
Abstract
This article examines the use of homeopathy from the perspective of Bourdieu’s theory of social space and practice. Theoretically, we elaborate that the use of alternative medicine is subject to practical logics that cannot be reduced to and are incompatible with a scholastic rationalist logic. However, belief in scientific logic and evidence, like belief in alternative rationalities, is situated in the social space of society itself, which can be involved in societal and political conflicts. To reveal the multiplicity of logic behind the use and non-use of homeopathy we combine multiple correspondence analysis and logistic regression models to analyze the position of the (non-)use of homeopathy in the social space and its relation to additional societal, political, and health-related factors. With survey data from the European Social Survey (ESS round 7, 2014) for Germany, Austria, and Switzerland, we show how the (non-)use of homeopathy and the different rationalities and societal antagonisms involved are structured by this transnational space but that certain sociodemographic factors produce effects beyond this social space.
Introduction
The coronavirus pandemic has dramatically increased awareness of the stances taken by different societal groups on crucial issues such as vaccination and medicinal therapies. The fact that specific milieus differ regarding their relations to official medicine is not new. The very history of the emergence of a professional modern field of medicine has taken place as a process of distancing from folk medicine or ‘quackery’ (Pinell, 2009). Yet this distinction is not as straightforward as it may seem: today, there are myriad competing products in the medicinal field, many of which claim to offer both scientific and alternative foundations. A prominent example of such alternative medicine is homeopathy, the belief in and use of products that follow Samuel Hahnemann’s ideas from 1796, involving a procedure of extreme dilution up to the point of non-identifiability. This form of alternative medicine, which was developed in pre-Empire Germany, has been gaining in importance worldwide, as has alternative medicine in general, particularly in Europe (Coulter and Willis, 2007; Fries, 2009; Meier-Girard et al., 2022). Such practices are especially common in German-speaking countries (Germany, Austria, and Switzerland) where approximately 40%–60% of people report that they have used some form of complementary medicine (see Kemppainen et al., 2018; Milenkovic et al., 2020; Weidmann, 2023).
Homeopathy has long been understood as a soft approach with little negative side effects and is even integrated in Germany’s and Switzerland’s official medicinal system 1 ; however, in recent years, concerns have arisen. In particular, research conducted in the wake of the pandemic has shown that alternative milieus that disproportionately condone homeopathy, and similar approaches often show a critical if not rejectionist stance toward vaccination (Casigliani et al., 2022; Jäckle and Timmis, 2024). Therefore, the question arises as to why in highly developed countries with a generally well-educated population and well-equipped health systems, a part of the population develops attitudes and behaviors that seem to be guided by ‘irrational’ beliefs.
In this study, we attempt to resolve this enigma by employing a practice–theoretical perspective to address different conditions and practical rationalities behind the use of homeopathy (UH). The advantage of this relational approach is that we analyze both objective sociodemographic characteristics and subjective cultural phenomena (Fries, 2009; Siahpush, 1998). It is exactly this theoretical combination that has increasingly fostered the use of Bourdieusian theory and methodology in recent health research (Cockerham, 2013; Collyer, 2018; Gatrell et al., 2004; Harsløf et al., 2023; Huppatz, 2015; Lo and Stacey, 2008; Mollborn et al., 2020; Veenstra, 2007; Veenstra and Abel, 2019; Williams, 1995). We add to this blossoming stream of research by systematically investigating the UH and by contextualizing such practices in terms of cultural, political, and scientific aspects. Moreover, in German-speaking discourse, UH is perceived not only as a socially and culturally structured issue but also as a political one (Coulter and Willis, 2007; Degele, 2000; Fries, 2009; Harsløf et al., 2023), we locate UH in a ‘politicized social structure’ (see Pappi, 2002), that is, a sociopolitical space (Schmitz and Horneber, 2022).
Using data from the European Social Survey 7 (2014) for Germany, Austria, and Switzerland (N = 5,321), we employ geometric data analysis to locate the UH in a transnational German-speaking sociopolitical space. We thereby shed light on the economic, cultural, and political contexts of a seemingly personal choice. In doing so, we reveal and explain not only the average socio-spatial positions of the use and non-use of this complementary medicine but also the different logics of practice that prevail in the German-speaking sociopolitical space. Taking into account this spatial contextuality and variation in homeopathy use, we then draw on other factors identified in the literature on health, such as health practices and health-related lifestyles, trust in the health care system, religiosity, and sociodemographic factors, to examine by means of logistic regression analysis the extent to which these factors yield additional effects, that is, effects beyond the position in the social space, on the UH. Overall, we offer a differentiated picture of structural and individual factors of homeopathy use.
A Bourdieusian approach to health research
In recent years, the use of Bourdieusian concepts has spread in the sociology of health and health research (Cockerham, 2013; Collyer, 2018; Gatrell et al., 2004; Harsløf et al., 2023; Huppatz, 2015; Lo and Stacey, 2008; Mollborn et al., 2020; Veenstra, 2007; Veenstra and Abel, 2019; Williams, 1995). Research referring to Bourdieusian concepts has established a strong link between social structures and health dispositions and practices (Collyer, 2018). In this view, health is seen as a genuine relational outcome (see Cockerham, 2013; Robison et al., 2020); that is, as largely affected and structured by the actors’ manifest (e.g. relationships, networks) and latent (e.g. resources, societal positions) relations. While this refers to the social relations that provide information and reference standards for medical practices, Bourdieu’s conception of relationality goes further: health-related practices are relational as they are set in relation to one’s own social position in society. This is implied in the concept of social space in which positions, dispositions, and the positioning of actors are relationally associated with each other. The advantage of this relational–spatial view is that explanatory factors that lie outside the acting subject can be systematically derived. As such, the relational view offers a way to transcend rationalist, methodological, individualist approaches to health practices. Different scholars (Cockerham, 2013; Huppatz, 2015) attribute the specific appeal of this approach to the general lack of theory in medical sociology and, more specifically, to its potential to investigate health as a function of relational social structures rather than in terms of methodological individualism. As we shall contend, this relational perspective is particularly well suited to health practices as it allows us to relate facets that have been largely unconnected in the literature so far.
Forms of capital and UH
Studies show that complementary medicine is associated with higher income (Faisal-Cury and Rodrigues, 2022; Kemppainen et al., 2018) and (occupational) class. For example, white-collar jobs (Avina and Schneiderman, 1978) and higher socioeconomic status (Faisal-Cury and Rodrigues, 2022; Lobera and Rogero-García, 2021) are linked with a higher probability of using homeopathy. This is in line with Bourdieu’s finding that spending and investments in health differ by class (Bourdieu, 1984 [1979]: 180, 190). This particularly comprises the investment in children’s health (Mollborn et al., 2020), for which the use of approved medication may be restricted and the UH is widespread (see Ernst, 1999; Madsen et al., 2003; Simpson and Roman, 2001), not least because many parents see it as a natural and risk-free option (Altunç et al., 2007; Ekins-Daukes et al., 2005).
