
Abstract
Volatile anesthetics have been shown to modulate polymorphonuclear neutrophil (PMN) functions. The aim of this study was to examine the impact of clinically relevant concentrations of sevoflurane (SEVO), a volatile anesthetic, on the release of reactive oxygen species (ROS), myeloperoxidase (MPO), and elastase (EL) from human activated PMNs. For this purpose, samples of whole blood were collected from healthy volunteers and exposed in vitro to 2.3% or 4.6% SEVO in air. To assess for a stimulus-dependent effect of the volatile anesthetic, PMNs were activated using different validated protocols. Artificial stimulation of neutrophils involved either a combination of cytochalasin B (CB) and N-formyl-methionyl-leucyl-phenylalanine (fMLP) or phorbol 12-myristate 13-acetate (PMA). In addition, a combination of lipopolysaccharide (LPS) and tumor necrosis factor alpha (TNF-α) was also tested as a natural activation mean of PMNs. The production of ROS by PMNs was assessed by L-012 chemiluminescence. Total MPO and EL released in supernatant were measured by enzyme-linked immunosorbent assay (ELISA). Furthermore, degranulation of the active fraction of MPO was also measured by specific immunological extraction followed by enzymatic detection (SIEFED). Overall, SEVO enhanced the release of ROS, MPO, and EL following artificial stimulation of PMNs but the volatile anesthetic inhibited the degranulation of active MPO and EL after neutrophil exposure to LPS and TNF-α. This study highlighted that the effect of SEVO on activated PMNs is dependent on the conditions of cell stimulation. These properties should be taken into consideration in future studies investigating immunomodulatory effects of volatile anesthetics.
Keywords
Introduction
Inflammation is an adaptive process involving activation of polymorphonuclear neutrophils (PMNs) which are among the first phagocytic cells recruited to remove damaged tissues and invading pathogens. 1 Although pivotal for innate immune defense, the response of PMNs lacks selectivity and can paradoxically inflict collateral damages to the host. Indeed, the oxidant response of PMNs leads to the release of reactive oxygen species (ROS) and myeloperoxidase (MPO) that are responsible for oxidative injuries to healthy tissues.2,3 In addition, neutrophils synthesize non-oxidant proteolytic enzymes such as elastase (EL) which has shown a high destructive potential on extracellular matrix and neighboring cells. 4 In clinical conditions, the oxidant burden of PMNs and the release of EL have been correlated with the severity of trauma and the risk of complications after major surgery.5,6
Halogenated anesthetics possess anti-inflammatory properties that have been advocated to potentially reduce the neutrophil-mediated damages associated with tissue trauma 7 and infection. 8 Halogenated anesthetics inhibit the neutrophil oxidative pathways9,10 and reduce EL release during inflammation.11,12 However, laboratory studies that specifically investigated the effects of volatile anesthetics on the production of ROS by PMNs led to variable results.13,14 Furthermore, there are only scarce data on the effects of volatile anesthetics on MPO9,10 and EL.11,12
We conducted the present in vitro study to precise the effects of clinically relevant concentrations of SEVO on the production of ROS, MPO, and EL from human PMNs activated in whole blood. For this purpose, we activated PMNs with different validated protocols. Artificial stimulation of PMNs involved a combination of cytochalasin B (CB) plus N-formyl-methionyl-leucyl-phenylalanine (fMLP) or phorbol 12-myristate 13-acetate (PMA) alone. CB, a cell-permeable fungal metabolite, sensitizes PMNs to subsequent stimuli through a cytoskeleton disrupting effect while fMLP, a synthetic compound acting on specific membrane receptors, mimics the N-formyl-peptides released from damaged mitochondria and bacteria during host cell injury and pathogen invasion. 15 PMA is a plant-derived analogue of diacylglycerol (DAG) that directly activates intracellular protein kinase C (PKC). 16 In addition to artificial stimuli, we activated PMNs with a natural receptor-dependent stimulus consisting of a combination of lipopolysaccharide (LPS) and tumor necrosis factor alpha (TNF-α). LPS is specifically recognized by PMNs through toll-like receptor 4 (TLR4). After exposure to LPS in vivo, TNF-α mainly produced by macrophages further amplifies PMNs reactivity via activation of the p55- and p75-TNF-α receptors. 17 For this study, we specifically postulated that SEVO might differentially affect the release of ROS, MPO, and EL depending on which compounds were used for neutrophil activation.
