
Abstract
Background:
Research on the mental health of medical students enrolled in Paraguayan universities has mainly examined the prevalence of anxiety and depression, with limited exploration of treatment access, barriers, and facilitators. Additionally, substance use, such as alcohol and other substances, is of significant concern because of its association with mental health issues. This study aimed to assess the prevalence of depression, anxiety, and substance use disorders, as well as to identify barriers and facilitators influencing medical students’ access to mental health and substance use treatment in the Republic of Paraguay.
Methods:
A national mixed-methods cross-sectional study was conducted with 532 medical students from public and private universities across the Republic of Paraguay. Data were collected via an online survey in 2024 using validated tools to measure mental health conditions, including alcohol and other substance use. Qualitative responses regarding barriers to and facilitators of treatment were categorized and analyzed.
Results:
The findings revealed high rates of anxiety (76.8%) and depression (39.3%). Substance use was also concerning, with 11.1% reporting alcohol-related problems and 1.9% reporting other substance-related problems. Barriers to seeking treatment included confidentiality concerns, stigma, and financial constraints, while facilitators included trust in the mental health system, emotional distress, and accessibility. Despite the availability of these services, many students felt unsupported by their universities.
Conclusions:
Paraguayan universities must urgently address the stigma surrounding mental health and substance use, improve service accessibility, and build trust in the academic environment. Tackling these issues is crucial for safeguarding medical students’ mental health and future.
This study identified high rates of anxiety and depression among medical students enrolled in Paraguayan universities, highlighting significant mental health challenges. Stigma, confidentiality concerns, and financial constraints were key barriers to accessing mental health services despite university-provided resources. The study findings emphasize the need for Paraguayan universities to enhance mental health support by emphasizing accessibility, reducing stigma, and building trust.Key Messages:
Medical students encounter significant challenges affecting their mental health and well-being. Studies indicate that academic pressures, including a demanding curriculum, limited free time, frequent exams, and high-performance expectations, are primary stress sources.1,2 These pressures often result in psychological distress, such as anxiety and depression, which are more common among medical students than the general population.3–5 Numerous studies conducted in the Republic of Paraguay have examined the prevalence of mental health disorders, such as anxiety and depression, among medical students.6–11 However, the specific barriers and facilitators influencing students’ decisions to seek mental health treatment remain underexplored, which is the central focus of this study. Mental health stigma in Latin American medical schools heightens students’ reluctance to seek help. The fear of being deemed unfit for medical practice often discourages students from disclosing mental health issues and seeking treatment. 12 Consequently, many universities in the region, including the Republic of Paraguay, have started providing mental health services. However, their effectiveness and accessibility need further evaluation. 13 This study fills this gap by employing a mixed-methods approach to examine the prevalence of depression, anxiety, and substance use, and the attitudinal, stigma-related, and logistical barriers to seeking treatment.
This study examined barriers and facilitators using both quantitative and qualitative methods. By involving medical students from the capital city (Asunción) and 11 out of the 17 departments in the Republic of Paraguay, this study provides a diverse sample that captures a wide range of experiences. The findings aim to inform policy enhancements in mental health services across Paraguayan universities and support broader efforts to improve medical students’ well-being throughout Latin America.
Methods
Ethical Considerations
This study received approval from the Department of Medical Psychology of the School of Medical Sciences at the National University of Asuncion, Paraguay (Reference 011-007-2024). All data were handled with confidentiality, equality, and justice, in alignment with the principles of the Declaration of Helsinki. The survey was conducted anonymously, and no identifying information was collected. Data were stored securely in password-protected systems accessible only to the research team. To ensure data integrity and avoid duplication, the survey system was configured to allow only one response per participant, and responses were reviewed for inconsistencies. Although it was not possible to identify participants who screened positive for mental health concerns or those who reported sexual harassment, all participants were provided with clear and accessible information about available mental health services and institutional reporting mechanisms. This manuscript follows the STROBE cross-sectional reporting guidelines, which are available as supplementary online material.
Design and Participants
This observational, mixed-method, cross-sectional study was conducted nationwide in the Republic of Paraguay through an online survey using nonprobabilistic consecutive sampling. 14 Data were collected from July 1 to August 31, 2024. Medical students aged 18 years or older from both public and private universities across the country voluntarily participated. The survey, disseminated via WhatsApp, Telegram, and email, provided participants with information regarding the study’s purpose, privacy considerations, and data handling prior to completion. Incomplete responses were excluded from the analysis. It is worth noting that online surveys have been shown to yield reliable and comparable results to those obtained from in-person samples. 15
Measures
Demographic and Academic Data
Participants disclosed their age and biological sex (male and female) and identified their gender (male, female, non-binary). 16 The categories used aimed to respect participants’ self-identification and provide flexibility for individuals with diverse gender identities. This approach aligns with recognized frameworks for gender diversity. 16 Additionally, they disclosed their nationality (multiple responses allowed) and Indigenous group affiliation in the Republic of Paraguay (yes, no). They reported their living arrangements (with family/partner, friends/roommates, or alone), their university type (public, private), the region of their University in the Republic of Paraguay, their academic year (first to sixth year), and whether they had employment alongside their studies.
Mental Health Status
Participants disclosed their primary stressors through a multiple-choice question with predefined options, including studies, finances, work, family, and others. Participants were instructed to select all applicable options from the provided list. The PHQ-2, GAD-7, and MULTICAGE CAD-4 were utilized to evaluate depression, anxiety, and alcohol and substance use, respectively.
