
Abstract
Background
Peripheral neutrophil-lymphocyte ratio (NLR), reflecting immune-inflammation status, shows great potential for tumor progression and outcome. Pre-treatment NLR does not fully reflect the immune-inflammatory response to treatment. This study aimed to introduce the NLR trend as a new indicator and to investigate its prognostic value in patients with nasopharyngeal carcinoma receiving radiotherapy.
Methods
This retrospective study evaluated patients with nasopharyngeal carcinoma treated with radiotherapy. The NLR trend value was calculated from the fitted line gradient via the NLRs before, during (at least once), and after each patient's first radiotherapy. The Kaplan–Meier curve and log-rank test were used to calculate and compare survival outcomes of different pretreatment NLRs and NLR trends for progression-free survival, locoregional recurrence-free survival (LRFS), and overall survival at 3 and 5 years. Multivariate Cox regression analyses were performed to assess the association between the NLR trend plus 3- and 5-year overall survival.
Results
The study included 528 patients. A lower NLR trend predicted worse progression-free survival, LRFS, plus 3- and 5-year overall survival. Multivariate Cox regression analysis showed that the NLR trend independently predicted 3- and 5-year overall survival. Sub-group analysis showed that the prognosis of patients with a low pretreatment NLR and a high NLR trend were superior to those of other groups.
Conclusion
The NLR trend independently predicted the prognosis of patients with nasopharyngeal carcinoma receiving radiotherapy. The NLR trend and the pretreatment NLR combination is more precise than pretreatment NLR in predicting prognosis. A high NLR trend may be evidence of a positive immune response to radiotherapy in patients with nasopharyngeal carcinoma.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is an endemic disease in China.1,2 Salted fish consumption, cigarette smoking, alcohol intake, and nitrite exposure are associated with an increased NPC risk.3,4 It is challenging to treat NPC with surgery because of its anatomic location and local aggression characteristics; 5 thus, radiotherapy (RT) with or without chemotherapy is the first-line treatment. 6 NPC's current survival prognostic and therapeutic evidence relies on the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC) tumor node metastasis (TNM) stage. 7
NPC prognosis has improved dramatically due to standard treatment strategies for patients based on the staging system. 8 However, locally advanced NPC prognosis is clinically heterogeneous and characterized by increased local recurrence and distant metastasis.9,10 This is because NPC cells have different biological behaviors, immune system levels, and chemoradiotherapy sensitivity. The clinical use of quantitative assessment of circulating Epstein–Barr virus DNA as an NPC surrogate biomarker increases population screening, prognosis, and disease surveillance. 1 However, it is expensive and has great inter-laboratory variability. Thus, identifying novel biomarkers for NPC prognosis and precise treatment stratification is still important. 11
Increasing evidence suggests that cancer-associated immune inflammation is a key determinant of outcomes. Rearrangements of hematological components, including neutrophils, lymphocytes, and monocytes, often manifest in the host immune system's tumor-related response. An abnormal white blood cell count is often the first motivation for cancer screening. The neutrophil-to-lymphocyte ratio (NLR) is generally believed to be a biomarker of the immune-inflammatory response to cancer.12,14 Elevated NLR has been associated with poor prognosis in many malignancies. 15 A correlation between an elevated NLR and a worse prognosis has also been found in NPC.16,17 NLR may be clinically useful for risk stratification, depending on its combination with other information in particular clinical scenarios. 18 However, pretreatment NLR alone cannot reflect the immune-inflammation status during therapy. In these cases, radiation oncologists cannot provide individual strategies based on the different responses to treatment in patients with NPC.
Therefore, we report a novel index of cancer-associated immune inflammation, called the NLR trend, from dynamically monitored NLR during therapy. This study aimed to investigate the prognostic value of the NLR trend in patients with NPC treated with conventional segmented RT alone and to compare NLR trend accuracy with pretreatment NLR and other common factors for NPC survival prediction.
Materials and methods
Patients
The study retrospectively investigated all newly diagnosed patients with NPC who underwent two-dimensional conventional radiotherapy (2DCRT) without chemotherapy between January 1992 and December 2005 at the Head and Neck Department of RT at the Hunan Cancer Hospital. The inclusion criteria were: (a) histologically confirmed NPC; (b) no malignancy history; (c) not on chronic steroid or immunomodulators; (d) stage I–IV disease (restaged according to the Chinese 2008 staging system 19 ); (e) patients without hematological disease, infection, inflammatory conditions, or hyperpyrexia, previous treatment (such as chemotherapy or RT) for NPC; (f) patients with complete blood count (CBC) tests obtained before, during (at least once), and after (BDA) first RT; and (g) patients with complete follow-up data. Eligible patients’ clinical features, including sex, age, Karnofsky Performance Scale, 20 AJCC/UICC 1997 stage, 21 and World Health Organization (WHO) histologic type, were acquired from medical records. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Hunan Cancer Hospital Ethics Board and hospital review committee. Informed consent was obtained from all the participants. This article is presented in accordance with the REMARK Reporting Guidelines (Supplemental Table 1). 22
Treatment
All patients who received 2DCRT without chemotherapy were immobilized in the supine position using a thermoplastic mask. Two lateral-opposing faciocervical portals were used to cover the nasopharynx and upper neck in one volume, followed by a shrinking-field technique to limit spinal cord exposure. The neck was treated with an anterior cervical field using a laryngeal block. Total radiation with doses 66–74 Gy, (2 Gy per fraction) was delivered to the primary tumor, 60–64 Gy to the other areas involved in the neck, and 50 Gy to the uninvolved areas. RT was administered 5 days per week in daily fractions of 2 Gy.
