
Abstract
Objectives
The objective of the present study is to describe the patterns of health service use and of prescription claims in the year preceding an offense leading to a verdict of not criminally responsible on account of a mental disorder (NCRMD).
Methods
Provincial health administrative databases were used to identify medical services, hospitalizations, and ambulatory prescription claims among 1,014 individuals found NCRMD in Québec. Contacts in the year preceding the offense were analyzed using descriptive analyses and latent class analysis.
Results
Overall, 71.4% of subjects were in contact with services for mental health reasons within a year of their NCRMD offense. Among those that received services and not hospitalized for psychiatric reasons at the time of the offense, 20.7% committed the NCRMD offense within a week of the most recent mental health contact. Among those that had at least one prescription claim for an antipsychotic, 45.8% were not taking any antipsychotic at the time of the offense. Latent class analysis provided a multidimensional representation of mental health service use and showed that 58.4% of subjects had no or very rare contact with services.
Conclusions
Many forensic patients are likely to have experienced service disruption or discontinuity while in the community, for reasons that may relate to perceived need for care, to service organization, or to the acceptability, availability, and accessibility of services. Given the serious impact of the “forensic” label on the lives of service users, not to mention the increased pressure on resources, the considerable economic costs, and the impact on victims, there is reason to advocate for a greater involvement of mental and physical health service providers in early prevention of violence, which requires reorganizing resources to share the forensic knowledge upstream, before an offense is committed.
The remarkable growth in the number of admissions to forensic mental health (MH) services over the past decades, particularly in Québec,1,2 suggests that the justice system has become a gateway to specialized MH care for many individuals with severe mental illness with disruptive behaviours.3–7 In Canada, the majority of individuals who are admitted to forensic MH services have been found not criminally responsible on account of a mental disorder (NCRMD) 1 for an offense committed “while suffering from a mental disorder that rendered [them] incapable of appreciating the nature and quality of the [offense] or of knowing that it was wrong.” 8
The use of section 16 of the Criminal Code in Québec is several folds more frequent9–11 from what is observed in the rest of the country: indeed, the NCRMD defense is used in Québec for offenses of lesser severity and for a greater diversity of diagnoses, suggesting that the NCRMD defense criteria of the Criminal Code may be operationalized more liberally or that there are less diversionary interventions used than elsewhere in Canada. 12 Using the NCRMD verdict as a de facto diversion scheme is not without consequences. Admission to forensic MH services increases stigma,13–15 in turn creating structural barriers to accessing and maintaining employment 16 and housing,17,18 and reducing the capacity of health and social services to appropriately meet their needs. 15 In addition, treating a patient in forensic MH services incurs costs almost five times greater compared to general MH services. 19 Some observers have also argued that this leads to a loop effect, with more resources allocated to forensic rather than general MH services, making access to care in the community increasingly difficult.2,20
Canadian studies have highlighted that nearly three quarters of people found NCRMD had been hospitalized for psychiatric reasons before the offense,12,21 which is similar to what was found in New Zealand. 22 This highlights the importance of examining which services are accessed by individuals before they are charged with an NCRMD offense to better meet their needs in the community. However, to our knowledge, the nature and frequency of MH services received before entry to forensic services remain undocumented.
Objectives
The objective of the present study is to describe the nature and extent of mental and physical healthcare use in the 12 months prior to an offense leading to a NCRMD verdict.
Methods
Sample and Procedures
Data were extracted from the National Trajectory Project, 9 a longitudinal file-based study of people declared NCRMD in Canada between 2000 and 2005. Due to the availability of administrative health services data, the present analyses are based on the Québec subsample only. There were a total population of 1,964 individuals with at least one NCRMD verdict in Québec during the sampling period. Random sampling with a finite population correction was applied in all administrative regions to obtain a representative sample of 1,094 subjects. Matching based on full name and date of birth with administrative health services data was successful for 1,020 subjects. The exact date of the offense was unknown for an additional 6 subjects, who were excluded. The present analyses therefore involve 1,014 subjects, for a total of 92.1% of the original sample. Women and people born outside of Canada were less likely to be included in the analyses due to unsuccessful matching with health data (see Table S1 of the online supplement for a detailed comparison).
The research protocol was approved by appropriate institutional ethics review committees (Douglas Mental Health Research Institute and Institut national de psychiatrie légale) Philippe-Pinel. Governmental health records were obtained through authorization from the Québec Commission d’accès à l’information.
Measures
Health services data were obtained from the Ministry of Health and Social Services’ MED-ECHO and the Régie de l’assurance maladie du Québec (RAMQ), a physician fee-for-service database on all medical interventions and prescription claims completed under the public insurance system. Given that provinces in Canada rely on universal, public, single-payer systems, these data are available for most services if people have remained in Québec.
A first dataset described all hospitalizations. We selected all hospitalizations with an admission date within a year of the offense and up to the day before the offense. Hospitalizations for a primary diagnosis of mental disorder (ICD-9 codes 290–319) were classified as psychiatric.