The Patient Health Questionnaire 2-Item (PHQ-2)
The PHQ-2 developed by Kroenke, Spitzer, and Williams includes the first two items from the nine-item Patient Health Questionnaire. 17 These items assess depressed mood and anhedonia over the past two weeks, the primary symptoms of depressive disorders. The PHQ-2 employs a 4-point Likert scale, with responses from 0 (not at all) to 3 (almost every day). A score of ≥3 suggests depression, with 83% sensitivity and 92% specificity for major depression. 17 This study utilized the Spanish version of the PHQ-2, which has demonstrated good reliability in previous research. 18
The Generalized Anxiety Disorder 7-Item (GAD-7)
The GAD-7 is a self-administered scale measuring generalized anxiety disorder symptoms through seven items scored from zero to three, yielding a total score between 0 and 21. Cut-off scores for mild, moderate, and severe anxiety are 5, 10, and 15, respectively, with a score of 10 or higher indicating potential GAD cases. 19 This study employed the Spanish version of the GAD-7, which showed strong psychometric properties. 20
The MULTICAGE Questionnaire of the Drug Dependency Care Center (CAD) San Blas of the Addiction Institute of Madrid Health (MULTICAGE CAD-4)
The MULTICAGE CAD-4 is a validated scale for assessment of Alcohol abuse/dependence and substance addiction. 21 Each issue is examined through four questions modeled after the CAGE scheme, covering self-perception, perception by cohabitants, guilt, and withdrawal or control issues. 22 The self-administered questionnaire uses a Yes/No scale, where none or one affirmative response indicates no problem; two affirmative responses suggest a possible problem; three responses indicate a probable problem; and four responses confirm the presence of a problem. A total of two or more affirmative responses per scale denotes problematic behavior. The full scale and its subscales demonstrate good psychometric properties. 21
Treatment Needs
Drawing from Wang et al.’s study and the 2019 National Survey on Drug Use and Health (NSDUH), the CAI Specifications for Programming, our questionnaire asked participants whether they had received substance use services (excluding cigarettes/e-cigarettes) or mental health services in the past 12 months (yes/no).23,24 Additionally, we inquired about any unmet treatment needs during this period. Participants who reported unmet needs for substance use or mental health treatment cited eight reasons for not seeking care, categorized into attitudinal, stigma-related, and instrumental barriers:25–27
Attitudinal Barriers
Concerns about confidentiality or consequences of disclosing information (e.g., legal trouble, forced treatment).
The belief that services would not help or that the problem could be handled independently.
Stigma-related Barriers
Embarrassment or fear of others’ opinions.
Concern about negative effects on academic or employment opportunities.
Instrumental Barriers
Concerns about service costs.
Lack of knowledge on where or how to access services.
Scheduling challenges (e.g., limited time, inconvenient hours).
Transportation difficulties (e.g., no transport, inconvenient location).
Mental Health Services at the University and Barriers and Facilitators to Treatment
Based on the research by Amarilla et al., participants were asked about the presence of any formal mechanisms for counseling or treating mental health issues at their University, such as a mental health department or designated professionals. 13 Participants were questioned about their comfort in disclosing mental health issues to family, friends, university peers, professors, and mental health advisors. Additionally, they were asked to report any experiences of mistreatment or sexual harassment by professors or peers. As in Wang et al., participants were asked open-ended questions about their mental health treatment experiences during medical school. Initially, we inquired about the extent of university support for mental health services and treatments for themselves or their peers. We then asked if they had ever used the school’s counseling services, followed by a question seeking reasons for or against seeking such services. 23 We asked participants who had sought school counseling about facilitators and categorized them into attitudinal, emotional, and instrumental groups. For those who had not sought school counseling, we inquired about barriers, which we categorized into attitudinal, stigma-related, and instrumental groups.25–27
Sample Size
The sample size was determined using Epidat 4.2 (Pan American Health Organization, Junta de Salud de Galicia, and Universidad CES de Colombia). The minimum required sample size was set at 530 participants, considering a 95% confidence level, a 4% precision, and an anticipated anxiety rate of 67.2% among medical students enrolled in Paraguayan universities.28,29
Data Analysis
Jamovi and RStudio were utilized for quantitative analysis. Descriptive statistics, including frequency tables, summarized categorical variables, while measures of central tendency and dispersion were used for numerical variables. The chi-squared (χ²) test assessed associations between categorical variables, with odds ratios (OR) and 95% confidence intervals (CIs) estimating the strength of these associations. The significance level was set at 5% (P < .05) for all tests.
For qualitative analysis, participants’ responses to open-ended questions about barriers and facilitators for treatment were examined. Facilitators were categorized into attitudinal, emotional, and instrumental, while barriers were categorized as attitudinal, stigma-related, and instrumental, with agreed definitions. Two researchers reviewed and categorized participants’ responses, which were then merged, and two additional researchers resolved discrepancies. The research team met periodically to clarify any unclear responses.
