
Abstract
Background:
Latin American countries have shifted from traditional diets rich in micronutrients to a Westernized diet rich in high energy-dense foods and low in micronutrients.
Objective:
This study aimed to determine the prevalence of adequate micronutrient intakes in urban populations of 8 Latin American countries.
Method:
Micronutrient dietary intake data were collected from September 2014 to August 2015 from 9216 men and women aged 15.0 to 65.0 years living in urban populations of 8 Latin American countries. Dietary intake was collected using two 24-hour recalls on nonconsecutive days. Micronutrient adequacy of intake was calculated using the Estimated Average Requirement cut-off method.
Results:
In general terms, the prevalence of inadequate intake of thiamine, riboflavin, niacin, folate, cobalamin, iron, phosphorus, copper, and selenium ranged from 0.4% to 9.9%. In contrast, the prevalence of inadequacy of pyridoxine, zinc, vitamin C, and vitamin A ranged from 15.7% to 51.5%. The nutrients with a critical prevalence of inadequacy were magnesium (80.5%), calcium (85.7%), and vitamin D (98.2%). The highest prevalence of inadequate intakes was observed in the low educational level, participants with overweight/obesity, in men, and varies according to socioeconomic status.
Conclusions:
There is an urgent need to define direct regional actions and strategies in Latin America aimed at improving micronutrient adequacy, either through staple food fortification programs, agronomic biofortification, or food policies that facilitate economic access to micronutrient-rich foods.
Plain language title
Description of the Vitamin and Mineral Consumption Status in Urban Cities of Latin America: Results of the Latin American Health and Nutrition Study.
Plain language summary
Vitamins and minerals are essential for maintaining good health. However, traditional Latin American diets are changing to include foods that have a lot of sugar and fat but fewer vitamins and minerals. This study was designed to analyze the consumption of these nutrients in urban cities of 8 Latin American countries. We collected food consumption information from September 2014 to August 2015 from 9216 men and women between 15 and 65 years old using a method called 24-hour recall. To find out if participants were consuming the necessary daily amounts of vitamins and minerals, intakes were compared with the daily recommended amounts suggested by the Institutes of Medicine of the United States. We found that Latin American urban populations consume fewer vitamins and minerals than recommended. In some cases, few people do not consume the required amounts of vitamins and minerals, but in other cases, many do not. For example, few do not consume enough thiamine, riboflavin, niacin, folate, cobalamin, iron, phosphorus, copper, and selenium. However an intermediate number of people do not consume enough pyridoxine and zinc, a high number consume little vitamin C and vitamin A, and many people consume very little magnesium, calcium, and vitamin D. We found that the people who consume fewer vitamins and minerals are mostly males, overweight/obese, have lower education and varies according to their financial resources. A deficient intake of vitamins and minerals showed up in most age groups, from adolescence to adulthood. To improve vitamins and minerals intake, it is important that some foods that are frequently eaten are fortified or that the price of foods that are high in vitamins and minerals is lowered.
Introduction
Micronutrients play a vital role in several biological functions and have implications on key metabolic processes in the body. 1 The deficiency of micronutrients has been linked to a wide range of adverse outcomes that can affect all life stages, such as birth defects, growth retardation, and impaired cognition. It can also exacerbate infectious and chronic diseases, greatly impacting morbidity, mortality, and quality of life. 2
Adequate micronutrient intake is a key element of diet quality. However, in the last decades, food environments in Latin American countries (LAC) have been undergoing various changes associated with demographic, epidemiologic, and nutrition transitions. 3 The consumption of traditional diets has decreased mainly in urban areas, shifting to a greater intake of energy, foods of animal origin, refined carbohydrates, added sugars, and salty foods, and a lower intake of legumes, vegetables, and fruits. 3 -5 As such, this modern food environment may impact the adequate intake of micronutrients in LAC, because: (1) energy-dense foods are low in micronutrients, 3 (2) the consumption of ultra-processed foods reduces dietary diversity and micronutrient intake, 6 and (3) the high added-sugar intake promotes micronutrient dilution. 7
Disparities in micronutrient intake related to socioeconomic status (SES) may also occur in different sectors of the Latin American population, further complicating the picture of adequate micronutrient intake in the region. In Latin America, the largest proportion of the population lives in urban areas 8 ; however, migration to urban areas shifted the location of global poverty to cities, triggering the process known as the “urbanization of poverty.” 9 Several studies conducted mainly in developed countries have found a positive association between SES and micronutrient intake, 10 but this association is still well understudied in middle-income countries. 10 Data from Brazil and Guatemala, among other LAC, show that the prevalence of inadequate micronutrient intakes declined with increasing income and educational levels. 11 -15
On the other hand, the literature 16 -18 has shown that many people with obesity have inadequate intakes of iron, calcium, magnesium, zinc, copper, folate, and vitamins A and B12, as a result of poor diet quality. This adds another risk factor for an inadequate intake of micronutrients in LAC, where overweight and obesity are predominant public health issues, 19 mainly in urban areas. 20
Multiple factors associated with the inadequate intake of micronutrients converge in the Latin American region can lead to significant disparities in dietary intake of these nutrients in various population groups. Therefore, this study aimed to determine the prevalence of adequate micronutrient intakes in 15- to 65-years-old urban populations of 8 LAC.
