
Abstract
Background:
Vitamin B12 deficiency is prevalent worldwide especially in vegetarian communities. Its deficiency in early childhood may result in serious neurological and cognitive deficits. It is important to know the prevalence among our infants and toddlers so that nutritional policy changes could be suggested in this regard.
Objective:
To evaluate the vitamin B12 status of apparently healthy Indian children between 6 and 23 months of age.
Methods:
Apparently healthy Indian children (n = 210), of age 6 to 23 months, attending pediatric outpatient department were recruited and samples obtained to evaluate their hemogram and levels of vitamin B12, folate, and ferritin. Data were analyzed to obtain the mean levels and the proportion of participants deficient in vitamin B12. The dietary habits of the children were also analyzed and correlated with their vitamin B12 status.
Results:
Vitamin B12 deficiency was observed in 37.6% of the participants.
Conclusions:
There is a high prevalence of vitamin B12 deficiency in our infants and toddlers, and there is need to initiate supplement to prevent any possible neurological consequences. Early initiation of animal milk had a positive effect on the vitamin B12 status of the child, though it was not significant.
Introduction
There is widespread prevalence of vitamin B12 (B12) deficiency in communities that are largely vegetarian. 1,2 This has been observed the world over even in developed countries. India is largely a vegetarian population, and micronutrient deficiencies abound in the community. 3 While iron has been always a focus of public domain, B12 deficiencies largely remain unrecognized and undiagnosed. 4 Deficiency of this nutrient is not only an important cause of anemia but its deficiency may cause impaired myelination, axonal degeneration, and cerebral atrophy resulting in substantial neurological deficits such as hypotonia, cognitive deficits, and developmental delay in children. 5 -7 This may remain undiagnosed and lead to a poor neurological and cognitive outcome for the child. Detecting this deficiency at an early stage and instituting appropriate therapy can be highly rewarding in preventing these effects. 8
Only a few studies have reported high prevalence rates of B12 deficiency in the population, and data are inadequate and insufficient in this field. Kapil et al detected B12 deficiency in 38.4% of children of 12 to 59 months age-group using radioisotope estimation method. 9 Another study by Houghton et al evaluated 77 children of 12 to 23 months age-group and reported 29% deficiency of this nutrient. 10
Our study was planned to evaluate asymptomatic children at the vulnerable age of 6 to 23 months, when most are making transition from mother’s milk to complementary foods and are also at the peak of neurocognitive development. Recognizing and treating B12 deficiency at this crucial stage could prevent serious neurodevelopmental deficits.
Materials and Methods
This cross sectional study was conducted in a tertiary care referral pediatric hospital of north India over a period of 1 year after due clearance from the institutional ethics committee. This hospital, being in the public domain with no user charges, caters to mainly low and middle socioeconomic population. Consecutive children presenting to immunization clinic were screened for possible inclusion. A detailed history was elicited to screen the participants for any chronic illness like kidney, liver, cardiac diseases, malabsorption, and for multivitamin supplementation in the past 3 months and those with any such history were excluded from the study. Participants with weight for length less than −3 z score of World Health Organization (WHO) growth standards were also excluded from the study. Apparently healthy children, of age-group 6 to 24 months, were offered participation in the study. A detailed physical examination was conducted to exclude any illness or chronic condition. Written informed consent was obtained from either of the parents before enrolling the child in the study. Diet at this weaning stage primarily consists of mother’s milk, bovine milk, and complementary foods and hence information was sought on the intake of these and the duration of time that the child had been taking these (as this would affect his or her B12 status). Two mL of venous blood was obtained under aseptic conditions and sent for hemogram, peripheral smear, serum folate, serum ferritin, and serum B12 levels. The biochemical tests were measured by automated analyzer (Acess II Beckman Coulter machine) based upon chemiluminescence immunometric assay method (coefficient of variation of less than 12%, less than 5%, and less than 6.5% for estimation of B12, folate, and ferritin, respectively).The normal ranges for serum B12, folate, and ferritin were defined as 200 to 700 pg/mL, 4 to 9 ng/mL, and 12 to 95 ng/mL, respectively. 11 Anemia was defined as hemoglobin less than 11g/dL. 12
Sample Size Estimation and Statistical Analysis
In a previous study, the prevalence of vitamin B12 deficiency in toddlers was 28%. To detect the same prevalence with precision of 5% and level of confidence of 90%, a sample size of 218 was required. The sample was stratified based on age; 70 participants each in the age-groups of 6 to 11 months, 12 to 17 months, and 18 to 23 months were enrolled.
