
Abstract
Common variable immunodeficiency disorders (CVIDs) represent a group of primary immunodeficiency diseases characterized by hypogammaglobulinemia and dysfunctional immune response to invading pathogens. Previous studies have indicated that CVID is associated with microbial translocation and systemic myeloid cell activation.
The goal of this study was to determine whether patients with CVID display elevated systemic levels of markers of granulocyte activation and whether the levels are further influenced by intravenous immunoglobulin (IVIg) infusions. The plasma levels of granulocyte activation markers elastase and myeloperoxidase were determined using enzyme-linked immunosorbent assay (ELISA) in 46 CVID patients and 44 healthy controls. All CVID patients were in a stable state with no apparent acute infection. In addition, granulocyte activation markers’ plasma levels in 24 CVID patients were determined prior to and 1 h following IVIg administration. Neutrophil elastase and myeloperoxidase plasma levels were significantly higher in CVID patients than in healthy controls. Systemic elastase levels were further increased following IVIg administration. In vitro stimulation of 13 CVID patients’ whole blood using IVIg in a therapeutically relevant dose for 2 h resulted in a significant increase in plasma elastase levels compared to unstimulated blood. The data presented here indicate that CVID is associated with chronic granulocytic activation which is further exacerbated by administering IVIg. Increased myeloperoxidase and elastase levels may contribute to associated comorbidities in CVID patients.
Introduction
Common variable immunodeficiency disorders (CVIDs) comprise the most frequent symptomatic primary hypogammaglobulinemia characterized by decreased immunoglobulin G (IgG) levels accompanied by decreased immunoglobulin A (IgA) and/or immunoglobulin M (IgM) serum levels and disturbed response to antigenic stimuli. 1 Clinically significant immunodeficiency in CVID patients is manifested by severe respiratory tract infections, diarrhea, and autoimmune disorders. 1
Neutrophil elastase and myeloperoxidase are stored in large quantities in the neutrophils’ azurophilic granules and are released into extracellular space following neutrophil activation. The release of elastase, a serine proteinase with broad substrate specificity, results in damage to host tissue in a wide range of inflammatory conditions. 2 Neutrophil elastase plasma levels were shown to be increased in patients with pneumonia,3,4 inflammatory bowel disease, 5 and preeclampsia. 6 Systemic levels of myeloperoxidase are elevated in patients with acute coronary syndrome, 7 pelvic inflammatory disease, 8 and rheumatic arthritis. 9
CVID was shown to be associated with an altered neutrophil phenotype characterized by decreased expression of surface markers CD15, CD11b, and CD16. 10 CVID patients display elevated systemic cytokine levels associated with granulocyte-macrophage lineage activation. 11 Decreased reactive oxygen species (ROS) production of granulocytes pretreated with toll-like receptor (TLR) 1/2 and TLR 4 agonists after stimulating with N-formylmethionyl-leucyl-phenylalanine (fMLP) was documented, suggesting disturbed granulocytic function in CVID patients. 10 However, no significant difference in granulocytic oxidative burst activity following stimulation with opsonized Escherichia coli or phorbol-myristate-acetate (PMA) was observed in CVID patients compared to healthy donors.12–14
The goal of this study was to determine whether the levels of granulocyte activation markers released from azurophilic granules are altered in patients with CVID and whether they are affected by the infusion of intravenous immunoglobulin (IVIg).
Materials and methods
Study participants
The study was approved by the Medical Ethics Committee of St. Anne’s University Hospital. Informed consent was obtained from all participants prior to inclusion in the study. A total of 46 CVID patients (25 females, 21 males; median age: 45, range: 22–82 years) were recruited. All patients fulfilled the International Consensus Document (ICON) diagnostic criteria for CVID. 1 The control group consisted of 44 healthy donors (23 females, 21 males; median age: 41, range: 19–78 years). The control persons were recruited mainly from the hospital employees and their relatives, not suffering from a known immunodeficiency or autoimmune disease.
