
Abstract
Background
Telemedicine is one of the major trends in the evolution of modern medicine. Telemedicine encompasses a wide range of services with different characteristics. Healthcare organisations know limited information on developing and utilising different types of telemedicine service programmes as well as factors and spatial and temporal characteristics that influence their development.
Objective
To analyse the factors influencing the development of telemedicine, and to explore the priority order of different telemedicine services carried out by healthcare institutions, as well as the spatiotemporal evolution characteristics.
Methods
This study selected Zunyi City, a national pilot city for telemedicine in China, and employed multinomial logistic regression to analyse factors influencing the provision of different types of telemedicine service programmes by healthcare institutions and evaluate the spatial and temporal evolutionary characteristics of spatially visualised telemedicine service programmes.
Results
When the price of services increased, providers were more inclined to conduct teleconsultation (OR: 1.023) and telepathology (OR: 1.058) than tele-imaging, and the willingness to conduct telecardiology (OR: 0.775) and telemetry (OR: 0.997) was relatively low. Patients’ out-of-pocket payments increased, and providers’ willingness to conduct teleconsultations (OR: 49.401) and telepathology (OR: 5.039) increased. Healthcare organisations at higher level were more willing to carry out teleconsultation (OR: 14.052), telepathology (OR: 8.071) and telemetry (OR: 13.113). Compared with private hospitals, public hospitals were 17.760, 12.248 and 87.860 times more likely to conduct teleconsultations, telecardiology and telepathology than tele-imaging. The effectiveness of telemedicine development may be related to the level of local economic development.
Conclusion
Medical institutions carry out telemedicine service programmes with a certain order of priority. Their decisions are often influenced by various factors such as price, out-of-pocket payment ratio and level and attribute of the healthcare organisation. The development of telemedicine may follow an inverted ‘U’ pattern with the level of regional economic development.
Keywords
Background
Telemedicine, as one of the important directions in the development of modern medicine,1–3 was first proposed by the American scholar Polishuk in 1976. 4 The World Health Organisation defined telemedicine at the Telemedicine and Global Health Development Conference in 1997 as medical care services over long distances and large spatial ranges based on information and communication technology. Telemedicine breaks through geographical barriers that traditional medical services are subject to in terms of space5,6 to effectively share medical resources and information transmission between regions and hospitals. It also reduces the patient's consultation time.7,8 Moreover, it optimises the allocation of medical resources and improves the efficiency of medical resource utilisation. 9
In China, the problems of imperfect infrastructure construction and serious imbalance in the distribution of medical resources among regions are highlighted. To address this obstacle, in 2014, China issued its first national-level guiding document for the establishment of telemedicine construction. Various pilot areas actively engaged in the practice and exploration of telemedicine services, designing a variety of services with different characteristics, including teleconsultation, tele-imaging, telecardiology, telepathology and telemetry. The costs for teleconsultation and telepathology are relatively high, and teleconsultation requires strong medical technical capabilities; telepathology necessitates specialised technical personnel and suitable medical equipment. Tele-imaging and telecardiography present data in the form of images. Tele-imaging involves the diagnosis of various diseases through CT, MRI, while telecardiography involves a single disease and focuses more on cardiac disease management. Telemetry is considered auxiliary diagnostic measures in certain situations. The main purpose of different telemedicine services in China is to solve the problem of uneven allocation of medical resources, 10 to bring high-quality medical resources to the grassroots level, to meet the diverse needs of different patients, to improve the accessibility of medical services, and to effectively enhance the sense of gain and well-being of the people.
Previous studies have focused on telemedicine supply models, policies and regulations, clinical efficacy, patient satisfaction and health outcomes. They evaluate and attempt to construct a dynamic new model of remote consultation,1,11 explore the impact of current policies on the development of telemedicine,12–14 investigate the current status of application of telemedicine in clinical outcomes,15–17 the economic and social benefits.18–20
More importantly, few existing studies have segmented telemedicine. Generalised telemedicine services do not reflect the development and use of different programmes. The unique economic attribute, scope of application, and usage scenarios of different telemedicine services have an impact on the decision-making of service providers, resulting in priorities and preferences. The mechanisms through which medical institutions carry out and utilise various types of telemedicine service projects and the influencing factors and spatiotemporal characteristics have not been elucidated.
This study utilises telemedicine data from Zunyi City, a national pilot city for telemedicine in China, and employs multi-variate unordered logistic (MNL) regression method to analyse the influencing factors of medical institutions providing different types of telemedicine services. By using ArcGis 10.8 to visualise the spatiotemporal evolution characteristics of the implementation of telemedicine service projects, the study can provide references and insights for other regions to carry out telemedicine services. This work contributes to improving the accessibility of medical services and supplements and expands the literature on telemedicine services research in low- and middle-income countries.
Objective
Preferences for the provision of different telemedicine service lines and the factors influencing them, with spatiotemporal profiling.
Methods
Study design and setting
In 2016, China issued the ‘Basic Functional Specifications for Telemedicine Information Systems’, which included services such as teleconsultation, tele-imaging diagnosis, telecardiography diagnosis and telepathology diagnosis within its basic functionalities. In 2018, Guizhou Province promulgated the ‘Implementation Details of the Guizhou Province Telemedicine Service Management Measures’, adding telemetry diagnosis. Under the general classification of telemedicine, telecardiography diagnosis is considered a type of tele-imaging diagnosis. The unit price list for medical services published by Zunyi City distinguishes between tele-imaging diagnosis and telecardiography diagnosis. Therefore, this study based on local practice categorises telemedicine service projects into teleconsultation, tele-imaging, telecardiography, telepathology and telemetry.
