
Abstract
Background:
Vitamin B12 deficiency is commonly diagnosed using thresholds developed for adults, yet emerging evidence indicates these levels may not be appropriate for children and adolescents. This misalignment can lead to underdiagnosis in younger populations, with potential long-term health implications.
Case Summary:
Chief Complaint: The 17-year-old female patient experienced severe fatigue, menstrual irregularities, psychological distress, and neurological symptoms over several years. The 13-year-old male patient had behavioral changes, gastrointestinal complaints, and sensory disturbances from an early age.
Diagnosis: Both adolescents displayed B12 levels that were considered low-normal based on adult thresholds, complicating their diagnostic processes. Their diverse and atypical symptomatology required a comprehensive review of their medical and family histories, clinical symptoms, and risk factors.
Intervention: Treatment included administration of hydroxocobalamin injections, complemented by dietary adjustments.
Outcome: Both patients responded well to the treatment, showing significant improvements in their symptoms and overall quality of life.
Conclusion:
The main takeaway from these cases is the importance of tailoring diagnostic adequate thresholds and treatment plans to the pediatric population to address and manage B12 deficiency effectively. This approach can significantly enhance patient outcomes and prevent the progression of potentially severe complications in later life.
Plain language title
Revisiting Diagnostic Criteria for Vitamin B12 Deficiency in Children and Adolescents, a Case Report
Plain language summary
Vitamin B12 deficiency is surprisingly common in kids and teenagers, but the problem is, only adult standards are available to diagnose it. Research shows that healthy children can have much different B12 levels than adults, meaning some kids with a deficiency might not get the help they need quickly. We share stories of 2 teenagers who suffered from B12 deficiency with very different symptoms, from extreme tiredness to mood changes and stomach issues. These cases show that diagnosing B12 deficiency can be difficult, especially with symptoms that don’t fit the usual pattern. However, once they were properly diagnosed and treated adequate, these young people saw significant improvements in their health. These cases highlight the need for new standards tailored to children, to better identify and treat B12 deficiency early on, improving their quality of life.
Keywords
Introduction
Vitamin B12 deficiency in children and adolescents is common and represents a significant health concern. 1 -5 Common causes of B12 deficiency in childhood include pernicious anemia, malabsorption syndromes, gastrointestinal surgeries, and nutritional deficiencies. 6
In addition to the fact that children can also develop a B12 deficiency due to underlying genetic and hereditary factors, scientists in the field are concerned about the growing number of people on a vegetarian or vegan diet who can develop a B12 deficiency. 7,8 In case of even reasonably adequate B12 levels in the mother’s body (with malabsorption or with a vegetarian or vegan diet), the cobalamin may be insufficient to pass on to the child via the umbilical cord. If the child is subsequently breastfed for months that contain too little vitamin B12, it may suffer serious health consequences. 9 -12 There is also a knowledge gap in recognizing the B12 deficiency symptoms in children; it sometimes takes years to get a proper diagnosis. 4,13 These findings are consistent with what we see in clinical practice.
Diagnostic Thresholds
The diagnostic cutoff values for symptomatic B12 deficiency in children delay treatment and, therefore, recovery. Published studies from 2003 to recently highlight the significant variations in age-related B12 levels in healthy children compared with the diagnostic thresholds of adults. 14 -19 With the caveat that some studies may have been conducted in children who attended the clinics for other conditions or underwent surgical procedures that may have affected the outcome of the blood values. Minor surgical procedures in children under nitrous oxide anesthesia, for example, can already influence the results in B12, methylmalonic acid (MMA), and homocysteine levels. 20,21
Current diagnostic criteria, aligned with those for adults, overlook substantial age-related variations in B12 levels observed in healthy young individuals. The average values for children aged 10 to 13 years are at least twice as high as for adults 14 -18,22,23 (Table 1).
Monsen et al, 2003: Cobalamin Status and Its Biochemical Markers Methylmalonic Acid (MMA) and Homocysteine in Different Age Groups from 4 Days to 19 Years.