Splenomegaly was defined as a spleen length > 11 cm in ultrasonography. Bronchiectasis was determined by high-resolution computed tomography (HRCT). The clinical phenotypes were defined as described in Chapel et al. 15 B-cell phenotypes were determined according to Wehr et al. 16 (EUROclass).
Plasma neutrophil elastase and myeloperoxidase determination
The blood was collected in an acute infection–free period. In 24 patients on IVIg treatment (aged 22–82 years), elastase and myeloperoxidase plasma levels were determined prior to and 1 h after the completion of IVIg infusion. 14
Human elastase and myeloperoxidase plasma levels were determined by enzyme-linked immunosorbent assay (ELISA), according to the manufacturer’s protocol (Hycult Biotech, Plymouth Meeting, PA, USA). The samples were collected into ethylenediaminetetraacetic acid (EDTA)-containing tubes (S-Monovette; Sarstedt, Nümbrecht, Germany) and placed on ice. Within 20 min, the plasma was separated by centrifugation for 15 min at 1500 g at 4°C. Without disturbing the buffy coat, the plasma was transferred into a polypropylene tube and centrifuged again for 15 min at 1500 g at 4°C. All plasma samples were stored at −20°C.
In vitro stimulation of blood with IVIg
A total of 13 CVID patients’ whole blood was collected into three heparinized tubes (S-Monovette) at room temperature. Plasma from the first tube was collected as described above. The second tube was incubated in a water bath at 37°C with gentle mixing every 30 min; after 2 h, plasma was collected. In the third tube, 10% IVIg at a dose of 5.7 mg/mL of heparinized blood (IVIg concentration adequate to the concentration in blood after infusion of 400 mg IgG/kg) was added. The subsequent procedure was identical to the one in tube number 2. Plasma elastase levels were determined as described above.
Statistical analysis
The results were analyzed using the Mann–Whitney rank-sum test, Wilcoxon signed-rank test, and analysis of variance (ANOVA) test as appropriate using Stata and GraphPad Prism 5 statistical packages. The results are presented as median (5th–95th centile).
Results
Plasma elastase and myeloperoxidase levels
Basic clinical and laboratory characteristics of the CVID patients are shown in Table 1. The absolute number of neutrophils was higher in CVID patients than that in the healthy controls (3.4 × 109/L (1.8–6.8) vs 2.7 × 109/L (1.8–4.4); P = 0.02). The CVID patients displayed significantly higher neutrophil elastase (100.5 µg/L; (55.8–184.0) vs 66.9 µg/L (42.2–99.6); P < 0.001) and myeloperoxidase (28.2 µg/L (15.2–56.6) vs 14.1 µg/L (8.4–19.7); P < 0.001; analyzed by Mann–Whitney test) plasma levels than the healthy controls (Figure 1). The difference remained significant after the CVID patients with C-reactive protein (CRP) higher than 10 mg/L (n = 7) were excluded from the analysis (elastase: 89.2 µg/L (54.8–162.1); P = 0.04; myeloperoxidase: 27.5 µg/L (12.1–55.9); P < 0.001). No significant differences were observed between patients treated with IVIg (n = 25) versus subcutaneous immunoglobulin (SCIg; n = 21) (P = 0.2 for elastase and P = 0.1 for myeloperoxidase). Compared to healthy controls, the levels of granulocytic markers were significantly higher in both IVIg (elastase: 110.4 µg/L (55.8–162.1); myeloperoxidase: 26.5 µg/L (12.1–44.7)) and SCIg (elastase: 83.1 µg/L (56.5–191.9); myeloperoxidase: 29.5 µg/L (17.1–62.5)) recipients (all P < 0.001; analyzed by Mann–Whitney test).
Clinical and laboratory characteristics of the patients at the time of the investigation.

IgG: immunoglobulin G; IgA: immunoglobulin A; IgM: immunoglobulin M; F: female; M: male; IVIg: intravenous immunoglobulin; SCIg: subcutaneous immunoglobulin; CRP: C-reactive protein; N: no disease-related complications; E: unexplained enteropathy; L: polyclonal lymphocytic infiltration; A: autoimmunity; ND: not detected.