A boost portal was performed, if necessary, during the last one-third of the treatment course. A booster dose (8–12 Gy per 4–6 fractions) was delivered to the skull base of patients with NPC involving the skull base and intracranial extension. The radiation energies used megavoltage photons (6 or 8 MV) and electrons.
Hematological tests
Blood samples (2 mL) from the patients for neutrophil and lymphocyte counts were obtained before breakfast CBCs were detected using a Sysmex XE-5000 automated hematology analyzer (Sysmex, Kobe, Japan). The tests were performed at least once before RT (usually 1 day before RT), once a week during RT, and once after RT (usually 1 week after RT).
NLR trend calculation
The NLR was calculated as the absolute neutrophil count divided by the absolute lymphocyte count. Each patient's NLR trend value equaled the gradient (slope) value calculated from a linear model on the NLRs’ BDA scatter plot.
Outcome and follow-up
Overall survival (OS) was selected as the primary endpoint, while progression-free survival (PFS) and locoregional recurrence-free survival (LRFS) were secondary endpoints. All terms were defined according to the NCI Dictionary of Cancer Terms (https://www.cancer.gov/publications/dictionaries/cancer-terms). The patients were followed-up every 3 months for the first 2 years, every 6 months for 3–5 years, and annually after 5 years. Follow-up time was calculated as the first day of therapy to either the day of the last follow-up or death.
Statistical analysis
The numerical variables were calculated as median and range, while categorical variables were presented as numbers and percentages. The pretreatment NLR and NLR trend cut-off values for survival prediction were determined using the receiver operating characteristic (ROC) curve (Youden index).
The Kaplan–Meier estimate and log-rank test were used to calculate and compare survival outcomes among the different groups of pretreatment NLR or the NLR trend via PFS, LRFS, and 3- and 5-year OS. Multivariate Cox regression was used to determine the independent association of the NLR trend with 3- and 5-year OS after adjusting for other confounding prognostic factors.
The survival prediction accuracy of the pretreatment NLR and the NLR trend was compared using the area under the curve (AUC) of the ROC curve. According to the cut-off values of pretreatment NLR and the NLR trend for OS prediction, the patients were divided into four sub-groups: (a) low pretreatment NLR and low NLR trend; (b) low pretreatment NLR and high NLR trend; (c) high pretreatment NLR and low NLR trend; and (d) high pretreatment NLR and high NLR trend. Kaplan–Meier curves of 3- and 5-year OS and Cox regression analysis stratified according to pretreatment NLR and the NLR trend subgroups were illustrated. They were calculated to compare the subgroups’ prognoses and confirm whether pretreatment NLR and NLR trend combinations could accurately predict OS. All data were analyzed using MedCalc statistical software (version 19.0; MedCalc Software, Mariakerke, Belgium) and R Project for Statistical Computing (4.0, https://cran.r-project.org). All tests were two-sided, and statistical significance was set at P < 0.05.
Results
Patient characteristics
A total of 528 patients with a median age of 46 years (range 18–77 years) who met the inclusion criteria were included in this study. The characteristics of patients with NPC are shown in Supplemental Table 2; 393 (74.4%) patients were males, and 135 (25.6%) were females, with a sex ratio of 2.9:1. Most patients had stage III or IV NPC (76.3%) and 210 (39.8%) received additional boost therapy. Within a median follow-up time of 76.4 months (range, 1–219 months), 316 (59.8%) patients died. The remaining 212 patients (40.2%) were either alive or lost to follow-up. The 3- and 5-year OS rates were 78.4% and 63.6%, respectively.
Pre-treatment NLR for survival analysis
The median pretreatment NLR was 2.81 (0.08–1458.33). The pretreatment NLR cut-off values for predicting PFS, LRFS, 3-year OS, and 5-year OS were 5.00, 2.53, 3.39, and 3.50, respectively. Patients were divided according to the cut-off values into low and high NLR groups. No significant difference was observed in PFS between the two groups. The LRFS, 3- and 5-year OS rates were significantly higher in patients with low NLR than in those with high NLR (Table 1).
Pre-treatment NLR cut-off values and prediction of survival analysis.