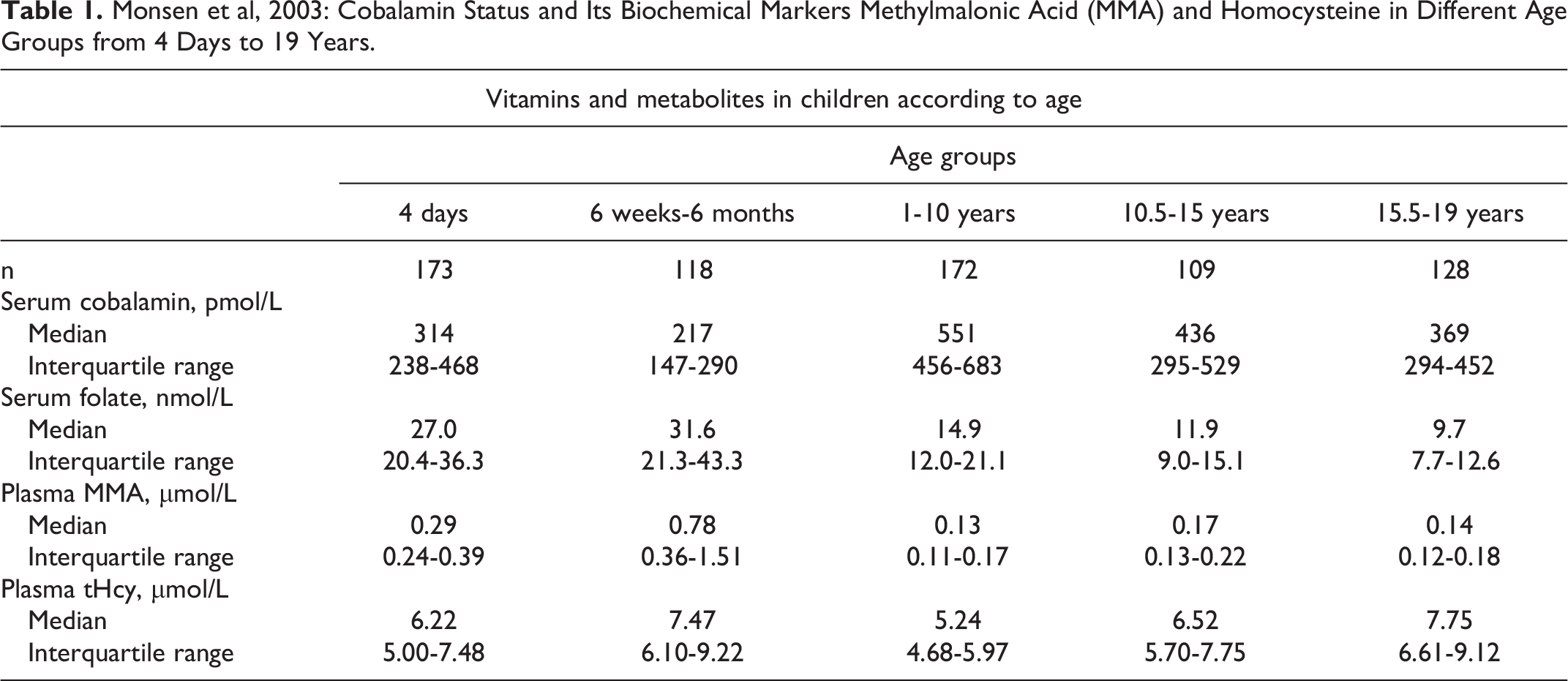
This disparity underlines the pressing need for adjusted diagnostic parameters to effectively address these distinctions and minimize the long-term health implications, thereby reducing distress and health care costs. Highlighted by 2 comprehensive cases, this manuscript emphasizes the importance of updated protocols in managing the diagnosis of B12 deficiency in the younger population.