Data were coded and entered into Microsoft Excel sheet. Statistical analysis was done by SPSS version 23. Descriptive statistics were done by calculating frequency with percentages, mean with standard deviation, or median with interquartile range as applicable. Significance of difference between 2 means was analyzed by independent sample t test, and significance of difference between 2 medians was analyzed by Mann-Whitney U tests. Pearson chi-square or Fischer exact test was done to test significance of difference between 2 proportions. A P value <.05 was considered significant.
Results and Analysis
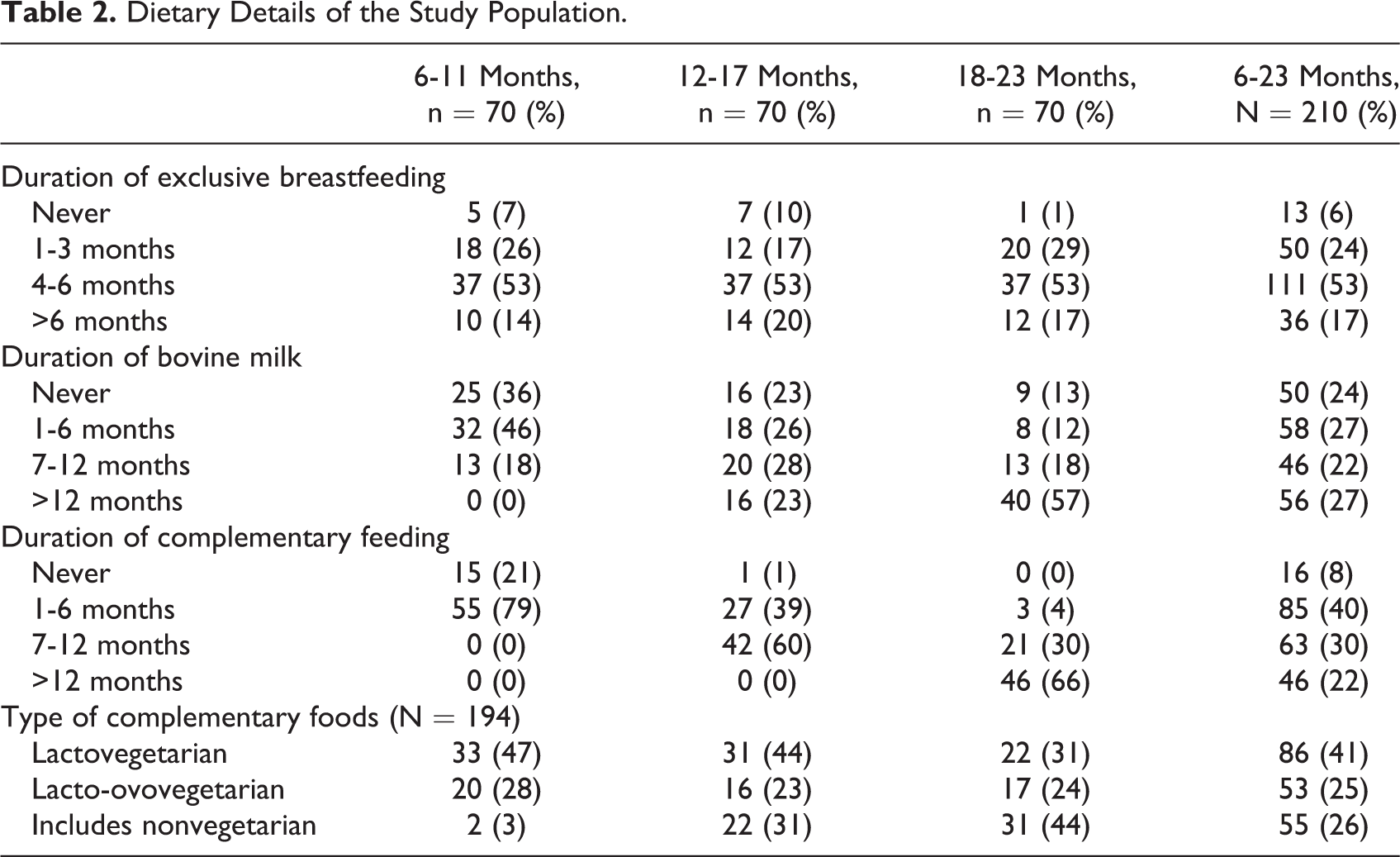
A total of 237 children were screened for possible inclusion in the study. Four were excluded on suspicion of a chronic ailment, 14 had received some form of multivitamin in the past 3 months, and 3 had weight for length less than −3 z score of WHO growth standards. Participation was refused by 6 parents. In all, 210 participants were thus enrolled in the research. The sociodemographic and dietary details of the study population are shown in Tables 1 and 2, respectively. The mean duration of exclusive breastfeeding in the study population was 4.9 ± 2 months and 