A second dataset described all medical services. We selected all services within a year of the offense, outside of psychiatric hospitalization periods, up to the day before the offense. Consistent with the literature, 23 we assumed that various medical acts provided for the same diagnosis, on the same day and at the same institution represented a single visit. We classified services in the following mutually exclusive categories: (1) emergency room visits for MH reasons with no resulting hospitalization; (2) ambulatory psychiatric consultations outside of the emergency room; (3) primary care consultations for MH reasons; (4) primary care consultations for physical health reasons; and (5) specialist consultations for physical health reasons.
Finally, a third dataset described all ambulatory prescription claims. All public assistance or disability benefit recipients, and all individuals not eligible for coverage by a private plan, have prescription coverage through the RAMQ. We identified psychotherapeutic agents based on the American Hospital Formulary Service classification, including antidepressants (281604), antipsychotics (281608), anxiolytics (282400), and antimanic agents (282800). To address the fact that the dataset does not include medications dispensed during hospitalization, we assumed that people hospitalized for MH reasons had most likely received some form of psychotherapeutic agent. However, because of the diversity in prescription practices for severe mental illnesses and increased off-label use24–26, we did not attempt to guess what family of medication (antidepressant, antipsychotics, etc.) had been administrated based on the primary diagnosis for the hospitalization.
Review Board 1 files were used to extract sociodemographic variables, clinical variables, and justice-related variables. The severity of the NCRMD offense was evaluated using the Crime Severity Index. 27 Criminal justice involvement history was identified using files from the Royal Canadian Mounted Police.
Analytic Approach
As a first step, we used descriptive analyses to outline the nature and extent of service use and pharmaceutical claims in the 12 months preceding the date of the NCRMD offense. As a second step, we used latent class analyses28–30 to identify patterns of MH services use, using the sum of four types of MH services contacts within a year of the offense as observed indicators and random