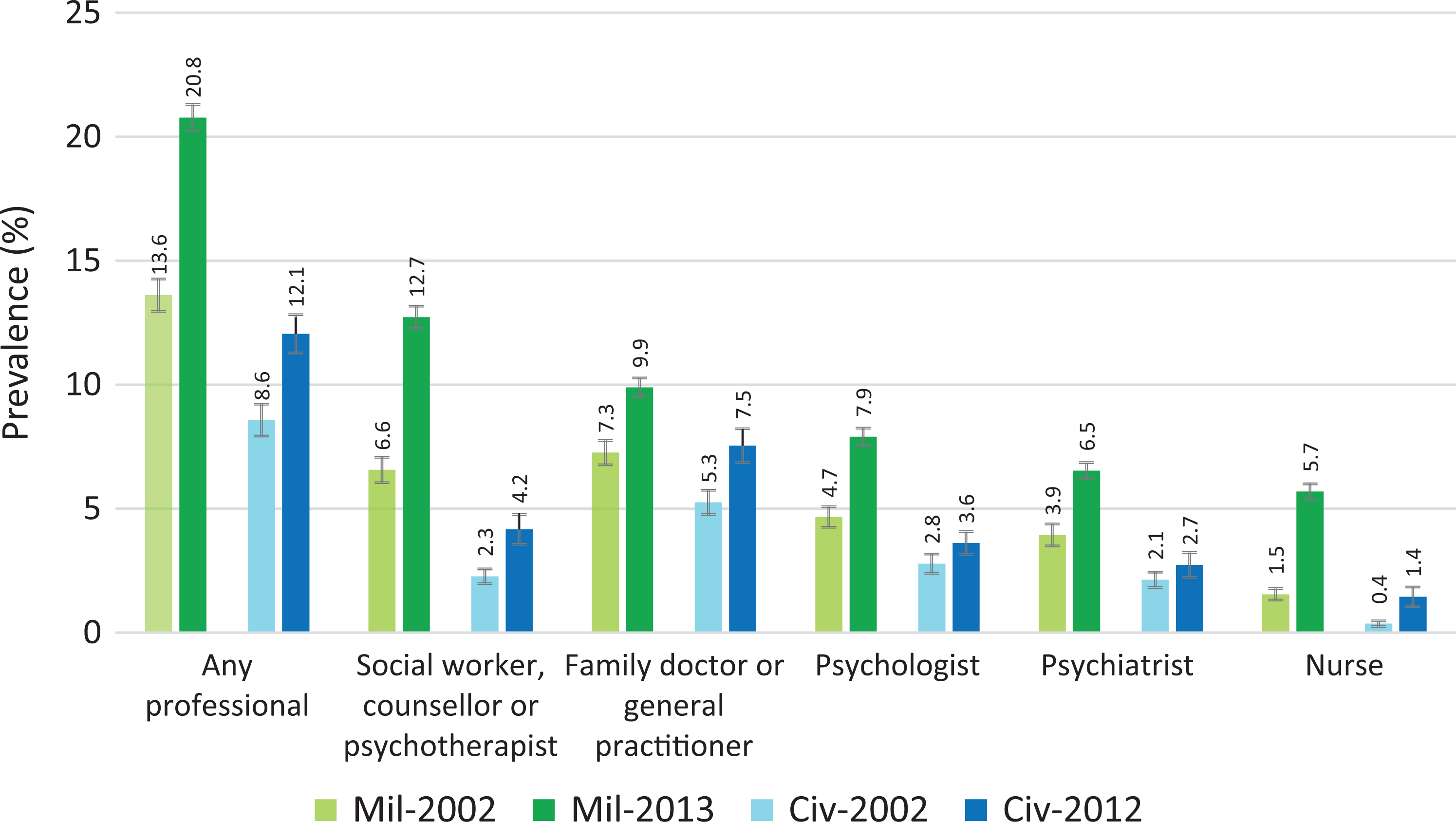
Adjusted prevalence of past-year MHSU by provider category, calculated using iterative proportional fitting weights. The error bars were calculated as prevalence point estimate ± 1 standard error of the prevalence point estimate. The adjusted prevalence rates for Mil-2002, Civ-2012, and Civ-2002 surveys were calculated using weights to approximate the population of Mil-2013 survey. The following variables were included in calculating iterative proportional fitting weights: age, sex, education, marital status, family income, ethnicity/cultural origin, self-reported mental health status, self-reported physical health, past 12-month major depressive episode, past 12-month suicide ideation, and attempt.
