
Abstract
Vitamin B12 deficiency can present with a variety of neurological and cognitive symptoms. Especially in elderly patients, vitamin B12 deficiency can be easily overlooked because symptoms may be attributed to comorbid conditions or solely to the aging process. In this case study, we present two patients, a 71-year-old man and a 74-year-old female, with vitamin B12 deficiency. The male patient had a history of (partial) resection of the ileum/jejunum/colon because of intestinal ischemia. The female patient had a history of hypothyroidism, type 2 diabetes with complications (including peripheral neuropathy), mitochondrial myopathy, and chronic lymphocytic leukemia. Both patients presented with severe fatigue, cognitive impairment, and impaired walking. Next to this, the male patient suffered from depressive symptoms and mild disorientation, and the female patient experienced neuropathic pain. She also mentioned a positive family history for B12 deficiency. The first patient had normal to high B12 levels because he was already on B12 injections (once every three weeks) because of an earlier diagnosed B12 deficiency. The female patient had B12 levels within normal range (holotranscobalamin 54 pmol/L) and her diagnosis was confirmed by elevated homocysteine and methylmalonic acid levels. Treatment with frequent hydroxocobalamin injections and other supplements significantly improved their cognitive, emotional, and motor functions. These cases underscore the need for a high level of clinical suspicion in elderly patients, also in cases of normal B12 levels but with clinical signs of deficiency and a positive risk factor, such as stomach or small bowel surgery or positive family history.
Plain language title
A case study of two elderly patients with vitamin B12 deficiency and neurological and cognitive complaints
Plain language summary
Vitamin B12 deficiency in elderly patients can be easily overlooked as symptoms can also be caused by other age-related diseases or the aging process. In our article we present two elderly patients, a 71-year-old male and a 74-year-old female, with neurological complaints, such as severe fatigue, cognitive decline, and walking impairment. The male patient had a history of small bowel surgery, and the female patient mentioned that she had several siblings with B12 deficiency. Additionally, the male patient suffered from depressive symptoms and mild disorientation, and the female had severe pain in her legs. The male patient already received B12 injections because of an earlier B12 diagnosis, but with a relatively low frequency. The B12 levels of the female patients were within the normal range. However, her diagnoses could be confirmed with additional laboratory measurements, such as homocysteine and methylmalonic acid. Treatment with frequent B12 injections and other supplements significantly improved their cognitive, emotional, and motor functions. Our study shows that clinicians should carefully consider the possibility of B12 deficiency in elderly patients with cognitive and neurological complaints, also in patients with B12 levels within the normal range, but with risk factors such as family members with B12 deficiency or conditions that may impair the vitamin B12 uptake, such as previous stomach or small bowel surgery.
Introduction
Vitamin B12 deficiency can manifest with various neurological, cognitive, and hematological symptoms. 1 -5 In clinical practice, vitamin B12 deficiency may be overlooked or misdiagnosed as extreme fatigue, cognitive deficits, and motor impairment can also be caused by other medical conditions. Moreover, these symptoms are also often attributed to the older age of senior patients. Besides this, the interpretation of laboratory test results to diagnose a (functional) vitamin B12 deficiency is not as easy as is often believed. 6 A thorough assessment of the patient’s medical history, clinical presentation, and laboratory findings can help identify a vitamin B12 deficiency. If adequate treatment has been initiated, a significant improvement in the quality of life can be achieved in elderly patients. 7 -11
With this case study, we want to highlight the importance of recognising the clinical significance of vitamin B12 deficiency and considering vitamin B12 deficiency as a possible cause of cognitive or other neurological symptoms in elderly patients, even when serum B12 levels are within the normal range. It also demonstrates the role of family history and other risk factors in diagnosing this condition and the importance of listening to your patients carefully to determine optimal treatment regimens.
Case 1
Medical History/Anamnesis/Physical Examination
A 71-year-old male presented with extreme fatigue, cognitive complaints, and walking disabilities. He had a history of (partial) resection of the ileum/jejunum/colon because of intestinal ischemia. One year before he was diagnosed with B12 deficiency (B12 92 pmol/L), and his general practitioner (GP) had started with B12 injections once every three weeks. He reported that since his intestinal resection three years earlier, he had suffered from progressively worsening fatigue, hypersomnia, emotional instability, depressive symptoms, short-term memory deficits, difficulty with writing and calculations, mild disorientation, confusion, impaired coordination, frequent falls, and muscle weakness. This led to significant impairments of activities of daily living, including walking and driving. Furthermore, he had run a housing company, but he was not able to do this anymore because of his physical and cognitive complaints.