The research nature of this study is an applied empirical study. Ethical approvals were granted by the Tongii Medical College, Tuazhong, University of Science (2022LSZ-S145). All data used in this study were obtained from a database and data were deidentified prior to analysis.
Key informant interviews
In this study, key informant interviews were conducted with managers of medical institutions of different levels and economic attributes in Zunyi City to analyse the factors affecting the development of different telemedicine service programmes in medical institutions. The patients were also interviewed to explore their use of telemedicine and their willingness to use it, in order to better enrich the quantitative findings with qualitative interview data.
The interviews with managers were: (i) What factors do you think affect the provision of telemedicine services by medical institutions; (ii) In which telemedicine service programmes do medical institutions carry out more; (iii) What do you think are the reasons for carrying out more of such telemedicine service programmes?
The interviews with patients were: (i) Are you willing to use telemedicine services? (ii) What kind of telemedicine service do you use more often? (iii) Why do you use this kind of telemedicine service?
Data source
We obtained research data from four sources. Firstly, we acquired telemedicine consultation data for 2020 and 2021 from the Medical Insurance Bureau of Zunyi City, from which the panel data from January 2020 to August 2021 is selected, consisting of 63,687 observations. Secondly, we obtained the hospital grades of the designated medical institutions from the official website of the National Health Commission of the People's Republic of China (NHC). Thirdly, we inquired about the attribute of the designated medical institutions from the National Enterprise Credit Information Publicity System. Lastly, the rise of telemedicine has the potential to innovate the spatial and temporal limitations of medical services and enhance the efficiency of resource allocation. Therefore, relying on Gaode Maps, we obtained the locations of various designated medical institutions and, based on their geographical positions, divided the areas where the designated medical institutions are located into Zunyi City and other regions.
This study only selected panel data from Zunyi City's telemedicine consultations for 20 months, from January 2020 to August 2021. And we conducted a retrospective analysis. Although this study obtained panel data on telemedicine visits in 2020 and 2021, the telemedicine programmes in Zunyi are collectively referred to in the system as ‘(new) teleconsultations’ from September 2021 onwards, which does not show the internal variability of telemedicine services and does not meet the data requirements of this study.
Data cleaning
This study fundamentally focused on revealing factors that affect the provision of different types of telemedicine service projects by medical institutions. The main entities considered are patients, medical institutions and health insurance.
As the demand side of telemedicine, the patient demographic characteristics were categorised as age and gender. Age is included in the model as a continuous variable, while gender is included as a binary variable.
As the supply side of telemedicine, medical institutions are influenced by factors such as the level of the institution and its economic attribute, all of which affect the provision of services. In China, medical institutions are primarily categorised into primary, secondary and tertiary levels, with higher levels indicating stronger service capabilities. Additionally, public medical institutions are more numerous and generally have higher service capabilities compared to private medical institutions. Therefore, the level of medical institutions is included in the model as an ordinal variable, while economic attribute are included as a binary variable.
As the payer, health insurance influences the revenue of medical institutions through factors such as patients’ insurance types, service prices and out-of-pocket payment ratio. These economic benefits, in turn, affect the implementation of telemedicine services. Since 2016, China's health insurance coverage types are divided into two categories: Urban and Rural Resident Health Insurance and Urban Employee Health Insurance. Different types of coverage offer varying reimbursement benefits. In China, medicines are classified into three categories: A, B and C. Category A medicines are fully covered by reimbursement. Category B medicines require 10% out-of-pocket expenses and the remainder are covered by reimbursement. And Category C medicines require complete out-of-pocket expenses. Different out-of-pocket payment ratios for medicines have an impact on patients’ choice of drugs, which in turn affects the economic efficiency of hospitals. Therefore, insurance type is included in the model as a binary variable, service unit price as a continuous variable, and out-of-pocket payment ratio as an ordinal variable.
Drawing on previous research and combining with Chinese characteristics, we have introduced geographical areas to obtain a more complete and objective estimation. Areas where the designated medical institutions are located are divided into Zunyi City and other areas based on their geographical location. Therefore, we included it as a binary variable in the model to ensure the objectivity and reliability of the regression results.
Statistical analysis
After the data were cleaned in Microsoft Excel, version 2018 for Windows, the data were analyzed using Statistical Package for the Social Sciences Statistics (SPSS) for Windows, version 28 software.
A descriptive analysis was used to summarise the data. The continuous variables were presented as means and the categorical variables were presented as numbers and percentages to present the different telemedicine service programme developments and the characteristics of different influencing factors. In addition, we used the one-way ANOVA and Chi-squared tests to determine the association between telemedicine service projects and independent variables for continuous and categorical variables, respectively. And we conduct multicollinearity test on all independent variables included in the analysis to ensure the objectivity and accuracy of the regression results. Figure 1 shows the methodological flowchart of this study.

Methodology flow chart.