In the military, there were significant absolute increases in MHSU prevalence over the past decade, by 2.59% to 6.17%, across providers, after adjustment for sociodemographic and clinical characteristics (Table 2). Much smaller increases—by 0.60% to 2.29%—were seen in comparable civilians. For all providers, the 2013 military sample had significantly higher—by 2.35% to 8.57%—prevalence of MHSU than the 2012 civilian sample.
Adjusted Absolute Differences in Past-Year MHSU Between Different Surveys, by Provider Category, Calculated Using Iterative Proportional Fitting.abcd
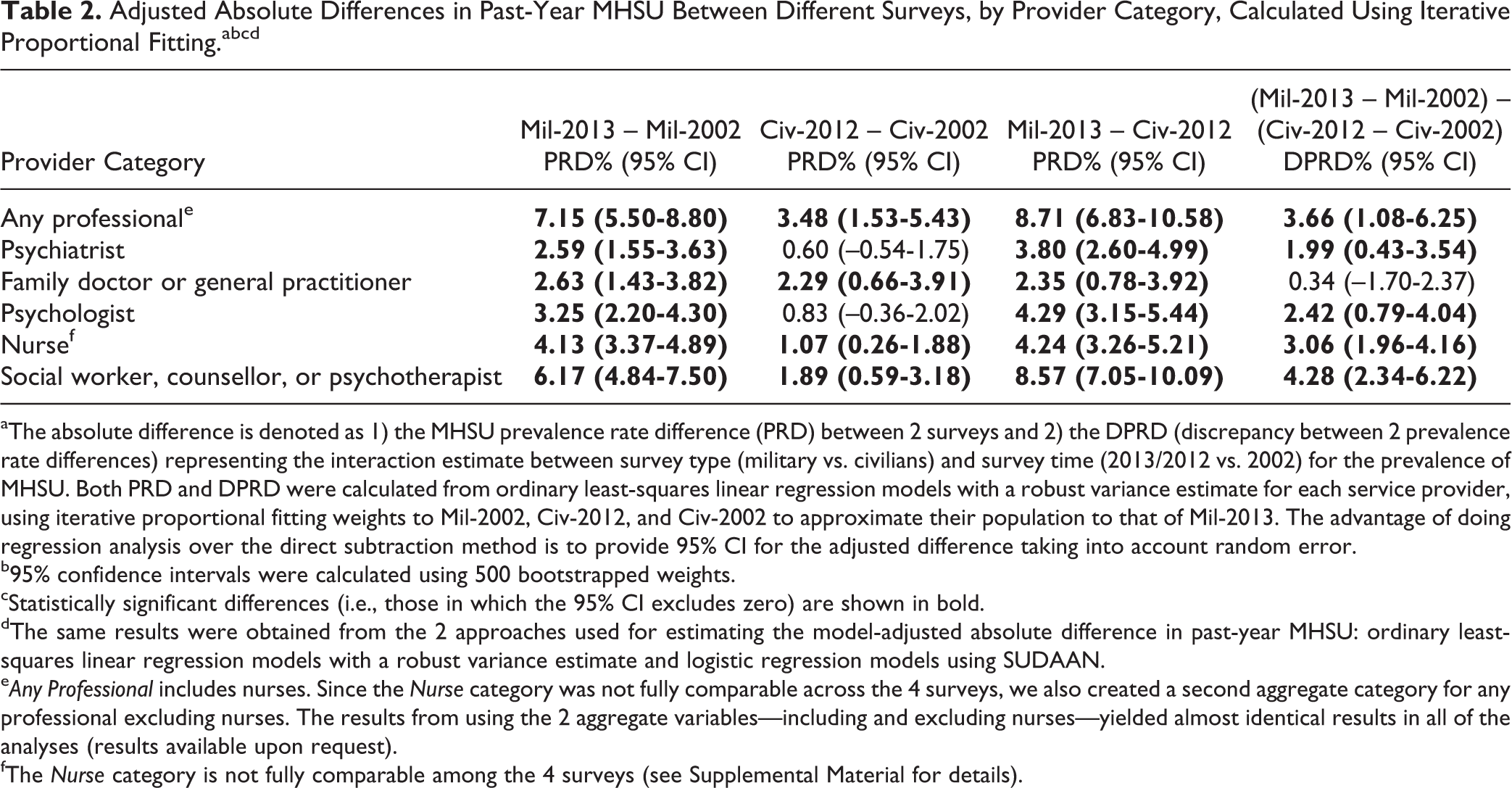
aThe absolute difference is denoted as 1) the MHSU prevalence rate difference (PRD) between 2 surveys and 2) the DPRD (discrepancy between 2 prevalence rate differences) representing the interaction estimate between survey type (military vs. civilians) and survey time (2013/2012 vs. 2002) for the prevalence of MHSU. Both PRD and DPRD were calculated from ordinary least-squares linear regression models with a robust variance estimate for each service provider, using iterative proportional fitting weights to Mil-2002, Civ-2012, and Civ-2002 to approximate their population to that of Mil-2013. The advantage of doing regression analysis over the direct subtraction method is to provide 95% CI for the adjusted difference taking into account random error.