This study used data derived from the Latin American Study of Nutrition and Health (ELANS), a multicenter cross-sectional survey originally designed to collect information on food and nutrient intake, nutritional status, and physical activity levels of nationally representative samples of urban populations of 8 LAC with regional human development indices ranged 1 to 15 (Chile: 1, Argentina: 2, Costa Rica: 3, Peru: 8, Brazil: 10, Colombia: 11, Ecuador: 12, and Venezuela: 15). 21 Results of the present study might help to lead public health policies in LAC countries with low development indices, in which the epidemiologic transition is in its early stages.
Methods
Study Design and Sampling
The study design and sampling are described in detail elsewhere. 22 Data were collected from September 2014 to August 2015. All participants <18-years-old provided a written informed assent and asked to obtain signed informed consent from their parents if they were interested in participating in the study. Adult participants gave their written informed consent. The Western Institutional Review Board (#20140605) approved and registered the ELANS protocol at ClinicalTrials.gov (#NCT02226627).
Data Collection
Demographic and SES variables
A questionnaire was used to collect data on sex, age, and years of education. A standard 3-level system was developed to categorize the educational level (none, low for primary school complete and incomplete, medium for secondary school complete and incomplete, and high for university studies or superior). 23 Socioeconomic status was evaluated using a country-dependent questionnaire based on the legislative requirements or established local standard layouts and classified into low, middle, and high status, based on the national indexes for each country. 24
Anthropometric assessment
Height and weight, measured by trained nutritionists following standardized procedures, 25 were used to calculate the body mass index (BMI). Body mass index for participants younger than 18-years-old was classified according to the percentile or z-score cut-off criterion for age and sex proposed by the World Health Organization (WHO). 26 For those older than 18-years-old, BMI was classified as underweight BMI <18.5 kg/m2, normal weight BMI 18.5-24.99 kg/m2, overweight BMI 25.0-29.9 kg/m2, and obese BMI ≥30.0 kg/m2. 27
Dietary intake
Dietary intake was collected by trained interviewers during 2 face-to-face household visits, using 24-hour recalls (24 h) on two nonconsecutive days, with an interval of up to 8 days between them, including both weekdays and weekend days. All local and traditional foods reported were harmonized with a USDA composition table considering the nutritional equivalency 28 and mandatory food fortification was taken into consideration according to each country’s legislation. Energy and micronutrient quantities were obtained, using the Nutrition Data System for Research (NDS-R) software version 2014. 29
Data Analyses
Nutrient usual intake analysis
The Multiple Source Method (http://mss.dife.de/tps/en) 30 was used to estimate the usual intake of 9 vitamins (thiamin [vitamin B1], riboflavin [vitamin B2], niacin [vitamin B3], pyridoxine [vitamin B6], folate [vitamin B9], cobalamin [vitamin B12], vitamin C, vitamin A, and vitamin D), and 7 minerals (calcium, iron, zinc, phosphorus, magnesium, copper, and selenium) to calculate the nutrient adequacy ratio (NAR). In addition, dietary intakes were converted to nutrient density (micronutrient intake/1000 kcal per day) to allow comparisons among groups of sex, age, SES, educational level, nutritional status, and countries. This was performed to avoid bias in the estimation of nutrient intake due to its strong association with energy intake.
Micronutrient adequacy
The NAR was calculated for the intake of 16 micronutrients. For each nutrient, the NAR is the ratio of a subject’s intake to the estimated average requirement (EAR) for the corresponding sex and age-group, according to the guidelines of the National Academy of Medicine (NAM) of the United States. 31 NAR values higher than 1 were truncated at 1, so a nutrient with a high NAR could not compensate for a nutrient with a low NAR. 32 Participants with a NAR value for a specific nutrient lower than 1 were considered with nutrient inadequacy of this nutrient. The EAR is the appropriate dietary reference intake to use when assessing the adequacy of group intakes. The micronutrient adequacy was calculated using the cut-point method. 33

The EAR cut-point method was used because all the assumptions the Institute of Medicine (IOM) indicated for its use were met. 34
Since the proportion of participants with usual dietary intake of micronutrients reaching the Upper Level was below 1.0%, this issue was not reported in this article.