Results
Demographics
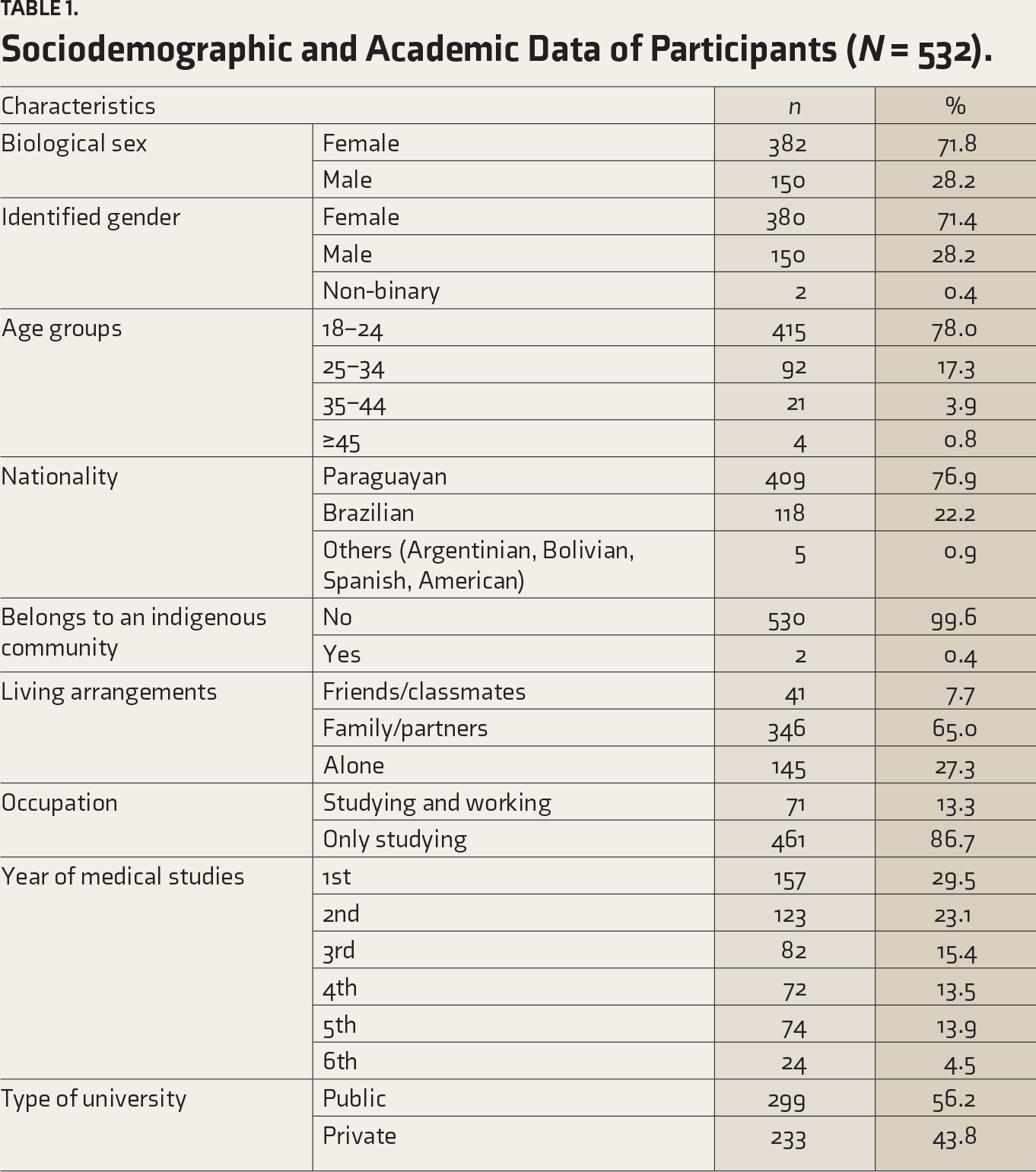
The study involved 532 medical students, averaging 22.93 years old (SD = 5.11), with ages ranging from 18 to 52. Participants were from the capital city, Asunción, and 11 out of the 17 departments in the Republic of Paraguay. Table 1 indicates that 71.8% were biologically female and 76.9% were Paraguayan, followed by 22.2% Brazilians. Regarding living arrangements, 65% resided with family or partners, while 27.3% lived alone. Additionally, 86.7% were solely dedicated to studying, with 13.3% also working.
Sociodemographic and Academic Data of Participants (N = 532).
Mental Health Status
Regarding stressors, 88.9% of students cited academic studies as a major stress source, followed by economic concerns (62.2%) and family issues (46.4%). Depressive symptoms were found in 39.3% of students using the PHQ-2 scale. Additionally, 76.8% screened positive for anxiety with a GAD-7 score of 10 or higher. Alcohol-related problems were reported by 11.1% of students, while 1.9% reported substance addiction, as assessed by the alcohol and substance addiction subscales of the MULTICAGE CAD-4 (Table 2).
Mental Health Status of the Participants (N = 532).
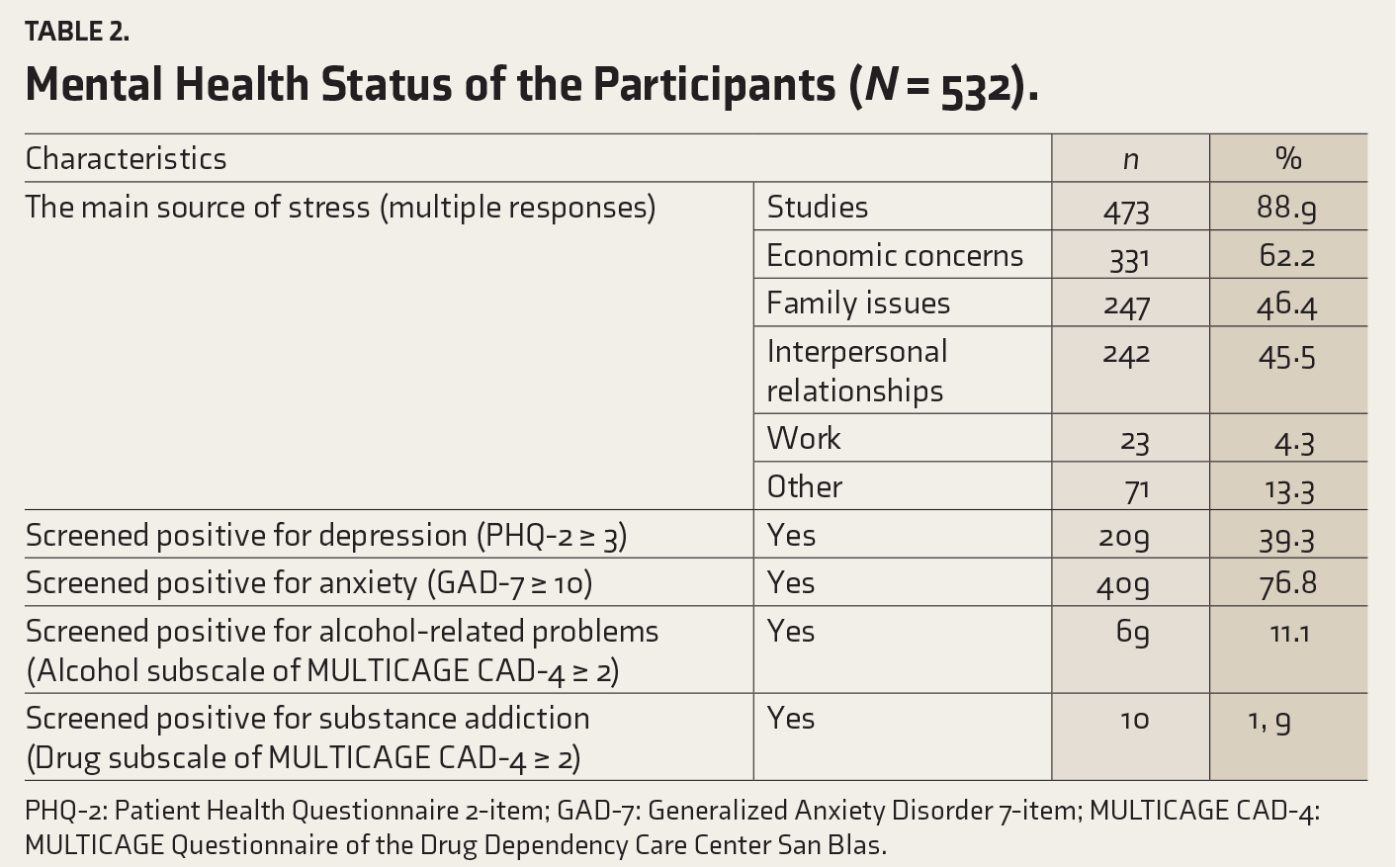
PHQ-2: Patient Health Questionnaire 2-item; GAD-7: Generalized Anxiety Disorder 7-item; MULTICAGE CAD-4: MULTICAGE Questionnaire of the Drug Dependency Care Center San Blas.