Serum immunoglobulin levels were determined before IVIg infusion or during routine follow-up in SCIg-treated patients.
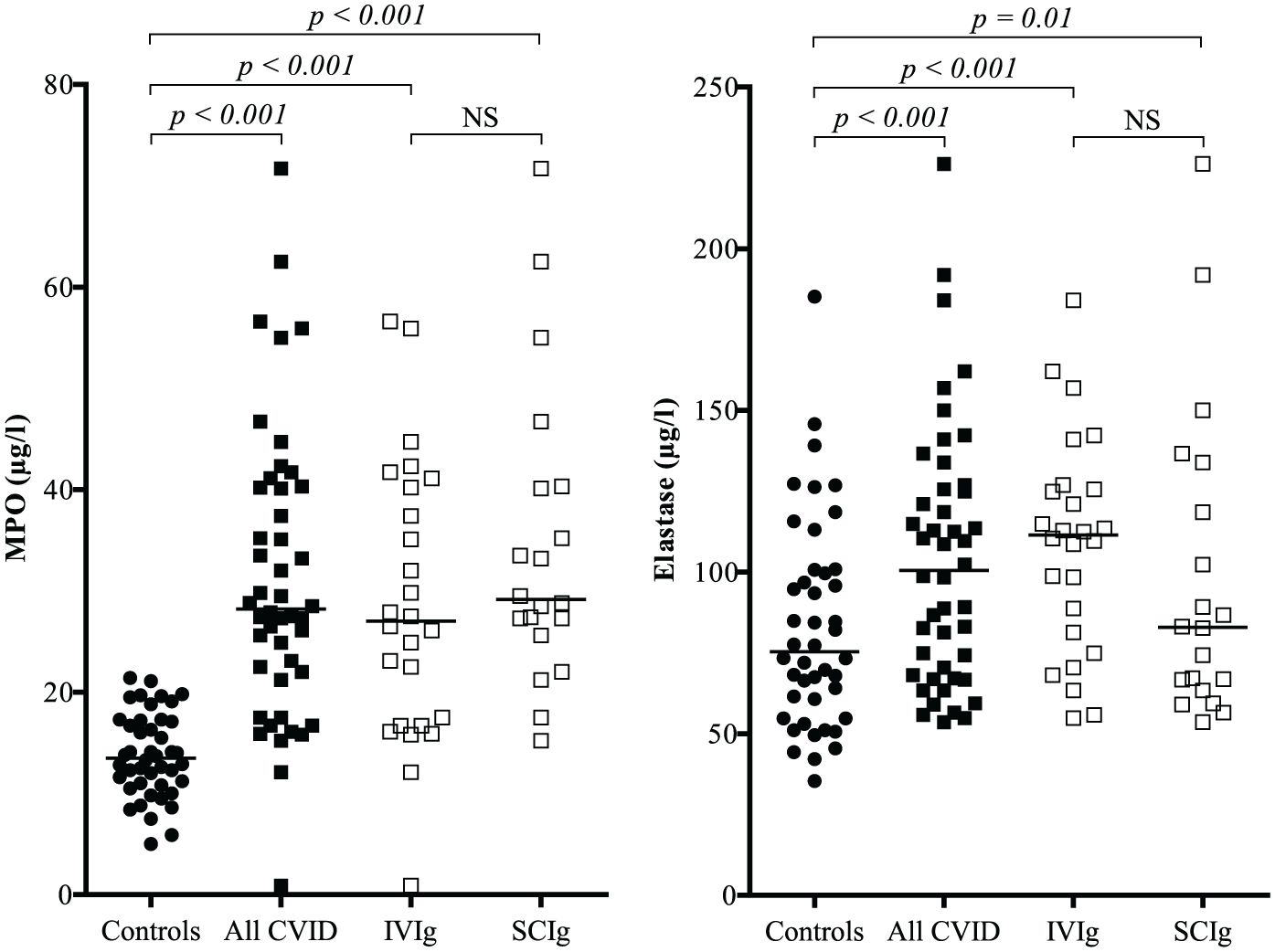
Plasma myeloperoxidase (MPO) and elastase levels in all CVID patients, patients on intravenous immunoglobulin (IVIg) and subcutaneous immunoglobulin (SCIg) treatments and healthy control donors.