Statistical analyses
Data were reported as means ± standard deviations (SD) for continuous variables and frequencies (%) for categorical variables. The normal distribution of continuous variables was assessed with the Shapiro-Wilk test. Between-sex comparisons in the proportions of participants by age-group, country, SES, educational level, and nutritional status were tested using the Chi-square test with the Bonferroni post hoc test when required. Likewise, the prevalence of nutrient inadequate intake by age-group, SES, educational level, and nutritional status were stratified by sex; and the differences among groups were tested using the Chi-square test with Bonferroni post hoc test. The energy intake comparisons among groups were tested using the Kruskal-Wallis test with a pairwise comparison post hoc test and Bonferroni correction for multiple comparisons. It is important to acknowledge that a collinear relation may exist between the variables SES and educational level. However, collinearity between these variables was not assessed given the scope of this study was mainly descriptive, and it did not aim to predict inadequate intake of micronutrients according to sociodemographic variables.
All tests were two-tailed, and P values < .05 were considered statistically significant. Data were analyzed using STATA software (version 14.1, 2015, College Station, TX, USA) 35 and IBM SPSS® (version 27, IBM Corp). 36
Results
General Characteristics of the Participants
The mean age of the study sample was 35.8 (±14.0) years (y). The highest proportion of participants was in the 20 to 49 y age-group (66.2%). Percentages of participants by age-group were statistically similar between sex categories only in the 20 to 49 y age-group (Table 1). The proportion of men and women was similar in the 8 countries participating in the study. The largest proportion of participants was in the middle (42.8%) and low (41.8%) SES, with low educational level (60.0%) and overweight/obesity (62.5% women and 56.4% men, P < .001).
Characteristics of the Participants in the ELANS Study.
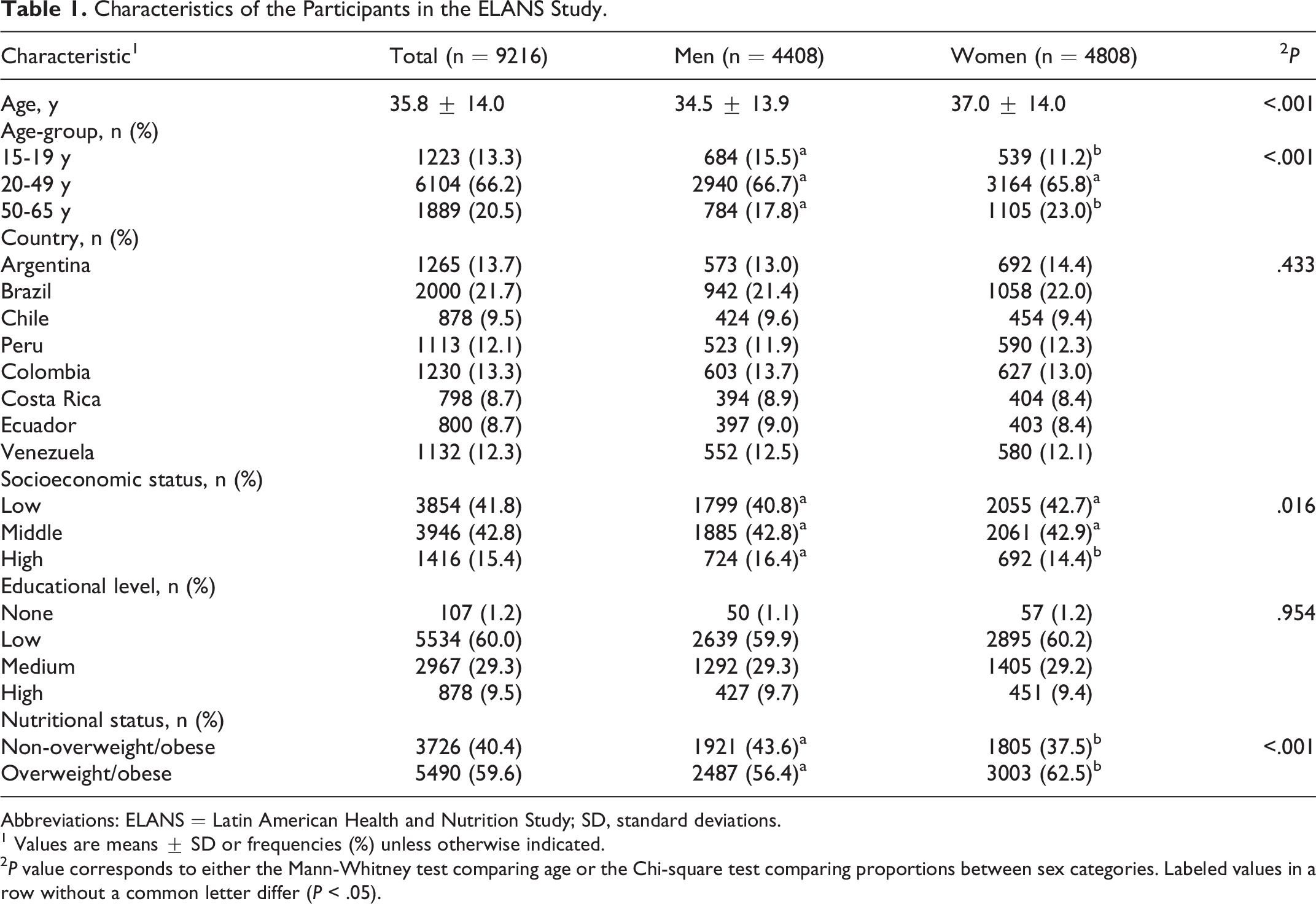
Abbreviations: ELANS = Latin American Health and Nutrition Study; SD, standard deviations.