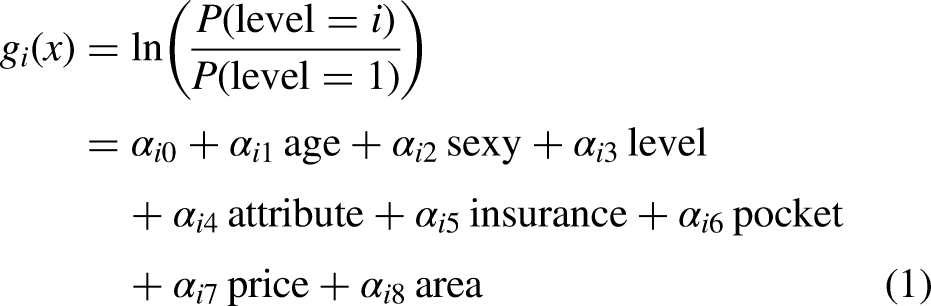
In multinomial logistic regression, the model is built using the natural logarithm of the ratio of each category of the dependent variable, excluding the reference category, to the reference category. Although this approach causes the dependent variable to lose its ordinal properties, it retains its categorical nature, which is acceptable for analysing the supply of telemedicine services. The dependent variable in this study has five different levels: teleconsultation, tele-imaging, telecardiography, telepathology and telemetry, which are assigned values of 0, 1, 2, 3 and 4, respectively. According to the requirements of the multinomial logistic regression model, the most frequently conducted tele-imaging is chosen as the reference category for the dependent variable. Assuming that all explanatory variables are effective in the multinomial logistic regression model, four different multinomial logistic regression equations can be obtained. The general form of the constructed multinomial logistic regression equation is shown in Equation (1):
Spatial visualisation analysis
The data on telemedicine service projects carried out in Zunyi counties (districts) from 2020 to August 2021 were imported into ArcGIS 10.8 for spatial distribution analysis. Five-category natural breakpoint method was applied to classify the 14 counties (districts) into five categories of very low, low, average, high and very high use levels and to map 2020 according to telemedicine service projects, respectively, January–August 2021 two-time cross-section of the spatial pattern evolution map.
Results
Results of key informant interviews
A total of 10 medical institution managers and 5 patients were interviewed, with the specific distribution shown in Table 1. Through key informant interviews, it was concluded that patients, healthcare providers and health insurance all influence the provision of telemedicine services. First, differences in patients’ age affect the choice of telemedicine service programmes, with older patients in relatively poorer health and with greater demand for telemedicine. Secondly, the service level and medical resource capacity of different levels of medical institutions, public and private hospitals vary greatly, affecting the ability of medical institutions to carry out telemedicine service programmes. Third, different medical insurance, reimbursement rates and unit prices of services will affect patients’ choices and the supply of medical services.
Summary of number of interviews.

Implementation of telemedicine services
Figure 2 shows the implementation of different telemedicine service programmes. A total of 63,687 observations were included in the study. Among the implemented telemedicine services, teleconsultation, tele-imaging, telecardiography, telepathology and telemetry accounted for 8.24% (n = 5248), 46.64% (n = 29,702), 19.96% (n = 12,709), 4.08% (n = 2,597) and 21.09% (n = 13,431), respectively. Tele-imaging had the highest implementation rate, while telepathology was the least implemented.