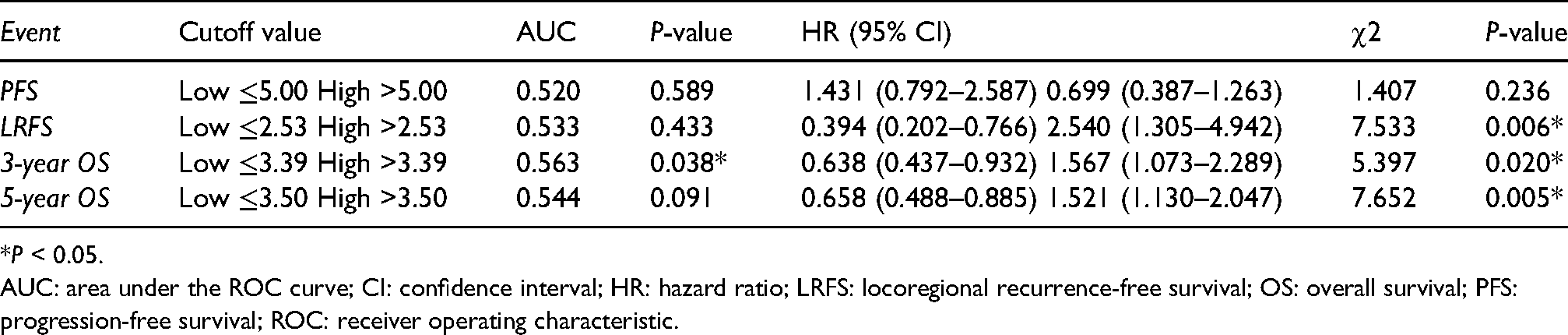
*P < 0.05.
AUC: area under the ROC curve; CI: confidence interval; HR: hazard ratio; LRFS: locoregional recurrence-free survival; OS: overall survival; PFS: progression-free survival; ROC: receiver operating characteristic.
NLR trend for survival analysis
The median NLR trend value was 0.81 (range 10.59–155.73). The NLR trend cutoff values to predict PFS and LRFS were 0.37 and 0.35, respectively (Supplemental Figure 1). The patients were divided into low- and high-trend groups according to the cut-off values. The PFS (hazard ratio (HR) 2.42; 95% confidence interval (CI) [1.45 to 4.04]; P = 0.000; Supplemental Figure 2(a)) and LRFS (HR 3.15; 95%CI [1.55 to 6.40]; P = 0.001; Supplemental Figure 2(b)) rates were significantly higher in the high NLR trend group than in the low NLR trend group.
The NLR trend cut-off values to predict 3-year OS and 5-year OS were 0.63 (P = 0.032, Supplemental Figure 3(a)) and 0.68 (Supplemental Figure 4(a)), respectively. The patients in the low-trend group had a lower 3-year OS than the patients in the high-trend group (HR 1.68; 95%CI [1.16 to 2.44]; P = 0.006; Supplemental Figure 3(b)), and a similar result was also observed in the 5-year OS of the two groups (HR 1.41; 95%CI [1.06 to 1.87]; P = 0.019; Supplemental Figure 4(b)).
Multivariate Cox regression analysis
Multivariate analysis showed that pretreatment NLR, NLR trend, age, T-stage, N-stage, and M-stage were independent risk factors for both 3- and 5-year OS, while AJCC/UICC stage and WHO type were not associated with 3- or 5-year OS (Figures 1 and 2).
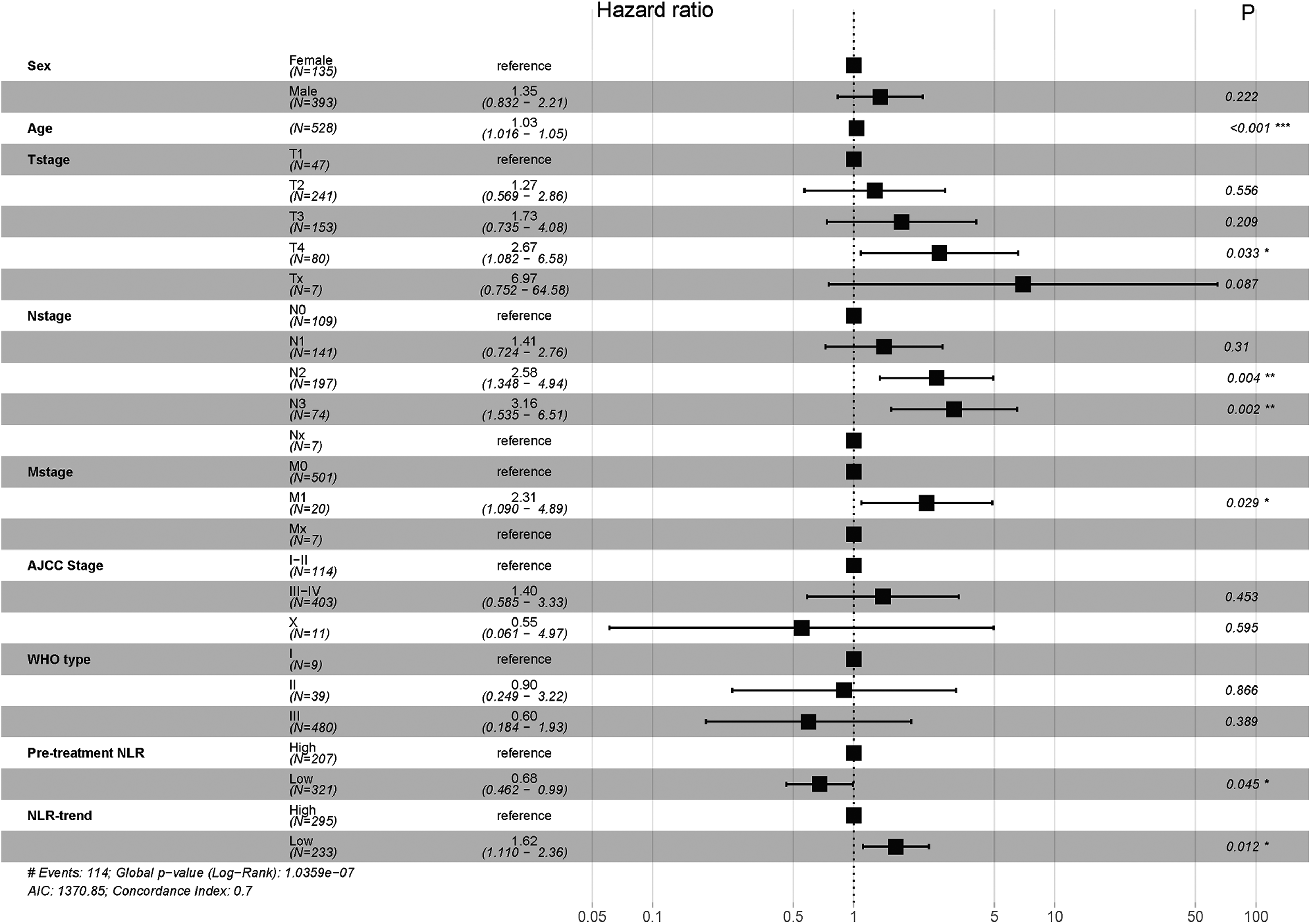
Forrest plot of multivariate analysis for 3-year overall survival of pretreatment NLR and NLR-trend determined by cut-off values for patients.