Case 1: Female, 17 Years Old, Residing With Her Parents
Background
A 17-year-old female student was referred to the B12 Institute by her general practitioner (GP). The patient’s medical history unveiled a progression of symptoms over the past 5 years, commencing with childhood fatigue, which hampered her daily activities. After menarche at age 12, the fatigue worsened, and she developed a concentration difficulty. The menstrual cycle was complicated by heavy bleeding, abdominal pain, and pronounced fatigue, often leading to school absences. These symptoms persisted, impacting her school performance and energy levels. There was minimal engagement in hobbies and social outings and a need for frequent rest periods during the day. The patient showed minimal physical activity due to post-exertion exhaustion. Her diet is balanced and nonvegetarian, and she reported no allergies. Family history revealed B12 deficiency in the patient’s mother and aunt.
Symptoms
Initial complaints included fatigue, pallor, sensitivity to cold, leg pain, eczema, headaches, menstrual distress, poor sleep, periodic flu-like symptoms, dizziness, psychological distress including depression, anxiety, irritability, auditory hallucinations, and concentration difficulties. Neurological manifestations such as leg muscle cramps, tingling sensations in the feet and lower legs, and skin numbness in the lower limbs were reported. Attempts to alleviate psychological symptoms with medication worsened her overall well-being. Commencement of the use of the contraceptive pill as a treatment for the heavy menstrual bleeding and dysmenorrhea further exacerbated her psychological distress.
Laboratory Findings
Serial laboratory assessments displayed fluctuating low-normal B12 levels over the years, decreasing to 169 pmol/L in December 2021 and a low holo-transcobalamin (holoTC) (Table 2). However, according to the GP and the psychiatrist, the results of the markers did not prompt treatment due to normal MMA levels, as indicated by the laboratory, despite a suboptimal holoTC level, which supported a functional B12 deficiency (Table 2). Further blood tests conducted in 2022 indicated a slight increase in B12 levels to 192 pmol/L, but still low for her age (Table 1), an increase in homocysteine to 10.8 μmol/L, and various other values within the normal range despite persisting anemia.
Blood Measurements Taken in B12 Institute.
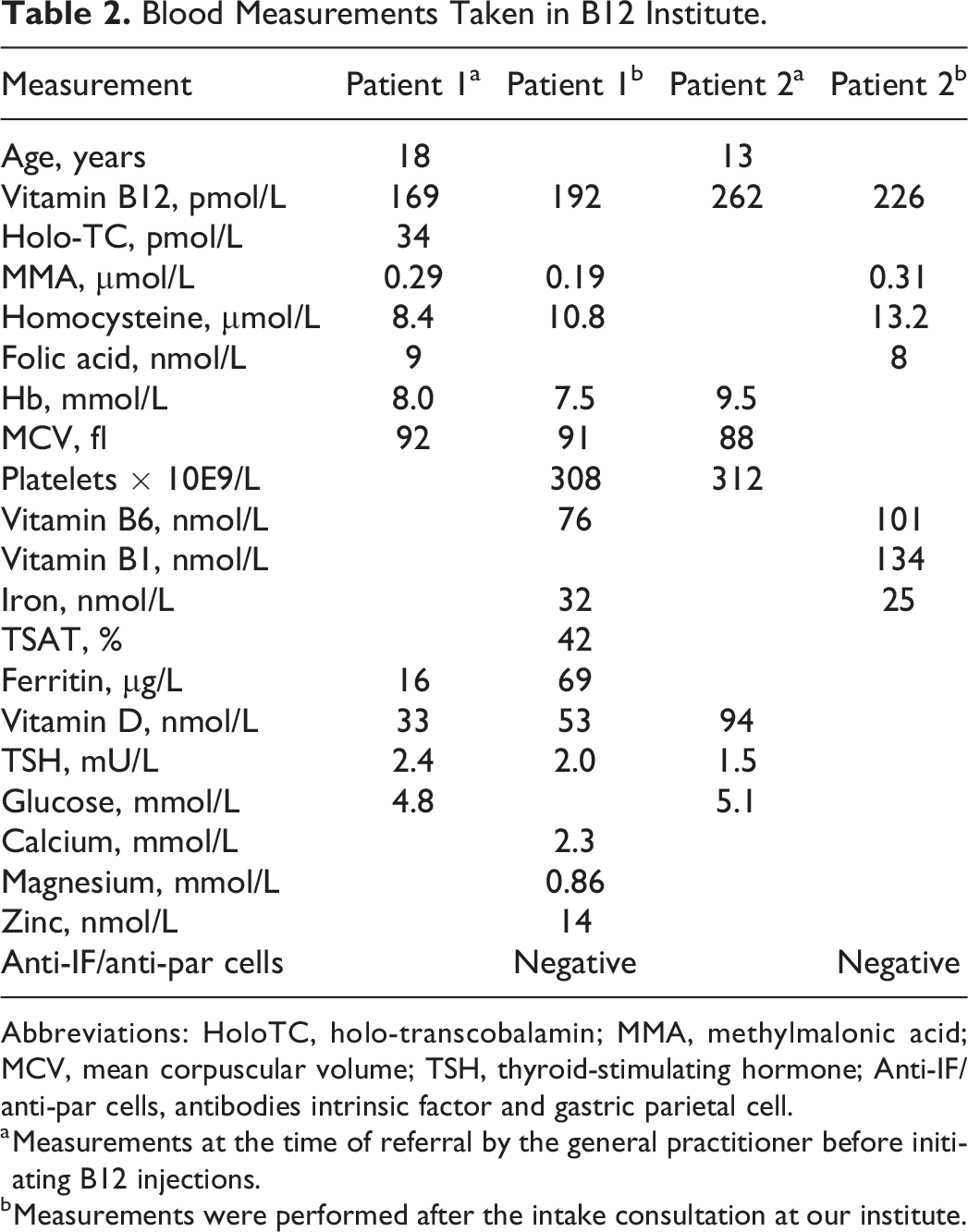