Materials and methods
Blood samples
After approval of our local Ethics Committee (2010-018453-35) and written informed consent, samples of whole venous blood were collected from 12 adult healthy volunteers (mean age of 36 years, range 25–50 years) into ethylenediaminetetraacetic acid (EDTA) tubes.
Assessment of sevoflurane cytotoxicity on PMNs
First, we performed a preliminary experiment to test the potential cytotoxic effect of the volatile anesthetic on neutrophils. Human PMNs were isolated as previously described 18 in phosphate-buffered saline (PBS). Isolated PMNs were exposed to 2.3% or 4.6% SEVO in air during 2 h at 37°C, and then, a Trypan blue exclusion test was used to assess the effect of the anesthetic on cell viability.
Stimulation of PMNs in whole blood
Primers and activators of PMNs were purchased from Sigma-Aldrich (Diegem, Belgium). PMNs’ responsiveness in whole blood was enhanced by prior exposure to the primers CB or Escherichia Coli–LPS. Full activation process was reached upon subsequent exposure to fMLP after CB or human tumor necrosis factor alpha (TNF-α) after LPS. In a third experiment, PMA was used alone since this compound is able to induce a strong neutrophil activation without previous priming. CB (5 mg/mL) was dissolved in dimethyl sulfoxide (DMSO), and an adequate volume of this solution was added to the whole blood to reach the final concentration of 5 μg/mL CB and 0.1% DMSO. PMA and fMLP were dissolved in DMSO, and aliquots were kept refrigerated at −20°C. Just prior to use, distilled water was added to the aliquots to obtain a stock solution of PMA (1.6 × 10−5 M) with 1% DMSO and a stock solution of fMLP (1 × 10−4 M) with 10% DMSO. Adequate volumes of these stock solutions were added to the whole blood to reach the final concentration of 8 × 10−7 M PMA and 0.05% DMSO or 1 × 10−6 M fMLP and 0.1% DMSO. When neutrophils were stimulated with CB-fMLP, the final percentage of DMSO into the sample was 0.2%. LPS (1 mg/mL), and TNF-α (1 µg/mL) was dissolved in a 20 mM PBS solution (pH 7.4) and added to the blood samples to reach the final concentration of 10 µg/mL LPS and 10 ng/mL TNF-α. For each stimulus, the effects of the vehicle solutions (DMSO solutions or PBS) were also studied as controls.
Exposure of blood samples to sevoflurane
Our methodology to expose blood samples to halogenated anesthetics has already been described.19,20 SEVO was administered for 1 h at concentrations of 2.3% and 4.6% to reproduce duration of anesthetic exposure and doses likely to be encountered in clinical practice. These concentrations of SEVO correspond to 1 and 2 minimum alveolar concentrations (MAC); 1 MAC (often referred to as the ED50) is defined as the concentration of volatile anesthetic required to suppress movement to a surgical incision in 50% of patients. SEVO (Sevorane®; Abbott Laboratories, Wavre, Belgium) was administered in an air tight modular incubator chamber (Billups-Rothenberg, Del Mar, CA, USA) with inflow and outflow connectors. SEVO was delivered with air as the carrier gas through the inlet port connected to a specific calibrated vaporizer (Dräger, Lübeck, Germany). The outlet port was connected to a Capnomac Ultima® multigas analyzer (Datex Ohmeda, Helsinki, Finland) that measured anesthetic concentrations.
Our experimental model consisted of an incubation of blood samples during 1-h exposure to air or SEVO with CB (5 μg/mL) or LPS (10 µg/mL) followed by activation with fMLP (10−6 mol/L) or TNF-α (10 ng/mL) in air. Stimulation with PMA (8 × 10−7 mol/L) was made without priming and after 1-h incubation of the whole blood in either air or SEVO. All the tests were performed under a slight stirring (70 r/min) and at 37°C.