Significantly elevated neutrophil elastase and myeloperoxidase plasma levels were observed in patients with splenomegaly (n = 21) than patients without splenomegaly (n = 24) (elastase: 114.9 µg/L (54.8–162.1) vs 76.4 µg/L (56.5–156.9); P = 0.005; myeloperoxidase: 35.2 µg/L (12.1–56.6) vs 26.5 µg/L (15.8–55); P = 0.02). No significant differences were observed between patients with (n = 19) and without (n = 26) bronchiectasis.
Using clinical phenotype classification, 15 patients classified as “no disease-related complications” (n = 28) displayed a lower plasma myeloperoxidase concentration (26.9 µg/L (15.2–55.9)) than patients with other complications of CVID (n = 18) (40.1 µg/L (12.1–71.7); P = 0.007). Patients with enteropathy (n = 8) had higher myeloperoxidase levels (42.9 µg/L (12.1–71.7)) than patients without this complication (n = 38) (27.3 µg/L (15.2–55.9); P = 0.006). No significant differences were observed between patients with (n = 7) and without (n = 39) lymphocytic infiltration, and with (n = 9) and without (n = 37) autoimmune disorders. No patient suffered from lymphoid malignancy. No significant differences were observed in plasma elastase levels.
The ANOVA test did not show any significant difference in elastase (P = 0.35) and myeloperoxidase (P = 0.06) plasma levels comparing patient groups defined according to EUROclass. 16
Effect of administering IVIg on plasma neutrophil elastase and myeloperoxidase levels
Administering IVIg resulted in a significant increase in neutrophil elastase plasma levels 1 h after treatment (P = 0.001; Wilcoxon signed-rank test; Figure 2). A trend toward increased myeloperoxidase levels was observed; however, the effect did not reach statistical significance (P = 0.17). No adverse reaction to infusion was observed in any of the participants.
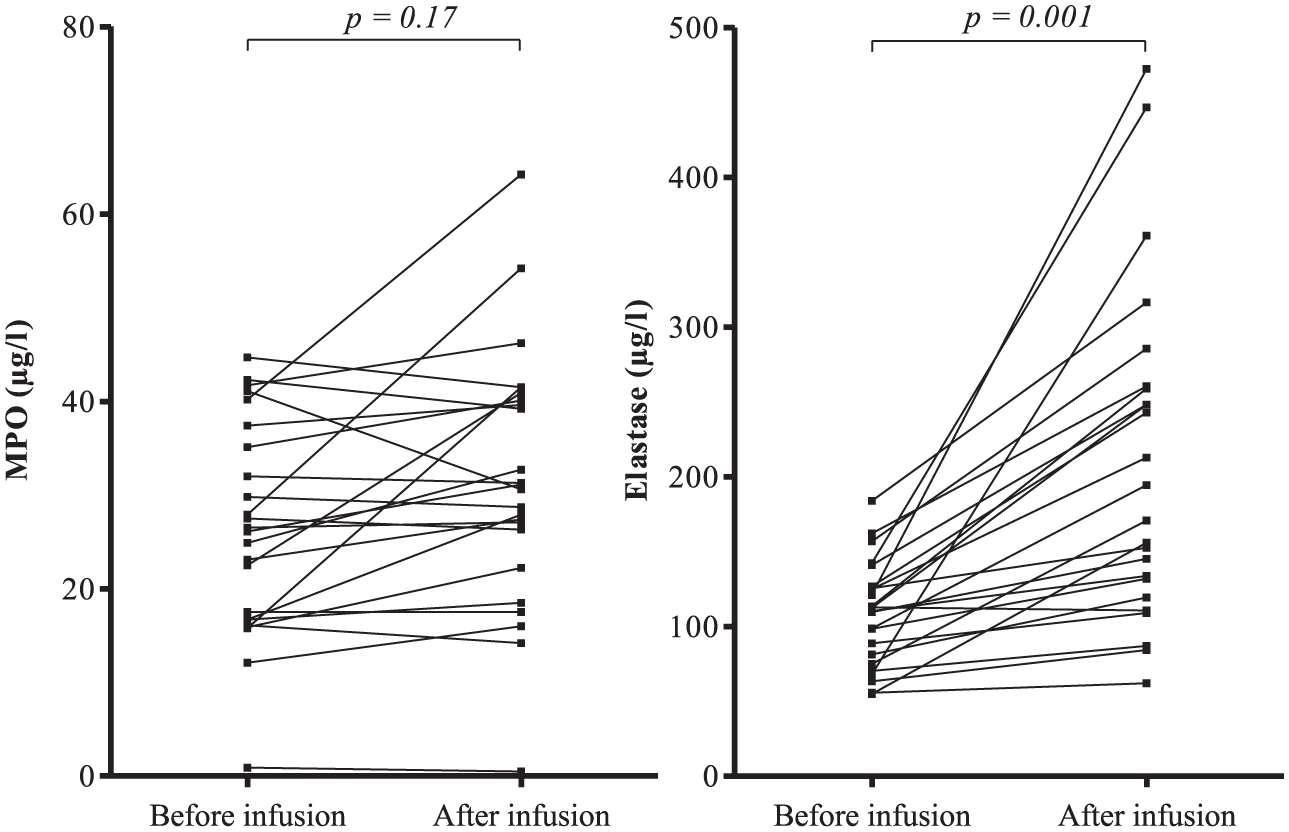
Plasma myeloperoxidase (MPO) and elastase levels before and 1 h after intravenous immunoglobulin infusion in CVID patients.
The in vitro effect of IVIg on elastase release