b95% confidence intervals were calculated using 500 bootstrapped weights.
cStatistically significant differences (i.e., those in which the 95% CI excludes zero) are shown in bold.
dThe same results were obtained from the 2 approaches used for estimating the model-adjusted absolute difference in past-year MHSU: ordinary least-squares linear regression models with a robust variance estimate and logistic regression models using SUDAAN.
eAny Professional includes nurses. Since the Nurse category was not fully comparable across the 4 surveys, we also created a second aggregate category for any professional excluding nurses. The results from using the 2 aggregate variables—including and excluding nurses—yielded almost identical results in all of the analyses (results available upon request).
fThe Nurse category is not fully comparable among the 4 surveys (see Supplemental Material for details).
The temporal absolute increase in the prevalence of MHSU was significantly greater in the military than in the comparable civilians for all providers except family doctor or general practitioner (Table 2). For family doctor or general practitioner, the absolute increase in the military was not significantly greater than in the comparable civilians.
Over the preceding decade, there were analogous significant relative increases in the military—by 1.56 to 5.39 times—in the prevalence of MHSU with all health care providers (Table 3). Comparable civilians had significant but smaller relative increases—by 1.55 to 3.01 times—in the prevalence of MHSU with nurses and social workers, counsellors, or psychotherapists. Notably, in comparable civilians, the prevalence of MHSU with psychiatrists, psychologists, family doctors, or general practitioners was almost unchanged. Compared with the 2012 civilian sample, the 2013 military sample had a significantly higher—by a factor of 1.51 to 7.39—prevalence of MHSU with health care providers.
Relative Differences in Past-Year MHSU Prevalence—Using Logistic Regression Standardization to Adjust for Survey Differences in Sociodemographic and Clinical Characteristics.abcd