The practices of parts of economically well-off classes and milieus in modern Western societies can be described less by dealing with illness than by an issue of self-optimization and commodification (see Harsløf et al., 2023: 391). Given the financial cost of homeopathic products and their implied promise of health-oriented optimization, it can be assumed that the UH for a considerable number of actors factually requires and is practically embedded in an advantageous economic situation.
Another recurrent finding concerns education. Studies have consistently shown that it is the highly educated rather than the less educated who are more likely to resort to such forms of supposedly irrational and – from an evidence-based medical standpoint – ‘useless’ alternative medicines (Aßmann and Betsch, 2023; Avina and Schneiderman, 1978; Faisal-Cury and Rodrigues, 2022; Kemppainen et al., 2018). In Bourdieusian terms, the assumption can be derived that high economic and cultural capital are associated with the UH.
From a rationalist and individualist perspective, it seems counterintuitive that highly educated and economically well-off individuals engage in a costly medical practice that has no scientific–empirical evidence (see Aßmann and Betsch, 2023; Clavarino and Yates, 1995; Follert and Daumann, 2021). Scientists recurrently stumble over the purported puzzle of highly educated actors choosing a seemingly irrational good (see Clavarino and Yates, 1995; Follert and Daumann, 2021). The Bourdieusian lens sheds light on this puzzle from a different perspective by integrating several empirical findings: cultural capital can be understood as linked to strong interest in medical topics, the gathering and critical examination of health-related information, and overall, striving to question and transcend outdated official knowledge. Cultural capital provides actors with the means to approach such topics in the first place and, as we shall discuss, to develop a critical stance on medicine and health systems.
Trust, skepticism, and practical integration of orthodox medicine
Trust in the official healthcare system is reported to be involved in the decision to use official medicinal products. Accordingly, distrust in official medicine (e.g. due to economization processes and the profit-oriented interest of pharmaceutical companies) is involved in the issue of the UH (see Degele, 2000: 54). Conversely, obtaining information from trusted sources such as family and friends plays a major role in alternative medicine (Öztürk et al., 2022). A similar pattern can be identified in the rejection of certain health practices, such as vaccination. Benin et al. (2006) showed that a trusting relationship with persons who are skeptical about vaccinations can explain vaccination rejection. A core aspect of this lies in the users’ comparisons with official medicine, namely the experience of consultations and therapies. Ciocănel et al. (2021) found ‘that proponents and users of homeopathy appeal to temporal properties of treatment, such as the longer duration of consultation, and of healing’ (p. 101). Some research indicates that receiving homeopathic treatment is seen as a more positive overall experience in comparison with medical consultations at mainstream institutions, especially regarding ‘concerns about communication with doctors’ (Vincent and Furnham, 1996: 37). Vice versa, in the context of vaccination decisions, it has been shown that ‘inhibitors of accepting vaccination’ included ‘feeling alienated by or unable to trust the pediatrician’ and ‘having a trusting relationship with an influential homeopath/naturopath’ (Benin et al., 2006: 1532). This trust is partially felt in reaction to the considerable increase in time spent during homeopathic consultation (see Ciocănel et al., 2021: 100). This is relevant because the effects of homeopathy are scientifically considered to be placebo effects (Shang et al., 2005), but in fact, placebo effects may include very complex, non-specific, and social contextual effects, especially as part of the social interaction during consultation (see Ernst, 2010; Ernst and Resch, 1995; Haresnape, 2013). Di Blasi et al. (2001) found that positive consultations can have beneficial effects for patients.
There is also a more fundamental critique of complementary and alternative medicine, such as homeopathy, namely their link to further-reaching societal issues. Studies have shown that users of homeopathic medicine are more skeptical about the efficacy of orthodox medicine (Furnham and Smith, 1988; Vincent and Furnham, 1996), which might be caused by public discussions on economization and the role of the pharmaceutical industry in medical systems (see Degele, 2000). This is partially an effect of disenchantment with traditional medicine and negative experiences, such as ‘failed biomedical treatments’ (Ciocănel et al., 2021: 101), the ineffectiveness of orthodox treatments, or even negative side effects from medication (Avina and Schneiderman, 1978; Vincent and Furnham, 1996). Furnham and Smith (1988) argued that it is not the mere belief that ‘traditional medicine is itself ineffective’ but the ‘disenchantment with, and bad experiences of, traditional medical practitioners’ that make people choose alternative medicine (p. 685).
The critical stance towards mainstream medicine seems to be partly embedded in an overarching general skepticism toward expert culture in Western societies, which manifests in a ‘cultural scepticism toward expert systems’ that ‘attends rejection of scientific medicine and the scientific systems of belief on which biomedicine is based that are characteristic of the “postmodern condition”’ (Fries, 2009: 335). Postmodernism has been related to the scant and declining trust in traditional authorities, which is part of the explanation of the use of complementary medicine (Coulter and Willis, 2007: 218–219). Thus, UH is embedded in overarching sociopolitical stances (Weidmann, 2023) that are often characterized by a detached attitude vis-à-vis the official institutional setting. Fries (2009) located the question of the UH in the context of ‘cultural antagonisms’ (p. 335). This medical stance, which is also a political one, not only opposes legitimate institutional structures but has additionally been harshly opposed in German-speaking political discourse by critics of homeopathy and the associated ideological dispositions. Notably, the defunding discourse that has been consequential in parts of Europe has caught on in German-speaking countries (Ashworth and Cloatre, 2024), spurring fierce debates about the legitimacy of UH.
Nonetheless, the reasons for using homeopathy are partially based on its scientific and medical appearance. The UH is not the result of a mere distrust in science but at least partially because its users see homeopathy as a social practice and a good that is highly laden with scientific connotation. Lobera and Rogero-García (2021) showed ‘that trust in the effectiveness of CAM therapies is not mutually exclusive with a belief in science for the general public’ and argued that the ‘scientific appearance of these alternative therapies, in terms of prescription, communication and marketing, may play an important role in determining trust in them for a large part of the population’ (p. 1278). Users of complementary medicine even state that treatment should concentrate ‘greater knowledge of the physiology of the body’ (Furnham and Forey, 1994: 458). Accordingly, empirical studies have shown that alternative medicine is often complementary to medical treatment rather than a substitute for it (see Astin, 1998; Bombardieri and Easthope, 2000; Fries and Menzies, 2000). In such milieus, 2 medical treatment is not, in general, rejected; instead, it is claimed that homeopathy has an alternative, superior approach to health issues, an approach that is scientific but without the negative consequences of official medication. Often, alternative drugs are labeled ‘complementary’, which further illustrates the fact that homeopathy and official medicine are practically interlinked rather than meticulously separated. Patients (Robert-Demontrond, 2023), doctors (Lobera and Rogero-García, 2021), and pharmacies combine and switch between homeopathy and mainstream medicine. Thus, ideologically, UH can be understood, on the one hand, as a confluence of modernism and enlightenment and, on the other hand, with traditionalism and anti-enlightenment.