125 of 210 received breastfeeds for 6 or more months. Our population relies substantially on packaged bovine milk available at dairy stores, and the mean age of initiation of bovine milk was 5.3 ± 3.9 months. Consumption of egg or meat more than once a week was noted in 32.8% (69/210). Hematological profile of the population is detailed in Table 3 with a high frequency of 79.5% (167/210) of children found to be anemic. Vitamin B12 deficiency was found in 37.6% (79/210) of children. Among the 3 age-groups (6-11, 12-17, and 18-23 months), 32 of 70 (46%), 19 of 70(27%), and 28 of 70(40%) were deficient in cobalamin, respectively. Cobalamin levels less than 100 pg/mL were noted in 24% (19/79) of the deficient children; the lowest level being 21.8 pg/mL. Folate was less than 4 ng/mL in 4.3% (9/210), and ferritin was less than 12 ng/mL in 39% (82/210) of population. Sociodemographic factors like gender, birth order, and socioeconomic status were not significantly associated with cobalamin deficiency (Table 4). However, those of higher birth order had a poorer cobalamin status.
Sociodemographic Details of the Study Population.
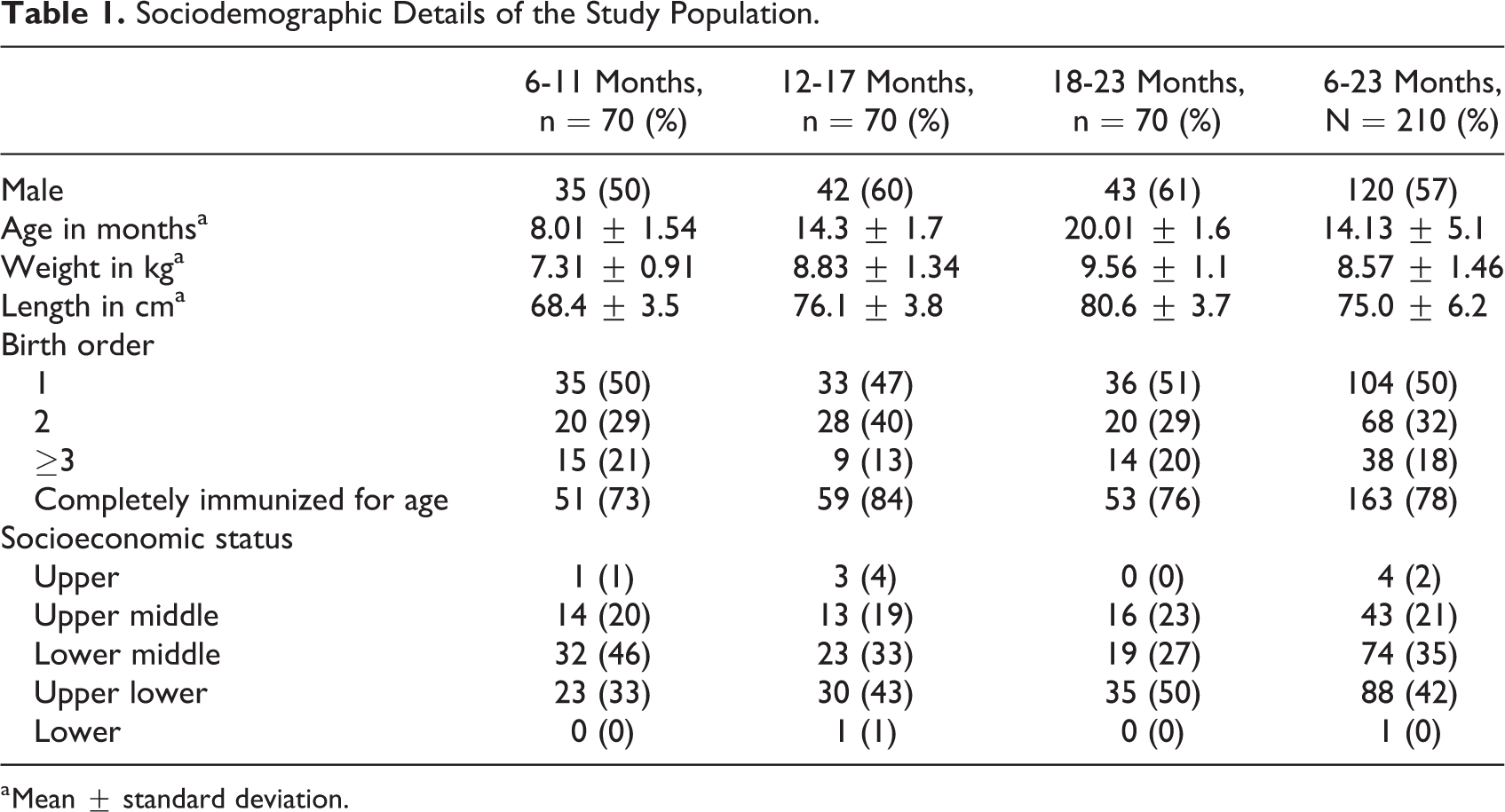
a Mean ± standard deviation.