Interestingly, he reported that after a B12 injection he had almost no complaints for three days and that he felt reasonably well up until day eight. The remaining two weeks after the injection, he experienced a significant impairment. For this reason, his GP had measured his B12 levels directly after an injection (>1467 pmol/L) and shortly before a new injection (316 pmol/L) and had concluded from these results that the B12 levels were within the normal range at all time points and opined that “therefore a treatment adjustment was not necessary”.
In addition to the cobalamin injections, he used B12 tablets once daily (1000 µg) and several other medications, including omeprazole, perindopril, acenocoumarol, loperamide as needed, multivitamins (including 400 µg folic acid), and ferrous fumarate 200 mg twice weekly. The neurological examination demonstrated intact light touch, absent right ankle vibration, and diminished left ankle vibration sense. The Romberg test was positive, and the patient exhibited unsteady balance during the “tightrope” test (walking in tandem gait). Fine tremors were observed in the hands. He also showed signs of emotional instability during the examination.
Laboratory Results
The results of our laboratory studies are shown in Table 1. The main findings were iron deficiency without anemia, and high folic acid and vitamin A levels due to over-supplementation. Glucose and prostate-specific antigen (PSA) levels were normal, and a M-protein was absent.
Laboratory Results.
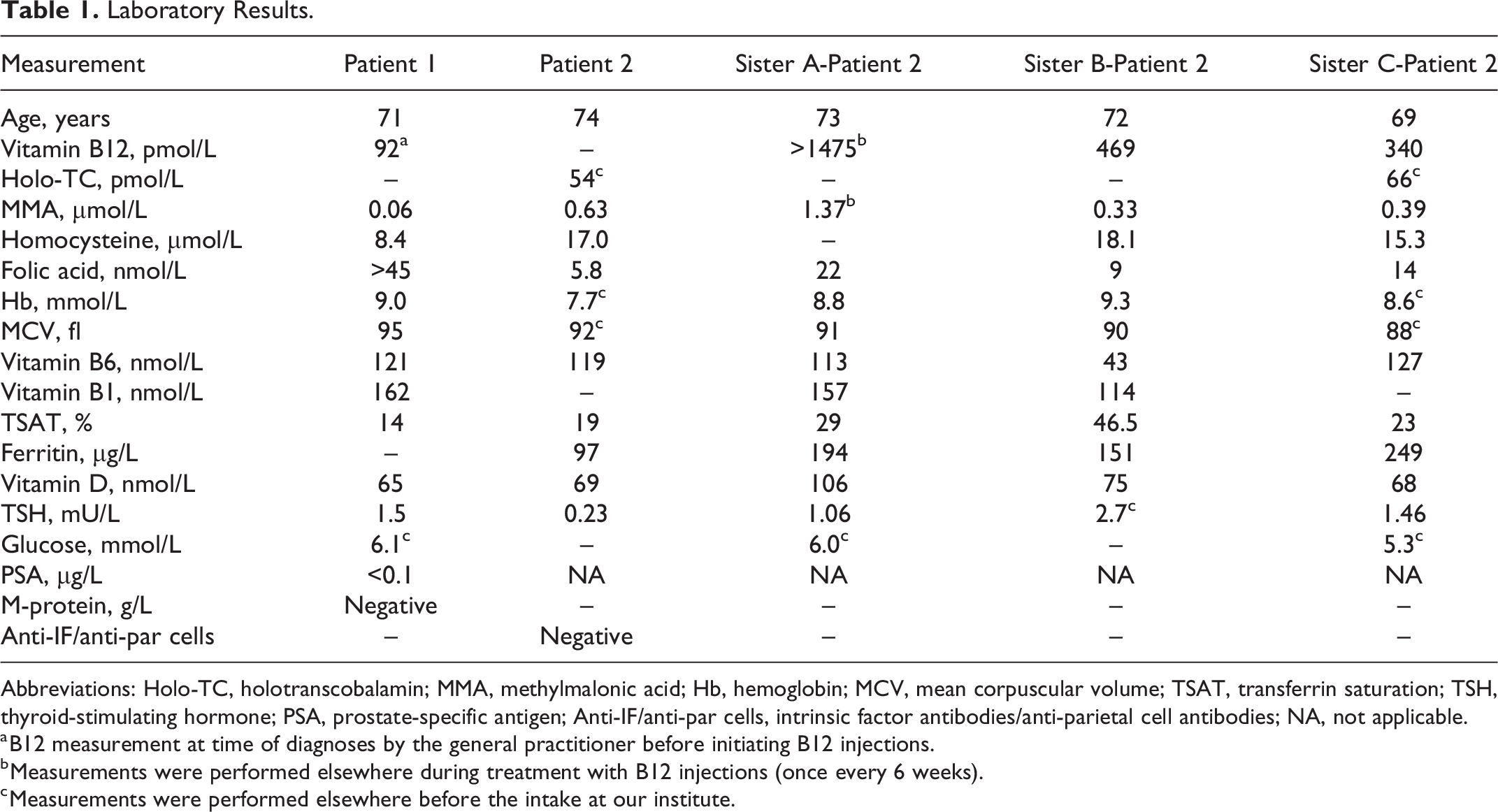
Abbreviations: Holo-TC, holotranscobalamin; MMA, methylmalonic acid; Hb, hemoglobin; MCV, mean corpuscular volume; TSAT, transferrin saturation; TSH, thyroid-stimulating hormone; PSA, prostate-specific antigen; Anti-IF/anti-par cells, intrinsic factor antibodies/anti-parietal cell antibodies; NA, not applicable.
a B12 measurement at time of diagnoses by the general practitioner before initiating B12 injections.
b Measurements were performed elsewhere during treatment with B12 injections (once every 6 weeks).
c Measurements were performed elsewhere before the intake at our institute.
As no apparent alternative cause was found, B12 deficiency with signs of peripheral neuropathy and possible dorsal column pathology was the most likely explanation. The B12 deficiency was attributed to the resection of the ileum and possibly exacerbated by the use of a proton pump inhibitor.
Treatment/Treatment Results