The inferential analysis on anxiety using the χ² test between biological sex and GAD-7 (χ² = 23.74; P < .01) showed a significant association. Female students had a higher prevalence of anxiety, with 315 females scoring positive compared to 94 males. The odds ratio for biological sex (female/male) was 2.80 (95% CI: 1.84–4.28), indicating that women are nearly three times more likely to experience anxiety than men. The χ² analysis between biological sex and the MULTICAGE CAD-4 drug subscale (χ² = 5.09; P = .02) revealed a significant difference. Males exhibited a higher prevalence of substance use, with six positive cases compared to four among females. Men were almost four times more likely to report substance use than women (odds ratio: 3.94, 95% CI: 1.09–14.16). Although the non-binary category of identified gender was included in the study, its small sample size did not allow for inferential statistical analyses.
A significant association was found between the drug subscale of the MULTICAGE CAD-4 and PHQ-2 categories (χ² = 4.03; P = .04), indicating a strong correlation between substance use and depressive symptoms. The odds ratio for individuals scoring positive on the drug subscale of the MULTICAGE CAD-4 was 3.70 (95% CI: 0.94–14.46), suggesting they were over three times more likely to exhibit depressive symptoms compared to those not reporting substance use. No other associations were found.
Treatment Needs
Over the past year, three participants (0.6%) received treatment for alcohol or other substance use, and seven (1.3%) needed but did not receive such services. All these individuals screened positive for alcohol-related issues (Alcohol subscale of MULTICAGE CAD-4 ≥ 2), and 14.2% screened positive for substance addiction (Drug subscale of MULTICAGE CAD-4 ≥ 2). Additionally, 129 participants (24.2%) received mental health treatment, whereas 261 (49.1%) reported an unmet need for mental health services. Among them, 48.6% screened positive for depression (PHQ-2 ≥ 3) and 86.2% for anxiety (GAD-7 ≥ 10). Table 3 lists the reasons for not seeking treatment among those with unmet needs for substance use or mental health services, with cost concerns being the most prevalent in both groups.
Reasons for Not Seeking Care Among Those Who Endorsed an Unmet Need for Care.
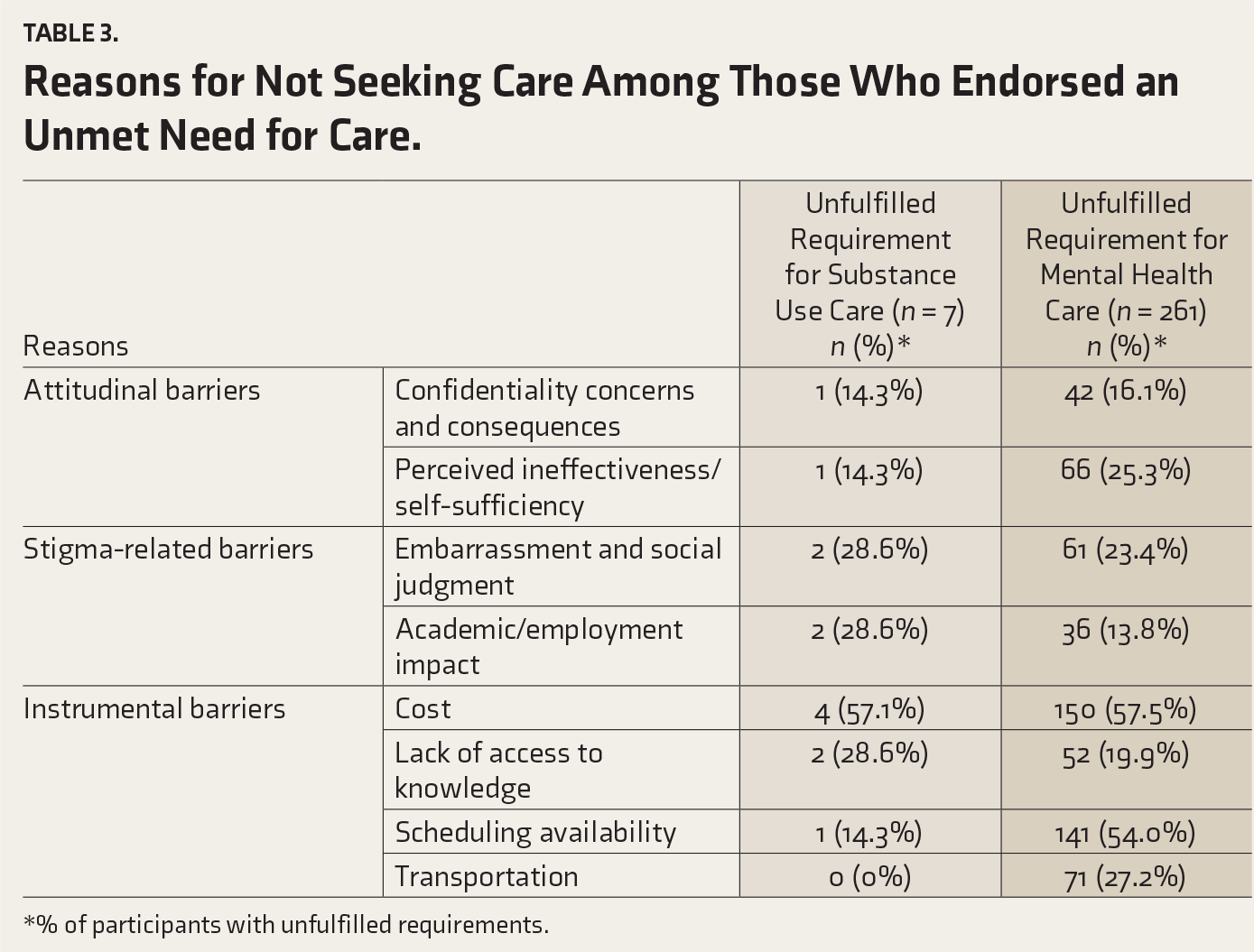
*% of participants with unfulfilled requirements.