Measurement of the production of ROS by PMNs in whole blood
To study the production of ROS by stimulated PMNs, the blood was diluted 50 times in PBS and poured (100 µL/well) into 96-well white microtiter plates (White Combiplate 8; Fisher Scientific, Gent, Belgium). CB or LPS was added immediately before the exposure to air or SEVO. Thereafter, all diluted blood samples were returned to room air at 37°C and PMNs were activated with fMLP, TNF-α, or PMA in the presence of 10 µL of a water solution of 8-amino-5-chloro-7-phenylpyrido[3,4-d]-pyridazine-1,4-(2H,3H) dione (L-012, 1.26 mg/mL), and chemiluminescence (CL) was measured for 60 min with a Fluoroskan Ascent FL (Thermo Labsystems, Helsinki, Finland) according to a method previously described by Imada et al. 21 with minor modifications. Thus, for these experiments, the total duration of priming plus activation steps of PMNs lasted 120 min. Control tests were performed in parallel with unstimulated blood samples in the same conditions and after exposure to air or SEVO.
Measurement of total MPO, active MPO, and EL released by PMNs in whole blood
For the measurement of total and active MPO fractions and EL released by activated PMNs, blood samples (2 mL/well) were put in a six-well cell culture plate (NunclonTM delta surface; Nunc, Roskilde, Denmark). Whole blood was incubated with CB or LPS during the 1-h exposure to air or SEVO. Thereafter, all blood samples were returned to room air at 37°C and PMNs were activated with fMLP, TNF-α, or PMA during 30 min. Thus, for these experiments, the total duration of priming plus activation steps of PMNs lasted 90 min. Control tests were performed in parallel with unstimulated blood samples also exposed to air or SEVO.
After 90 min, blood samples were centrifuged (450g, 10 min) and the plasma was collected to measure total MPO, active MPO, and EL released by PMNs. Before the MPO assays, plasma samples were diluted 10 fold with 20 mM PBS buffer at pH 7.4 and added with 5 g/L bovine serum albumin (BSA) and 0.1% Tween 20. An ELISA was used to measure total human MPO (MPO ELIZEN; Zentech, Liège, Belgium). The active MPO fraction released by PMNs was measured by a method called “specific immunological extraction followed by enzymatic detection” (SIEFED) developed for the specific detection of active human neutrophil MPO. 22 For the measurement of EL, plasma was diluted 100 fold with a ready-to-use diluent provided by the manufacturer, and then, EL was measured with a human PMN elastase ELISA kit (ab119553; Abcam).
Statistical analysis
According to previous studies in animal,19,20 we estimated that 12 samples of blood (each sample drawn in a different healthy donor) would be sufficient to detect differences in ROS, total MPO, active MPO, and EL between control and SEVO-exposed blood. The experiments were conducted independently for the 12 individual samples of blood with each condition repeated in duplicate. The relative effects of stimulation and SEVO were calculated for each independent experiment in comparison to the unstimulated control group in air such that results are normalized by donor. Global data obtained from the 12 samples of blood are presented as median and quartiles (interquartile range, minimum–maximum) in relative values (%) of the control groups (unstimulated cells in air defined as 100%) and analyzed using Kruskal–Wallis test with Dunn’s post hoc test for multiple comparisons between groups with the software GraphPad Prism 7.0c (GraphPad Software, San Diego, CA, USA); p < 0.05 was considered statistically significant.
Results
Effect of sevoflurane on PMNs viability
The viability of PMNs measured by the Trypan blue exclusion test was >95% and not significantly different after exposure to air, 2.3% and 4.6% SEVO. Thus, the changes observed in ROS production and MPO or EL release were not attributable to neutrophil death induced by SEVO exposure during the time interval of investigations.
Effect of sevoflurane on the production of ROS by PMNs
As compared with unstimulated PMNs, control tests with DMSO alone or PBS alone showed no significant changes in the release of ROS either under air (+2%, p > 0.05 with DMSO 0.05%; +4%, p > 0.05 with DMSO 0.2%; +3% with PBS), 2.3% SEVO (+7%, p > 0.05 with DMSO 0.05%; +6%, p > 0.05 with DMSO 0.2%; +6% with PBS) and 4.6% SEVO (+6%, p > 0.05 with DMSO 0.05%; +5%, p > 0.05 with DMSO 0.2%; +7% with PBS). The combination of CB + fMLP and PMA resulted in a significant increase in ROS production as compared with unstimulated cells either in air or under 2.3% and 4.6% SEVO. The combination of LPS + TNF-α slightly increased the production of ROS in air and in 2.3% and 4.6% SEVO, but these differences were not statistically significant (Figure 1). Furthermore, in comparison with the corresponding tests performed in air, 2.3% SEVO significantly increased the production of ROS by CB + fMLP-stimulated PMNs (+273%) but did not affect the ROS production by unstimulated PMNs and by PMA- and LPS + TNF-α-stimulated neutrophils. Under 4.6% SEVO, the production of ROS increased significantly with CB + fMLP- (+ 316%) and PMA-stimulated PMNs (+ 12%) in comparison to the corresponding air conditions but no differences were observed for unstimulated and LPS- + TNF-α-stimulated PMNs (Figure 1).