starts. We elected to conduct latent class analysis based on the hypothesis that a significant proportion of participants had very few MH services contacts. Using latent class analysis allowed a more multidimensional and nuanced perspective compared to simply describing the proportion of participants with zero MH services contacts. Under the latent class framework, we would be able to identify a group of participants who had one or two contacts with the healthcare system but no consistent follow-up. Participants with different service use patterns were compared on several sociodemographic, clinical, and offense-related characteristics using adjusted F-statistics for survey design from regressions followed by Sidak-adjusted pairwise comparisons. All analyses were weighted to account for the sampling strategy. We conducted the latent class analysis using Mplus 8 and all other analyses using Stata 15.
Results
The analyzed sample was composed of 86.2% men who were, on average, 36.6 years old (SD = 12.7). The majority were single (85.3%), born in Canada (66.0%) and had pensions, welfare or disability benefits as main income (74.6%). Psychotic disorder was the most common diagnosis at the time of the verdict (66.0%), along with mood disorder (28.4%). Almost a third (29.7%) had concomitant substance use disorder and 9.7% had a concomitant personality disorder.
Overall, 71.4% of subjects (n = 727) were in contact with MH services within a year of their NCRMD offense, a proportion that decreased to 59.0% in the 6 months prior (n = 602; see Table 1). Among those that received services and who were not hospitalized for psychiatric reasons at the time of the offense, one in five (20.7%, n = 148) committed the NCRMD offense within a week of the most recent contact (see Figure 1).
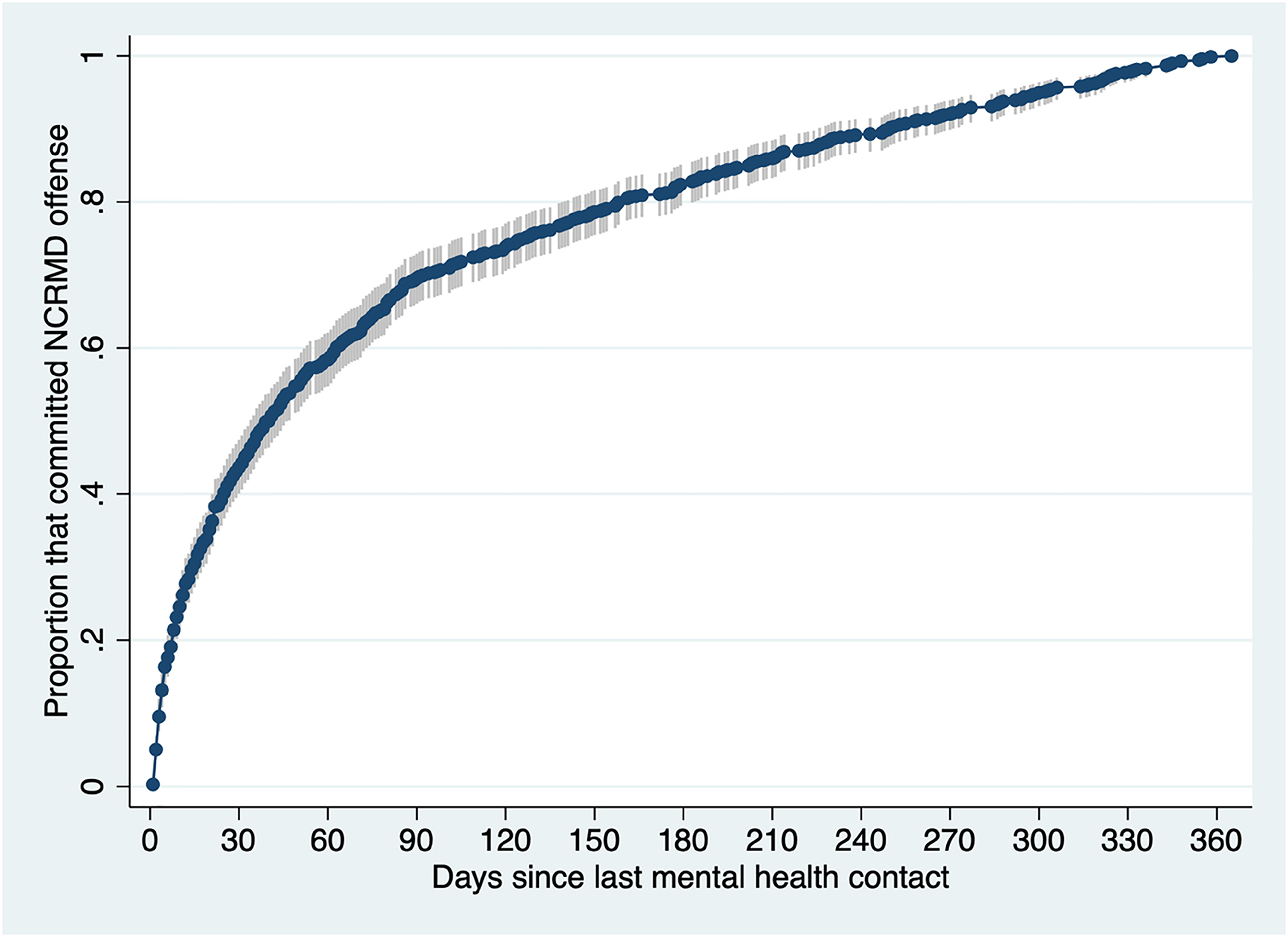
Failure function showing the cumulative proportion of subjects who committed an offense for which they were found Not criminally responsible on account of a mental disorder (NCRMD) at different time points after their last mental health contact. This failure function graph includes only subjects (n = 692) who had a least one contact with mental health services in the 12 months within their offense and who were not hospitalized at the time of the offense.
Nature and Extent of Individual Mental Health Service Use.
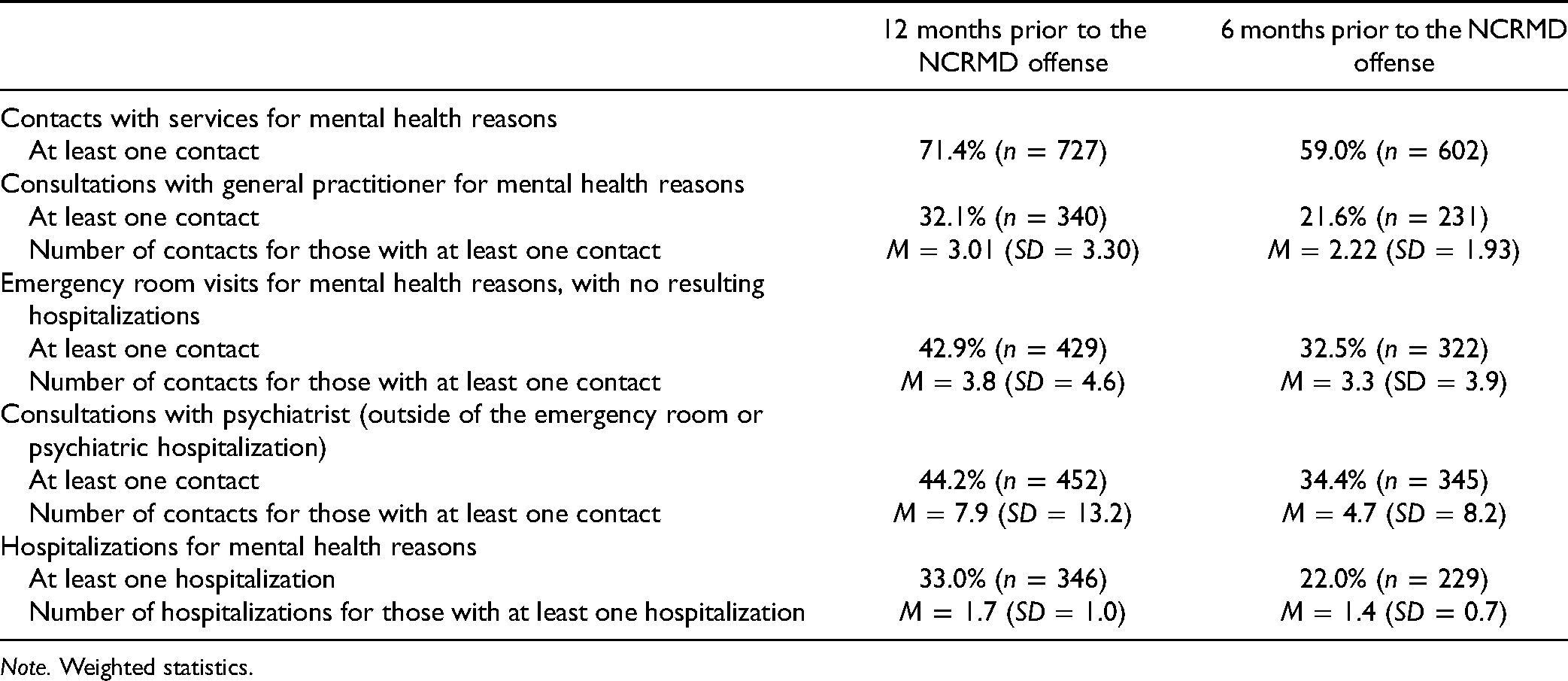
Note. Weighted statistics.