Homeopathic practices, lifestyles, and milieus
Health research has increasingly engaged with the Bourdieusian perspective to address the relationship between class, health, and lifestyles (see, e.g. Cockerham, 2013; Gatrell et al., 2004; Huppatz, 2015; Veenstra, 2007; Williams, 1995). Lifestyles constitute patterns of practices that integrate seemingly independent aspects of life such as health, politics, and culture. Thus, lifestyles are a crucial concept in understanding the emergence of different practical logics underlying different health practices and health conditions.
The issue of lifestyles and overarching ways of life and dispositions can be related to the aspect of health conditions. Especially in aging Western industrialized societies, such as Germany, Austria, and Switzerland, which are associated with an ‘increasing prevalence of chronic diseases such as arthritis, rheumatism, and back and neck injuries’ (Fries, 2009: 334; see also Coulter and Willis, 2007: 218–219). Furthermore, Schäfer (2004) showed that allergies, another chronic health issue that is prevalent in rich Western societies, are often treated by complementary medicine. In this context, studies have pointed out that classical biomedicine is insufficiently responsive to the plight and suffering of patients with chronic diseases, and the patients then turn to alternative remedies and approaches (e.g. Bausell et al., 2001; Fries and Menzies, 2000; Millar, 1997). Chronic illness, unrecognized health issues, and other diseases with diffuse symptoms that are difficult to diagnose and treat conventionally are found to foster engagement with complementary and alternative medicine and, in particular, homeopathy (Avina and Schneiderman, 1978; Burke and Herlambang, 2012; Fries, 2009; Jacobs et al., 1998; Kemppainen et al., 2018; Millar, 1997).
Notably, not only the objective but also the subjective dimension plays a crucial role: The perceived health status of both the body and the mind may increase the probability of a patient using homeopathy (Faisal-Cury and Rodrigues, 2022). Patients suffering from a chronic illness subjectively report that they experience good progress under homeopathic care (see Avina and Schneiderman, 1978). Especially if an illness becomes part of everyday life, it can foster UH as a coping practice. Such ‘alternative medicine use’ can be traced back to ‘health care alternatives’ being ‘more congruent’ with specific ‘values, beliefs, and philosophical orientations toward health and life’ (Astin, 1998: 1548) and, overall, be part of overarching lifestyles and milieus.
Looking on empirical research from a Bourdieusian perspective, the focus can be placed on different lifestyles and milieus that might be prone to UH. For some, as Furnham and Forey (1994) showed, complementary medicine users are characterized by particularly ‘self- and ecologically aware lifestyles’ (p. 458). Here, the UH is part of a lifestyle that includes, for example, the ‘regular consumption of fruits and/or vegetables and regular physical activity’ (Meier-Girard et al., 2022: 1) and, vice versa, avoids smoking, being overweight, and obesity.
The rise of alternative medicine can also be understood in the context of the aforementioned postmodern culture and a corresponding postmodern disposition, with its return to alternative spiritualities and ‘civil religions’ in Western, secular societies (Abheiden et al., 2020; Coulter and Willis, 2007). For many users, complementary medicine seems to practically fill the gap created by secularization. Siahpush (1998) showed ‘that the set of postmodern values, in comparison to dissatisfaction with the medical encounter, is by far a better predictor of attitudes towards alternative medicine’ (p. 67). Röding (2022) found that the UH is prevalent in the post-materialist milieu of the new petty bourgeoisie rather than in the materialist milieus of the middle classes. These values comprise antitechnology sentiments, holism, belief in the value of natural substances, and being an active participant with equal rights in the process of becoming healthy. Some actors with ‘holistic’ dispositions favor a return to the ‘natural as holistic, spiritual, and benevolent in contradiction with what is perceived as the scientific and technological oppression and authority of biomedicine’ (Fries, 2009). Therefore, as a morally-laden and experience-oriented practice, homeopathy can also be understood as what Bourdieu (1984 [1979]: 367) called a self-optimizing ‘cult of personal health and psychological therapy’ that is ‘consistent with the more or less secularized forms of the search for religious salvation’.
A variety of studies have consistently shown that women are more likely to consume alternative and complementary medicine across societies and cultures (Faisal-Cury and Rodrigues, 2022; Kemppainen et al., 2018; Lobera and Rogero-García, 2021; Meier-Girard et al., 2022). As could be established by research, spirituality-based decisions for the UH are associated with female dispositions as discussed by Coulter and Willis (2007) in their ‘gendered spirituality thesis’: Women do not only engage in UH more often but embed these practices in an overarching postmodern lifestyle of spiritual wellbeing, alternative ‘green’ disposition, and modern consumerism (p. 219).
We also assume a specific intellectual position that transcends Western rationality with considerable interest in education, science, and medicinal professionalization. Such scientific habitus should possess high cultural capital and formal education. For this humanistic disposition, the societal acceptance of scientific reasoning and form is part of the success of homeopathy. Especially for the cultural milieus of the upper classes, a tendency to simultaneously approve general principles of science while rejecting overly technical, economized, instrumental, and positivistic scientific medicine seems to be a plausible configuration.
In light of the economic background of the UH and the economic dimension of the homeopathic industry in German-speaking countries, UH may as well be understood as an outcome of a consumerist disposition, which is specific to certain milieus that can afford such practices. The choice of homeopathy from a set of possible medicinal choices is in line with the Western culture of autonomous, individual responsibility and consumerism (having the choice between options; see Coulter and Willis, 2007). In Western, affluent, and postmodern societies, health is not simply the absence of disease and pain; under the conditions of an increasingly economized medicine (Degele, 2000), health is increasingly seen as a form of capital in which to invest by means of active self-management practices (Harsløf et al., 2023). From this perspective, health and a person’s body are individual assets that can be optimized and for which the autonomous individual is responsible, for example, for choosing the optimal health product. Complementary and alternative medical products thus further the universe of individual options, especially for the higher classes, and form an amalgamation of ecological and neo-liberal ideologies that is very successful in German-speaking countries. 3
Accordingly, while Bourdieusian expectations align with empirical findings, suggesting that highly educated and affluent women should engage in UH, the theoretical framework offers a more differentiated perspective, capturing a wider range of dispositions, lifestyles, and social milieus.