1 Values are means ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to either the Mann-Whitney test comparing age or the Chi-square test comparing proportions between sex categories. Labeled values in a row without a common letter differ (P < .05).
Micronutrient Intake According to Sex, Age-Group, SES, Educational Level, and Nutritional Status
In general, all the evaluated micronutrients had an inadequate intake, although the severity of the inadequacy varied between nutrients (Table 2). For thiamine, riboflavin, niacin, folate, cobalamin, iron, phosphorus, copper, and selenium, the prevalence of inadequate intake ranged from 0.4% to 9.9%. In contrast, the prevalence of inadequate intake of pyridoxine, zinc, vitamin C, and vitamin A ranged from 15.7% to 51.5%. The nutrients with a critical prevalence of inadequacy were magnesium (80.5%), calcium (85.7%), and vitamin D (98.2%) (Table 2). Similar results were found when micronutrient analyses were performed for each participant country in the study (Supplementary Material: Table S1).
Usual Daily Intake of Micronutrients by 1000 kcal and Prevalence of Inadequate Intakes in the ELANS Study and According to Sex.
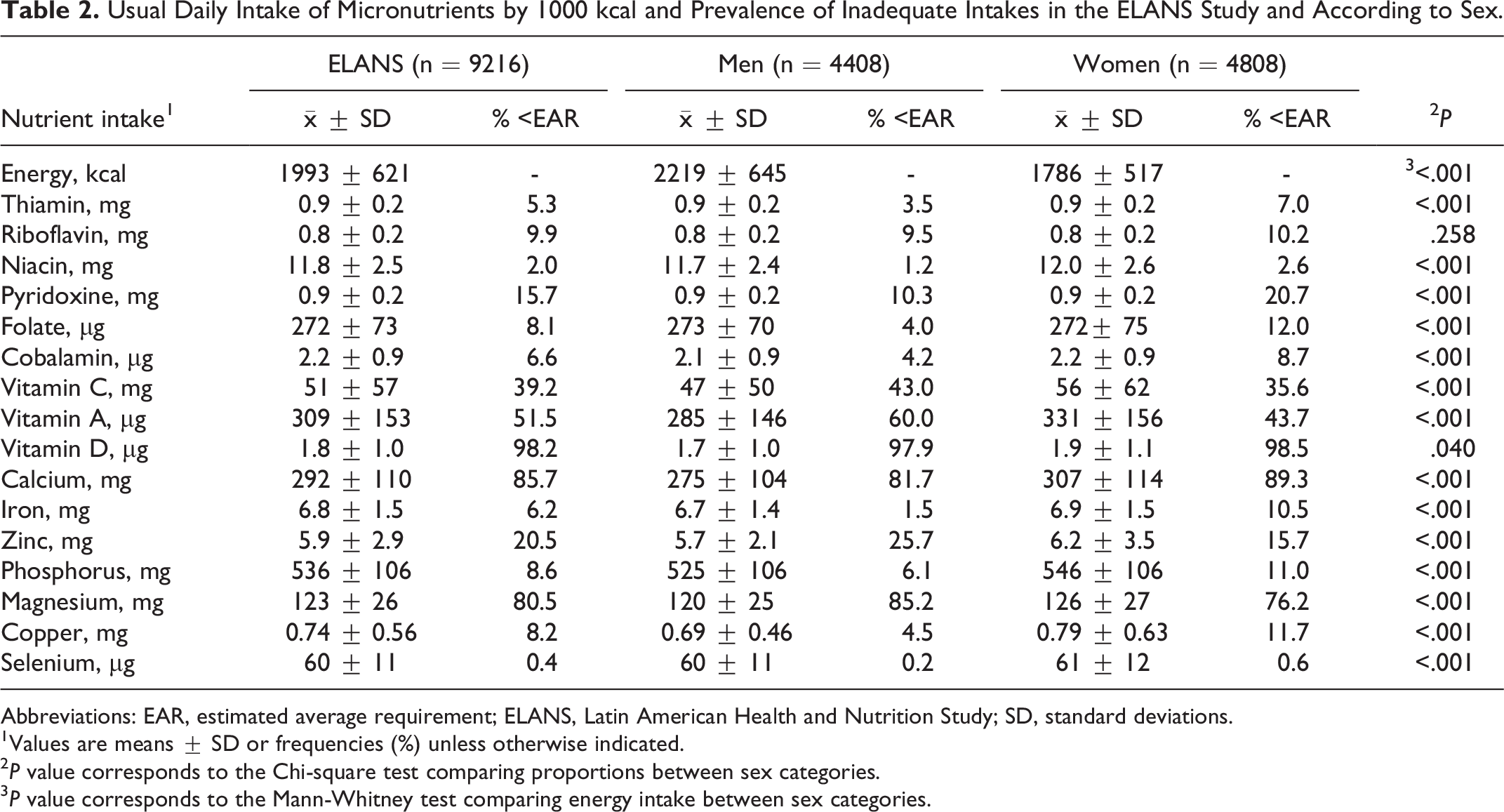
Abbreviations: EAR, estimated average requirement; ELANS, Latin American Health and Nutrition Study; SD, standard deviations.