Nature and Extent of Service Use
Medical services
A total of 11,156 medical services were provided to 866 participants (85.4%), of which 54.2% were MH services. In terms of physical health services, the most common categories of diagnoses associated were injury or poisoning (35.5%). Among services provided for MH reasons, 3.0% were for drug or alcohol misuse, whereas schizophrenia spectrum psychoses (34.7%) and affective psychoses (12.7%) were the reason for most services. As many as 32.5% of MH services were provided by general practitioners, with the rest almost exclusively provided by psychiatrists.
A total of 44.2% (n = 452) consulted a psychiatrist on an ambulatory basis and 32.1% (n = 340) consulted a general practitioner for MH reasons. Almost half of subjects (43.9%, n = 151) that consulted a general practitioner regarding their MH received no services from a psychiatrist for the same period. A substantial proportion of subjects visited the emergency room for MH reasons without subsequent hospitalization: 42.9% (n = 429) in the previous 12 months, and 32.5% (n = 322) in the previous 6 months. Among those that visited the emergency room within 12 months of their offense, 21.8% (n = 96) were not in contact with any other non-emergency ambulatory MH services for the same period.
Hospitalizations
Overall, there were 746 hospitalizations among 410 participants (40.4%). Of all psychiatric hospitalizations, 43.7% were for schizophrenia spectrum psychoses and 20.4% for affective psychoses. Less than 5% were for drug or alcohol misuse. MH concerns were noted in 55.7% of physical health hospitalizations. A third (33.0%, n = 346) of subjects were hospitalized for psychiatric reasons within a year of their offense.
Prescription claims
Half of participants (50.8%, n = 512) filled at least one prescription for a psychotherapeutic agent within a year of their offense. When assuming that people who had been hospitalized for MH reasons had most likely received a psychotherapeutic agent during their hospitalization, the proportion increased to 59.8% (n = 602). Outside of a hospitalization, 40.1% (n = 404) filled at least one prescription for an antipsychotic drug—and 45.8% of those were not on any antipsychotic at the offense—and 16.6% (n = 167) for an antidepressant. Only 3.4% of all antipsychotic prescriptions were long-acting injectables, prescribed to a total of 66 subjects.
Patterns of MH Service Use
Based on best fit indices and parsimony, we selected the 4-class model (BIC = 21,833.152, entropy = 0.935, BLRT P < 0.001). While the 5-class model also presented good fit indices, it resulted in minimal improvement of indices (BIC = 21,340.255) and included classes of fewer than 1% of the sample, indicating overfitting (see Table S2 in the online supplement).
The largest class (58.4%) represented a pattern of no or rare contact with MH services (see Figure 2 and Table 2). One in five participants (18.9%) had been hospitalized for psychiatric reasons but 71.4% of those did not consult a psychiatrist outside of the period of hospitalization. A third (34.2%) had filled a prescription claim in the community for a psychotherapeutic agent, and 22.9% for an antipsychotic agent specifically.