Abbreviations: HoloTC, holo-transcobalamin; MMA, methylmalonic acid; MCV, mean corpuscular volume; TSH, thyroid-stimulating hormone; Anti-IF/anti-par cells, antibodies intrinsic factor and gastric parietal cell.
a Measurements at the time of referral by the general practitioner before initiating B12 injections.
b Measurements were performed after the intake consultation at our institute.
Conclusion and Treatment
We concluded that there was a prolonged untreated B12 deficiency. Because of the apparent neurological symptoms, treatment with hydroxocobalamin was initiated at a dose of 1000 µg intramuscularly twice a week. 24 -26 After a post-surgery relapse, the injection frequency was intensified following the equivalent of the recently published British Medical Journal (BMJ) guidelines for B12 deficiency treatment (“with severe neurological symptoms: every 48 hours intramuscular (i.m.) injection of hydroxocobalamin 1000 µcg until symptoms disappear”). 27
Present Status
The patient had a substantial improvement in her physical and psychological well-being. There was a substantial rise in energy levels. All neurological symptoms, that is, tingling sensations and dumbness, completely disappeared during the first treatment year. She resumed regular attendance at school and internships, engaged in social activities, and reported significant improvement in her menstrual problems. Psychological symptoms declined, leading to a reduction in medication usage, with no relapses observed. Only her sleep medication was continued.
Case 2: Male, 13 Years
Background
This case involves a 13-year-old boy who presented at our outpatient clinic exhibiting symptoms atypical for his age and developmental stage, alongside a notable familial history of B12 deficiency. His mother had a prolonged history of B12 deficiency despite prior treatment, prompting a referral to our clinic for a second opinion after remaining anemic with persistent physical complaints.
The mother’s B12 deficiency, managed through hydroxocobalamin injections every 6 to 8 weeks, had a potential impact during her pregnancy, where her B12 levels were notably low (156 pmol/L) at 5.5 months’ gestation. After giving birth to her son, after 39.1 weeks of pregnancy, the child weighed 3350 grams. She breastfed her infant for 9 months and gradually introduced him to solid food following national guidelines. When he was 3, he began displaying behavioral and physical anomalies.
