
Abstract
Background:
Vitamin B12 deficiency is a critical medical condition that, if left untreated, can lead to severe symptoms and potentially serious and life-threatening complications. Clinical guidelines are designed to provide a standardized approach to diagnosis and treatment, aiming for consistency and effectiveness. However, it is well-established that not all patients fit into general guidelines.
Objective:
To investigate the clinical relevance of the submitted research to support these protocols for diagnosing and treating a B12 deficiency.
Approach:
Conducting a literature review of the references focused and used on diagnosing and treating vitamin B12 deficiency in adults and children.
Results:
No robust clinical trial nor RCT has been found to back up the current protocols. The research used is primarily based on assumptions rather than solid clinical evidence.
Conclusion:
Existing guidelines for vitamin B12 deficiency need to be significantly revised and improved through clinical research, clinical experience by experts in the field with input from patient groups worldwide.
Plain language title
Analyzing the Lack of Research on Vitamin B12 Deficiency Guidelines: Insights from Studies and Clinical Advice
Plain language summary
This study dives into Vitamin B12 deficiency, stressing its serious health impacts and potential life-threatening complications when not treated. The study aims to investigate the scientific articles supporting these guidelines and their clinical relevance, conducting an in-depth analysis of literature references. The manuscript investigates and criticizes current guidelines for B12 deficiency, pointing out 4 key issues reported by patients and clinicians worldwide. The results are grouped into 4 sections:
In the discussion, the manuscript argues that awareness of guidelines is low, and evidence-based guidelines may lack practical relevance. It suggests a significant revision of guidelines based on robust clinical evidence, advocating for personalized treatment, patient monitoring tools, controlled trials, and age-related healthy levels. Recognizing diverse patient needs and implementing individualized therapies are crucial for improving care for those with vitamin B12 deficiency, emphasizing the importance of early recognition and intervention.
Keywords
Introduction
A deficiency in Vitamin B12 is a significant medical concern that, when not addressed, may result in pronounced symptoms and potentially pose grave and life-threatening complications. 1 Clinical guidelines are designed to provide a standardized approach to diagnosis and treatment, aiming for consistency and effectiveness. 2 In medical practice, practitioners must offer precise recommendations from the most robust clinical evidence combined with their clinical expertise and discernment.
Many guidelines for diagnosing and treating B12 deficiency have been drawn up worldwide. However, patients from groups with B12 deficiency and experienced clinicians worldwide have reported 4 significant problems they experience in the guidelines and protocols for diagnosing and treating B12 deficiency. A maintenance dose once every 2 or 3 months after the “loading dose of 10 injections” is sufficient for some but not all patients to prevent a relapse of complaints. Oral supplementation does not work for every patient, especially those with moderate to severe symptoms or neurological complaints. Children also suffer from a B12 deficiency; symptomatic children suspected of having a B12 deficiency are often not diagnosed or treated. Diagnosis is often missed or delayed due to a knowledge gap regarding the many and varied clinical presentations of B12 deficiency and misinterpretations of blood values.
Objective
To investigate which published scientific articles are used to support those guidelines and whether they have clinical relevance.
Approach
An in-depth analysis of the literature references used to draw up the guidelines for diagnosing and treating B12 deficiency.
Results
Treatment Protocol Regarding Maintenance Dose
The protocols for treating B12 deficiency stated that “after an initial loading dose, you may switch to the maintenance dose once every 2 to 3 months.” The argument to substantiate this guideline is that the liver will be sufficiently replenished after the loading dose and that a liver typically contains enough cobalamin to last 2 or 3 years. As proof, the 1957 research by Marianne Swendseid is often used, for instance, in the Netherlands. 3,4 Yet, if you read this study in its entirety, it is not about the clinical effectiveness of the presence of cobalamin; it is only provided as proof that livers with cirrhosis contain less cobalamin than livers without cirrhosis: a clear and distinct conclusion from good research. At the end of the publication, a hypothesis is written: “If one has a liver weight of 1500 Gm and if there is 0,70 Gm B12 present, and if one needs 0,24 Gm much cobalamin in the body and if the cobalamin present is available to the body, then one has enough cobalamin in the liver for two to three years.” However, this theory has never been tested clinically but is used to substantiate the treatment.
Recent data analysis from the Nexo Lab of the University Arhus shows that after a Roux-en-Y, Gastric Bypass, and Gastric Sleeve, patients’ levels of total serum B12 and holotranscobalamin (holoTC) drop, and methylmalonic acid (MMA) and homocysteine rise significantly after 75 days. After 150 days, MMA and holoTC especially fall into inadequate values. The researchers concluded that their “data challenge the concept that liver B12 stores secure long-term maintenance of B12 status” 5 (Figure 1).