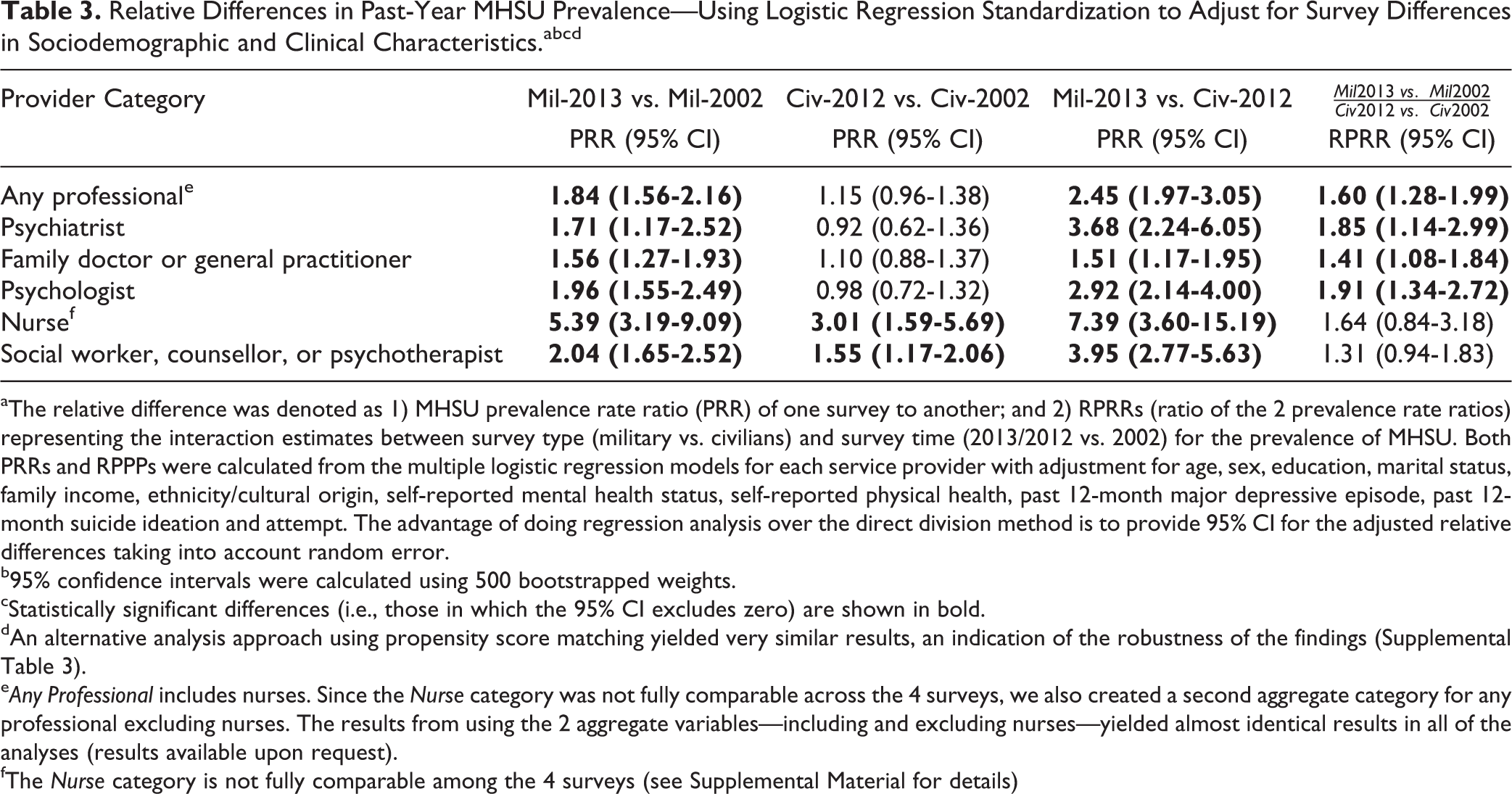
aThe relative difference was denoted as 1) MHSU prevalence rate ratio (PRR) of one survey to another; and 2) RPRRs (ratio of the 2 prevalence rate ratios) representing the interaction estimates between survey type (military vs. civilians) and survey time (2013/2012 vs. 2002) for the prevalence of MHSU. Both PRRs and RPPPs were calculated from the multiple logistic regression models for each service provider with adjustment for age, sex, education, marital status, family income, ethnicity/cultural origin, self-reported mental health status, self-reported physical health, past 12-month major depressive episode, past 12-month suicide ideation and attempt. The advantage of doing regression analysis over the direct division method is to provide 95% CI for the adjusted relative differences taking into account random error.
b95% confidence intervals were calculated using 500 bootstrapped weights.
cStatistically significant differences (i.e., those in which the 95% CI excludes zero) are shown in bold.
dAn alternative analysis approach using propensity score matching yielded very similar results, an indication of the robustness of the findings (Supplemental Table 3).
eAny Professional includes nurses. Since the Nurse category was not fully comparable across the 4 surveys, we also created a second aggregate category for any professional excluding nurses. The results from using the 2 aggregate variables—including and excluding nurses—yielded almost identical results in all of the analyses (results available upon request).
fThe Nurse category is not fully comparable among the 4 surveys (see Supplemental Material for details)
The temporal relative increase was significantly greater in the military than in the comparable civilians for psychiatrists, psychologists, and family doctors or general practitioners (Table 3). For nurses and social workers, counsellor, or psychotherapists, the relative temporal increase in the military was not significantly greater than in comparable civilians.