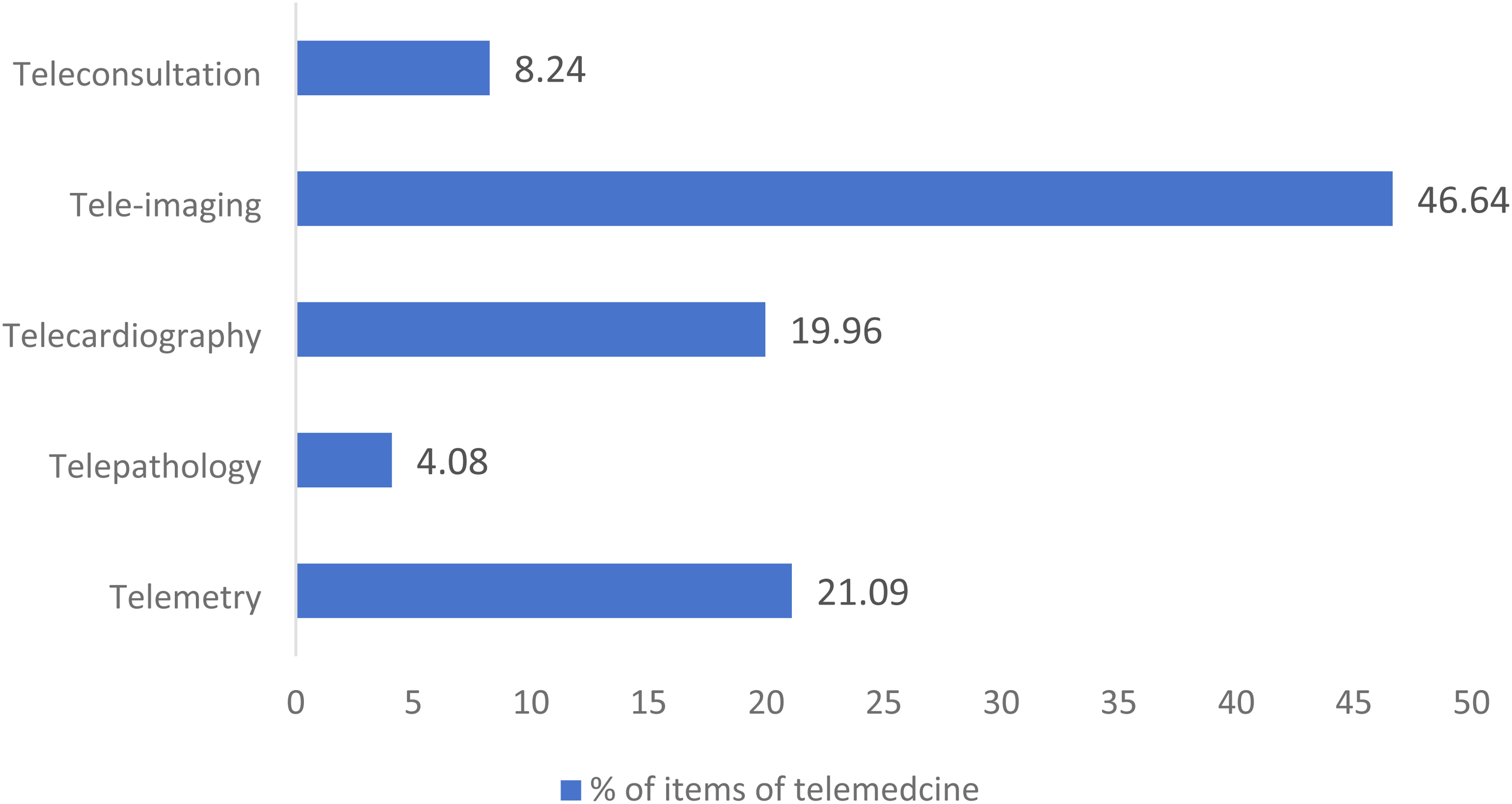
Development of different telemedicine service programmes.
Demand side: patient sociodemographic information
Table 2 shows the socio-demographic information of the patients. The average age of patients using telemedicine is 55.84 years. Patients using Teleconsultation and Telecardiography services have an average age higher than the overall average, with Telecardiography reaching 60.55 years. The proportion of female patients using telemedicine is higher than that of male patients, at 53.79% (n = 34,256) and 46.21% (n = 29,431), respectively.
Sociodemographic information of patients in different telemedicine services.

Supply side: basic information of medical institutions
The level reflects differences in the allocation of medical resources. The higher the level, the higher the level of service of the medical institution and the more complex health-care services it is able to carry out. Economic attributes refer to public and private. In China, public hospitals are the mainstay of the healthcare system, with richer medical resources and more advanced technical support, and a higher degree of patient trust; private hospitals provide personalised or specialised services, and are clearly market-based.
Table 3 shows information about the healthcare organisations. Among the levels of medical institutions, level 1 medical institutions have the highest proportions in teleconsultation, tele-imaging, telecardiography and telemetry, accounting for 70.20% (n = 3,684), 95.51% (n = 28,369), 99.40% (n = 12,633) and 56.91% (n = 7,643), respectively. Level 2 medical institutions conduct the most telepathology, accounting for 57.03% (n = 1,481), while level 3 medical institutions have the lowest proportions in all categories. Public hospitals have the highest overall proportion at 80.63% (n = 51,350). In telemetry, the proportion of private hospitals is greater than that of public hospitals, at 59.81% (n = 8,033) and 40.19% (n = 5,398), respectively. In other telemedicine services, public hospitals have higher proportions than private hospitals.
Information of medical institution in different telemedicine services.

Payer: health insurance status
In China, basic medical insurance is mainly divided into ‘urban and rural residents medical insurance’ and al insurance is mainly divided i’, both of which have different reimbursement rates and cover different groups of people, and will directly affect patients’ ability to pay and choice of services. The out-of-pocket payment ratio determines the proportion of healthcare costs that the patient has to bear, which directly affects the patient's choice of telemedicine services. The unit price not only affects patients’ choice of telemedicine service items, but also has an impact on healthcare organisations to carry out telemedicine service items.