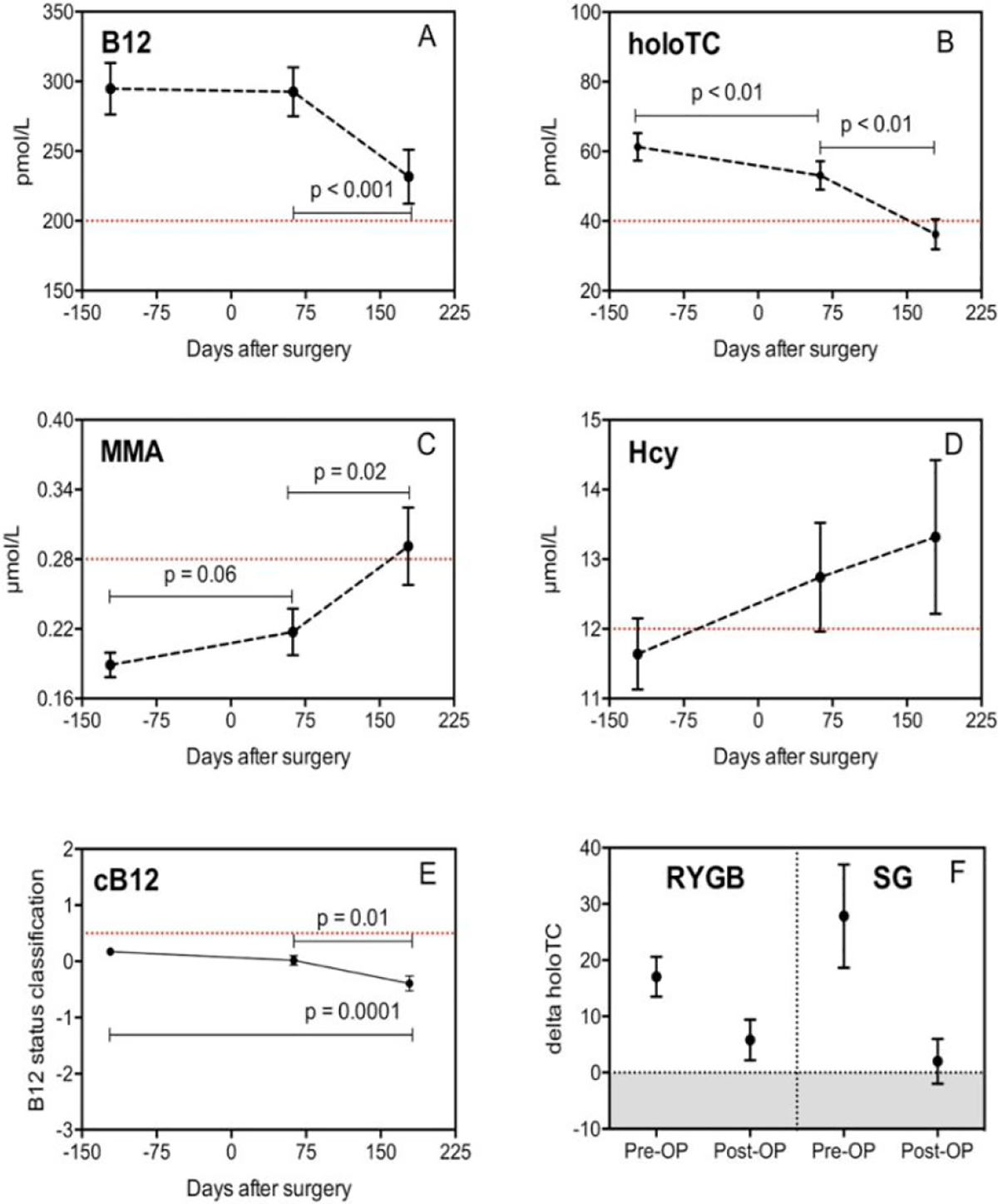
Early changes in vitamin B12 uptake and biomarker status following Roux-en-Y gastric bypass and sleeve gastrectomy. Source: Kornerup et al. 5
Also, there is no proof of the “storage of cobalamin” as “in a box.” Absorption and reabsorption of cobalamin is an ongoing complex biological system in which substances are continuously converted into other active substances. 6 -8
Apart from the research mentioned earlier, a 2019 study implemented a brief 1-month intervention focused on a vegetarian diet. Findings from the Lederer (2019) study indicate that within 4 weeks of reduced vitamin B12 intake by healthy volunteers, holo-TC, the active form of vitamin B12 in plasma, experienced an immediate decrease and, as a result of this, an increase in MMA and homocysteine. 9
Treatment Protocol Regarding Oral Supplementation
The effectiveness of oral supplementation, which is increasingly recommended as the first or sole treatment, remains questioned by many researchers, clinicians, and experts. 10 -14 Clinical trials and interventions used as proof that oral supplements work just as well as injections mainly focus on raising blood values rather than assessing clinical outcomes. 15 -18
This is, in fact, a contradiction with what is correctly stated in the B12 deficiency guidelines of the Netherlands from NHG: “testing after supplementation to monitor the effectiveness of the treatment is pointless; B12 blood value will always rise.” 4 Also by passive diffusion.