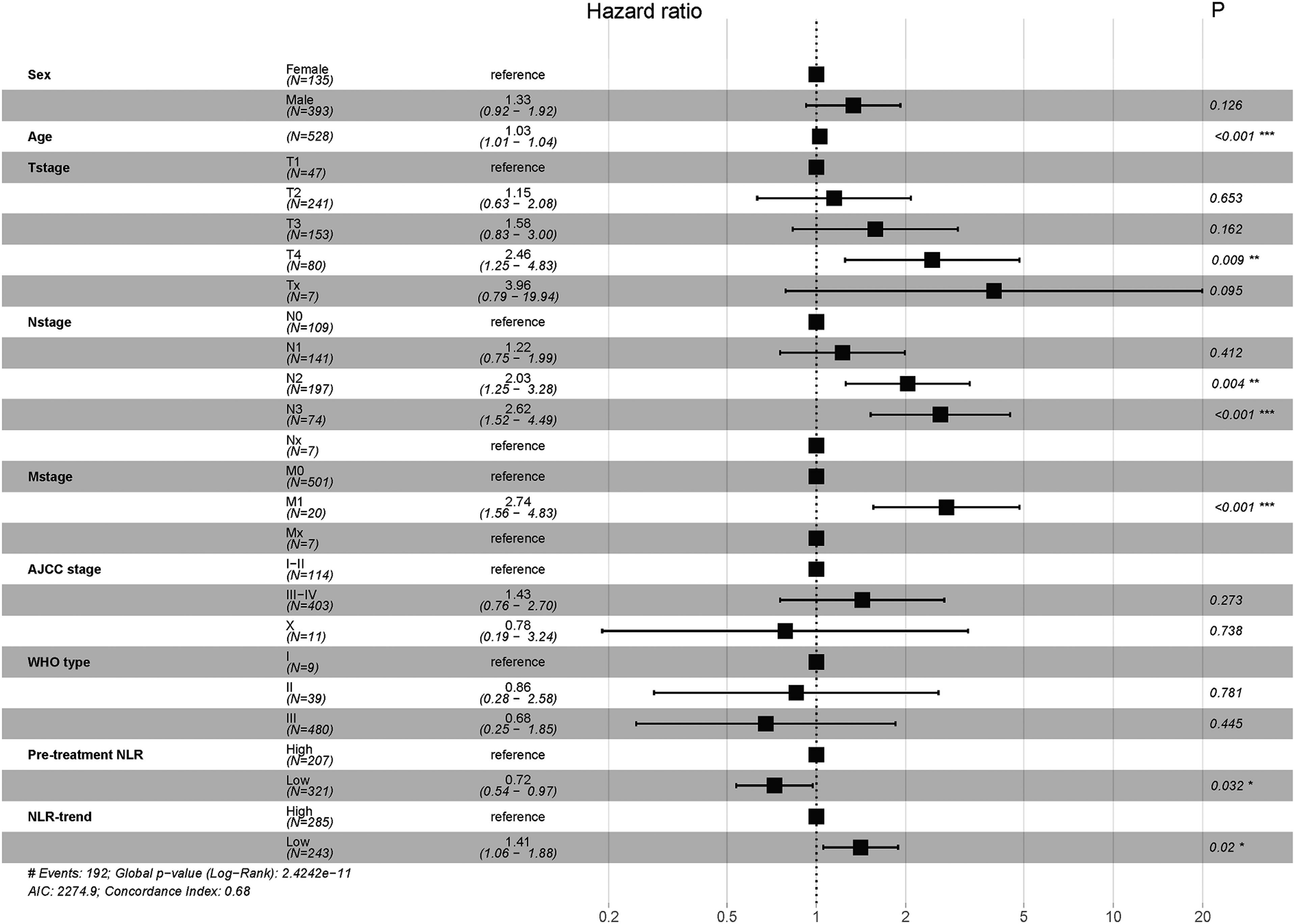
Forrest plot of multivariate analysis for 5-year overall survival of pretreatment NLR and NLR-trend determined by cut-off values for patients.