To evaluate the potential activation effect of IVIg on CVID neutrophils, whole heparinized blood was stimulated with IVIg. As shown in Figure 3, 2-h cultivation of patients’ blood at 37°C leads to an increase in the elastase concentration in plasma by 74.5% (37.2%–273.3%). Stimulating whole blood from CVID patients with IVIg leads to an increase in plasma elastase levels by 104.0% (56.2%–301.3%). The difference between the increase with and without IVIg was statistically significant (P = 0.017; Wilcoxon signed-rank test; Figure 3).

Plasma elastse concentration levels of 13 CVID patients after in vitro stimulation with IVIg.
Discussion
The presented data, together with previously published observations, are indicative of an ongoing chronic granulocytic activation in CVID patients. The cause of activation of granulocytes in CVID remains unclear. However, the data are consistent with a potential role of translocation of microbial products from the intestinal lumen into the systemic circulation. Microbial translocation is observed in various pathological conditions including HIV-1 infection, inflammatory bowel disease, and hepatitis B and C infections.17,18 Bacterial and fungal products’ translocation results in systemic immune activation. 17 We and others have previously presented evidence of chronic microbial translocation in CVID patients.19–21. Furthermore, CVID patients display an altered cytokine signature profile consistent with an ongoing activation of cells of monocytic and granulocytic lineages. 11
In our study, we observed increased serum elastase and myeloperoxidase levels in patients with splenomegaly compared to patients without splenomegaly. Except for the observation showing higher serum myeloperoxidase levels in patients with splenomegaly and liver cirrhosis compared to patients without splenomegaly, 22 to our knowledge, no association of splenomegaly with myeloperoxidase and elastase levels has been previously reported. However, splenomegaly in CVID is frequently associated with other complications, for example, cytopenias, hepatomegaly granuloma, enteropathy, autoimmunity, or bronchiectasis.15,23 Although we did not observe elevated levels of both granulocyte activation plasma markers in subjects with bronchiectasis, autoimmunity, or lymphatic infiltration in our cohort, the myeloperoxidase levels were lower in patients in the “no disease-related conditions” group 15 than the group with disease-related conditions and increased in patients with enteropathy.