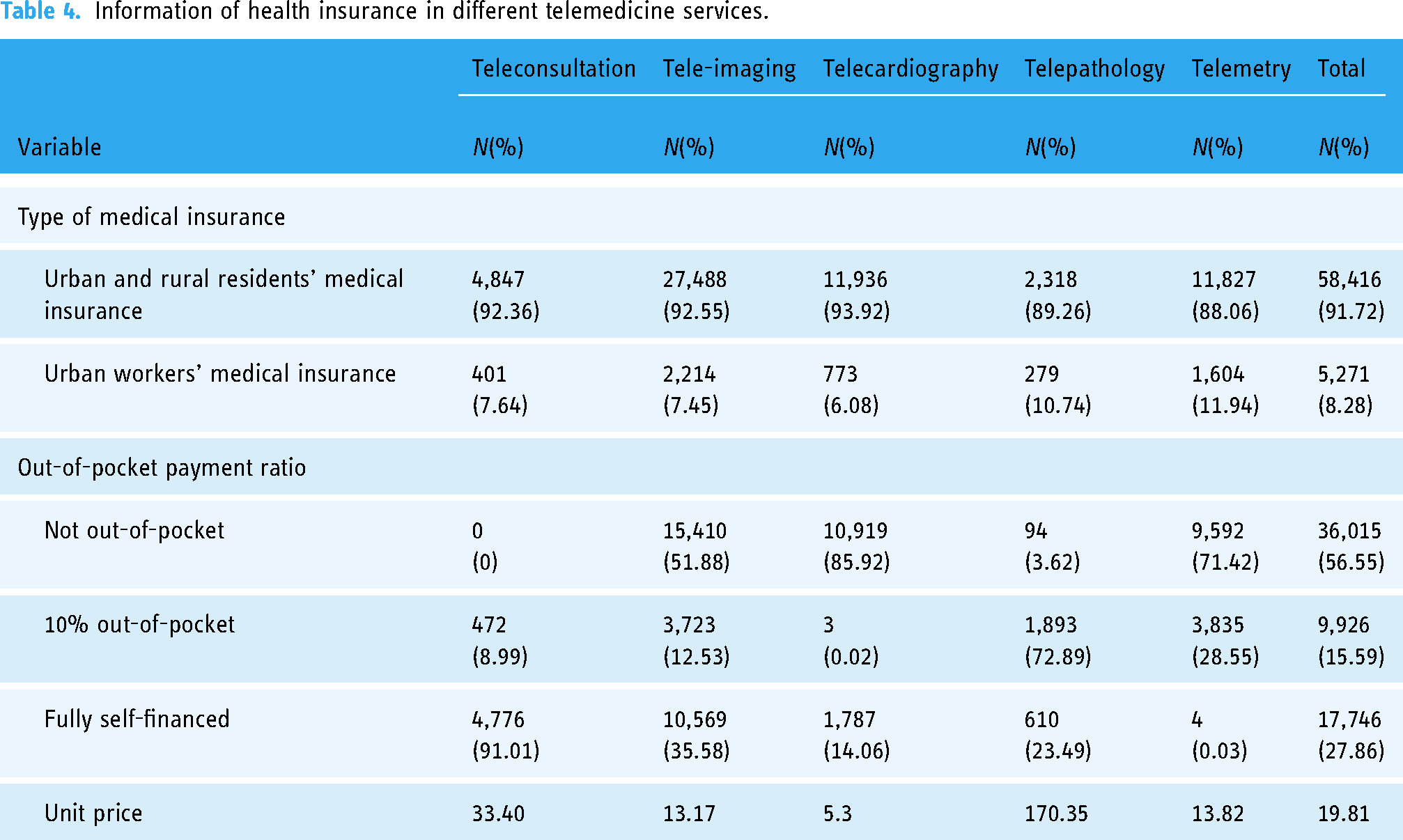
Table 4 shows the information about health insurance. 91.72% of telemedicine patients are covered by Urban and Rural Residents’ Medical Insurance, and this group accounts for the majority in all telemedicine services. In teleconsultation, 91.10% (n = 4,776) of the medicines require full self-financing; in tele-imaging, telecardiography and telemetry, the highest proportions of medicines are fully reimbursed, accounting for 51.88% (n = 15,410), 85.92% (n = 10,919) and 71.41% (n = 9,592), respectively. In telepathology, 72.89% (n = 1,893) of the medicines are 10% out-of-pocket before being reimbursed, and 23.49% (n = 610) of the medicines are fully self-financed.
Information of health insurance in different telemedicine services.
Geographic areas
With the problem of uneven distribution of medical resources highlighted in China, telemedicine is especially critical in areas where medical resources are scarce, transport is inconvenient and the economy is underdeveloped.
Table 5 shows information about the geographic area. In Zunyi City, most patients choose medical institutions located within the city for their telemedicine services, with only 3.66% (n = 2,330) choosing institutions outside the city.
Information of geographic area in different telemedicine services.

The association of telemedicine service provision and the characteristics with the dependent variable
Table 6 shows the results of one-way ANOVA for continuous variables in the independent variables and chi-square test for categorical variables. The differences in age, gender, type of medical insurance, out-of-pocket payment ratio, unit price of services, level and economic attribute of medical institutions and area of consultation were statistically significant for each service of telemedicine (P < 0.05).
General statistics of each service item of telemedicine.

Note: a is the value of F.