Comparison of ROC curves for survival prediction
The AUC from ROC curves of the NLR trend and NLR for predicting PFS, LRFS 3-year OS, and 5-year OS were 0.56 (95%CI 0.52–0.60) versus 0.52 (95%CI 0.48–0.56), 0.60 (95%CI 0.56–0.64) versus 0.53 (95%CI 0.49–0.58), 0.57 (95%CI 0.52–0.61) versus 0.56 (95%CI 0.52–0.60) and 0.55 (95%CI 0.50–0.59) versus 0.54 (95%CI 0.50–0.59), respectively (Supplemental Figure 5). There was no statistically significant difference between the NLR trend and NLR for all predictions (P > 0.05).
Sub-group analysis
The patients with 3- and 5-year OS in the four subgroups differed significantly, and the prognosis of those with low pretreatment NLR and high NLR trend were superior to that in the other three groups (Figures 3(a) and (d)). In patients with low pretreatment NLR, a low NLR trend was associated with a lower 3-year OS (P = 0.008, Figure 3(b)), while no significant difference was found between the high and low NLR trends in high pretreatment NLR patients (Figure 3(c)). A low NLR trend predicted a lower 5-year OS in patients with a low pretreatment NLR, although the difference was not statistically significant (P = 0.051, Figure 3(e)). The Cox regression analysis of 3-year and 5-year OS also showed that the prognosis of patients with low pretreatment NLR and a high NLR trend improved significantly (Figure 4).
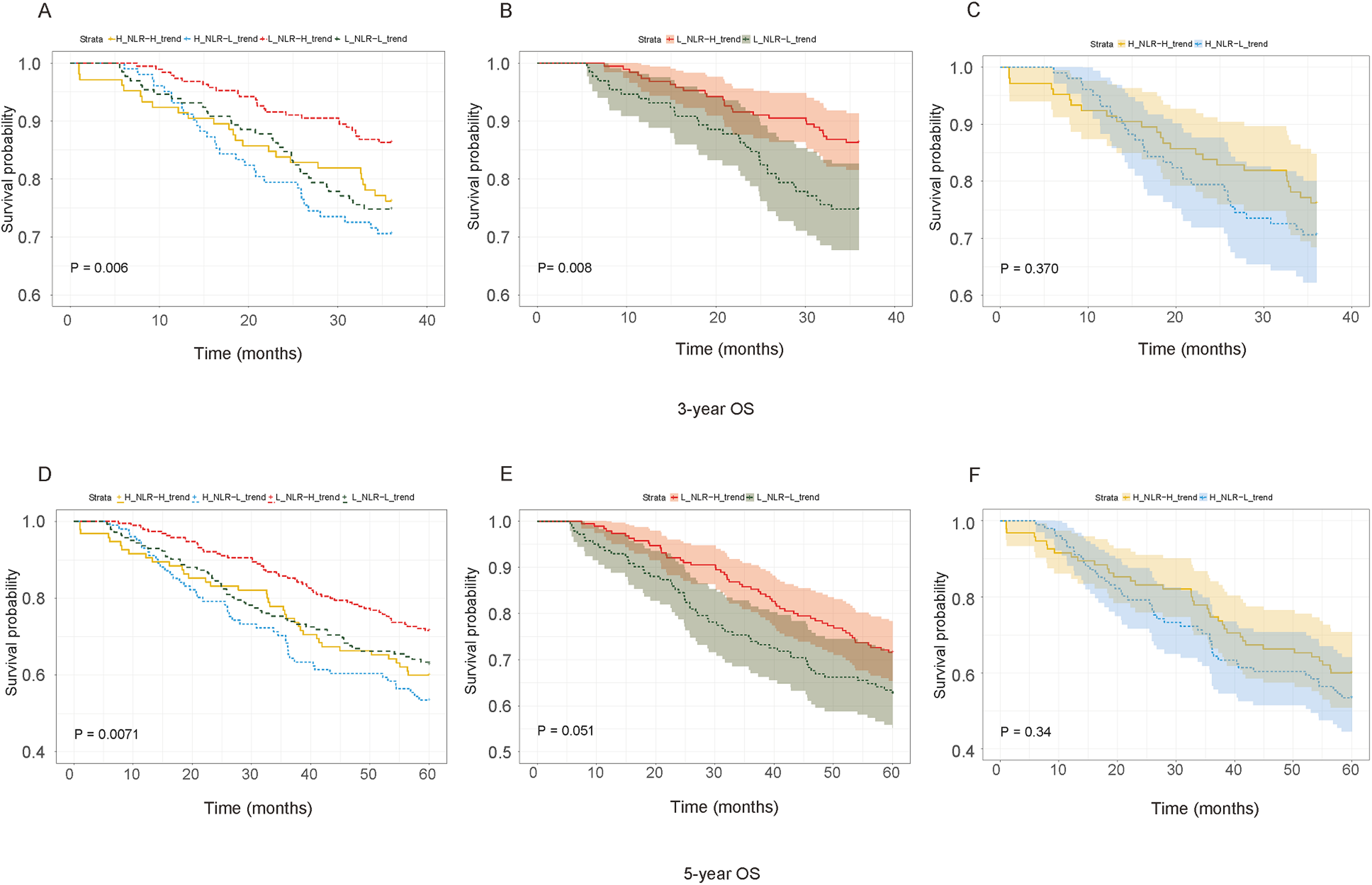
Kaplan–Meier 3-year overall survival curve stratified according to pretreatment NLR and NLR-trend for: (a) comparison between low pretreatment NLR and low NLR-trend, low pretreatment NLR and high NLR-trend, high pretreatment NLR and low NLR-trend and high pretreatment NLR and high NLR-trend; (b) the comparison between high NLR-trend and low NLR-trend of low pretreatment NLR patients; (c) the comparison between high NLR-trend and low NLR-trend of high pretreatment NLR patients. Kaplan–Meier 5-year overall survival curve stratified according to pretreatment NLR and NLR-trend for: (d) comparison between low pretreatment NLR and low NLR-trend, low pretreatment NLR and high NLR-trend, high pretreatment NLR and low NLR-trend and high pretreatment NLR and high NLR-trend; (e) the comparison between high NLR-trend and low NLR-trend of low pretreatment NLR patients; (f) the comparison between high NLR-trend and low NLR-trend of high pretreatment NLR patients.