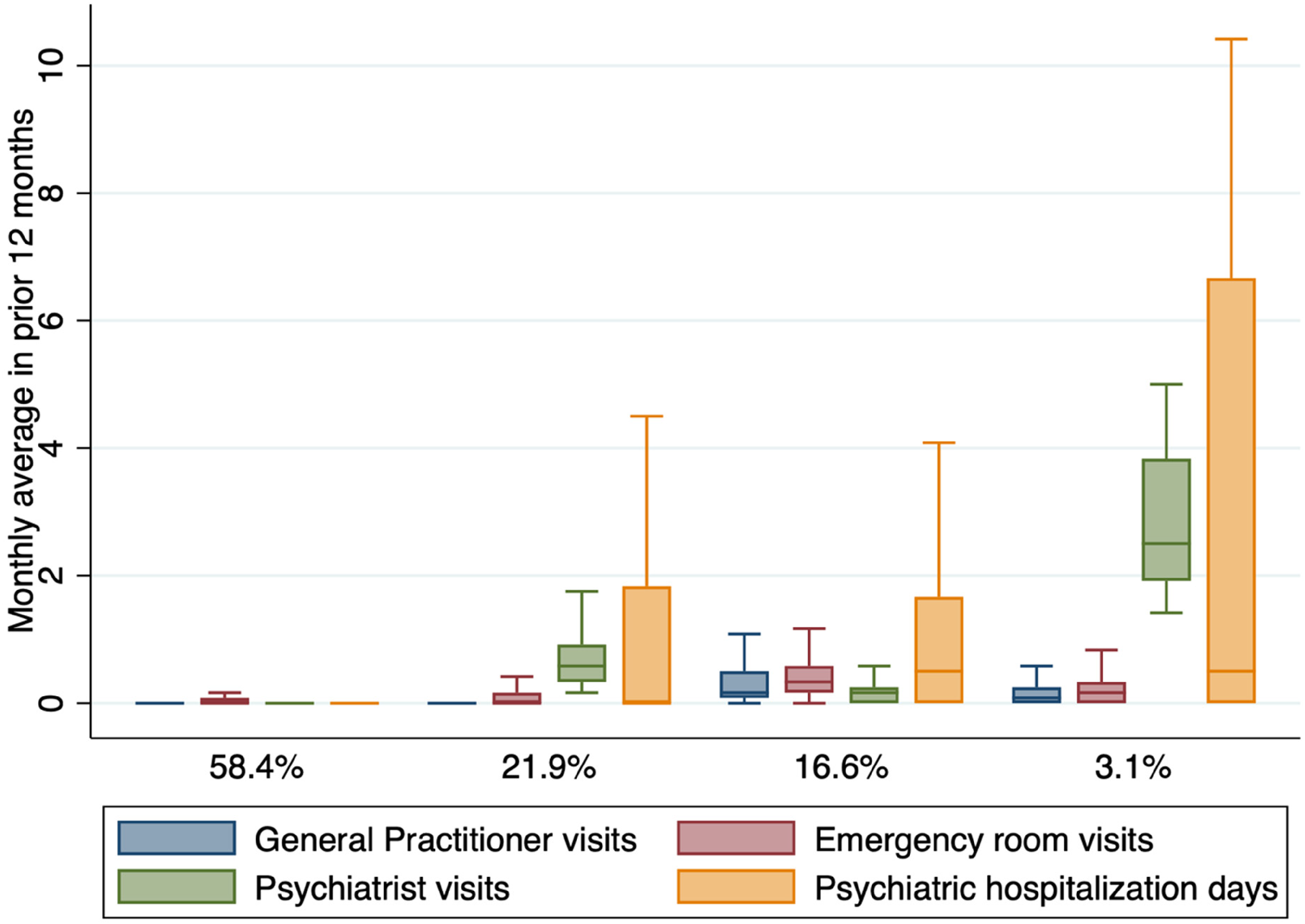
Patterns of mental health service use. The box plots represent the distribution of monthly average service use in the 12 months prior to the offense leading to a verdict of non criminal responsibility on account of a mental disorder (NCRMD). The boxes represent the interquartile range and are divided by a line that represents the median.
Detailed Service Use in the 12 Months Prior, by Mental Health Use Pattern.
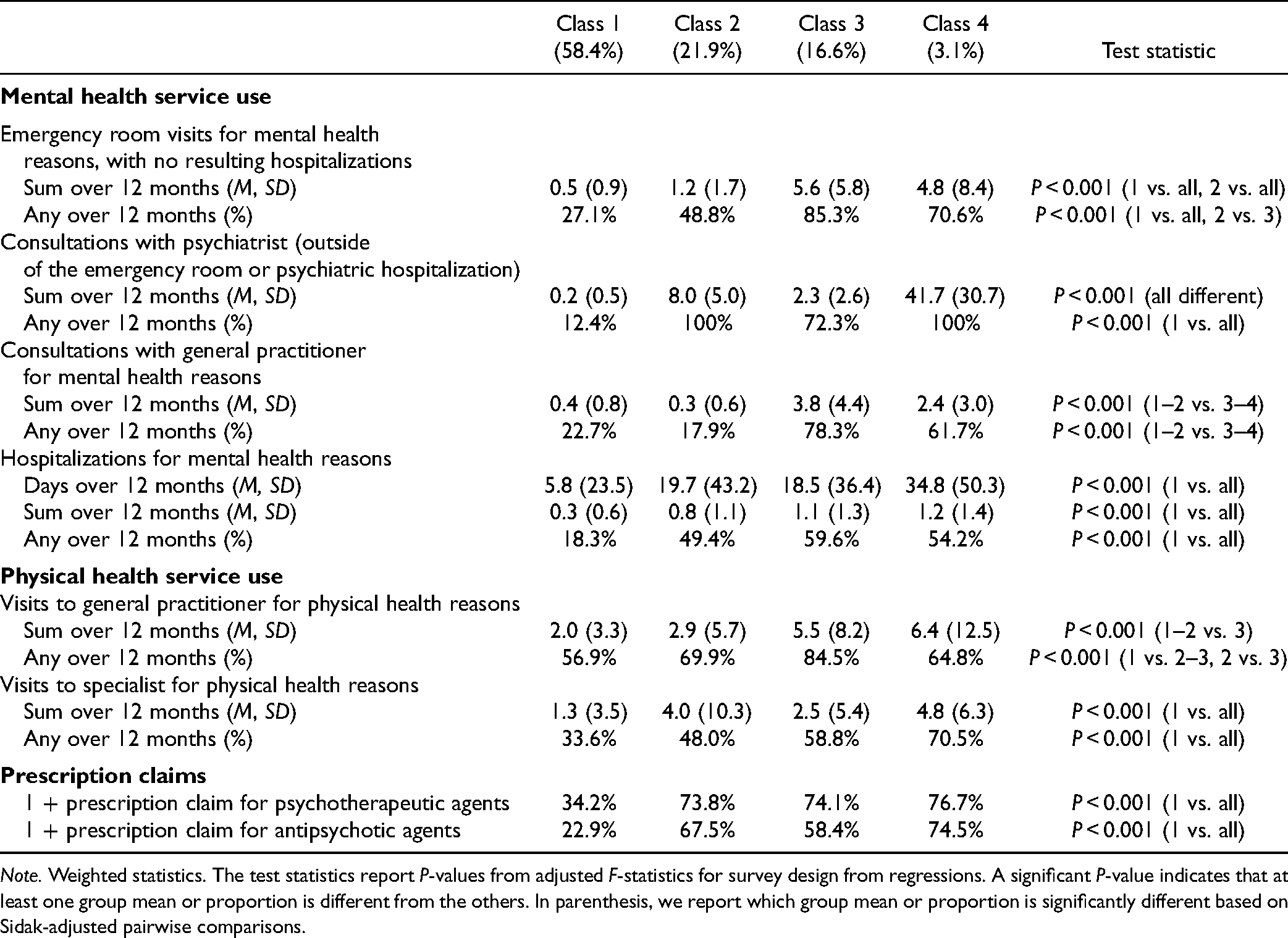
Note. Weighted statistics. The test statistics report P-values from adjusted F-statistics for survey design from regressions. A significant P-value indicates that at least one group mean or proportion is different from the others. In parenthesis, we report which group mean or proportion is significantly different based on Sidak-adjusted pairwise comparisons.
The three other classes presented qualitatively different service use patterns but were similar in terms of other characteristics (see Table 3). Class 2 (21.9%) comprised participants with a pattern consistent with specialized care, with relatively frequent psychiatrist consultations, but few visits to primary care or emergency room for MH reasons. Class 3 (16.6%) comprised participants with a pattern of primarily non-specialized care, with the greatest mean of visits to general practitioners and the emergency room. Finally, class 4 (3.1%) included individuals with a pattern of highly intensive service use, with highly frequent psychiatrist consultations, but also emergency room visits and primary care visits.
Sociodemographic, Clinical and Offense- or Justice-Related Characteristics, by Mental Health Use Pattern.
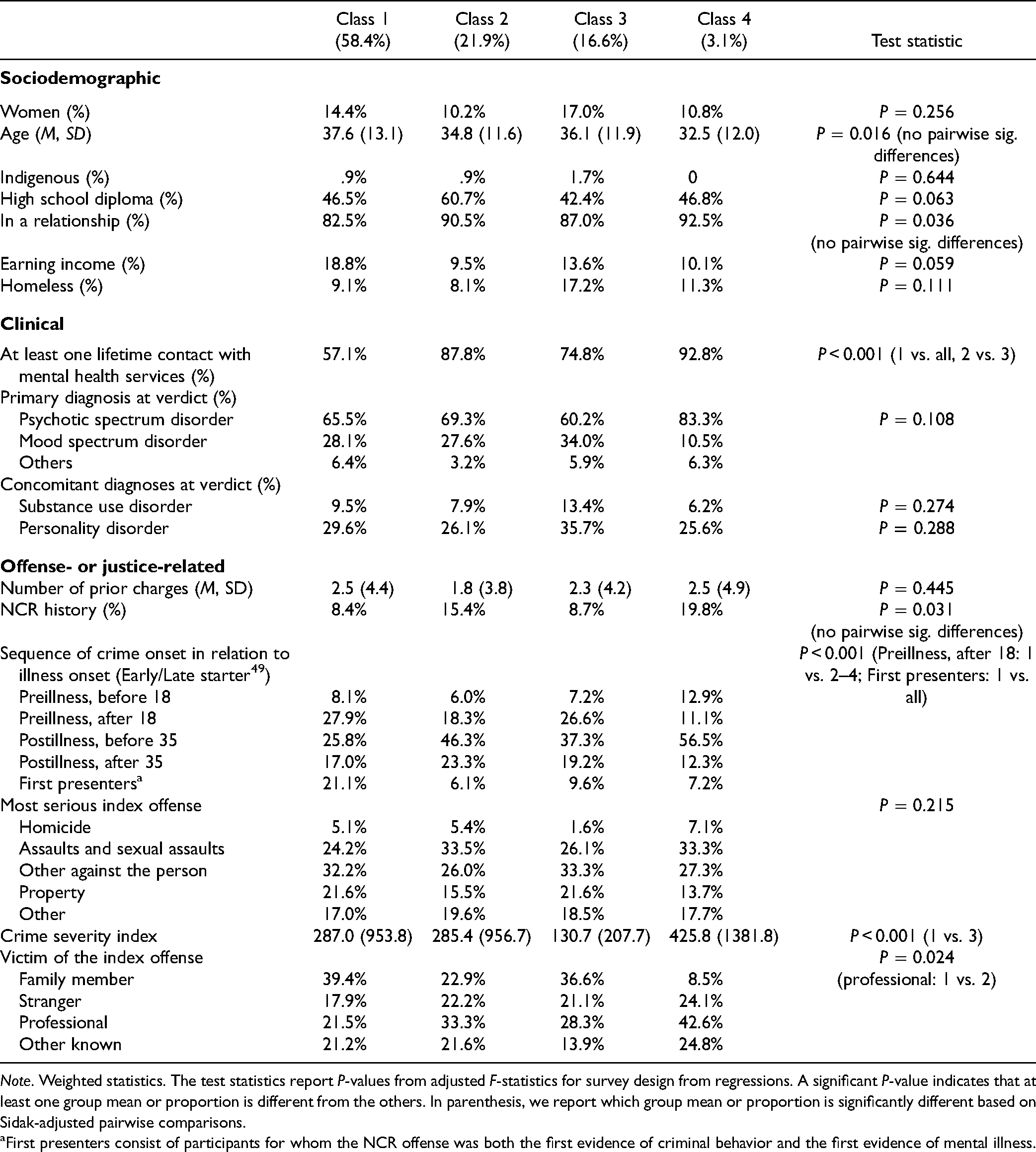
Note. Weighted statistics. The test statistics report P-values from adjusted F-statistics for survey design from regressions. A significant P-value indicates that at least one group mean or proportion is different from the others. In parenthesis, we report which group mean or proportion is significantly different based on Sidak-adjusted pairwise comparisons.
First presenters consist of participants for whom the NCR offense was both the first evidence of criminal behavior and the first evidence of mental illness.
Discussion