Multicollinearity test
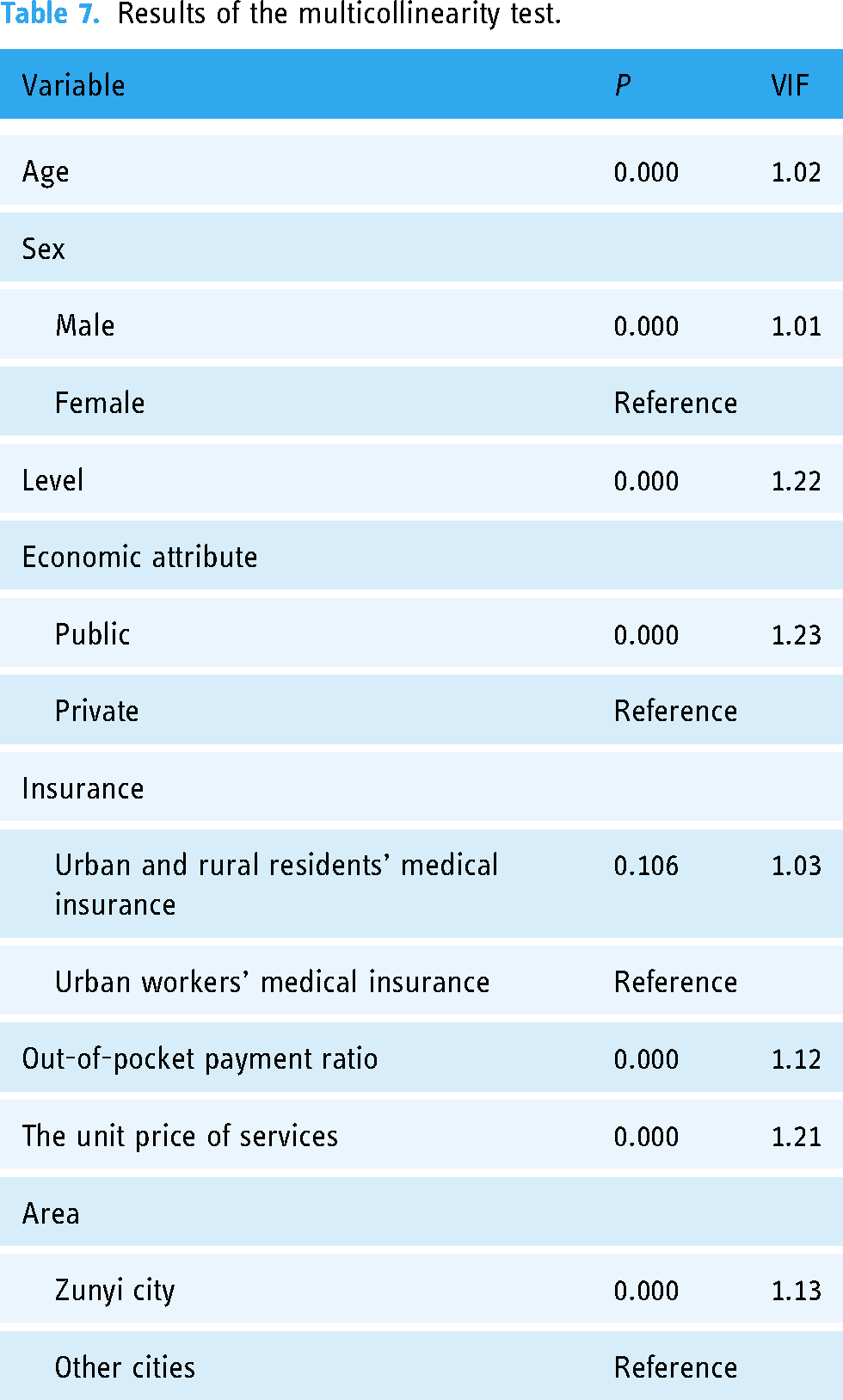
Table 7 shows the results of the Multicollinearity test for the variables. Only the type of medical insurance has a P-value of >0.05, which is not significant, while the P-values of the remaining variables are less than 0.001, which indicates that the differences are extremely significant. Therefore, the variable of health insurance was excluded. In addition, the variance inflation factor (VIF value) as well as the mean value of VIF for all the variables were less than 5, and multicollinearity was not found.
Results of the multicollinearity test.
Multinomial logistic regression
Table 8 reports the estimation results of the MNL model and is divided into four parts: the first group is used to analyse the results of teleconsultation with tele-imaging, the second group is used to analyse the results of telecardiology with tele-imaging, the third group is used to analyse the results of tele-imaging with telepathology and the fourth group is used to analyse the results of tele-imaging with telemetry. Among the seven explanatory variables, including age, gender, level and economic attribute of medical institutions, out-of-pocket payment ratio, the unit price of services, and geographical areas, the relationship between the out-of-pocket payment ratio, the unit price of services, level and economic attribute of the medical institutions had a statistically significant effect on the selection of all telemedicine services (P < 0.05).
Regression results.

The results of the MNL model showed that the higher the level of the medical institution is, the stronger the willingness to carry out teleconsultation, telepathology and telemetry will be (ORs of 14.052, 8.071 and 13.113, respectively), and did not tend to choose telecardiography diagnosis. In addition, the higher the level, the weaker the provider's willingness to conduct telecardiography and the more willing they are to conduct tele-imaging.
Compared with private hospitals, the probability of public hospitals carrying out teleconsultation and telecardiology diagnosis is 17.760 times and 12.248 times higher than that of tele-imaging diagnosis, and the multiplier of carrying out telepathology diagnosis is as high as 87.860 times. At the same time, public hospitals are less willing to carry out the telemetry and diagnosis.
A 1-unit increase in the out-of-pocket rate increased the probability of providers conducting teleconsultation and telepathology by 48.407 and 4.039 times, respectively. The probability of choosing telecardiology and telemetry diagnosis was smaller (ORs of 0.591 and 0.242).
For every 1-unit increase in price, the probability that a healthcare organisation will conduct teleconsultation and telepathology increases by 0.023 and 0.058 times. By contrast, telecardiography and telemetry presented lower sensitivities relative to tele-imaging (ORs of 0.775, 0.997).