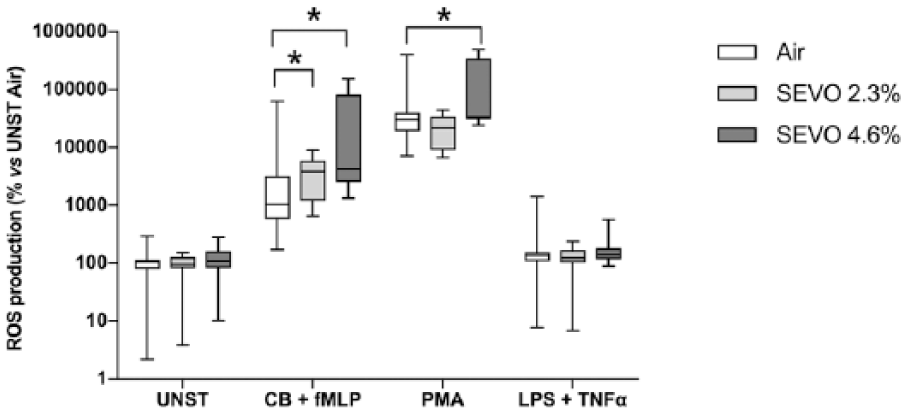
Effect of sevoflurane (SEVO) on the production of ROS by unstimulated (UNST), CB + fMLP-, PMA- and LPS + TNF-α-stimulated neutrophils in whole blood. Results are expressed as relative values (%) of the unstimulated control group in air considered as 100%. Data are median (interquartile range, minimum–maximum) of 12 independent experiments carried out in duplicate (n = 24). *p < 0.05 for the difference between air and SEVO-exposed samples within each condition of neutrophil activation.
Effect of sevoflurane on total MPO release by PMNs
As compared with unstimulated PMNs, control tests with DMSO alone or PBS alone showed no significant changes in the release of total MPO either under air (−3%, p > 0.05 with DMSO 0.05%; +5%, p > 0.05 with DMSO 0.2%; +4% with PBS), 2.3% SEVO (+5%, p > 0.05 with DMSO 0.05%; −4%, p > 0.05 with DMSO 0.2%; −5% with PBS), and 4.6% SEVO (+6%, p > 0.05 with DMSO 0.05%; +6%, p > 0.05 with DMSO 0.2%; +7% with PBS). As compared with unstimulated cells, CB + fMLP and PMA significantly increased the total MPO release by PMNs in air and in 2.3% and 4.6% SEVO. In addition, LPS + TNF-α significantly increased the total MPO release in air and 4.6% SEVO but not in 2.3% SEVO (Figure 2). Furthermore, in comparison with the corresponding tests performed in air, 2.3% SEVO did not change the release of total MPO by unstimulated and stimulated PMNs. However, 4.6% SEVO increased the release of total MPO by CB- + fMLP-stimulated PMNs (+87%) but not by unstimulated PMNs and PMA- and LPS- + TNF-α-stimulated PMNs (Figure 2).