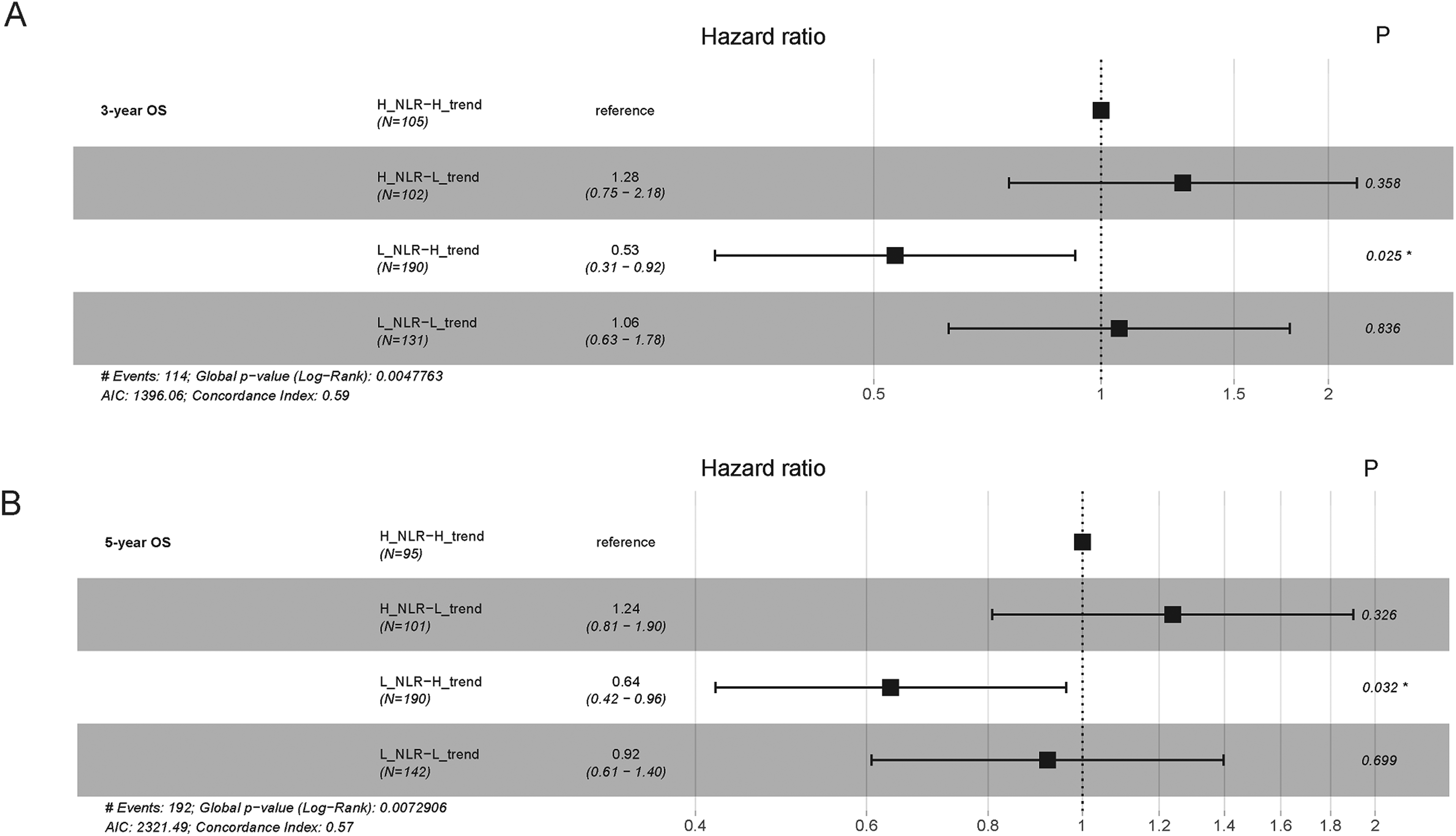
Forrest plot of sub-group Cox regression analysis for 3-year overall survival (a) and 5-year overall survival (b) stratified according to pretreatment NLR and NLR-trend.