Discussion
Several key findings emerge from our work: First, in the Canadian military there was a clear and consistent pattern of improvement (i.e., increase) in MHSU over the past decade across a variety of provider types. The magnitudes of these changes were large, representing an absolute increase in those seeking any professional care of 7.15%, corresponding to an 84% relative increase. Second, in comparable Canadian civilians, MHSU remained either unchanged or increased only slightly. Third, the increases in MHSU over time were consistently greater in the military than in the comparable civilian sample.
Differences in MHSU at the military and civilian populations at the 2 time points can emanate from both differences in military and civilian populations and differences in the mental health systems they access. Given that we carefully controlled for differences in important sociodemographic and clinical need variables in the 2 populations, we suspect that our findings emanate from differences in military and civilian mental health systems at the 2 time points.
In Canada, military personnel access a parallel medical and mental health care system that serves only the military. Unlimited professional mental health care (including medications) is provided at no cost to the patient. Members can access professional care from social workers and mental health nurses without referral—even walk-in service is available. Specialty mental health services are available at all major bases, and transportation to care is provided for those in more remote areas. For those who prefer to seek care outside of the CAF, a free, confidential employee assistance program is offered.
In contrast, while civilians have universal health insurance through provincial and territorial plans, most plans do not cover medications, and coverage of psychotherapy services is also uneven. In fact, structural barriers to mental health care were prevalent in civilians in 2002. 22 Thus, differences in terms of the structure of mental health care in the military versus the civilian mental health system in Canada were already in place in 2002, the first time point of interest for the present analysis. Our findings of greater MHSU in the military versus civilians even in 2002 suggest that such differences in the structure of care delivery do indeed facilitate MHSU. This observation coheres with civilian research showing that better insurance coverage and better access to mental health care lead to greater MHSU. 23
Since 2002, the CAF has engaged in extensive mental health systems renewal. 9 Key clinical changes relevant to access to care include more than doubling the number of mental health clinicians, opening additional clinics for those with occupational trauma-related problems, and implementation of a system-wide tele-mental health system. Resilience and mental health literacy training is now required regularly throughout service, and various anti-stigma campaigns have taken place. More detailed and systematic screening for mental health problems occurs before and after overseas deployments and during periodic medical examinations that are required every 2 to 5 years. A national Directorate of Mental Health was launched to coordinate this full range of programs and services, something not possible in the fragmented civilian mental health system in Canada. Changes in the Canadian civilian mental health since 2002 have been limited to largely strategic initiatives, such as the founding of a national Mental Health Commission and the publication of a mental health strategy 24 ; some national destigmatization efforts have been made as well. The structural problems with uneven insurance coverage and difficulties accessing specialty services persist. 25
The additional reinforcements in the military mental health system since 2002 were associated with large absolute and relative increases in MHSU in our military population. Similar investments in the U.S. military 8 have also borne fruit. 5 Decreases in delay to care in the Canadian military have been recently reported. 26 These findings also cohere with recent findings showing greater perceived need for care and perceived sufficiency of mental health care in the Canadian military versus comparable civilians, 27 even after adjusting for differences in need as we did in the present analyses.
We documented at most small gains in MHSU in civilians relative to 2002. While we can speculate that these may be related to strategic initiatives (such as the establishment of a national Mental Health Commission), to specific anti-stigma efforts, 28 or to evolutionary improvements in attitudes towards mental health care, with cross-sectional survey data we cannot definitively link any of these factors to the observed small gains. Gains in MHSU in civilian populations have been noted in other countries. 2 –4 Nevertheless, the greater investments in the military mental health system were associated with much more dramatic temporal gains in MHSU, relative to comparable civilians.
Strengths and Limitations
The primary strength of the present study is the almost identical methods across the 4 surveys in the 2 populations at contemporaneous time points—this is unique in the extant literature. 29,30 The primary limitation of the study is its observational and cross-sectional nature, making it impossible to interpret with confidence the reasons for the differences in MHSU we observed between the 2 populations at the 2 time points. We believe that differences in the structure of the military versus civilian mental health systems and the greater mental health services renewal in the military system likely account for these changes, but other factors might be at play. Our careful adjustment for sociodemographic differences and for differences in need among the survey populations and the replication of the results using different statistical approaches argue against technical factors as the explanation.