Symptoms
Early behavioral issues encompassed anxiety, specific food aversions, and urinary concerns. He also presented with a history of intestinal problems, sensory disturbances, delayed speech, and, by the age of 11, progressed to severe fatigue, difficulty sleeping, migraines, muscle pain, abdominal pain, digestive disturbances, and heightened sensory reactions. These symptoms led to the discontinuation of sports activities in which he excelled, such as taekwondo and football.
Family History
The family history indicated multiple autoimmune conditions within the family, including Hashimoto’s thyroid disease, vitiligo, and rheumatic disorders in the boy’s mother, uncle, and grandmother, suggesting a potential familial genetic predisposition to autoimmunity.
Laboratory Findings
Serial B12 assessments showed fluctuating but suboptimal levels over time, supporting the clinical suspicion of B12 deficiency. Other associated markers, such as MMA and tHcy, also aligned with the diagnosis (Table 2, Table 1 used for references).
Treatment and Outcome
Following a comprehensive evaluation involving family history, symptoms, and laboratory outcomes, a treatment plan commenced with hydroxocobalamin injections i.m. of 1000 µg twice a week, closely monitoring associated nutrient levels. Additional measures included dietary adjustments, vitamin D supplements, and a low-dose prescription of valproic acid to manage migraines.
Present Status
After 2 years of treatment, the 16-year-old patient has significantly improved all symptoms. On a maintenance dose of hydroxocobalamin 1000 µg, once every 48 hours, he reports enhanced school performance, diminished mood swings, resolution of sleep and abdominal pain, digestive disturbances, and a gradual improvement in fatigue. While not engaging in sports, he has resumed outdoor activities, such as cycling, and shows typical teenage interests without significant physical or academic limitations. The patient chose not to reduce to fewer injections given his good functioning and virtually complaint-free state after suffering severe migraine attacks with auras, loss of strength in limbs, and underlying hereditary burden. The neurologist advised also against reducing the number of injections the patient was receiving. Overall, he presents as a content and thriving adolescent.
Discussion
Due to significant fluctuations in specific psychomotor development and the constraints of diagnostic tests employed in this age category, minor neurological symptoms like tremors or twitching, as well as slight developmental delays might not be noticed as abnormal in young infants and, therefore, a B12 deficiency can be easily overlooked. 13 If not addressed, a lack of vitamin B12 can cause severe and debilitating symptoms in adults and children. Because the average B12 levels in healthy children significantly differ from those in adults, establishing specific cutoff points as a diagnostic tool for children with B12 deficiency is crucial for accurate diagnosis and treatment (Table 1).
Conclusion and Recommendations
Children can develop a B12 deficiency with serious health consequences. Early diagnosis and treatment are, therefore, essential to prevent severe symptoms. Vitamin B12 values and the connected metabolites have been established by analyzing blood samples from healthy children. Because B12 deficiency in children is not rare, a protocol with revised diagnostic tools based on B12, MMA, holoTC, and homocysteine values determined in healthy children should be developed as soon as possible to prevent the possibility of missing a diagnosis with resulting severe and perhaps permanent complications. Until then, consider using the published average values that have already been established as diagnostic tools and implement them into clinical practice. Suppose there are risk factors for a B12 deficiency in the form of a positive family history of B12 deficiency (or another autoimmune disease), and the patient presents with symptoms; in that case, treatment can be considered analogous to the Dutch LESA or Landelijke Eerstelijns Afspraak (transl.: National Primary Care Agreement) protocol to avoid an expensive MMA determination. 25 Also, therapy is recommended analogous to guidelines from the British Committee for Standards in Hematology and the new vitamin B12 protocol published in the BMJ. 27,28
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241252850 - Vitamin B12 Deficiency in Children and Adolescents: A Case for Revised Diagnostic Parameters
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241252850 for Vitamin B12 Deficiency in Children and Adolescents: A Case for Revised Diagnostic Parameters by Clara H. M. Plattel, Sandra Lever, Charlotte P. M. Simons and Vera Haitsma in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.