In addition, Bourdieu's relational thinking will suggest that nonusers of homeopathy should also be taken into account. As previously discussed in the context of high cultural capital, some actors (what the rationalist view would erroneously generalize) can be expected to follow a matter-of-fact instrumental-rational disposition that considers the ideological component of homeopathy unattractive and is instead interested in scientifically proven medications. Based on the discussed findings on cultural and economic capital, we also expect a (male) working-class habitus from corresponding milieus with its own specific stance toward homeopathy. Bourdieu (1984 [1979]) found that the working classes are more attentive to the strength of the (male) body than its shape, and tend to go for products that are both cheap and nutritious, [while] the professions prefer products that are tasty, health-giving, light and not fattening. Taste, a class culture turned into nature, that is, embodied, helps to shape the class body (p. 190).
Bourdieu (1978: 838) also assumed that lower classes have a rather instrumental relation to their bodies. We can extend this insight to the health realm and assume that for those actors, the same applies to medications, namely that they should be effective. Thus, for parts of the male working class, we expect a disposition that rejects medications that are embedded in complex scientific and esoteric semantics and, eventually, will show little to no interest in homeopathy.
Empirical research and its theoretical reflections thus allow us to paint a differentiated expectation regarding the possibly different practical logics behind the use and non-UH (see Gale, 2014). In theoretical terms, the according milieus with their characteristic lifestyles are conceptualized in relation to each other, that is, as a social space structured by forms of capital and occupied by typical positions of groups and practices (Bourdieu, 1984 [1979]), such as the use or non-UH. Based on a spatial reconstruction, the differences between the groups can not only be conceptualized and depicted but can also be made accessible for reflection on the societal and political struggles involved (see Bourdieu, 1984 [1979]; Schmitz and Horneber, 2022; Schneickert, in press) and the role they play in practices of (not) using homeopathy.
Data and methods
Data
We used survey data from the seventh round of the European Social Survey (ESS, 2014) for Germany, Austria, and Switzerland. The samples were drawn using random sampling and can be considered representative of the populations in key characteristics. For the specific purpose of this study, we defined the working sample as the subset of the German-speaking areas. Since we were interested in the German-speaking population, we removed all cases in which the interview language was not German. In order to analyze occupational classes, we used only cases that had an International Standard Classification of Occupations (ISCO) code and could, therefore, be assigned to one of the occupational classes according to Oesch (2006a, 2006b). After excluding n = 220 missing values (4.0%) in the remaining sample because of cumulating missing values on central indicator variables, the final sample consisted of N = 5,321 individuals.
For the analyses that referred to the pooled data set, we weighted the data according to the population sizes in the countries. 4 The German sample had an oversampling of East Germans that had to be corrected. Therefore, we used the product of the population weight and the post-stratification weight.
Variables
Dependent variable
Use of homeopathy:
We measured the UH with a dichotomous variable that was situated in a battery of questions regarding health decisions that asked respondents which of 12 treatments they had used in the last 12 months (binary, use/non-use; see Table 2 for the distribution of the dependent variable by country).
Sociopolitical space (active variables)
For the active construction of a sociopolitical space that allows us to localize the (non-)UH as well as their practical contexts (milieus), we mobilized indicators on ‘occupational fractions’ (see Bourdieu, 1984 [1979]; Brisson and Bianchi, 2017), indicators for cultural and economic capital, and political indicators (see Table 3 for descriptive statistics). 5
Occupational fractions:
We employed the eight-class scheme by Oesch and differentiated between production workers, service workers, clerks, small business owners, sociocultural (semi)professionals, technical (semi)professionals, the self-employed and large employers, and (associate) managers using the provided syntax for ESS data from Oesch (2006a, 2006b).
Economic capital:
For economic capital, we used the equivalized households total net income as an indicator. To construct this variable, we divided the total net income by the square root of the household size and created quartiles, while adding a category for missing values. The final variable had five categories: low income, lower middle income, upper middle income, high income, and no income information.
Cultural capital:
As we combined data from three nations with different educational systems, we used the harmonized International Standard Classification of Education (ISCED) variable to assess cultural capital, collapsing categories into a four-category scheme (ISCED I and II = low education, ISCED IIIb = lower middle education, ISCED IIIa and IV = upper middle education, ISCED V1 and V2 = high education).
Political self-placement
To assess political self-identification, we employed the commonly used left–right scale, collapsed the categories, and added a category for missing information, which resulted in a variable with six categories (very left, left, middle, right, very right, and non-information).
Homosexuality
We measured attitudes toward sexual diversity with a recoded 5-point scale indicating the degree to which respondents agreed with the statement that ‘lesbians and gays are free to live as they wish’. As very few answered ‘strongly disagree’, we collapsed the disagree categories, resulting in a four-category variable (disagree, neither, agree, strongly agree).
Migration
To assess attitudes toward migration, we used a five-category unweighted mean index of three items on attitude toward migration: (1) if migration enriches a country’s culture; (2) enriches a country’s economy; and (3) if the country is overall better or worse off with migration; (alpha = 0.85). The values were rounded to use the variable categorical in comparison to the other indicators and in the multiple correspondence analysis (MCA).
Redistribution
We measured attitudes toward redistribution with a 5-point scale indicating how strongly respondents agreed with the government taking measures to reduce differences in income levels. As very few strongly disagreed, we collapsed categories and ended up with four categories (1 = disagree, 2 = neither agree nor disagree, 3 = agree, 4 = strongly agree).
Sociodemographic indicators
Gender and age
We used a dummy variable for gender (0 = male, 1 = female) and a continuous variable for age (in years).
Religiosity:
Assessed on an 11-point scale from 0 = not at all religious to 10 = very religious, which we divided by 10 to a range of 0–1, reflecting maximum effects (not at all religious vs very religious) for easier interpretation in the regression.
Children at home:
We used a dummy variable that indicates if the respondent lives with children at home (0 = not living with children, 1 = living with children).
Health and lifestyle indicators
Visit of health professionals
We used two binary variables to assess if the respondents discussed their health with a ‘general practitioner’ or a ‘medical specialist (excluding dentists)’ in the last 12 months.
Trust in healthcare system
We used an 11-point scale on which respondents had to assess the quality of the healthcare system in their country (0 = extremely bad, 10 = extremely good). We divided this scale by 10 to a range of 0–1 of maximum effects (extremely bad vs extremely good) for easier interpretation in the regression.