Mental Health Services at the University and Barriers and Facilitators to Treatment
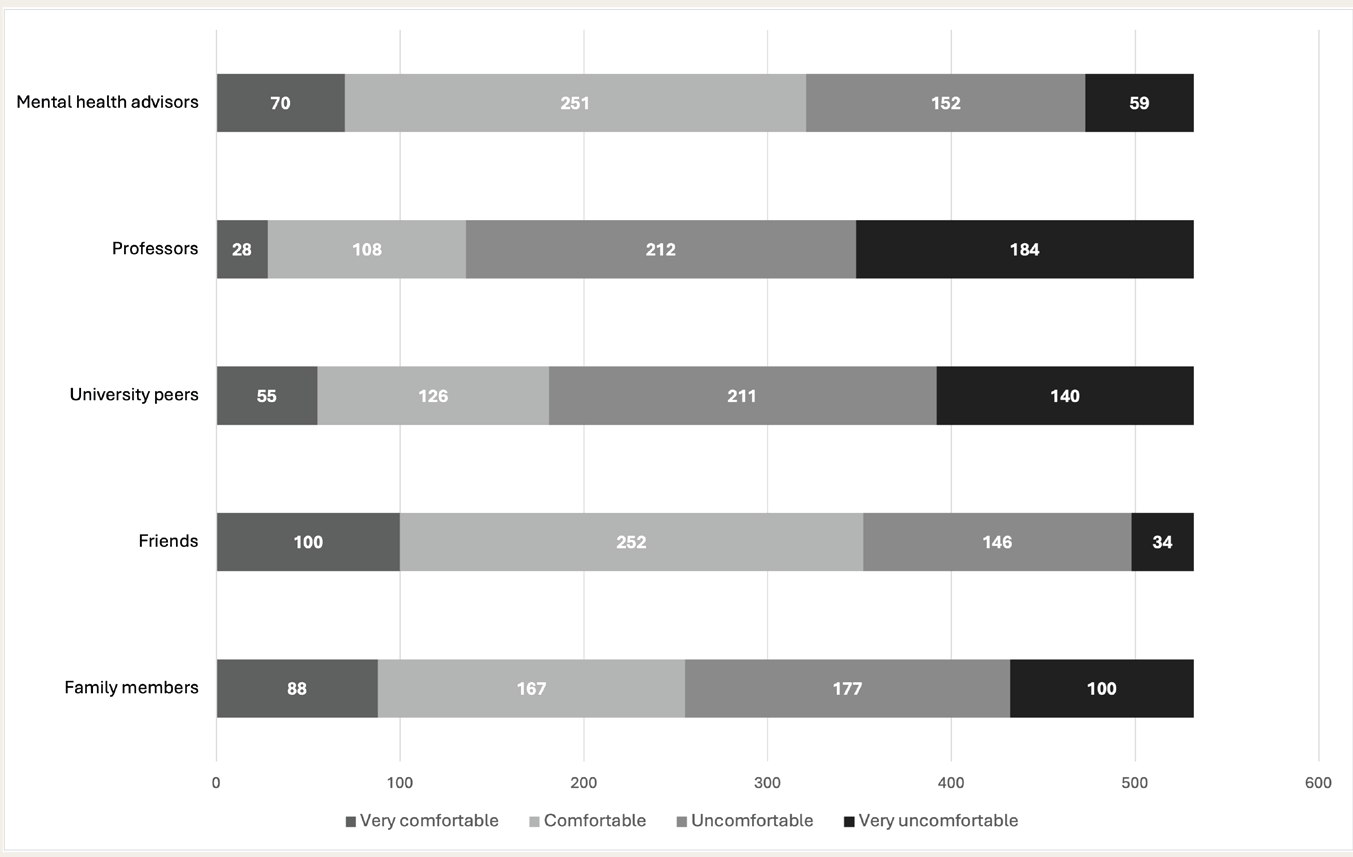
Among the participants, 415 (78.0%) indicated that their university had an official entity offering mental health counseling or treatment (e.g., a mental health department or designated professionals). However, 311 participants (58.45%) expressed feeling uncertain or rarely supported by their university when they or their peers needed mental health services, while only 16.7% reported feeling well-supported. Participants generally felt comfortable (n = 252) or very comfortable (n = 100) disclosing mental health issues to a friend, whereas they felt uncomfortable (n = 212) or very uncomfortable (n = 184) disclosing the same to a professor. Figure 1 displays the varying comfort levels reported by medical students regarding mental health disclosures.
Participants’ Level of Comfort in Disclosing Mental Health Issues (N = 532).
Among the participants, 85 (16.0%) reported mistreatment by professors and 66 (12.4%) by peers; additionally, 10 participants (1.9%) reported sexual harassment by both professors and peers.