Dietary Details of the Study Population.
Age-Wise Depiction of Hematological Parameters.a
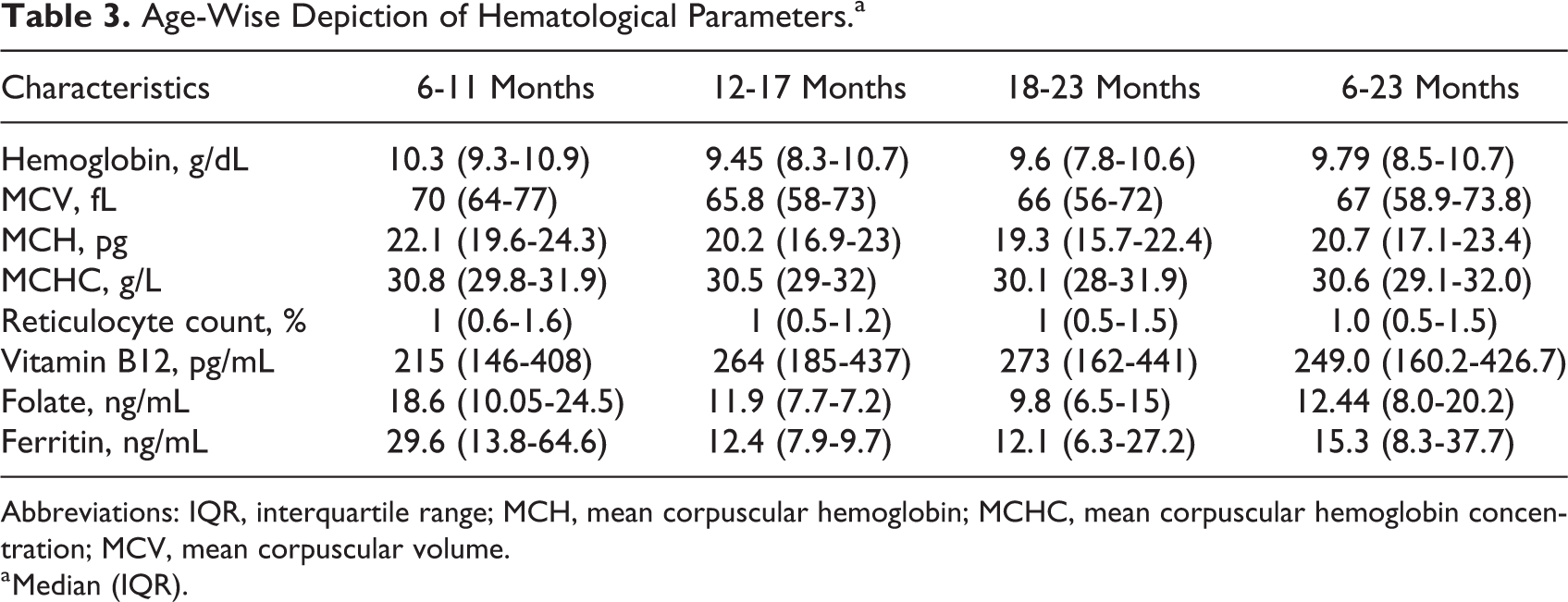
Abbreviations: IQR, interquartile range; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume.
a Median (IQR).
Univariate Analysis of Sociodemographic and Dietary Factors Associated With Vitamin B12 Deficiency.
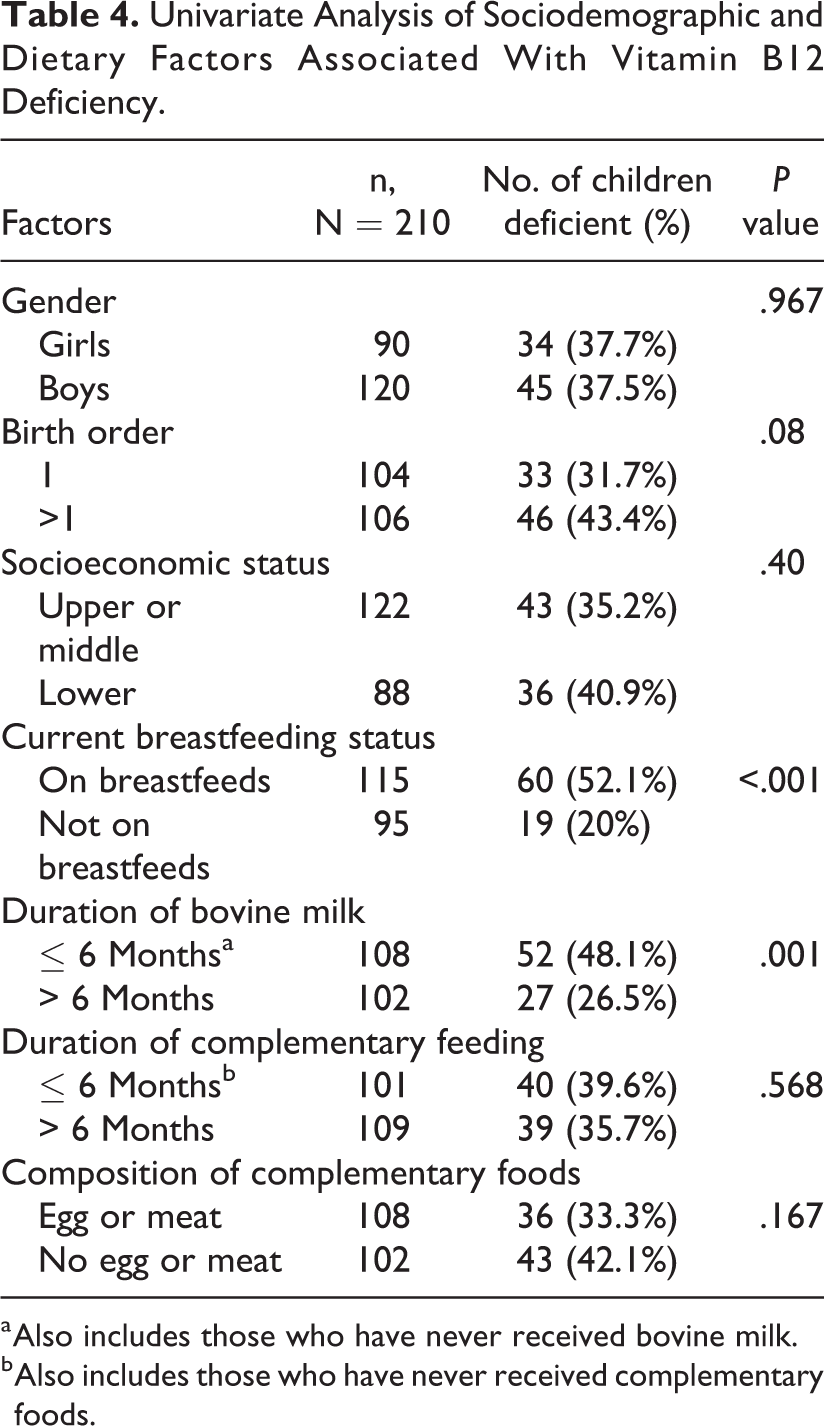
a Also includes those who have never received bovine milk.
b Also includes those who have never received complementary foods.
Analysis of the dietary factors revealed that intake of bovine milk had a positive effect on the B12 status of the individual (Table 4). On the other hand, those who were still receiving breastfeeds had a compromised B12 status. Median cobalamin levels in children who were not completely weaned off breast milk by 1 year of age was 199 pg/mL (127-301 pg/mL), whereas it was 354 pg/mL (237-532 pg/mL) in those who were completely weaned off before 1 year of age. This observation was also statistically significant (P value <.001).Intake of animal source foods improved the B12 status but not significantly so. It was also observed that 50 of 210 children were not provided any kind of bovine milk and 16 of 210 