1Values are means ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to the Chi-square test comparing proportions between sex categories.
3 P value corresponds to the Mann-Whitney test comparing energy intake between sex categories.
Differences in the prevalence of inadequate intakes for all nutrients were statistically significant between sexes (P < .05), except for riboflavin. The prevalence of inadequate intake of zinc, magnesium, and vitamins C and A was higher in men than in women. On the contrary, inadequate intake of vitamin D and calcium was higher in women than in men (Table 2).
Table 3 shows the analysis of micronutrient adequacy by sex and age-group. In adolescent boys, the prevalence of inadequate intake of riboflavin (28.2%) and calcium (88.7%) was significantly higher (P < .001) than that observed in men aged 20 to 49 years (6.9% and 80.3%, respectively) and in those aged 50 to 65 years (2.9% and 80.6%, respectively). In contrast, the prevalence of inadequate intake of zinc (34.3%), vitamin C (45.9%), and magnesium (89.5%) was significantly higher in men aged 50 to 65 years than in younger men. In general, the mean prevalence of inadequate intakes of vitamins A and D in men was 60.0% and 97.9%, respectively, with no significant differences between age groups.
Usual Daily Intake of Micronutrients by 1000 kcal and Prevalence of Inadequate Intake According to Sex and Age-Group.
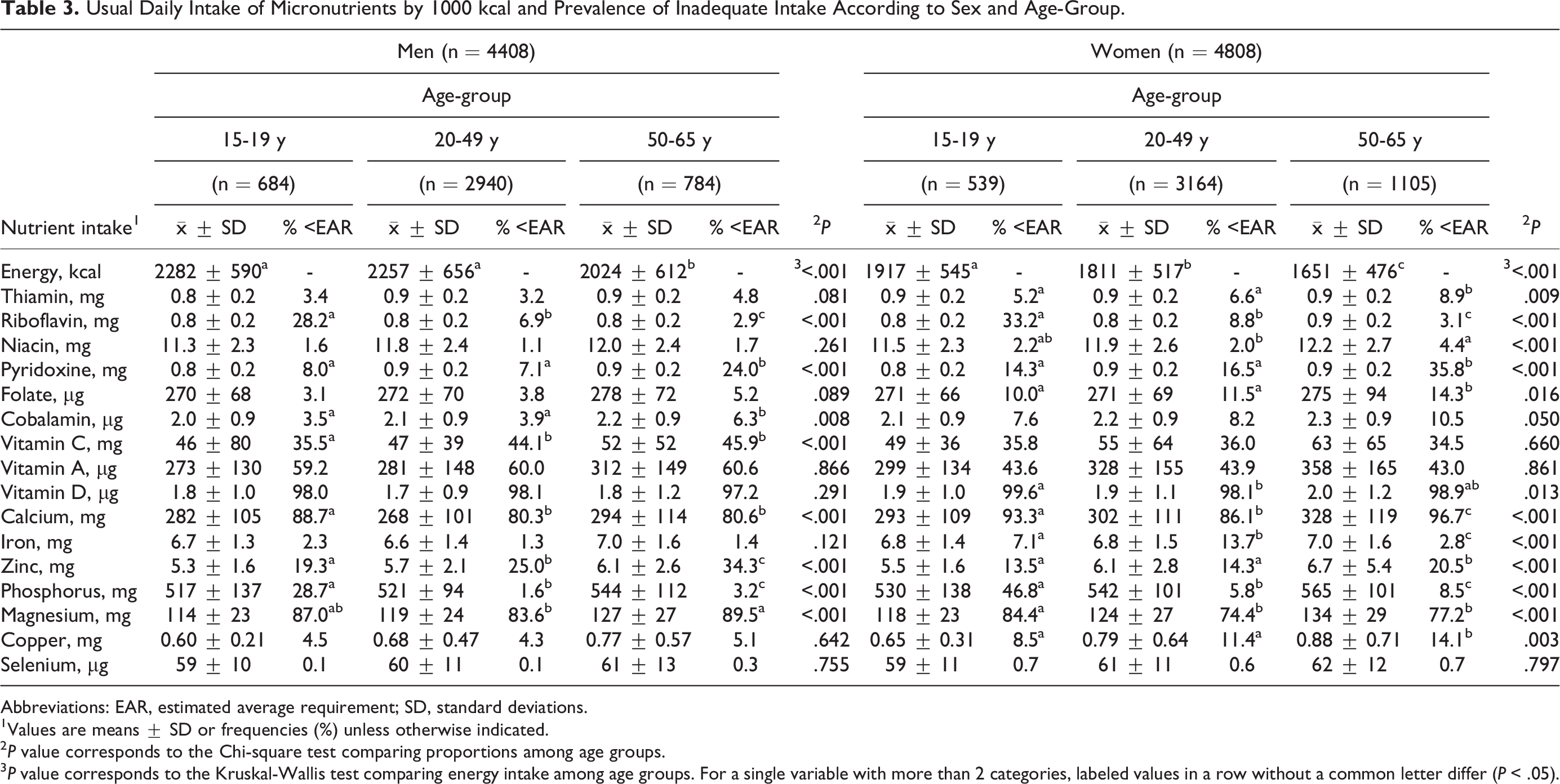
Abbreviations: EAR, estimated average requirement; SD, standard deviations.
1Values are means ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to the Chi-square test comparing proportions among age groups.