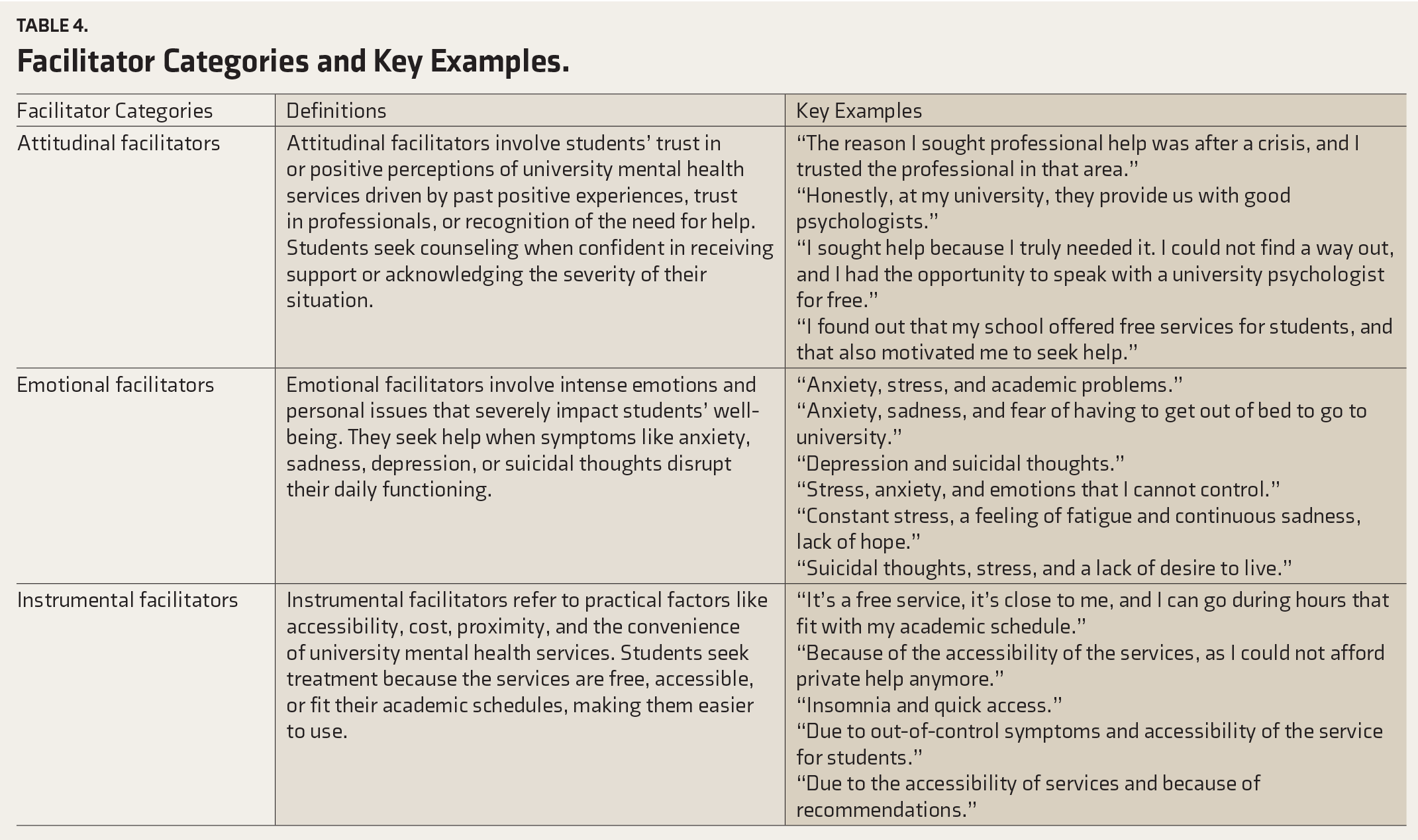
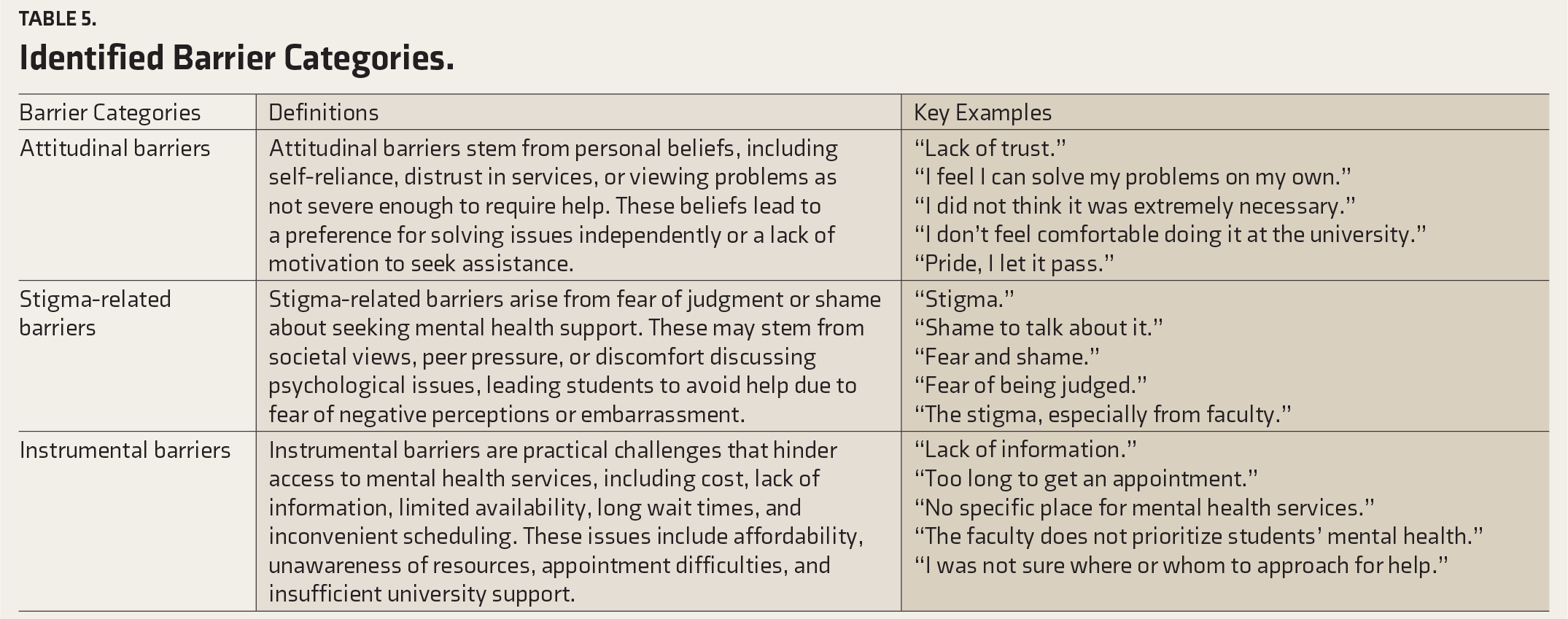
Qualitative analysis identified various facilitators for seeking mental health treatment, categorized into attitudinal, emotional, and instrumental groups, with specific definitions established for each.25–27 The categories of facilitators, along with key exact quotes from the open-ended responses, are presented in Table 4 (Supplementary online material). The participants noted several barriers to seeking mental health treatment in medical schools. These barriers were categorized into attitudinal, stigma-related, and instrumental barriers, and specific definitions were similarly agreed upon for each.25–27 Table 5 displays the identified barrier categories, accompanied by key verbatim quotes from the open-ended responses (Supplementary online material).