The present paper is the first study to provide a clear picture of the frequency, nature, and pattern of health services use, including prescription claims, of a large group of people found NCRMD prior to their offense. It highlights that around half of future forensic patients receive no consistent care within the MH system in the year prior to their offense despite being known by MH services for a severe mental illness. While it is possible that some participants received MH services that were not available through our dataset, for example from a salaried physician or another professional 2 , this finding may also suggest that many forensic patients are likely to have, voluntarily or involuntarily, experienced service disruption while in the community, for reasons that may relate to perceived need for care or to the acceptability, availability, and accessibility of services. 31 For example, data indicate that patients are often discharged from a psychiatric hospitalization with no follow-up appointments, either scheduled or attended. Research has shown that about one third of patients with severe mental illness disengage from MH services, 32 and that a forensic history is a predictor of disengagement, as service users report not being listened to by providers, 33 perceiving the providers’ attitude as negative or discriminating, and experiencing service discontinuity. 34
On the other hand, our findings show that a large proportion of individuals accesses care, often with monthly psychiatrist consultations. Notably, reasons for MH service use before an offense are different from those from a cohort of people incarcerated in provincial jails. 35 Less than 5% of all psychiatric hospitalizations were for substance-related disorders in the NCRMD sample, compared to a third among people found criminally responsible. 35 We did not find any differences between patterns of MH service use in terms of other characteristics, which suggests that systemic factors may play a more important role than individual factors.
Together with the finding that many committed the NCRMD offense within a short period after a MH services contact, this turns the attention towards potential for early intervention in terms of violence and justice involvement prevention within the health care system (potential intervention strategies are detailed below, in the implications). While it is not possible to know with certainty who will be admitted to forensic MH services in the near future, early intervention can target service users that have a severe mental illness and are at risk of criminal justice involvement, based on risk assessments.