children were not given any complementary foods. Diluted formula feed was being given in 21 of 210 cases and this was in small amounts and in addition to bovine milk and hence was not considered separately for analysis.
Discussion
Of the 210 apparently healthy children of 6 to 24 months, 37.6% were found to be cobalamin deficient. Such a high rate in healthy young population should be considered as an alarming situation because cobalamin deficiency in early life may lead to devastating complications which may not be reverted even after adequate supplementation in the later years. 13
The sociodemographic parameters studied (sex, birth order, socioeconomic status) had no significant association with B12 deficiency. It was observed that consumption of bovine milk significantly improved the B12 status of the child. This is consistent with the higher B12 concentration known to be present in bovine milk than in breast milk. 14,15 Consumption of complementary foods did not improve the B12 status. Surprisingly, even consumption of egg or meat and their frequency of consumption were not significantly associated with B12 levels despite these foods being sources of cobalamin. This might be due to the fact that the proportion of these foods in the diet is minimal unlike in Western populations where these foods constitute major part of the diet. Thus, the overall B12 intake from these foods per day may be very low.
Surprisingly in this study, a longer duration of breastfeeding was significantly associated with B12 deficiency. This may be explained by the fact that most of Indian mothers are known to be deficient in B12; hence the baby (with impoverished B12 stores) gets breast milk deficient in B12. 16 -19 Also, children with continued breastfeeding consume bovine milk and complementary feeds in fewer quantities, thereby aggravating the deficiency. So, while breastfeeding is extremely important for the overall nutrition and well-being of the infant and is recommended till 2 years of age, it is also important to note that the impoverished societies need to focus on and improve the micronutrient health status of the mother. Our findings are in consonance with those of Pasricha et al who observed significant association of B12 deficiency with continued breastfeeding among 12- to 23-month-old rural Indian toddlers. 20 The prevalence of cobalamin deficiency observed by them was, however, very less (9 of 396).