3 P value corresponds to the Kruskal-Wallis test comparing energy intake among age groups. For a single variable with more than 2 categories, labeled values in a row without a common letter differ (P < .05).
The prevalence of inadequate intake of riboflavin (33.2%), phosphorus (46.8%), magnesium (84.4%), and vitamin D (99.6%) was higher for adolescent girls than for women aged 20 years and older. In contrast, the inadequate intake of calcium (96.7%), pyridoxine (35.8%), zinc (20.5%,) and folate (14.3%) was significantly higher in women aged 50 to 65 years than in those under 50 years of age. On average, the prevalence of inadequate intake of vitamins A and C in women was 43.7% and 35.6%, respectively, with no significant differences between age groups. Regardless of age-group, the prevalence of inadequacy of vitamin D, calcium, and magnesium in both men and women was remarkably high.
Table 4 shows the prevalence of inadequate intake of micronutrients according to sex and SES. The prevalence of inadequate calcium intake was significantly higher (P < .001) in men with high SES (85.4%) compared to men with middle (81.3%) and low (80.5%) SES. In contrast, inadequate intake of vitamins C and D was significantly higher in men with low SES; however, vitamin D insufficiency ranged from 98.5% for low SES to 98.1% for high SES. The prevalence of inadequate intake of vitamin A and magnesium for men in the 3 SES levels was around 60% and 85%, respectively, with no significant differences between them.
Usual Daily Intake of Micronutrients by 1000 kcal and Prevalence of Inadequate Intake According to Sex and SES.