Analysis of the pharmaceutical data suggests that half of those who had a prescription claim for an antipsychotic were no longer on any antipsychotic at the time of the offense. This result is consistent with those of a study of antipsychotic discontinuation in Québec, which found that continuation of antipsychotic therapy was very low, both among new users (around 5.5% at 1-year) and among past users beginning a new course of treatment (less than 5% at 1-year). 36 Unfortunately, given the administrative nature of the present dataset, it is unclear what proportion of treatment discontinuations is the result of a decision made by the patient, the physician, or both. A recent review of MH service users’ experiences highlight that the decision to discontinue medication may be motivated by the desire to regain a certain sense of control and autonomy, 37 highlighting the importance that providers work with the patients when it comes to the subject of medication and discuss acceptability and potential side effects so that they can make an informed decision that respects their right to self-determination. In fact, a systematic review found that therapeutic alliance and illness literacy were among the most important dynamic predictors of treatment adherence in patients with schizophrenia or bipolar disorder. 38 It should also be highlighted that, for some service users, compliance may be improved using long-acting injectable antipsychotics. An ethnographic examination of barriers to using long-acting injectable antipsychotics suggested that psychiatrists unnecessarily restrict the prescription of long-acting injectable antipsychotics to service users with demonstrated non-adherence to oral medication 39 , whereas algorithms suggest considering and discussing this option with most patients. 40
Implications
Our findings highlight the opportunity for greater involvement from primary care clinicians and general psychiatry clinicians in the early prevention of entry to forensic services through a NCRMD offense. There is a need for an in-depth investigation of strategies for engaging and supporting them in playing this pivotal role.