Elevated systemic elastase and myeloperoxidase levels may significantly contribute to the pathogenesis of CVID complications. Neutrophil elastase is involved in destroying the extra-cellular matrix in chronic obstructive pulmonary disease 24 and plays a pathogenic role in forming bronchiectasis. 25 Neutrophil-derived myeloperoxidase is involved in inducing oxidative stress and producing proinflammatory cytokines including interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF)-α. 24 Therapeutic approaches targeting granulocytic enzymes or curbing their proinflammatory properties may be beneficial to CVID patients.
Here, we report that the administration of IVIg resulted in elevated systemic concentrations of neutrophil elastase and a trend toward an increased concentration of myeloperoxidase at 1 h following the treatment. Limited data are available regarding the effect of IVIg on polymorphonuclear neutrophil (PMN) degranulation upon IVIg stimulation in vitro. Van Mirre et al. 26 observed decreased elastase release in isolated granulocytes stimulated by aggregated IgG by adding monomeric IgG (obtained from IVIg). This effect was not observed when PMNs were activated by fMLP/cytochalasin B; monomeric IgG alone did not stimulate PMN, suggesting that monomeric IgG acts as a low-affinity FcγR antagonist. On the other hand, in the whole blood, under the in vitro conditions more similar to our experiments, Teeling et al. 27 showed that in vitro exposure of whole fresh blood from healthy donors to commercially available IVIg preparations at therapeutically relevant levels resulted in neutrophil degranulation and a release of elastase and lactoferrin. This effect was mainly mediated by the dimeric and polymeric fractions of the IVIg derivate and was dependent on FcγRII. 27 Currently available commercial preparations of IVIg contain less than 3% of polymeric IgG. 28 Whether or not neutrophil activation by IVIg depends on the presence of polymeric IgG warrants further investigation.
Other studies support potential activation of granulocytes by IVIg. Higurashi et al. 29 showed that IVIg administration increased the production of ROS from TNF-α-primed PMN in a process dependent on both the Fab and Fc domains of IgG and interaction with FcγRIII. Similarly, using whole-blood conditions, Casulli et al. 30 showed that IVIg at low concentrations induced PMN activation indicated by decreased CD62L and increased CD11b surface expression, enhancement of oxidative burst, and prolonged cell survival. In contrast, at higher concentrations, IVIg inhibited lipopolysaccharide (LPS)-induced CD11b degranulation and priming of oxidative burst. 30
Limited information is available regarding the effect of IVIg administration on neutrophils in vivo. A significantly reduced capacity for PMA-induced ROS production by PMN obtained from CVID patients after administering IVIg was observed. 14 No effect on CD11b, CD16, and sialic acid–binding immunoglobulin-like lectin (Singlec) 9 expression on PMNs or ROS production induced by opsonized E. coli was documented in this study. 14
Compared to our report, Prezzo et al. 13 recently observed decreased serum elastase levels in patients with CVID treated by IVIg compared to healthy controls; the levels decreased 1 h after IVIg infusion. The results are not consistent with our study. The differences may be influenced by various factors, including the general clinical health of the investigated patients, the immunoglobulin brand used (stabilizers present in different brands), and others. A probable explanation may also be the variances in the handling of patients’ plasma. Compared to our study, Prezzo et al. 13 used heparinized plasma. Significant differences in sampling conditions when determining the plasma elastase levels were previously demonstrated. 31 Our observation of increased plasma elastase levels after IVIg treatment is supported by the fact that previous studies showed an increase in proinflammatory cytokines after IVIg infusions, including neutrophil-activating cytokines TNF-α, IL-6, and IL-8.32,33 The observation of an increase in plasma elastase levels following IVIg infusion is supported by other reports of in vitro elastase release 27 and general granulocyte activation29,30 after in vitro stimulation of whole blood by IVIg.
In summary, the data presented here indicate chronic granulocyte activation in CVID patients, independent of concurrent infection and other forms of disease exacerbation. Administering IVIg further enhances granulocytic degranulation in CVID patients. Pharmacologically targeting granulocytic activation and degranulation may represent a novel approach to CVID treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. L. obtained consultation fees from Shire Plc and Octapharma AG. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the Czech Health Research Council (No. 15-28732A).