Other research focuses only on the elderly with no harmful health conditions. 16,19 Some of the 31 patients suffered from B12 deficiency malabsorption due to their diet. 19 Even the latest Cochrane review showed that the evidence that oral was just as effective as intramuscular cobalamin injections was “low to very low” because it was never adequately tested in a clinical setting. Also, there were generally too few patients included in the mentioned studies.
Diagnostic Tools for Diagnosing B12 Deficiency in Children
Children, just like adults, can suffer from a nondietary and dietary B12 deficiency with just as serious health consequences as adults. 20 -23 For children, a laboratory protocol for adults is used for diagnosis. Therefore, the general guidelines for diagnosing B12 deficiency do not include children.
However, since 2003, by Monsen et al, the median and interquartile values of B12, MMA, and homocysteine in children have been recorded and published through blood analyses 24 (Table 1). This pioneering research revealed substantial differences between adults and healthy children in B12, holoTC, MMA, and homocysteine levels. Those levels were substantially higher (sB12, holoTC) or lower (MMA, homocysteine). Other scientists repeat this research with similar outcomes as a result. 24 -28 Despite these differences, which can be well explained since cobalamin is not only involved in the production of red blood cells but is also essential for cell division and DNA (children are developing), existing guidelines do not address children with vitamin B12 deficiency. 21 This practice may lead to underdiagnosis and unnecessary suffering in children. Poor long-term outcomes of a B12 deficiency in children have been recorded. 29,30
Changes in Serum Cobalamin, Serum Folate, Plasma tHcy, and Plasma MMA in Children From Day 4 Throughout…a
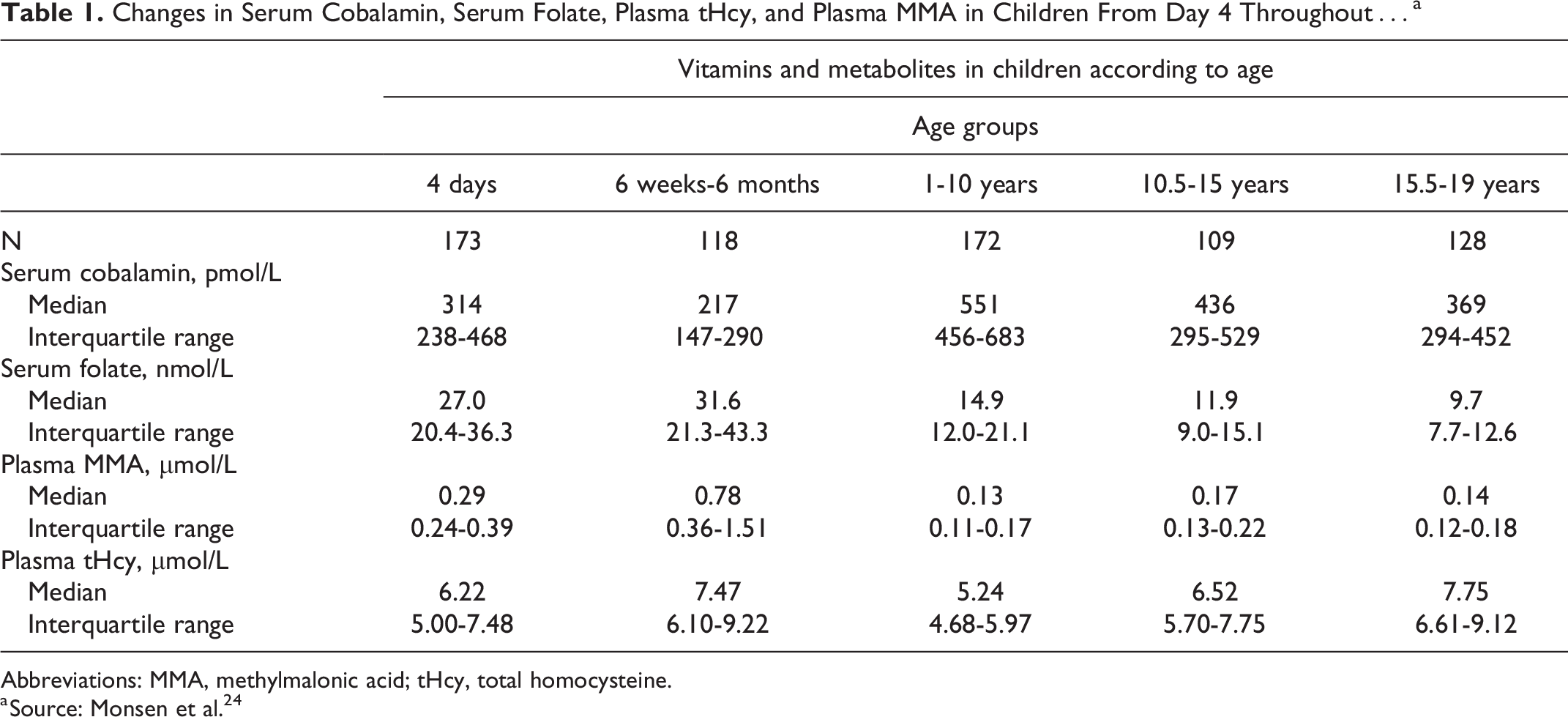
Abbreviations: MMA, methylmalonic acid; tHcy, total homocysteine.