Smoking:
Smoking behavior was measured on a 5-point scale (0 = never smoked to 4 = smoke daily), which we divided by 4 to a range of 0–1 of maximum effects (never vs daily) for easier interpretation in the regression.
Healthy nutrition
As another indicator of a healthy lifestyle, we used an indicator measuring how often respondents eat vegetables or salad (excluding potatoes but including frozen vegetables) on a scale from 0 = never to 6 = more than three times a day. We again rescaled by dividing by 6 to a range of 0–1 of maximum effects (never vs 3 + a day) for ease of interpretation.
Chronic health issues
As a proxy for chronic health issues, we used an indicator variable (binary) that indicated if respondents had experienced allergies in the last 12 months.
Analytical strategy
Our theoretical engagement with the literature yielded the information that the use and non-UH can be approached in two ways. On the one hand, we assumed competing and partially simultaneous logics behind UH that characterize different positions in a common sociopolitical space; on the other hand, other causes for UH were discussed that seem to affect individuals in the same way, independent from their milieu background and socio-spatial position. To integrate both perspectives, we employed a Bourdieusian understanding of method combination. 6 First, we explored the phenomenon of UH by means of MCA in its spatial position and dispersion (Benzécri, 1976; Blasius et al., 2020; Lebaron, 2009).
In Distinction, Bourdieu (1984 [1979]: 451–453) assumed strong homology of political and social space (for France at a certain point in time). Recent studies have been attesting strong homology of social and political spaces for modern European societies (Atkinson, 2024; Flemmen and Haakestad, 2018; Harrits et al., 2010; Jarness et al., 2019; Lindell and Ibrahim, 2021). In this study, we do not want to ask about this correspondence, but rather, assuming a clear homology between the two spaces, we will analyze how UH relates to a sociopolitical space. This perspective is particularly relevant given that, in recent years, political differences in the German-speaking world have been compounded by social differences (Gethin et al., 2021; Schmitz and Horneber, 2022). The relative positions and dispersions of the use and non-use homeopathy are modeled as a passive indicator. Subsequently, the residual factors that may operate independently or in addition to the space were investigated using logistic regression (Schmitz, 2024), thus adding to the explanation and understanding of the phenomenon beyond the explanation yielded by geometric data analysis. The previously extracted latent dimensions of MCA were then used as scales and included as predictors in the logit model.
Findings
Figure 1 shows the results of the MCA. Overall, the result is a two-dimensional solution of good quality, with the first two dimensions combining 71% of the total variance (see Tables 4 and 5 in Appendix 1 for detailed model statistics).
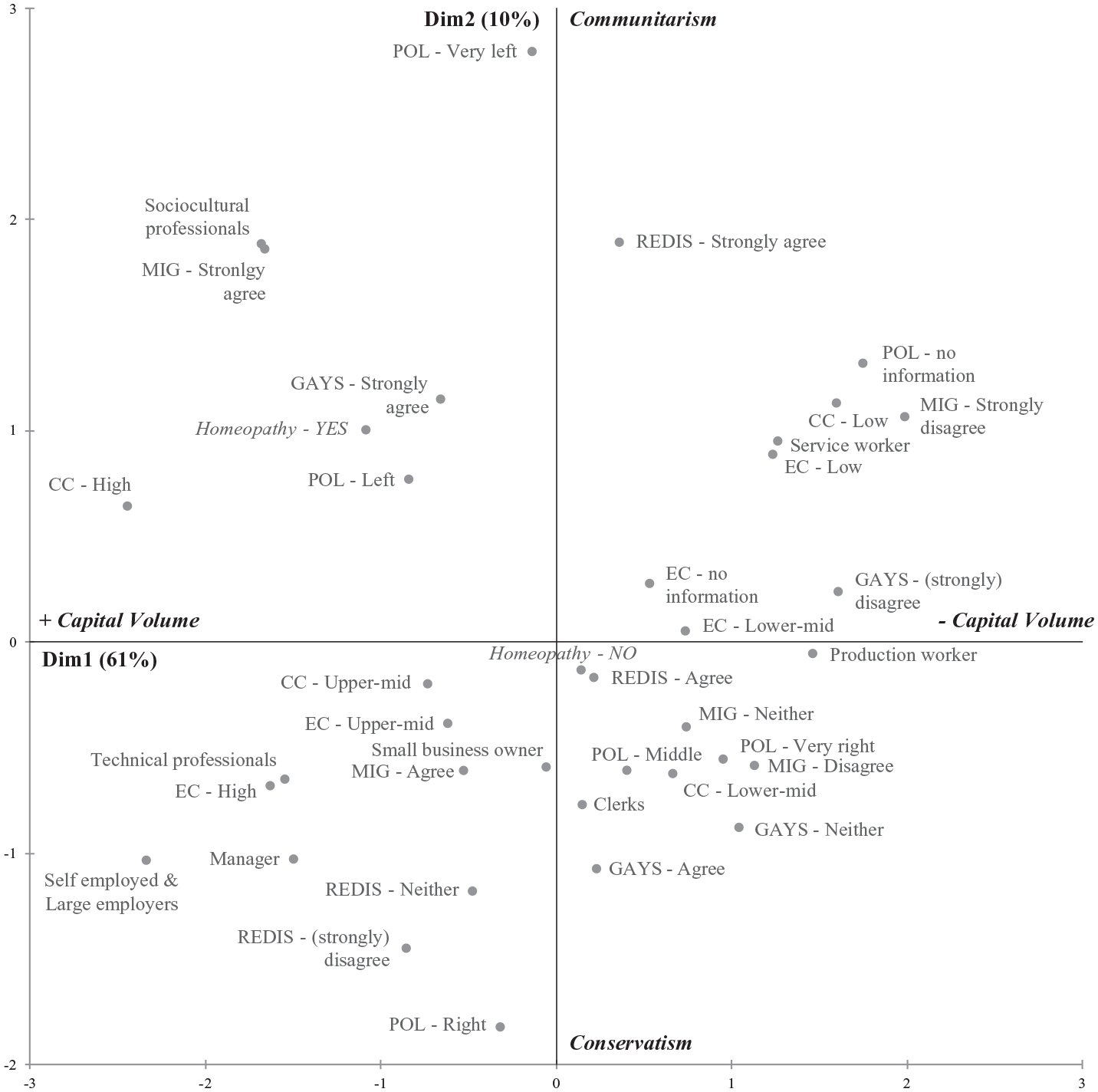
Homeopathy-use in the German-speaking sociopolitical space (MCA).