Discussion
This study targeted patients who only received radiotherapy to exclude the effect of chemotherapy on NLR, and the NLR trend was calculated from dynamically monitored NLRs during RT. A low NLR trend was found to be a poor predictor of PFS, LRFS, 3-year OS, and 5-year OS in patients with NPC who underwent RT. Multivariate analysis revealed that the NLR trend was an independent prognostic factor. Similarly, Li et al. 23 found that the delta-NLR obtained from pre- and posttreatment NLRs was an independent prognostic factor for OS in early-stage colon cancer; patients with increased delta-NLR had a favorable clinical outcome. Peng et al. 24 concluded that an increased NLR helped predict worse OS and recurrence-free survival in patients with small hepatocellular carcinoma who underwent curative resection. NLR change prognostic values are dissimilar in different cancers, and exploration of the reasons behind this are interesting.
In recent years, evidence has shown that cancer-associated inflammation is a key determinant of various tumors’ prognosis and therapeutic decisions.25,26 The correlation between an elevated NLR and poor prognosis is based on immune-inflammatory theories. Inflammation represents the host immune response to malignancy with respect to neutrophil and lymphocyte activities on tumor cell invasion into the peripheral blood. Neutrophils and related cytokines are the main mediators of angiogenesis and growth in circulating tumors. 27 A decrease in lymphocyte count usually indicates lymphocyte-mediated anti-tumor immunity inhibition and poor clinical outcomes.28,29 However, pretreatment NLR prognostic ability has not been conclusively determined for NPC. Recently, a pooled study of two randomized controlled trials revealed the negative result that a high pretreatment NLR was not associated with OS, PFS, and DMFS. 30 Similar results were found in our study, which showed that pretreatment NLR was not significantly correlated with PFS. This negative result can be attributed to several reasons. First, the NLR cut-off value for prediction was confirmed using different methods, such as the median value or ROC curve. 31 Second, the evidence was mostly from retrospective series with sample and design biases. Third, collecting NLR data only once before treatment can be affected by many factors, including age, environment, and immune condition, resulting in heterogeneous results. The NLR trend in our study was a neutrophil-lymphocyte change type that reflects the immune-inflammatory response to treatment. Although there was no statistical significance between the NLR trend and NLR predictions, the NLR trend is slightly better. Subgroup analysis in the present study revealed that the NLR trend and NLR combination were more precise in predicting survival. Even though a low pretreatment NLR means favorable outcomes, the prognosis of patients with a low pretreatment NLR and a low NLR trend was still poor in the current study (P < 0.05). Thus, radiation oncologists could optimize the NLR trend strategies during treatment.
With diagnostic imaging and RT technology development, especially intensity-modulated RT (IMRT), the 5-year OS of patients with NPC has reached more than 90%.32,33 Although formerly regarded as a mere immunosuppressive treatment, pre- and clinical observations indicate that RT can elicit an immune response against the tumor.34,35 The response was first observed as an infrequent “abscopal effect” that emerged from the tumor remission phenomenon outside the radiation field in satellite secondary tumors. 36 However, the basic consensus of the interaction between RT and the immune system has always existed. The use of large segmentation, such as stereotactic body RT, instead of conventional segmented RT used in head and neck tumors, may trigger an immune response, called the abscopal effect. 37 Also, it is difficult to generate abscopal effects by RT alone; however, it frequently emerges in patients treated with combined RT and immunotherapy 40. 38 For example, Hsu et al. 39 and Ma et al.’s 40 programmed death-1 and programmed death-ligand 1 inhibitor trials revealed objective response rates of 25.9% and 20.5%, respectively. Without precise stratification and prognosis indices, determining who receives systemic intensification or deintensification with RT and when remains difficult.41,42 This study's high NLR trend reflects immune-inflammation transformation during RT, which may be positive antitumor response evidence (Figure 5).