Facilitator Categories and Key Examples.
Identified Barrier Categories.
Discussion
To the best of our knowledge, this is the first published Latin American mixed-methods study examining medical students’ mental health and treatment needs, identifying barriers and facilitators to seeking treatment for mental health and substance-use issues. Academic studies were the primary stressor, with nearly 90% of the participants noting their significance. Economic concerns affected over half of the respondents, and almost half of them mentioned family-related issues. These findings align with prior research on medical students enrolled in Paraguayan universities, emphasizing academic pressure, financial challenges, and family issues as major stressors.12,30 Stress is well-documented among medical students, with academic demands being the primary source of stress. Manandhar and Pramanik identified academic stressors as the most significant, followed by social pressures. 31 Pérez-Dominguez et al.’s multi-center study found that Latin American medical students faced greater stress than their non-Latin American counterparts, mainly due to academic demands. 32 Financial concerns also significantly contribute to stress, as students worry about their economic situation, which impacts their academic performance and well-being. 33 In Latin America, financial instability and high medical education costs exacerbate this stress. 34 Family issues further burden students, with research showing that family expectations and responsibilities intensify stress. 35 The interplay of academic, financial, and familial stressors necessitates comprehensive support systems to ensure the well-being and success of future healthcare professionals.
Our findings revealed a high prevalence of depression (39.3%) and anxiety (76.8%) among the screened individuals. This aligns with recent studies highlighting the elevated rates of mental health issues in medical students compared with the general population, emphasizing the need for improved mental health support in medical education.36,37 A Latin American multi-center study found anxiety and depression symptoms in 87.14% and 66.88% of medical students, respectively. 38 In Brazil, research has reported a prevalence of 29.8% for depression, 30.1% for anxiety, and 25.3% for stress among medical students. 39 A study in the Republic of Paraguay using the PHQ-2 and GAD-7 found that 60.3% of university students reported symptoms of depression, and 58.5% reported symptoms of anxiety. 40 In a separate study focusing on medical students, 49.6% screened positive for depression and 67.2% screened positive for anxiety. 28 Our analysis of anxiety concerning biological sex found a significant correlation between gender and anxiety disorder prevalence, consistent with research showing females report higher anxiety levels than males. 41 In Latin America and the Republic of Paraguay, female medical students have higher mental health disorder rates than males.12,38 Biological factors, psychosocial stressors, and societal expectations may contribute to this disparity, exacerbating mental health symptoms in women.42–44
In our study, 11.1% of participants reported alcohol-related problems, while 1.9% reported substance addiction. Medical students appear particularly vulnerable to substance use due to academic pressures, often using alcohol and other substances as coping mechanisms, thereby reinforcing the link between stress and substance use in this population.45–47 Our analysis also revealed a significant gender difference in substance use, with men being almost four times more likely to use substances compared to women. This finding aligns with broader research indicating that men generally have higher rates of illicit substance use compared to women. 48 Supporting evidence also indicates that male medical students report higher substance use rates due to cultural and social factors.49,50 Research has indicated a significant link between substance use and depressive symptoms among medical students. Our findings show that students using substance are over three times more likely to exhibit depressive symptoms compared to non-users. This finding supports the existing literature on the strong correlation between substance misuse and mental health issues, particularly depression. Santosh et al. observed that academic pressure drives substance use among medical students as a coping mechanism. 51 Al-Farhan et al. highlighted the need to examine substance abuse prevalence and its mental health consequences in this population. 52 Furthermore, stress from medical training is a significant factor contributing to substance abuse and depressive symptoms. 53
In our study, 48.6% of medical students with positive depression screening and 86.2% with positive anxiety screening reported unmet mental health needs. Additionally, 100% of those with alcohol-related problems and 14.2% of those with substance addiction reported a lack of care. These findings are significant, as untreated mental health problems can harm academic performance, clinical skills, and overall well-being, affecting both individual students and the broader healthcare system.54,55 Our study identified significant barriers to mental health care among medical students, persisting through higher training levels and potentially causing dropouts.23,56 Economic concerns were reported as primary instrumental barriers. University students face obstacles, including costs, lack of information, limited availability, long wait times, and inconvenient scheduling. Financial constraints notably deter help-seeking; for instance, high service costs in Bangladesh lead students to prefer digital health solutions. 57 Students with lower socioeconomic backgrounds encounter greater financial barriers. 58 Scheduling conflicts were also common, especially for students balancing academics and part-time jobs, resulting in missed appointments and reduced help-seeking. 59 Our qualitative analysis confirmed that medical students face several barriers, including a lack of information, insufficient support, and long wait times for mental health services. Additionally, academic pressure reduces students’ availability to seek help. Many participants also reported institutional shortcomings, such as a lack of prioritization of mental health, inadequate facilities, and staffing shortages. 59
Quantitative and qualitative analyses revealed stigma-related barriers to seeking mental health care, with 13.8% to 28.6% of participants refraining due to embarrassment, fear of others’ opinions, and potential negative impacts on their academic reputation or future employment. Participants emphasized stigma from faculty, using terms like “stigma,” “shame,” and “fear.” Research indicates that concerns about confidentiality and stigma significantly deter medical students from seeking help. This aligns with findings of widespread stigmatizing attitudes toward mental illness among medical students globally, which are influenced by the high stress and competitive nature of medical education, among other factors.60,61 In the Republic of Paraguay, mental health issues are highly stigmatized, leading students to avoid seeking help for fear of rejection, differential treatment, or being deemed unfit for medical practice, which is justified by the ostracization and mistreatment faced by students open about their mental health struggles.2,12 This challenging environment exacerbates the difficulties faced by students already struggling with their mental health. Attitudinal barriers were reported by approximately one in four individuals with unmet mental health needs and one in ten individuals with substance-related issues. Medical students cited reasons such as “lack of trust,” belief in self-sufficiency, or viewing help as unnecessary. Research shows that barriers such as self-sufficiency beliefs and discomfort with professional help are common. Several studies have found that individuals often preferred handling problems independently and doubted mental health care effectiveness.57,62,63 Medical students frequently expressed views like “I let it pass” or “I did not think it was extremely necessary,” indicating a preference for personal coping over professional help. 63 These barriers contribute to students’ reluctance to seek necessary assistance.