The first dimension covers 61% of variance and is determined above all by cultural capital, occupations, economic capital, and to some extent, attitudes toward migration – we label this dimension capital volume. From left to right in the space, the volume of capital tends to decrease, with the least economic and cultural capital in the upper right quadrant. In the left part of the space (the ‘upper class’), cultural capital in the upper quadrant differentiates from economic capital in the lower quadrant, with corresponding opposites in the occupations, such as sociocultural professionals (top left) and technical professionals, managers, and the self-employed and large employers (bottom left).
The second dimension ties up another 10% of the total variance and roughly represents a political contrast between communitarism (top of the space) and conservatism (bottom of the space), which in the German-speaking space summarizes the contrast between the socioeconomical and sociocultural political left and right. However, the individual modalities – as already mentioned in the case of attitudes toward migration – to some degree load on both dimensions so that diagonal antagonisms in the interplay of class structuring and ideological positioning emerge. In the upper left section, for example, we find position-taking as characteristic of the cultural left, and in the upper right section, the economic left. In the lower left quadrant (economic pole of the upper class), the economically right-wing positions (against redistribution) are considered, while culturally right-wing positions are further to the right of the space. 7
Overall, the two-dimensional space represents the transnational sociopolitical space of German-speaking countries. This space, however, does not represent two independent dimensions for socio-structural versus political aspects but rather tightly interconnected socio-structural and political logics (see Bourdieu, 1984 [1979]): For example, we see that low capital volume is associated with the absence of political stances and anti-gay and anti-migration positions. In addition, culturally left positions are at the top left, whereas the stance against redistribution that describes the top right suggests the presence of economic libertarianism. Thus, the classical left–right dimension does not run linearly through the space but has to be differentiated into cultural left, economic left, libertarian, and conservative.
Within this space, we project the UH as a passive (illustrative) variable – this approach within geometric data analysis allows us to examine the position of additional variables that were not involved in the construction of the space itself. The typical position of UH is located at the top left of this space. This position is associated with higher capital volume and particular closeness to sociocultural professions. Regarding the ideological aspect, UH is close to a pro-homosexual and pro-migration stance and, thus, typically embedded within a left-liberal stance. Remarkably, and in contrast to the depiction of homeopathic use as an ‘irrational’ practice of rather uneducated strata – perhaps even close to questionable political positions in the realm of anti-scientific beliefs and conspiracy theories – UH is instead embedded in high cultural capital.
These patterns support our assumption that the effect of homeopathy is partially based on the embedding of this practice in privileged socio-spatial positions and healthy lifestyles. Yet, we also see that the position of homeopathy use is not at the extreme top left but somewhat closer to the middle of the space. This suggests that there is considerable variation in this practice, spreading over large parts of the space and comprising different social classes and political dispositions.
Figure 2 shows the space of individuals with UH marked in black diamonds and non-UH in gray hollow circles; both categories are further described by concentration ellipses. The space of individuals reveals a striking dispersion of both UH and non-UH, and the overlap of both ellipses illustrate that there is considerable variation and, thus, need for further explanation of both practices. 8 Not least, the location of the modality of UH in the upper left quadrant needs to be understood in relation to the center of non-usage of homeopathy at the lower right. The association with above-average cultural and economic capital, and especially with sociocultural professions and left-liberal position-taking, is, at least partly, a function of the non-UH position (low cultural and economic capital, workers, right wing). Both insights indicate that the social profile of homeopathic users and practitioners cannot be limited to a single social figure, social class, and practical logic. In particular, the empirical evidence suggests that UH is far from constituting a phenomenon that is exclusive to the well-educated upper classes and left-leaning milieus of the space. Rather, homeopathy is also associated with different capital endowments and class positions in the sociopolitical space and thus arguably embedded in many other practical contexts. Likewise, neither can the non-UH be reduced to a single social class but spreads over and intersects large parts of the space as well, comprising, for example, parts of the economic and even cultural upper classes.
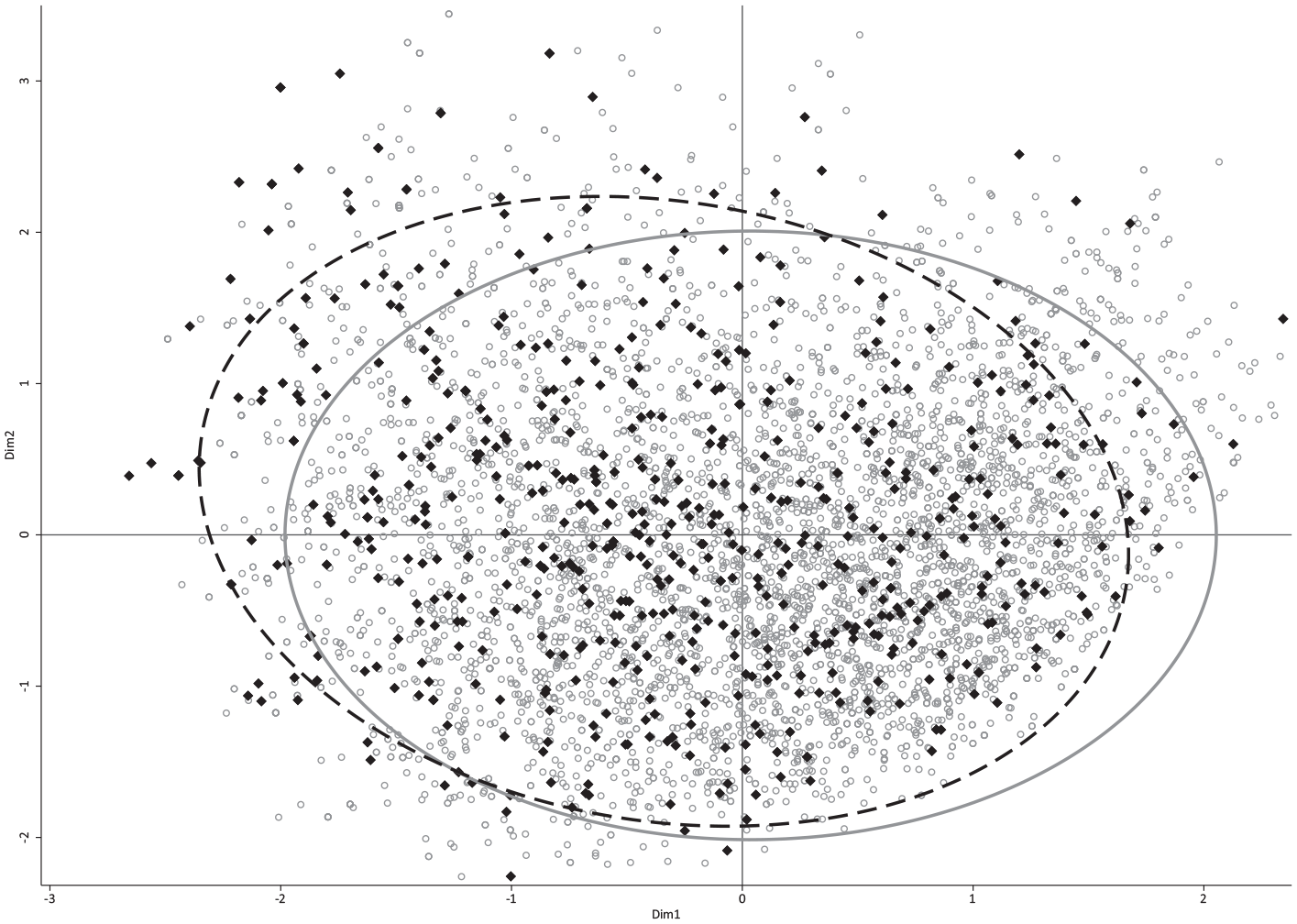
Cloud of individuals with concentration ellipses.