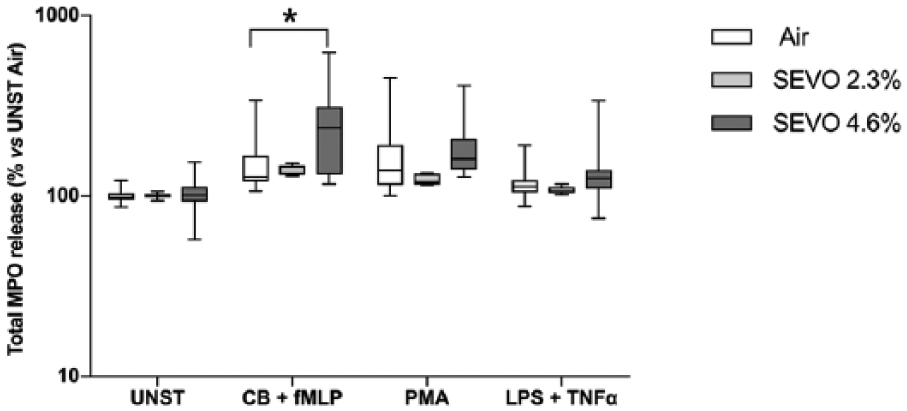
Effect of sevoflurane (SEVO) on the release of total MPO by unstimulated (UNST), CB- + fMLP-, PMA-, and LPS- + TNF-α-stimulated neutrophils in whole blood. Results are expressed as relative values (%) of the unstimulated control group in air considered as 100%. Data are median (interquartile range, minimum–maximum) of 12 independent experiments carried out in duplicate (n = 24). *p < 0.05 for the difference between air and SEVO-exposed samples within each condition of neutrophil activation.
Effect of sevoflurane on active MPO release by PMNs
As compared with unstimulated PMNs, control tests with DMSO alone or PBS alone showed no significant changes in the release of active MPO either under air (+4%, p > 0.05 with DMSO 0.05%; −5%, p > 0.05 with DMSO 0.2%; −2% with PBS), 2.3% SEVO (+3%, p > 0.05 with DMSO 0.05%; +7%, p > 0.05 with DMSO 0.2%; −4% with PBS) and 4.6% SEVO (+5%, p > 0.05 with DMSO 0.05%; −3%, p > 0.05 with DMSO 0.2%; −2% with PBS). The combination of CB + fMLP and PMA alone as well as the combination of LPS + TNF-α resulted in a significant increase in active MPO degranulation in air, 2.3% and 4.6% SEVO (Figure 3). In comparison with the corresponding tests in air, 2.3% SEVO significantly increased the release of active MPO by CB + fMLP- (+580%) and PMA- (+93%) stimulated PMNs. Conversely, this concentration of SEVO significantly reduced the active MPO release by unstimulated (−36%) and LPS + TNF-α- (−23%) stimulated PMNs. Administration of 4.6% SEVO significantly increased the degranulation of active MPO by CB + fMLP- (+85%) stimulated PMNs but decreased it significantly by unstimulated (−32%) and LPS- + TNF-α- (−33%) stimulated PMNs. At this concentration, the volatile anesthetic did not change the release of active MPO from PMA-stimulated PMNs (Figure 3).

Effect of sevoflurane (SEVO) on the release of active MPO by unstimulated (UNST), CB + fMLP-, PMA-, and LPS + TNF-α-stimulated neutrophils in whole blood. Results are expressed as relative values (%) of the unstimulated control group in air considered as 100%. Data are median (interquartile range, minimum–maximum) of 12 independent experiments carried out in duplicate (n = 24). *p < 0.05 for the difference between air and SEVO-exposed samples within each condition of neutrophil activation.
Effect of sevoflurane on EL release by PMNs
As compared with unstimulated PMNs, control tests with DMSO alone or PBS alone showed no significant changes in the release of EL either under air (−2%, p > 0.05 with DMSO 0.05%; −3%, p > 0.05 with DMSO 0.2%; +4% with PBS), 2.3% SEVO (−3%, p > 0.05 with DMSO 0.05%; +1%, p > 0.05 with DMSO 0.2%; −5% with PBS) and 4.6% SEVO (+3%, p > 0.05 with DMSO 0.05%; +2%, p > 0.05 with DMSO 0.2%; −2% with PBS). As compared with unstimulated cells, CB + fMLP and PMA significantly increased the release of EL by PMNs in air and in 2.3% and 4.6% SEVO. However, LPS + TNF-α had no significant effect on EL release in air as well as under 2.3% and 4.6% SEVO (Figure 4). Furthermore, in comparison with the corresponding tests performed in air, 2.3% SEVO significantly increased (+ 129%) the release of EL by CB- + fMLP-stimulated PMNs and significantly decreased it (−8%) when PMNs were stimulated with LPS + TNF-α. No effect of SEVO was observed on EL degranulation by unstimulated and PMA-stimulated PMNs. At 4.6%, SEVO did not change the release of EL either by unstimulated nor stimulated PMNs (Figure 4).