For the past decades, services have been highly fragmented, and the role of coordinating care has been relegated to the service user and their loved ones. A qualitative meta-synthesis of the experience of pathways to MH services highlight that patients and their caregivers often do not know what resources exist, experience difficulties with narrow eligibility criteria, and report lack of discharge planning after hospitalization and multiple unwanted service interruptions. 41 Navigating the system after the initial contact may prove to be a challenge for several patients, especially for those who have behaviors that can be perceived as disturbing or aggressive and be rejected by services. The present findings show that, while some receive sustained MH care, improving the integration of services to reduce fragmentation and service discontinuity may improve the quality of services received for many, and possibly reduce the need for forensic MH services. Several strategies to improve continuity of care among people with severe mental illness has been put forth, including community MH teams and assertive community treatment. 42 For those with past justice involvement, forensic assertive community treatment 43 could be used to address the psychiatric symptoms and the risk of additional offenses.
In addition to service fragmentation, the organization of clinical and financial resources in a reactive rather than preventative manner limits the possibility of the healthcare system to respond appropriately to the needs of patients with severe mental illness and disturbing or aggressive behaviors in a timely manner. Currently, the expertise and investments in violence and crime prevention are concentrated in highly specialized forensic MH services, which are accessible to patients only after an offense. Forensic MH services have traditionally been conceived as a tertiary care system, but there is an argument to be made for a balanced care continuum, with forensic-informed low-intensity community services as the lower tier and high-security custodial services as the upper tier. 6 This would require sharing the knowledge upstream and offer additional training to general practitioners, nurses, and psychiatrists. The scientific literature has discussed the potential of approaches based on the assessment of risk of violence in MH services, often using structural professional judgment tools that are increasingly implemented internationally 44 as they show promises assisting multidisciplinary and intersectoral teams in formulating and communicating a structured judgment regarding risk to prevent entry to forensic MH services or the criminal justice system more generally. 45
Limits and Future Studies
The present paper has some limitations. First, the data dates to 2000–2005—however, very little changes have been made to the organization of MH services in the past years, except for psychotherapy coverage by public insurance, to which access remains very difficult. Nevertheless, we would suggest that a replication study be done with a more recent sample, in Québec and other Canadian provinces. Such a study could also shed light on the prescribing practices and patterns of pharmacotherapy in this population, and compare with a matched sample of service users who were not admitted to forensic services to highlight the specific barriers and challenges experienced by people who are susceptible to justice involvement. Furthermore, exploring the pathway that leads to several NCRMD finding could be worth exploring in this context. 46 Second, while the RAMQ dataset provide a complete portrait of physician-provided services and prescription claims, it remains medically oriented and does not provide details regarding contacts with community organizations and other psycho-social services that can play a key role in risk assessment and management. Third, as discussed in the introduction, Québec is a unique jurisdiction in Canada when it comes to use of the NCRMD regime, but also in terms of the duration and criteria for community treatment order and involuntary hospitalization. 47 While this may limit the generalizability of the findings, it should be highlighted that the vast majority of people found NCRMD annually in Canada are in Québec, which suggests that our findings remain highly relevant. Finally, administrative health data provide very little explanations regarding the reasons behind lack of access, treatment interruptions, and discontinuity of care. A qualitative study to understand the experiences of services in the community by patients found NCRMD could shed light on barriers to accessing appropriate healthcare.
Conclusion
Given the serious impact of the “forensic” label on the lives of service users, not to mention the increased pressure on resources, the considerable economic costs, and the impact on victims, there is reason to advocate for a greater involvement of mental and physical health service providers in early prevention of violence or criminal offending, which requires reorganizing resources to share the forensic knowledge upstream, before an offense is committed. Equitable access to health services should also be further examined among people with severe mental illness and behaviors perceived as disturbing or aggressive, so that the care of this underserved population is better coordinated after an initial contact with services so that their needs are fully met, without having to use the justice system to access specialized, appropriate care.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437221076723 - Supplemental material for Care Pathways, Health Service Use Patterns and Opportunities for Justice Involvement Prevention Among Forensic Mental Health Clients
Supplemental material, sj-docx-1-cpa-10.1177_07067437221076723 for Care Pathways, Health Service Use Patterns and Opportunities for Justice Involvement Prevention Among Forensic Mental Health Clients by Marichelle C. Leclair, Yanick Charette, Malijaï Caulet and Anne G. Crocker in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
Marichelle Leclair acknowledges the financial support of the Canadian Institutes of Health Research in the form of a Vanier scholarship and of the Observatoire en justice et santé mentale as a fellowship while working on this manuscript. Yanick Charette received salary awards from the Fonds de recherche Québec—Santé.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Fonds de recherche du Québec - Santé (grant number 6356–2004) and a grant from the Mental Health Commission of Canada. The National Trajectory Project received funding from Fonds de recherche Québec—Santé Grant 6356–2004 and the Mental Health Commission of Canada.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.