We thus employ logistic regression analysis (Table 1) to model UH by means of indicators, derived from the theoretical reflections outlined in chapter 2, that may add to the effects of the sociopolitical space.
Logistic regression of use of homeopathy on central indicators.

SE: standard error; CI: confidence interval; MCA: multiple correspondence analysis.
Exponentiated coefficients; robust standard errors in parentheses. Weighted. Country controls: Germany [ref.], Austria, Switzerland. The MCA-dimensions were inverted for ease of interpretation, so that high values indicate high capital volume in f1 and conservatism in f2.
p < 0.05, **p < 0.01, ***p < 0.001.
The regression analysis shows the effect of the two latent dimensions extracted from the MCA. Increasing values on the first dimension (decreasing capital volume) are associated with a reduced UH. Higher values on the second dimension (more communitarian attitudes instead of conservative ones) are correlated with a slightly higher UH. As derived from the literature, sociodemographic play an important role, and this is independent of the dimensions of the sociopolitical space.
Women use homeopathy more frequently than men, younger people more frequently than older people (the average age in the sample is just under 50 years), and living with children does not statistically increase UH in a significant way beyond these factors.
The presence of allergies served as a proxy for chronic diseases that – for some – can only be treated to a limited extent with conventional medicine. This positive relation also shows that there are certain medical situations that make the UH more likely.
Smoking as an indicator of an unhealthy lifestyle and unhealthy practices is associated with lower UH. Conversely, a healthy diet is positively associated with UH: Individuals who eat vegetables several times a day have a highly increased odds ratio of having used homeopathy compared to individuals who never eat vegetables (maximum effect as detailed earlier).
With respect to health practices and associated lifestyles, both the visit to a generalized practitioner (everyday ailment) and the visit to a specialist (such as doctors who treat back pain or allergies) are positively associated with UH. Therefore, the UH is a hybrid practice that empirically overlaps with consultations in orthodox medicine. In fact, the assumption that homeopathy and mainstream medicine are mutually exclusive practices cannot be generalized. The UH, much like other more established forms of medical self-care, reflects an active commitment to managing one’s own health.
Second, the regression analysis shows that the UH is influenced throughout the social space by a low level of trust in the state of the health system. This considerable effect is independent of sociodemographic factors or health-related lifestyle factors. This finding attests that trust in the healthcare system does not vary solely due to the lifestyles and sociodemographic profiles of compartmentalized milieus in the social space but exerts independent effects – measures to prevent the population from losing trust in the healthcare system, for example, decommodification, are therefore of great importance for public health.
Finally, religious respondents use homeopathy more often, suggesting a latent communality between religious belief and belief in homeopathy, which can be interpreted not only as heterodox rationality but also in the context of ‘quasi-religious’ orientations and functions (see Čavojová and Ersoy, 2019; Lindeman, 2011; Van den Bulck and Custers, 2009).
Conclusion
The use of homeopathy poses a considerable challenge for the scientific field in several aspects. As a widely practiced method, it appears to fundamentally conflict with the principles of modern science. By adopting homeopathy, individuals and groups are engaging with alternative forms of rationality and knowledge that often diverge from conventional scientific understanding. This divergence involves not only rejecting mainstream medical knowledge but also developing and institutionalizing a distinct system of beliefs. Consequently, homeopathy can be seen as a challenge to established medical expertise. Insofar, the investigation of homeopathy and its criticisms within the contexts of everyday life and sociopolitical stances can provide valuable insights into the contentious dynamics of contemporary Western societies.
The German-speaking region is especially noteworthy in this regard given the long-standing historical roots and institutionalization of both homeopathy and medicine oriented to established scientific principles, a tension that is particularly prominent in our times. Over a long time, within this region, the integration of homeopathy with official health systems as ‘complementary medicine’ has been causing tensions between established medical practices and alternative approaches, blurring the division between ‘scientific’ and ‘non-scientific’ health practices. This ambiguous demarcation lies at the heart of the success of homeopathy in the German-speaking world and the incessant controversies surrounding it. While research has primarily focused on individual use, often seeking to highlight its supposed ‘irrationality’, our approach adopts a relational perspective on the sociopolitical space, reconstructing how (non-) UH is embedded within different practical rationalities and milieus and how these, in turn, relate to and eventually influence each other.
Our findings attest that UH reflects deeper socioeconomic and cultural dynamics, thereby corroborating, contextualizing, and extending prior research on the causes of UH. Our results show that UH is a practice often employed to address everyday health challenges that, in the eyes of those affected, cannot be adequately treated by conventional medical interventions, which are typically perceived as disruptive to daily life; in contrast, UH is perceived as more seamlessly integrated into it. However, not all societal positions and lifestyles are equally inclined to UH.
On the one hand, UH is in considerable part associated with a specific position in the sociopolitical space characterized by high capital volume (especially cultural capital), sociocultural occupational class fractions, and a rather communitarian political attitude. Thus, a privileged social position and a moderate left to mainstream political disposition are particularly conducive to UH. The healthy lifestyle of this milieu, which is above-average populated by female actors, is characterized by self-reflexive practices regarding a healthy diet and other health decisions in which UH is an organically integrated part, not only serving as a medical alternative but also as a marker of social identity.
On the other hand, first, the practice of UH considerably disperses over the social space so that the social profile of homeopathic users and practitioners cannot be limited to a single social figure. Our findings indicate that not only are well-educated, upper-class, left-liberal (communitarian) female individuals prevalent among homeopathic users but also that homeopathy is used by an array of other groups in the social space, 9 spreading over the space and including actors with low capital volume as well as from conservative milieus.