We increased the frequency of hydroxocobalamin injections (1000 µg) to every other day and the B12 tablets were stopped. 12 Multivitamin supplementation was reduced to twice a week, and during the treatment folic acid doses were adjusted according to serum levels. The patient’s ferrous fumarate dose was increased, and vitamin C supplementation was added. The patient showed almost immediate improvement in emotional stability and energy. After 1 year of treatment, his motor abilities normalised, and he experienced a complete recovery from his cognitive and emotional complaints, enabling him to resume an active and social life, including normal walking, driving, and running his housing company. On physical examination the Romberg test also normalised.
Case 2
Medical History/Anamnesis/Physical Examination
The second patient is a 74-year-old woman who presented with severe cognitive and neurological complaints. She reported debilitating fatigue in combination with hypersomnia, brain fog with memory deficits, poor concentration and organising skills, and difficulties finding words. Her walking was impaired due to muscle weakness, and balance and coordination skills problems, and she experienced frequent falls. She also mentioned impaired motor skills of her hands. She suffered from severe pain and muscle cramps in her legs and had a diminished sense of touch from her feet up to her knees. She had difficulties focussing her eyes, and upon inquiry she mentioned impaired hearing and tinnitus. She had an extensive medical history including vitamin B12 deficiency in 2004 for which she was treated with B12 injections once every six weeks for a year. At the time of presentation, she had not been treated with B12 injections or supplements for years. Her further medical history included hypothyroidism, type 2 diabetes with complications including ischemic heart disease, diabetic retinopathy, and neuropathy. Furthermore, she was diagnosed with a mitochondrial myopathy (although the muscle biopsy and genetic testing was not conclusive) and chronic lymphatic leukemia (CLL), for which she had received different forms of chemotherapy. She was taking multiple medications, including ibrutinib, levothyroxine, insulin, vitamin D, gabapentin, paracetamol (PCM), and magnesium supplements. Physical examination revealed diminished fine touch of the foot soles, absent position sense of the toes, a positive Romberg sign, and the inability to perform tandem gait.
Laboratory Results
Table 1 shows the laboratory results of this patient. Her holotranscobalamin was in the normal range, but a vitamin B12 deficiency could be confirmed because both her homocysteine (Hcy) and methylmalonic acid (MMA) levels were elevated. Next to this she had folic acid deficiency, an elevated vitamin B6 level, and her hypothyroidism was slightly over supplemented.