Our research identified several attitudinal, emotional, and instrumental factors that encourage students to seek mental health support. Attitudinal facilitators, such as trust in university services, positive past experiences, and self-recognition of the need for help, are motivating factors. Medical students are more likely to seek counseling when they believe that they will receive effective support. Furthermore, respondents mentioned trust in professionals and free service availability as motivators, with comments such as, “The reason I sought professional help was after a crisis, and I trusted the professional in that area” and “I found out that my school offered free services for students, and that also motivated me to seek help.” These responses highlight the significance of trust and accessibility in promoting mental health care. 64
Previous research indicates that mental health symptoms significantly drive help-seeking behaviors. These “emotional facilitators” stem from intense emotions or personal struggles that severely impact students’ well-being. Students seek support when symptoms, such as anxiety, sadness, depression, or suicidal thoughts, become overwhelming and disrupt their functioning. Research shows that intense emotions, such as anxiety, depression, and hopelessness, significantly drive students to seek mental health care. For instance, studies have indicated that medical students with high levels of anxiety and depression are more likely to recognize their need for mental health services. 23 Wakefield et al. noted that viewing help-seeking as courageous rather than dependent facilitates this process. 65 In the qualitative analysis, students emphasized how emotional distress drives their urgent need to seek help. These findings emphasize the crucial role of emotional distress in motivating students to pursue mental health care.
Approximately 80% of the medical students surveyed reported that their university offered formal counseling or mental health treatment services. These services act as instrumental facilitators, where accessibility, cost, proximity, and convenience encourage students to seek help, aligning with the literature that emphasizes the importance of accessible mental health services in educational settings. 66 Over half of the participants felt unsupported by their university when seeking mental health services, citing distrust and dissatisfaction as barriers to seeking help, a finding corroborated by other researchers. 67 Students often feel unheard, their concerns ignored, and that medication is prioritized over other treatments, necessitating a review of care practices to improve accessibility, efficiency, and student-friendliness. 13 Most participants felt comfortable disclosing a mental health issue to a friend but uncomfortable with a professor, fearing being seen as unfit to practice medicine or experiencing mistreatment. 12 Notably, 16% of the participants reported mistreatment by professors, 4% by peers, and 1.9% reported sexual harassment by both professors and peers. These findings highlight the need for universities to address harassment and mistreatment by implementing clear policies and procedures for thorough, confidential investigations. 68
The strengths of this study include a diverse sample of medical students from the Republic of Paraguay. The mixed-methods approach integrates quantitative and qualitative techniques, providing a comprehensive understanding of mental health, treatment needs, and the barriers and facilitators to seeking care among medical students in the country and the broader Latin American region. The limitations include the cross-sectional design, which restricts causal inference; the overrepresentation of women, which affects generalizability; potential self-selection bias due to voluntary participation; and possible response bias related to the disclosure of substance and alcohol use. Additionally, information about mental health services at the University was based solely on participants’ accounts, which may not accurately reflect all the services available. This limitation emphasizes the potential need to increase awareness of existing mental health resources among medical students. Moreover, the scales used in this study were primarily screening tools, and the actual prevalence of the diagnoses may vary. Future research should address these limitations by incorporating longer follow-up periods as medical students progress through their education.
Conclusion
Our study revealed high levels of anxiety, depression, and unmet mental health needs among medical students enrolled in Paraguayan universities. Key stressors included academic pressure, financial issues, and family responsibilities, whereas stigma, attitudinal barriers, and practical challenges impeded access to care. Despite the availability of services, many students felt unsupported by their universities because of distrust and dissatisfaction. This highlights the urgent need for universities to improve their mental health services by addressing barriers to health care. Future research should explore long-term strategies to foster a supportive academic environment among medical students.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
This study was conducted within the framework of the Program of Initiation to Scientific Research of the Network of Student Researchers in Neurosciences and was approved by the concerned ethics committee of the School of Medical Sciences at the National University of Asuncion, Paraguay (Reference 011-007-2024). The data were treated with confidentiality, equality, and justice, in accordance with the Helsinki principles.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant information sheet was provided, and written informed consent was obtained prior to the administration of the survey. Participants who requested feedback from the survey were invited to write their e-mail addresses to receive useful information or suggestions.
Red de Estudiantes Investigadores en Neurociencias
Matías Franco Di Giuseppe, Basilio Ruiz-Galeano, Elías René Rolón-Méndez, Patricia Lorena Martínez-López, Katja Victoria Heinichen-Mansfeld, Sebastián Barboza-Basualdo.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.