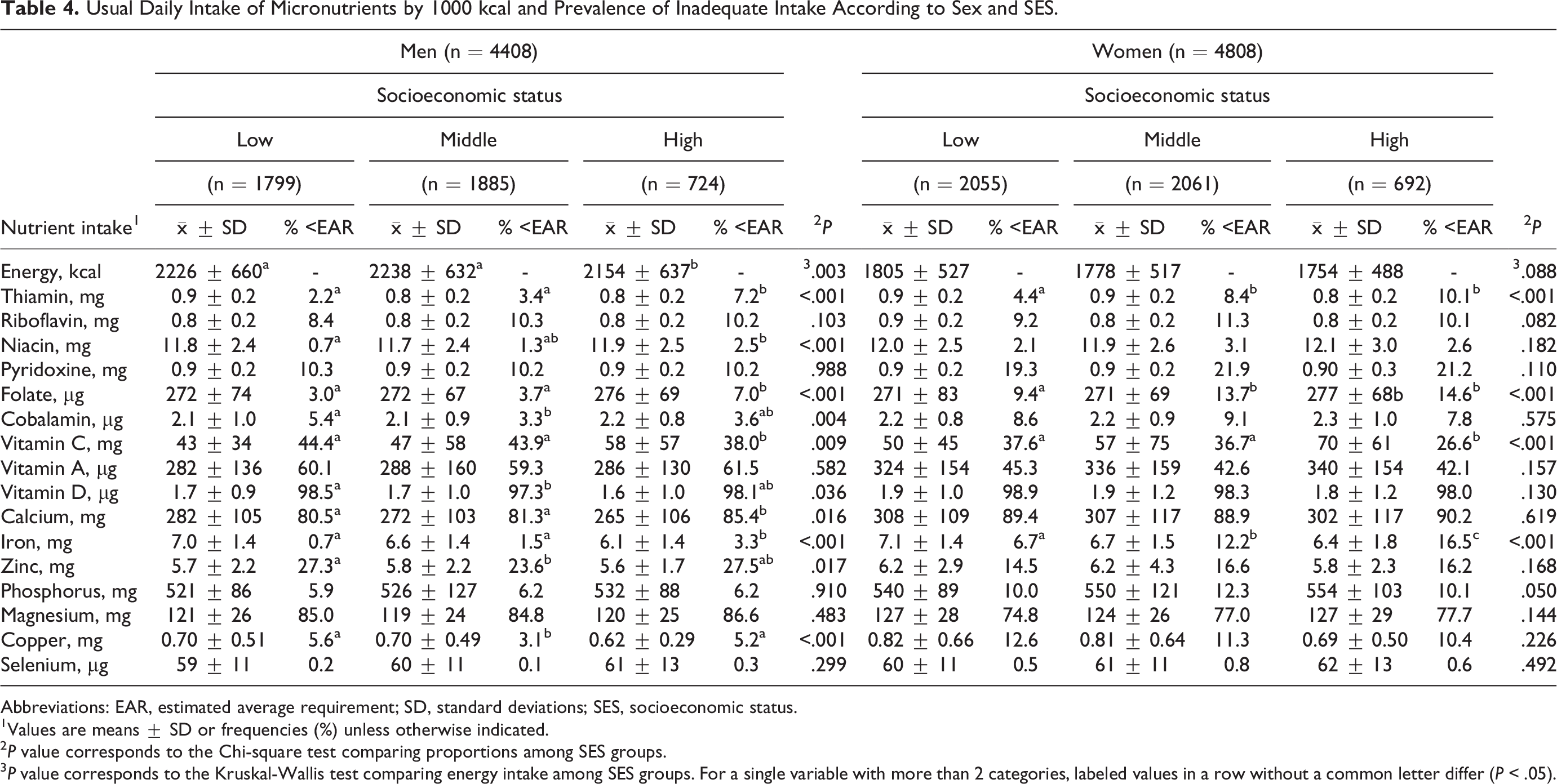
Abbreviations: EAR, estimated average requirement; SD, standard deviations; SES, socioeconomic status.
1Values are means ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to the Chi-square test comparing proportions among SES groups.
3 P value corresponds to the Kruskal-Wallis test comparing energy intake among SES groups. For a single variable with more than 2 categories, labeled values in a row without a common letter differ (P < .05).
In women with high SES, the inadequate intake of vitamin C (26.6%) was significantly lower than in women with middle (36.7%) and low (37.6%) SES. However, the highest prevalence of inadequate iron intake was observed in women with high SES (16.5%) and the lowest in those with low SES (6.7%). Likewise, a higher inadequate intake of folate was evidenced in women with high SES than in those with low SES (14.6% and 9.4% respectively, P < .001). Inadequate intakes of vitamin A, vitamin D, calcium, and magnesium in women were similar in the 3 SES levels. However, the prevalence of inadequate intake of these nutrients was considerably high, ranging from 42.1% (for vitamin A) to 98.9% (for vitamin D).
When analyzing the adequacy of micronutrient intake by educational level (Table 5), the prevalence of inadequate intake of vitamin C, vitamin A, vitamin D, calcium, and zinc was significantly higher (P < .001) in the participants with a lower educational level (none or low) than in those with a medium or high educational level. Zinc inadequacy was higher in men and women, included in the “none” educational category than in those in the low educational level. Inadequate intakes of vitamin D were similar in both men and women regardless of educational level, ranging from 100% for those included in the “none” educational category to around 98% for those with a high educational level. Inadequate magnesium intakes were similar in men of all educational levels, ranging from 90% for those included in the “none” educational category to 84.1% for those with a high educational level. In the case of women, the prevalence of magnesium inadequacy was significantly higher for those included in the “none” educational category than in women with a high educational level (86% and 68.5%, respectively, P < .001). Regardless of educational level in both men and women, inadequate intakes of vitamin A, vitamin D, calcium, and magnesium were remarkably high. Additionally, inadequate intakes of vitamin C and zinc were high in participants included in the “none” educational category.
Usual Daily Intake of Micronutrients by 1000 kcal and Prevalence of Inadequate Intake According to Sex and Educational Level.