As most of the Indian population is vegetarian by nature, they are under lifelong risk of cobalamin deficiency unless supplemented. Several studies done in Indian adult population and especially in pregnant women highlight the widespread cobalamin deficiency present in the community. In a large hospital-based cross sectional study on 2660 participants aged 0 to 96 years, the prevalence of cobalamin deficiency was reported as 44.6%. 21 In a study conducted by Refsum et al in Pune on 204 men and women aged 27 to 55 years, 47% were found to be cobalamin deficient. 22 In another similar study conducted by Yajnik et al on 441 middle aged men 67% were deficient. 23 Studies conducted by Pathak et al and Samuel et al in Indian pregnant women showed deficiencies of 71% and 51%, respectively. 16,24 Surveys estimating prevalence of B12 deficiency in adolescents have revealed varying figures of 32.4%, 72.7%, 73.5%. 25 -27
Although there are some studies addressing the cobalamin deficiency among anemic children that reported prevalence of 22% to 62%, 28,29 very few studies have been done among healthy children.
In a large community based study conducted in 2261 children aged 6 to 30 months of low- to middle-income families from New Delhi by Taneja et al, 4 the prevalence of B12 deficiency was found to be 28%. The method used for estimation of B12 in this study was a microbiological assay which has poor precision and low specificity. 30 A large sample size of this study, however, makes the results noteworthy. This study has attributed the deficiency to prolonged breastfeeding, delayed introduction of complementary foods, lack of fortification of feeds, low consumption of animal source foods, and high rates of gastrointestinal infections in their study population. Hanumante et al found that 14% of the asymptomatic toddlers with mean age of 2.4 years were cobalamin deficient. 31 This study attributed the deficiency to low intake of animal source foods and typical Indian vegetarian diet. In a recent community based cross sectional study on 470 Indian children aged 12 to 59 months, the prevalence of B12 deficiency was observed to be 38.4%, very similar to our findings. 9 They observed a higher prevalence in children who had vegetarian food habits (50.4%) than those who were nonvegetarian (33.8%). 9
Among reports from other countries, the situation is similarly dismal. 32,33 In an assessment of B12 status of 302 infants of Guatemala, 90 were found deficient. 32 Maternal plasma B12 concentration and B12 intake from complementary foods were positively associated with infant plasma B12. Infants who were breastfeeding had a higher frequency of B12 deficiency than those who were non-breastfeeding. Maternal B12 deficiency was also the most common finding in newborn screening results published recently from Germany. 34
As already mentioned, prevalence of cobalamin deficiency in our study was 37.6%. This high prevalence in our infants and toddlers reflects the impoverished nutrient status of their diet and the need for supplementation could not be overemphasized. The use of chemiluminescence assay for biochemical measurements adds to the reliability of our results.
Our study also has several limitations. Although we recruited only apparently healthy children, our study being a hospital-based study may not be directly comparable with other population-based studies. Correlation has not been done with B12 status of the mothers.
Assessment of homocysteine and methylmalonic acid levels would have been useful in combination with B12 levels but could not be estimated. 35 An assessment of daily amount of B12 present in daily dietary intake content would have helped further in the interpretation of the study findings. Despite these limitations, this study is one of the few studies on B12 status of healthy children.
Conclusions
The findings of the study show the widespread prevalence of B12 deficiency in infants and young children, which cannot be overlooked, and whose consequences can be easily prevented by dietary modifications and supplementation, beginning early in life.
Footnotes
Acknowledgments
The authors thank Dr Anup Mohta, Director, Chacha Nehru Bal Chikitsalaya and Dr B. Talukdar, Head of Department, Department of Pediatrics, Chacha Nehru Bal Chikitsalaya, Delhi-110031, for their help during the study.
Authors’ Note
Dr Medha Mittal is the proofreader.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.