a Source: Monsen et al. 24
Delay in Diagnosis and Treatment
Several factors underlie the delay in diagnosis and therapy: There is a need for more awareness and knowledge in recognizing B12 deficiency symptoms in adults and children.
31,32
The subtle and diverse clinical manifestations of B12 deficiency may mimic other medical conditions, especially in the absence of anemia.
33
-36
Health care professionals sometimes need to remember to consider B12 deficiency in the differential diagnosis, resulting in prolonged investigations and misdiagnosis.
37
-43
Failure to use and inaccessibility of second-line tests, such as the metabolites MMA and homocysteine. These tests are essential in diagnosing B12 deficiency when blood levels of B12 are low-normal to normal.
44
Standardization of serum vitamin B12 assays still needs to be completed: there are differences in measuring and testing methods at different laboratories.
45,46
Discussion
There is evidence that awareness of existing guidelines is generally low; it is also widely acknowledged that general guidelines may only be suitable for some patients.
47
Without robust clinical evidence, “evidence-based guidelines” may not provide sufficient guidance.
48
In case of a lack of relevant RCTs in guidelines, patient support tools are working more positively to help individualize patient decisions.
2
In 1990, the Institute of Medicine released a report to promote greater standardization and consistency in developing guidelines. This report was subsequently updated in 2011. They stated that for the guidelines to be considered reliable and effective in clinical practice, these recommendations must:
Be based on a systematic review of the existing evidence (with clinical relevance Clara Plattel). Be developed by a knowledgeable, multidisciplinary panel of experts and representatives from key affected groups. Consider essential patient subgroups and patient preferences, as appropriate. Be based on an explicit and transparent process that minimizes distortions, biases, and conflicts of interest. Provide a clear explanation of the logical relationships between alternative care options and health outcomes and provide ratings of both the evidence quality and the recommendations’ strength. Be reconsidered and revised as appropriate when crucial new evidence warrants modifications of recommendations.
49
These excellent recommendations still need to be adequately implemented in the guidelines on all points. Patient input and input from independent clinical experts are essential. Recently, a comprehensive set of treatment guidelines that meet the Institute of Medicine’s criteria for setting up guidelines has been published by Wolffenbuttel et al. 10 Unfortunately there is still a long way to go. 2,50
Conclusion
The existing guidelines for vitamin B12 deficiency need significant revision and improvement because they are primarily based on assumptions rather than robust clinical evidence to validate treatment duration, frequency, and form, particularly in assessing clinical outcomes. As a result, patients often face relapses and ongoing symptoms after being placed on maintenance doses or put on oral supplements. There is no diagnostic guideline specifically for children. Cutoff values for adults are used for the diagnosis of B12 deficiency in children, and therefore, many children go undiagnosed and untreated.
Recognizing the symptoms and the distinct needs of different patients and embracing individualized treatments are vital steps toward improving the quality of care for individuals with vitamin B12 deficiency. This will save a lot of suffering and costs. Early recognition and intervention are critical for preventing irreversible damage and promoting a timely recovery for affected individuals.
Recommendations
Developing guidelines as indicated by the Institute of Medicine (2011) Adding personalized treatment Creating a patient monitoring tool with the Patient Reported Outcome Measures method Setting up controlled intervention trials with clinical outcome measures Define “B12 deficiency” and establish age-related levels in healthy children Standardize serum vitamin B12 assays Define: “Healthy levels”
Supplemental Material
Supplemental Material, sj-docx-1-fnb-10.1177_03795721241241552 - Lack of Clinical Evidence Regarding the Guidelines for Vitamin B12 Deficiency: An Analysis From Literature and Recommendations From Clinical Practice
Supplemental Material, sj-docx-1-fnb-10.1177_03795721241241552 for Lack of Clinical Evidence Regarding the Guidelines for Vitamin B12 Deficiency: An Analysis From Literature and Recommendations From Clinical Practice by Clara H. M. Plattel in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.