Treatment/Treatment Results
Our patient received hydroxocobalamin injections (1000 µg, 2/week), folic acid supplementation (0.5 mg, 2/week), and an adjustment of levothyroxine treatment. Within 1 month, the patient experienced significant improvements in fatigue, balance, and focus and vision. Her medical condition improved further, and after 1 year of treatment, she reported a marked improvement in her energy levels, walking ability, and cognitive functioning. She mentioned that she could engage in sport activities again, that “she was able to think clearly again”, and that her brain fog had resolved. However, she still experienced severe pain in her legs and had muscle cramps. Therefore she requested an increase in hydroxocobalamin injections. Although we explained that increasing the frequency of B12 injections might not alleviate these symptoms, because they could also be caused by her other medical conditions (diabetic neuropathy and side-effects of her chemotherapy), our patient expressed a strong preference to try this, nonetheless. Surprisingly, 4 months after this adjustment (hydroxocobalamin injection1000 µg, 3/week) she reported a marked improvement in her neuropathic pain and muscle cramps, and she was able to stop her pain medication (paracetamol and gabapentin). Unfortunately, during the next year her neuropathic pain relapsed, and she preferred to return to twice weekly B12 injections. She also experienced deterioration of her muscle strength and walking ability, probably due to her mitochondrial myopathy. However, up until this day she is able to engage in sporting activities, and she has no cognitive complaints.
Family History
Interestingly, our patient had three sisters with a history of B12 deficiency. They also had elevated Hcy and MMA levels despite serum B12 levels within the normal range (see Table 1), suggesting a familial component. All sisters received hydroxocobalamin injections two to three times a week, and two of them reported significant clinical improvements upon treatment. However, the tinnitus of the youngest sister, which was one of her most troublesome physical complaints, did not improve, and she stopped treatment after six months. A few months later she restarted B12 injections at a low frequency (once-monthly), because she had the impression that her muscle complaints increased after she had completely stopped B12 injections. An exome analyses of six vitamin B12 related genes (including TCN2, MMACHC, CD320, CBLIF, ABCD4, and MMADHC) of our patient (case 2) did not reveal a causal genetic deficit. However, this does not rule out a familial component, since clinical phenotypes can also be the result of a combination of common genetic variants, epigenetic phenomena, other (unknown) genes that were not analysed, and regulatory elements that are not part of an exon.
Discussion
This study and others reinforce the importance of recognising and treating B12 deficiency in elderly patients with psycho-neurological symptoms and cognitive decline. 9,11,13 Both cases show that elderly B12 patients can benefit largely from adequate vitamin B12 treatment, even in individuals with significant comorbidity (see Table 2 for an overview of our main recommendations based on our case study).