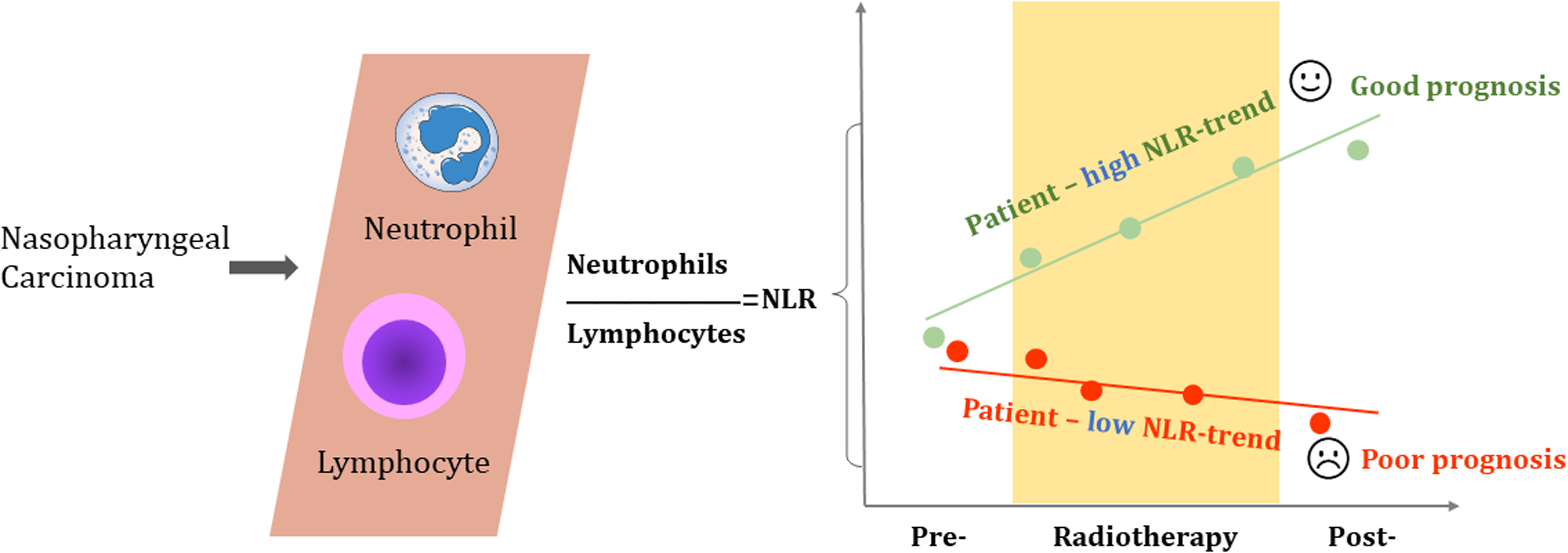
The illustrated summary of NLR-trend for nasopharyngeal carcinoma.
This study has some limitations that should be addressed. First, the data were old and varied over more than 20 years. However, these cases are precious because they received RT alone in the past, which excluded the effect of combined chemotherapy. Second, 2DCRT is not currently the first-line NPC treatment, and whether the similar response in NPCs can be triggered by other RTs, such as IMRT, remains unknown. Third, several different versions of the staging systems have existed over the years, and the data were restaged according to the Chinese 2008 staging system. Fourth, as a retrospective study, a number of CBC tests could not be arranged, and the time point and CBC test frequency could affect the linear fitting to calculate the trend. A well-designed prospective clinical trial is needed to prove the prognostic value of the NLR trend.
Conclusions
The NLR trend is a new independent prognostic factor for patients with NPC treated with RT. The combination of the NLR trend and pretreatment NLR is more accurate in predicting NPC prognosis than pretreatment NLR alone. A high NLR trend may be evidence of a positive immune response to RT in NPC, and it can be a promising index for individualized radioimmunotherapy.
Supplemental Material
sj-tiff-1-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-tiff-1-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-tiff-2-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-tiff-2-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-tif-3-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-tif-3-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-tif-4-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-tif-4-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-tiff-5-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-tiff-5-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-docx-6-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-docx-6-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-docx-7-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-docx-7-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-docx-8-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-docx-8-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Supplemental Material
sj-xlsx-9-jbm-10.1177_03936155221110250 - Supplemental material for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy
Supplemental material, sj-xlsx-9-jbm-10.1177_03936155221110250 for Neutrophil-to-lymphocyte ratio trend: A novel prognostic predictor in patients with nasopharyngeal carcinoma receiving radiotherapy by Pei Yang, Yu Zhao, Hao Liang, Guanzhi Zhou, Bassem Youssef, Hesham Elhalawani, Meizhen Li, Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Abdallah Sherif Radwan Mohamed, Nantavithya Chonnipa, Danita Kannarunimit, Yingrui Shi, Hui Wang and Clifton David Fuller in The International Journal of Biological Markers
Footnotes
Acknowledgments
The authors gratefully acknowledge the help of the support from the information department of Hunan Cancer Hospital for providing previous release files of the database.
Authors’ contributions
Pei Yang conceived and designed the research. Hao Liang and Yu Zhao performed the statistical analysis and data visualization. Pei Yang and Hao Liang drafted the manuscript. Guanzi Zhou, Meizhen Li, Bassem Youssef, Hesham Elhalawani, and Abdallah Sherif Radwan Mohamed made critical revision of the manuscript for key intellectual content. Fengbo Tan, Yi Jin, Hekun Jin, Hong Zhu, Yingrui Shi, and Hui Wang acquired, cleaned, and organized the data. Nantavithya Chonnipa, Danita Kannarunimit, and Clifton David Fuller did the methodological assessment and reviewed the data analysis. Pei Yang and Yu Zhao contributed equally to this work.
Availability of data and materials
All data generated and analyzed during this study are included in this article. The supplementary materials have been uploaded.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Hunan Cancer Hospital Ethics Board and the hospital Review Committee. Informed consent was received from all the participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from the Chinese National Cancer Center (No. NCC2017A17, No. NCC2017L01), the Hunan Provincial Science and Technology Department (No. 2020RC2061), and the National Natural Science Foundation of China (No. 81702956), and the Hunan Cancer Hospital Climb Plan (YF2020006).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.