However, we could only adjust for those need-related factors that were measured in all 4 surveys. Neither civilian survey measured posttraumatic stress disorder, which may have been more prevalent in the military population and which has increased in the military population since 2002. 31 This motivated our inclusion of other indicators of need (current self-rated mental and physical health, current psychological distress). These indicators, however, can be both antecedents and consequences of care, and the recall period for the service use (past year) does not correspond to those measures of need. In sensitivity analyses (Supplemental Tables 4-6), the inclusion of additional need-related variables did not change the essence of the results.
In this study, our aim was to look at changes in MHSU in active Regular Forces military members over a period of roughly 10 years and to compare those to changes in comparable civilians. In doing so, we wanted to answer a counterfactual question: What would be the prevalence of MHSU in members of the CAF if they were not in the CAF? 29 This approach excludes large portions of the civilian population (e.g., the unemployed) and is vastly different than looking at changes in MHSU in the entirety of the military and the entirety of the civilian populations; consequently, our findings regarding civilians comparable to Canadian Regular Forces members may not and likely do not generalize to the entire civilian population.
In this paper, we took a well-established approach in the existing literature 3 –6 to look at changes in MHSU over time, carefully controlling for changing need, and as in previous studies, we interpreted increases in MHSU as indications of improved or better access. However, the survey data do not allow us to rule out other possible explanations of the observed increase in MHSU, such as unnecessary or inefficient use of services. Perhaps more important, the cross-sectional nature of the data prevents us from linking the observed increase in MHSU in the military to subsequent better mental health outcomes. Thus, it is unclear to what extent the observed increases in military MHSU over the past decade translated into meaningfully better mental health and well-being for military members. Additional limitations of our study (e.g., the use of self-report methods that introduce selection, recall, and social desirability biases) have been previously noted in extant population health literature. 12,32 Encouragingly, emerging research has used administrative data to look at MHSU patterns—for instance, a recent study looking at MHSU among released CAF members (i.e., veterans). 33 Future work should explicitly compare results across studies using different methods.
While our findings speak strongly to the potential impact of mental health system renewal in other health systems, both military and civilian, there were many differences in the military and civilian health systems (especially with respect to access to care and insurance coverage) in 2002, and mental health services renewal in the CAF since then has been multifaceted and evolutionary in nature. We therefore cannot tie the advantages in MHSU in the military and its improvement over time to any particular policy, program, or service. Deeper analysis of the survey data we used should shed light on the contribution of some facets of mental health renewal, such as the CAF’s mental health education and training program.
Conclusions
Using comparable survey data from Canadian military personnel and civilians in 2002 and 2012/2013, we found that Canadian Regular Forces personnel were much more likely to use mental health services than their comparable civilian counterparts, even before the transformative changes in the military mental health system over the past decade. The past decade of mental health services renewal in the Canadian military has been associated with a widening of this gap. These findings speak to the potential of reinforcements in mental health systems to increase use of mental health services, thereby limiting the impact of mental disorders on populations.
Supplemental Material
Online_Supplemental_Material - Do Investments in Mental Health Systems Result in Greater Use of Mental Health Services? National Trends in Mental Health Service Use (MHSU) in the Canadian Military and Comparable Canadian Civilians, 2002-2013
Online_Supplemental_Material for Do Investments in Mental Health Systems Result in Greater Use of Mental Health Services? National Trends in Mental Health Service Use (MHSU) in the Canadian Military and Comparable Canadian Civilians, 2002-2013 by Deniz Fikretoglu, Aihua Liu, Mark Allen Zamorski, Corneliu Rusu, and Rakesh Jetly in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Since the time of the research, the affiliation for one of the authors has changed. Dr. Corneliu Rusu is now in the Directorate of Mental Health, Canadian Forces Health Services Group, Ottawa, Ontario.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an internal grant to Dr. Fikretoglu from the Directorate of Mental Health, Canadian Forces Health Services Group, at the Department of National Defence. Dr. Liu was a contract biostatistician for the grant.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.