Effect of sevoflurane (SEVO) on the release of EL by unstimulated (UNST), CB + fMLP-, PMA- and LPS + TNF-α-stimulated neutrophils in whole blood. Results are expressed as relative values (%) of the unstimulated control group in air considered as 100%. Data are median (interquartile range, minimum–maximum) of 12 independent experiments carried out in duplicate (n = 24). *p < 0.05 for the difference between air and SEVO-exposed samples within each condition of neutrophil activation.
Discussion
In this in vitro study, we observed that (1) SEVO modulated the release of ROS, MPO, and EL in a direction that was dependant on the nature of compounds used to activate PMNs and (2) clinically relevant concentrations of SEVO showed immunomodulatory potentials through the inhibition of active MPO and EL degranulation from PMNs when stimulated with a combination of the natural compounds LPS and TNF-α.
Several studies assessing the modulating effect of volatile anesthetics on neutrophil functions in vitro have already been published. Unlike other investigators who worked with isolated cells,13,14 we did not separate PMNs from blood in order to avoid procedural activation of cells and with the objective to keep them as close as possible to the physiological environment, except for chemiluminescence assays which required blood dilution in buffer. The concentrations of SEVO used for our investigations (i.e. 2.3% and 4.6%) were representative of that administered in the daily practice of anesthesia with fast and predictable equilibration of anesthetic partial pressure between the gaseous and the liquid phase. 23
The effect of volatile anesthetics on ROS production by isolated human PMNs has been investigated using various techniques.13,14 In this study, we used the highly sensitive L-012 probe that has been demonstrated useful for our purpose by its ability to emit a more sensitive luminescence response than other photometric methods. Furthermore, the L-012 probe has shown to allow detection of ROS produced by neutrophils without isolation of these cells from whole blood. 21 Although other cells from whole blood, particularly monocytes, could also produce ROS, their contribution was probably of minor importance in the experimental conditions of our study. First, in blood of healthy subjects, PMNs are approximately 10-fold more numerous than monocytes. In addition, it has been demonstrated that peripheral blood monocytes are far less reactive 24 and generate several times less ROS than neutrophils after activation with soluble compounds such as those employed in this study.25,26 Furthermore, evidence indicates that stimulation of PMNs leads to a more immediate respiratory burst (within minutes), whereas respiratory burst of monocytes peaks later and lasts for several hours, far beyond the time limit of detection fixed by our experimental protocol. 27
Using artificial stimulation of PMNs with CB + fMLP or PMA, we could detect a production of ROS one or several thousand times higher than that of unstimulated neutrophils and SEVO, particularly at 4.6%, further augmented this production. In a previous study by Nakagawara et al., 13 isoflurane at clinically relevant concentrations similarly increased the respiratory burst of isolated human neutrophils during fMLP challenge. By contrast, Fröhlich et al. 14 showed that sevoflurane, halothane, and enflurane reduced H2O2 production by human neutrophils when stimulated with fMLP although desflurane increased this response. Despite CB + fMLP and PMA are effective to induce respiratory burst, these artificial activators have limited biological relevance because of their non-physiological mechanisms of action. Therefore, an important part of our investigations focused on the effect of SEVO on PMNs activated with a natural stimulus consisting of a combination of LPS and TNF-α. The combination of LPS and TNF-α used in this study is a pertinent in vitro surrogate for the natural activation of neutrophils that could occur during clinical anesthesia. Increased release of LPS and TNF-α has been reported after major surgery 28 and the concentrations administered in whole blood for our in vitro experiments are in the range of those that have been measured in clinical conditions.29,30 This combination of LPS and TNF-α increased ROS production by PMNs but the increase was not significant. This limited effect of LPS and TNF-α on respiratory burst is concordant with other studies and may reflect a low expression of LPS and TNF-α receptors and a poor activation of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase. 31 SEVO at 2.3% or 4.6% did not change the release of ROS by resting PMNs or after activation with LPS and TNF-α.