Analysis of the spatio-temporal evolution of telemedicine service programmes in Zunyi City
Figure 3 shows that different telemedicine services present different characteristics at different times. Low values are mainly distributed in the east and north of the country, where the economic level is poor. Teleconsultation is characterised by ‘low-value expansion.’ The low-value districts and counties of tele-imaging are mainly in the eastern and north-western regions. Telecardiography is carried out in fewer areas; in 2021, there will still be nine counties that have yet to carry out this service. Telepathology presents the spatial and temporal evaluation characteristics of ‘high-value expansion and low-value contraction’. Telemetry shows the characteristic of ‘bipolar contraction, median expansion’, with a significant decrease in extremely low-value areas. In addition, Rincheon is the district and county with the highest level of economic development in Zunyi City, but it has the lowest value in each of the four remote service items, and a lower value for telemetry.

Changes in telemedicine services in Zunyi in 2020 and 2021.
Discussion
Principal findings
To our knowledge, this study is the first in mainland China to use the MNL model to explore the influencing factors and spatial and temporal evolutionary characteristics of telemedicine service provision.
This study resulted in three key findings. First, the level and economic attribute of healthcare institutions, the out-of-pocket payment ratio and the unit price of services affect the supply of different telemedicine services in healthcare institutions.
Second, all medical institutions will tend to prioritise projects that are expensive and provide profit. In the higher level of hospitals and Chinese public hospitals, the willingness to carry out the projects that require more medical resources and higher medical technology is stronger, that is teleconsultation and telepathology diagnosis. Tele-imaging, telecardiology and telemetry have their own focus in different levels and attribute of medical institutions.
Third, the effectiveness of telemedicine development may have a non-linear inverted ‘U’ pattern with the level of economic development.
Comparison with other studies and explanation
Level of medical institution
This study indicates that compared to tele-imaging, higher-level medical institutions exhibit a stronger willingness to engage in teleconsultation, telepathology and telemetry, with telecardiography being relatively weaker. Zhang X and others previously concluded in their analysis of telemedicine in Henan Province that teleconsultation and telepathology are more commonly conducted in higher-level hospitals. 21 This study supports the idea that the present study. During the field research, it was found that more complex telemedicine services are carried out by high-level medical institutions, such as teleconsultation, telepathology, etc., and that telemetry is carried out more often, mainly because of the needs of the disease, and that the hospital has advanced equipment to deal with the disease more accurately.
This is mainly related to the significant differences in the allocation of healthcare resources across different levels of medical institutions.22,23 Higher-level medical institutions typically gather experts in the field and possess more advanced medical equipment. 23 Wilson ML and other scholars, when exploring key gaps in accessing pathology and laboratory medicine services, also concluded that well-equipped medical institutions are crucial for accurate diagnosis and effective treatment. 24 Teleconsultation, telepathology and telemetry can cover more about the precise analysis of the case and personalised treatment, which cannot be provided by tele-imaging. Dealing with complex and special cases should maximise the technical advantages of high-level medical institutions, expand the influence. Tele-imaging covers a variety of systems of disease screening,25–28 making it relatively complex, whereas telecardiography involves fewer diseases. In addition, some primary care institutions can carry out primary telecardiography, and the price of telecardiography service is 5.3 yuan, which is the lowest economic benefit for high-grade hospitals.
Economic attribute of medical institutions
This study also investigated the economic attribute of healthcare organisations with a view to understand the extent to which it influences healthcare organisations that carry out different telemedicine service programmes. The study results indicate that compared to private hospitals, public hospitals in China have a higher willingness to engage in teleconsultation, telecardiography and telepathology than in tele-imaging, and a lower willingness to engage in telemetry. Although the Chinese government is strongly supporting private hospitals, 29 public hospitals have richer medical resources and more advanced technical support. Patients also have higher trust and reliance on public hospitals. The interview process with patients also revealed that patients preferred telemedicine services in public hospitals, and although hospitals were able to provide similar services, patient trust was not strong. Tele-imaging often requires higher level of investment in imaging equipment and technological updates, while teleconsultation, telecardiology and telepathology rely more on the knowledge output and data analysis of a team of specialists. Healthcare organisations may not be inclined to carry out tele-imaging due to cost considerations. Public hospitals have a lower willingness to engage in telemetry diagnosis. This finding may be due to the fact that public hospitals themselves have access to more satisfactory testing services, and patients do not need remote testing, so the demand is low.
Out-of-pocket payment ratio
Previous studies have demonstrated that changes in telemedicine reimbursement policies and coverage have led to variations in the adoption and usage rates by healthcare providers.30,31 Whether telemedicine can be reimbursed remains controversial in China. 32 Relative to the reimbursement rate is the out-of-pocket ratio. The results of this study indicate that with an increase in the out-of-pocket proportion, medical institutions show a greater willingness to engage in teleconsultation and telepathology compared to tele-imaging, and a higher willingness to engage in tele-imaging than in telecardiography and telemetry. On one hand, teleconsultation is usually able to connect to high-quality healthcare resources, and telepathology involves complex processes of sample collection and transmission, 33 both of which are costly. The increase in the out-of-pocket percentage means that health insurance reduces the subsidy for this part of the service, and healthcare organisations are more willing to carry out value-added telemedicine services. On the other hand, telecardiology is not out-of-pocket and only out-of-pocket for 10% of the patients amounted to 85.94%, and telemetry is even as high as 99.97%. If the proportion of out-of-pocket payment rises, then these patients will resist, thus reducing the demand, lowering the level of medical service utilisation, resulting in a waste of medical resources, and reducing the willingness of medical institutions to carry out the service.