Second, non-UH can also be understood as a practice that is particularly likely in certain regions of the sociopolitical space, namely those of less capital, particularly less cultural capital, and with conservative or traditional attitudes, such as those associated with a (male) working-class habitus and respective occupational fractions (Bourdieu, 1978: 838; 1984 [1979]: 190) and milieus (such as traditional working-class milieus for whom UH may appear unattractive due to its effects not being immediately apparent or precarious milieus who lack the cultural and economic basis for the homeopathy option and who presumably follow a taste of medical necessity).
Yet, non-UH, as well, does considerably spread over the space, comprising parts of the high economic and cultural capital strata. As for UH, qualitative further research should investigate our finding that non-UH is not exclusively linked to milieus with low cultural capital and may comprise, for example, academic milieus, whose high cultural capital is expressed in evidence orientation aligned with institutionalized science or conservative upper-class milieus, which seek to have their health treated by conventional medicine (including technology- and cost-intensive treatments in private clinics).
While homeopathy is – from the perspective of evidence-based medicine – not directly involved in the actual maintenance or improvement of health beyond a placebo effect, it is often integrated into broader, healthier lifestyle practices. Practitioners and proponents in this specific position are at risk of erroneously concluding that homeopathy itself is a key factor in promoting health. The underlying reason for this misinterpretation lies in the practical context in which homeopathy is used; that is, it is embedded within a lifestyle that emphasizes holistic health, including an above-average healthy diet, exercise, and wellness practices of economically and culturally privileged milieus. As a result, the perceived benefits of homeopathic treatments might be conflated with the overall positive effects of these comprehensive lifestyle changes and socioeconomic positions in social space. This association can obscure the distinction between possible direct (medical) impacts of homeopathy and the social benefits, not only of healthier lifestyle decisions but also those resulting from UH as a distinctive social practice vis-à-vis different social milieu.
The rationality of a practice like homeopathy is reflected in its adaptation to the specific context 10 in which it is applied, thereby demonstrating a form of practical rationality. This practical rationality, which is, for example, associated with proto-scientific practices such as doing ‘research’ online, does not involve scientific rationality as aligned with contemporary, legitimate, institutionalized scientific consensus. Nevertheless, the spatial position of the majority of UH and the according practical rationality are associated with high cultural capital.
However, rationality in a specific, legitimate sense also has its specific position in the sociopolitical space. Yet, this position and implied scientific belief are actually rather close to the ‘anti-scientific’ one of UH adherents. This spatial proximity may partly explain the pronounced polarization between supporters and opponents of UH in German-speaking countries, and the reason the discourse surrounding UH has escalated into a subject of extensive and contentious debate.
In the relational view employed here, even the seemingly personal decision for or against a medical product is intimately connected with manifest as well as latent ethical, sociocultural, and sociopolitical antagonisms – symbolic struggles. It should be noted that UH is in the top left of the space, not least because non-use has its center of gravity in its bottom right near the origin of the space. Non-use and even rejection of homeopathy are more typical of actors with lower cultural and economic capital, so that the societal image of homeopathy users contrasts with that of actors with lower cultural and economic capital. This finding allows for a range of interpretations to be considered, indicating that the distinction between the use and non-UH is capable of symbolizing societal differences and might be involved in contributing to their perpetuation.
Bourdieu’s spatial perspective draws our attention to the social, political, and symbolic struggles that underlie and are involved in the seemingly personal decision to use homeopathy (Röding, 2022). This is particularly evident in the apparent inability of milieus that see themselves on the side of science, reason, and truth to comprehend those who, from the perspective of the former, are purely irrational opponents of scientific evidence and, therefore, open to alternative medicine. Harsløf et al. (2023) argued that the increasing importance of individual health investments can be seen as a trigger and amplifier for symbolic boundary-drawing and social closure. This is the case when the health investments of some mean the exclusion and alienation of others and thus create a polarization in health behavior. If we employ this view on the issue of homeopathy use and non-use, we can ask for the distinctive and boundary-drawing effects of homeopathy use within sociopolitical spaces.
Cleavages between medicinal fractions are embedded in cultural, political, and social antagonisms of different milieus and between classes and class fractions in society. UH is particularly well suited to reinforce and confirm these groupings and distinctive demarcations since it refers to and questions the basic attitudes, values, and rationalities in different social milieus. From this perspective, the conflict between conventional medicine and alternative medicine is not just a conflict between different epistemological assumptions or general support or rejection of ‘the’ science but is embedded in sociocultural and sociopolitical struggles. In a similar way and for similar reasons, Fries (2009) dealt with the question of the UH in the context of ‘cultural antagonisms’.
The issue of UH can be understood as both a reflection and a catalyst of societal struggles; the question of what is true medicine and what is quackery is increasingly being played out in the sociopolitical space. Conversely, the medical field seems to be in a state of not only judging the status of legitimate vs illegitimate medicine but also the associated political and cultural class division (Delhey et al., 2017) of the social world. The contentious discourse around homeopathy mirrors the ongoing cultural and social conflicts by aligning with broader debates about health, wellness, medical authority, and overarching sociopolitical tensions. Conversely, these social struggles can be involved in the establishment of health cultures and lifestyles to which the practice of homeopathy can belong, albeit as a reflexive quasi-political statement or rather implicit dispositions that negatively react to mainstream expert discourses.
Footnotes
Appendix 1
Correlations of MCA dimensions and indicators.

| Dim1 (Capital volume) | Dim2 (Conservatism) | |
|---|---|---|
| Female | −0.05*** | −0.15*** |
| Age | −0.03* | 0.09*** |
| Children | 0.01 | 0.03* |
| Religiosity | −0.05** | 0.11*** |
| Doctor visit | −0.06*** | −0.02 |
| Specialist visit | 0.09*** | −0.02 |
| Trust in healthcare | 0.04** | 0.08*** |
| Smoking | −0.11*** | −0.09*** |
| Eating vegetables | 0.16*** | −0.03* |
| Allergies | 0.10*** | −0.06*** |
MCA: multiple correspondence analysis. Dimensions are reversed as in Table 1, so that high values indicate high capital volume in dim1 and conservatism in dim2.
p < 0.05, **p < 0.01, ***p < 0.001.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
ESS Round 7: European Social Survey Round 7 Data (2014). Data file edition 2.2. Sikt – Norwegian
Agency for Shared Services in Education and Research, Norway – Data Archive and distributor of ESS data for ESS ERIC. DOI: 10.21338/NSD-ESS7-2014.
ESS Round 7: European Social Survey (2018): ESS-7 2014 Documentation Report. Edition 3.2. Bergen, European Social Survey Data Archive, Sikt – Norwegian Agency for Shared Servicesin Education and Research, Norway for ESS ERIC. DOI: 10.21338/NSD-ESS7-2014.