Beside ROS production, we measured the effect of SEVO on MPO degranulation. MPO is a myeloid cell-specific enzyme, synthesized during the promyelocytic stage. In mature leucocytes, intracellular MPO concentrations are four times higher in neutrophils than in monocytes, while lymphocytes are devoid of MPO. 32 Therefore, measurement of MPO in plasma is considered as an accurate and relatively specific marker of neutrophil activation. 33 To the best of our knowledge, this is the first study to assess the direct effect of a volatile anesthetic on human MPO. For this purpose, we used two complementary immunological techniques such as ELISA and SIEFED in order to discriminate the effect of SEVO on total and active fractions of MPO released by PMNs. Such discrimination is important from a pathophysiological point of view because the active fraction of the enzyme is only responsible for cytotoxic injuries. 34 As previously demonstrated in animal models,19,20 SEVO had a more important impact on the active fraction of MPO than on the total enzyme. Furthermore, the volatile anesthetic showed a different activity depending on which compounds were used to activate PMNs. Although SEVO enhanced MPO release when PMNs were stimulated with artificial compounds, it reduced active MPO degranulation from LPS/TNF-α-stimulated PMNs. Such discordance in neutrophil responses have been attributable to the different levels at which interaction occurs between activators and anesthetics in the cell transduction pathways.14,35,36 Animal models of inflammation suggested reduced MPO levels during volatile anesthetic treatment.10,37 This study provides additional evidence that SEVO directly inhibits MPO release from human PMNs during activation with natural pro-inflammatory compounds. Our data are in line with other ones indicating a reduced reactivity of phagocytes to LPS and TNF-α during volatile anesthetic treatment8,38 which could involve a downregulation of TLR4 and TNF-α receptor expression and signaling.39,40
Beyond MPO, EL is another important cytotoxic enzyme released from primary granules of neutrophils.41,42 Although blood monocytes can also release EL, their contribution to the results observed in this study is probably limited. Indeed, not only monocytes are less numerous than neutrophils in normal blood, but also their whole-cell extracts contain considerably less EL than a comparable number of PMNs. 43 By contrast to MPO, we only measured the release of total EL and not active EL. Measuring active EL could have rise to different results as suggested by studies indicating a discrepancy between EL antigen detected by ELISA and EL enzymatic activity. 44 Nonetheless, the effects of SEVO on EL seemed consistent with its effects on MPO. Although SEVO tends to increase EL release by artificially activated PMNs, it led to a slight reduction of EL degranulation by LPS- and TNF-α-stimulated PMNs. Inhibition of EL may be an additional feature of the anti-inflammatory properties of the volatile anesthetic. Accordingly, Schmid et al. 11 demonstrated lowered EL levels in human blood during sevoflurane exposure for simulated extracorporeal circulation. Schilling et al. 12 showed that volatile anesthesia was more efficient than intravenous anesthesia for reducing alveolar EL and pulmonary inflammation during thoracic surgery.
Although this work was not designed to investigate the mechanisms of SEVO interaction with neutrophils, our results seem concordant with previous mechanistic studies. We showed that sevoflurane reduced neutrophil degranulation when LPS/TNF-α receptors are activated but not when stimuli target intracellular elements such as the cytoskeleton or PKC. Accordingly, Fröhlich et al. 14 demonstrated that halothane, enflurane and sevoflurane decreased neutrophil response to receptor-dependent but not to receptor-independent stimuli. Saad et al. 35 achieved the same results with isoflurane. These authors suggested that volatile anesthetics interfere with the neutrophil signaling transduction machinery at a site located downstream of membrane receptors and upstream of PKC. However, despite recent advances in this field of research, the specific targets of volatile anesthetics in the neutrophil transduction pathway have not yet been fully characterized. 1
The limitations of our study mainly rely on the in vitro design of our experiments. Sampling of blood in EDTA tubes complexes extracellular calcium and deprives PMNs of a pivotal signaling messenger for MPO and EL degranulation. 45 Dilution of blood in PBS to study ROS production led to little change in the partition coefficient of SEVO as compared with whole blood. 23 Furthermore, this study was not designed to assess a dose-dependent effect of SEVO which would have required evaluation of a wide range of anesthetic concentrations. Finally, our methods employed to activate PMNs represent very simplistic models that do not reproduce the far more complex features of neutrophil activation occurring during inflammatory response. Therefore, interpretation of the results observed in this study must be done with caution.
In conclusion, this study establishes that sevoflurane can modulate the release of ROS, MPO, and EL from human neutrophils activated in vitro and that this effect of the volatile anesthetic is stimulus-dependent. The main finding of this work is that clinically relevant concentrations of sevoflurane can reduce active MPO and EL following activation of neutrophils with a combination of natural proinflammatory compounds.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the own financial resources of the CHU de Liège and the University of Liège.