Main Learning Points.
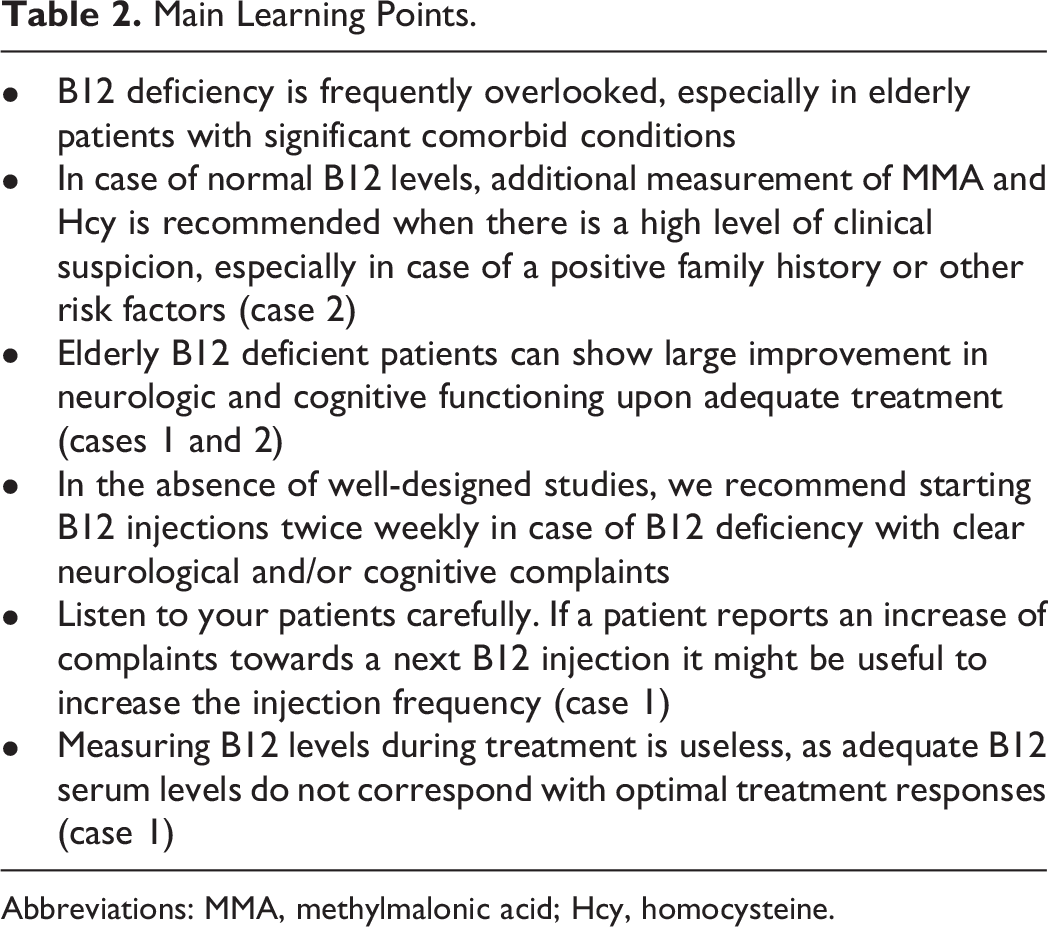
Abbreviations: MMA, methylmalonic acid; Hcy, homocysteine.
Currently, well-designed trials are needed to establish optimal treatment protocols for vitamin B12 deficiency. In the absence of these studies, we usually start with twice weekly hydroxocobalamin injections (1000 µg) in case of neurological symptoms in line with the Dutch national formulary. 14 Alternatively, B12 injections on alternate days can be started as Wolffenbuttel et al proposed in a recent publication. 12 Once symptoms have subsided or do not improve any further, injection frequency can be reduced slowly. In our experience, and in line with the protocol of Wolffenbuttel, it may take months or even years for neurological signs and symptoms to resolve completely. This may be longer than frequent B12 injections are often prescribed in clinical practice.
As Case Study 1 shows the measurement of cobalamin levels during vitamin B12 treatment is useless as adequate cobalamin levels do not correspond with optimal treatment responses. 12 Furthermore, this case study illustrates that if symptoms increase toward the next injection, it might be useful to increase the injection frequency. This might also be helpful if neurological symptoms do not resolve completely (Case Study 2).
Case Study 2 shows that B12 deficiency might be present even when B12 serum levels are within the normal range. Therefore, we recommend additional measurement of Hcy and MMA if there is a high clinical suspicion, especially in case of a positive family history or other risk factors. Furthermore, this case study illustrates that large treatment effects can be achieved even in the presence of significant contributing conditions such as type 2 diabetes with complications, myopathy, and side effects of chemotherapy for CLL.
Some authors have raised concerns that B12 supplements might induce a slightly increased risk for malignancies. 15 -18 Furthermore some chemotherapies might be less effective in combination with vitamin B12 treatment. However, this effect has only been studied for a few substances. 19 Our patient 2 indicated that she preferred quality of life above a (theoretical) risk that her chemotherapy might be less effective or her CLL might progress. So far, after two years of treatment, her CLL has been stable. Our patient received ibrutinib for an indefinite period (until disease progression or unacceptable toxicity). In the event that a course of chemotherapy is needed for a short period, we usually advise to temporarily stop the B12 treatment (and folic acid supplements) or decreasing B12 injection frequency if stopping is not feasible.
In summary, our case study reinforces the importance of recognising and treating vitamin B12 deficiency in elderly patients with psycho-neurological symptoms and cognitive decline, as they can benefit largely from adequate treatment. Well-designed studies are needed to determine optimal treatment regimens, to confirm long-term safety and efficacy and to improve diagnostic tools. For now, health care providers should take patients’ medical history and symptoms seriously, especially in elderly individuals, to ensure timely diagnosis and appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.