Unit price of service items
Whether the costs incurred by medical institutions in carrying out telemedicine service programmes can be reasonably reimbursed is a core factor that affects their ability to carry out different telemedicine service programmes. In previous studies, it has been demonstrated that the issue of cost-effectiveness is faced in telemedicine.34,35 China has not yet fully established a financial compensation mechanism for telemedicine construction in medical institutions. The results of this study indicate that with an increase in price, medical institutions show a higher willingness to engage in teleconsultation and telepathology compared to tele-imaging, while their willingness to engage in telecardiography and telemetry is lower than for tele-imaging. This may be related to the cost reimbursement and substitutability of different service items.
Teleconsultation and telepathology have higher costs; teleconsultation can provide high-quality services, 36 and telepathology involves a high level of diagnostic difficulty. 37 Higher prices help providers cover the costs of such services, and more cost-effectiveness helps providers increase such services. It can also stimulate investment and service upgrades in healthcare organisations. In addition, tele-imaging is crucial for the diagnosis of many diseases 38 and is highly irreplaceable. Telecardiography and telemetry are considered auxiliary diagnostics in some cases; if prices rise, patients might opt for alternative options. The medical institutions’ managers and patients alike share the view that the increase in the number and popularity of intelligent wearable devices has led to a significant reduction in patient demand for telecardiology, and how patients do not need to rely on traditional telecardiology services by monitoring their own health in real time through portable devices. Demand decreases, and the frequency with which healthcare organisations carry it out decreases accordingly. Additionally, the results of this study indicate that the unit prices for telecardiography and telemetry are relatively low (5.3 yuan and 13.82 yuan, respectively). Even if prices increase, the revenue growth for service providers remains slow, reducing the motivation for medical institutions to offer these services.
Spatiotemporal evolution characteristics
This study found that the effectiveness of telemedicine development may have a non-linear inverted ‘U’ pattern with the level of economic development. Xu W and others believe that the coverage of telemedicine is highest in the western region, followed by the central region and lowest in the eastern region. There is a negative relationship between regional development levels and telemedicine coverage. 39 This differs from the conclusions of this study, possibly because it focuses on a national scale, whereas this study is specific to Zunyi City, which has a smaller scope.
Although economically underdeveloped regions have received financial support from the government, 40 their utilisation remains insufficient. 41 Most patients are unaware of the advantages of telemedicine and are accustomed to face-to-face consultations, leading to poor implementation of telemedicine. However, the best economic condition of the region is due to the economic development of the region. At high level of medical care, patients enjoy the best medical services. Face-to-face treatment can meet the needs of patients. On the other hand, regions with medium level of economic development have sufficient funds to build a telemedicine service system; patients have a greater demand for higher-level services, which together promote the development of telemedicine.
Insufficient research
This study has three limitations. First, due to the limitations of acquiring data, only the telemedicine consultation data of Zunyi City from 2020 to August 2021 were included in the analysis. The short duration of the study, as well as the limitations of the study's data variables, do not fully reflect the factors influencing the supply of telemedicine services. Secondly, When examining the characteristics of spatio-temporal evolution, it only correlates economic levels with the implementation of local telemedicine services, which is far from sufficient. Given that the study period includes the COVID-19 pandemic in China, future research should further explore the impact of telemedicine interventions at different stages on patient health outcomes or patient satisfaction. Finally, the global healthcare system has undergone tremendous changes due to the impact of COVID-19. To avoid cross-infection of the virus, many patients have turned to online telemedicine, which is an ideal way to ensure medical services without increasing the risk of virus transmission. However, in this paper, this influence of the COVID-19 pandemic was not considered due to limited data.
Conclusion
Medical institutions have a certain order of priority in carrying out telemedicine service programmes. Their decisions are often influenced by factors such as price levels, out-of-pocket payment ratio and level and economic attribute of the medical institution. In addition, regions with low levels of economic development tend to have poor telemedicine service programmes. For this reason, the state should focus on its policy-oriented role and implement financial tilts and special funds to help economically disadvantaged regions. They should provide the necessary financial, technological and resource support to effectively deal with various difficulties and constraints encountered in telemedicine practice. Breaking down time and space constraints will enable patients to enjoy high-quality medical and health-care services close to their homes and promote fair access to and equalisation of medical services.
Footnotes
Abbreviations
Contributors
Xueyu Zhang and Yingchun Chen designed this study and performed the statistical analysis. Xueyu Zhang wrote the main manuscript text. Huawei Tan participated in data analysis. All authors reviewed the manuscript.
Consent to participate
No informed consent was required for this study. All data used in this study were obtained from a database and data were deidentified prior to analysis.
Consent for publication
Not applicable
Data availability
The data that support the findings of this study are available from Zunyi City Local Health Security Administration but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. However, data are available from the authors upon reasonable request and with permission of Zunyi City Health Security Administration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approvals were granted by the institutional review board of the Tongii Medical College, Huazhong University of Science and Technology (2022LSZ-S145).
Funding
This study was supported by grants from the National Natural Science Foundation of China (71974066, 72374076).
Guarantor statement
We the undersigned declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere.
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
Guarantor: Xueyu Zhang.