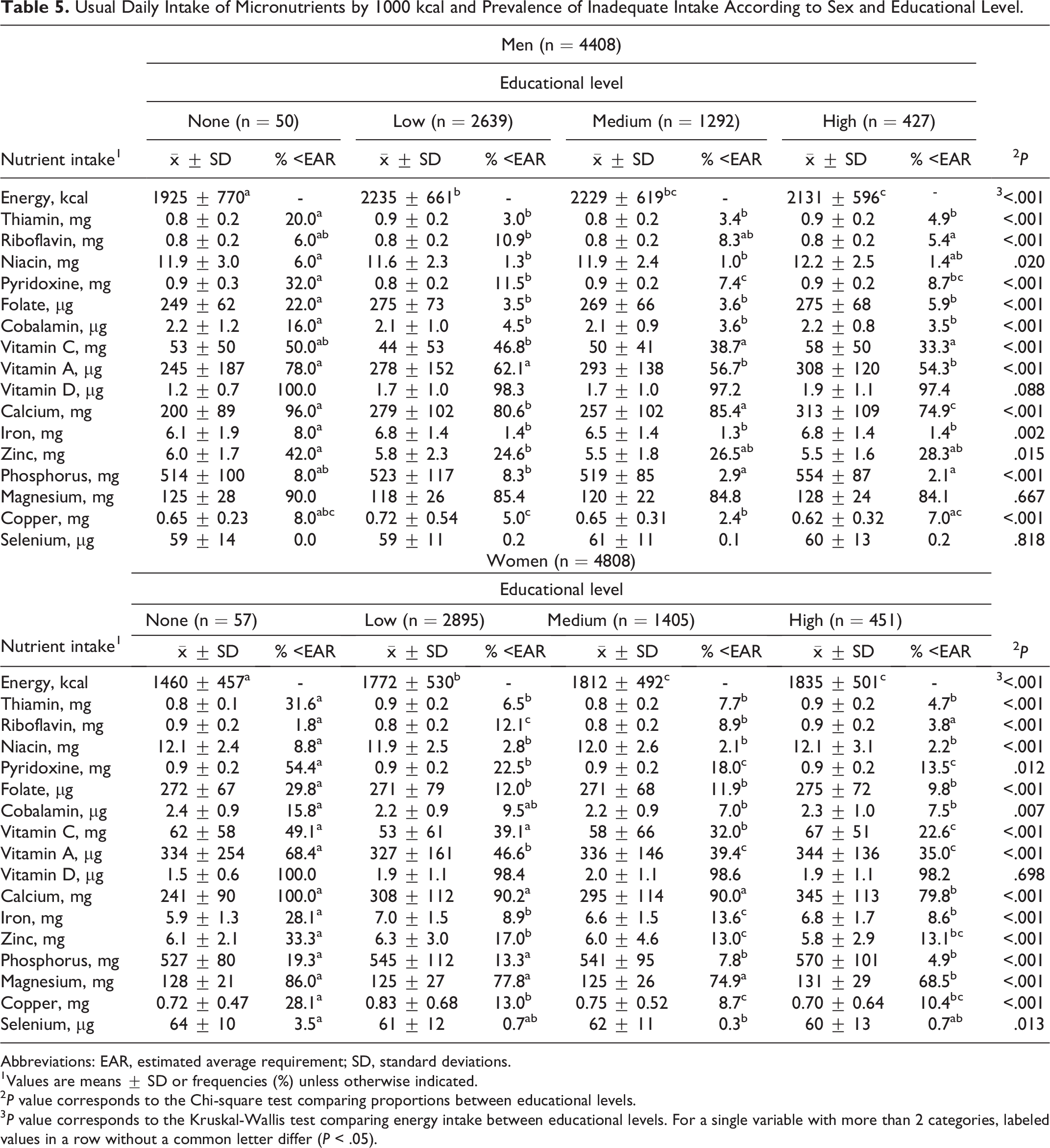
Abbreviations: EAR, estimated average requirement; SD, standard deviations.
1Values are means ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to the Chi-square test comparing proportions between educational levels.
3 P value corresponds to the Kruskal-Wallis test comparing energy intake between educational levels. For a single variable with more than 2 categories, labeled values in a row without a common letter differ (P < .05).
The prevalence of inadequate intakes of pyridoxine (12.0%), vitamin C (44.8%), vitamin A (62.6%), and magnesium (87.1%) was higher in overweight/obese men than in those without this nutritional status (Table 6). The prevalence of inadequate intakes of vitamin A and calcium did not vary according to the nutritional status of men. However, the prevalence of inadequate intake of calcium and vitamin D was very high (close to 80% and 98%, respectively) in both obese and non-obese men.
Usual Daily Intake of Micronutrients by 1.000 kcal and Prevalence of Inadequate Intake According to Sex and Nutritional Status.
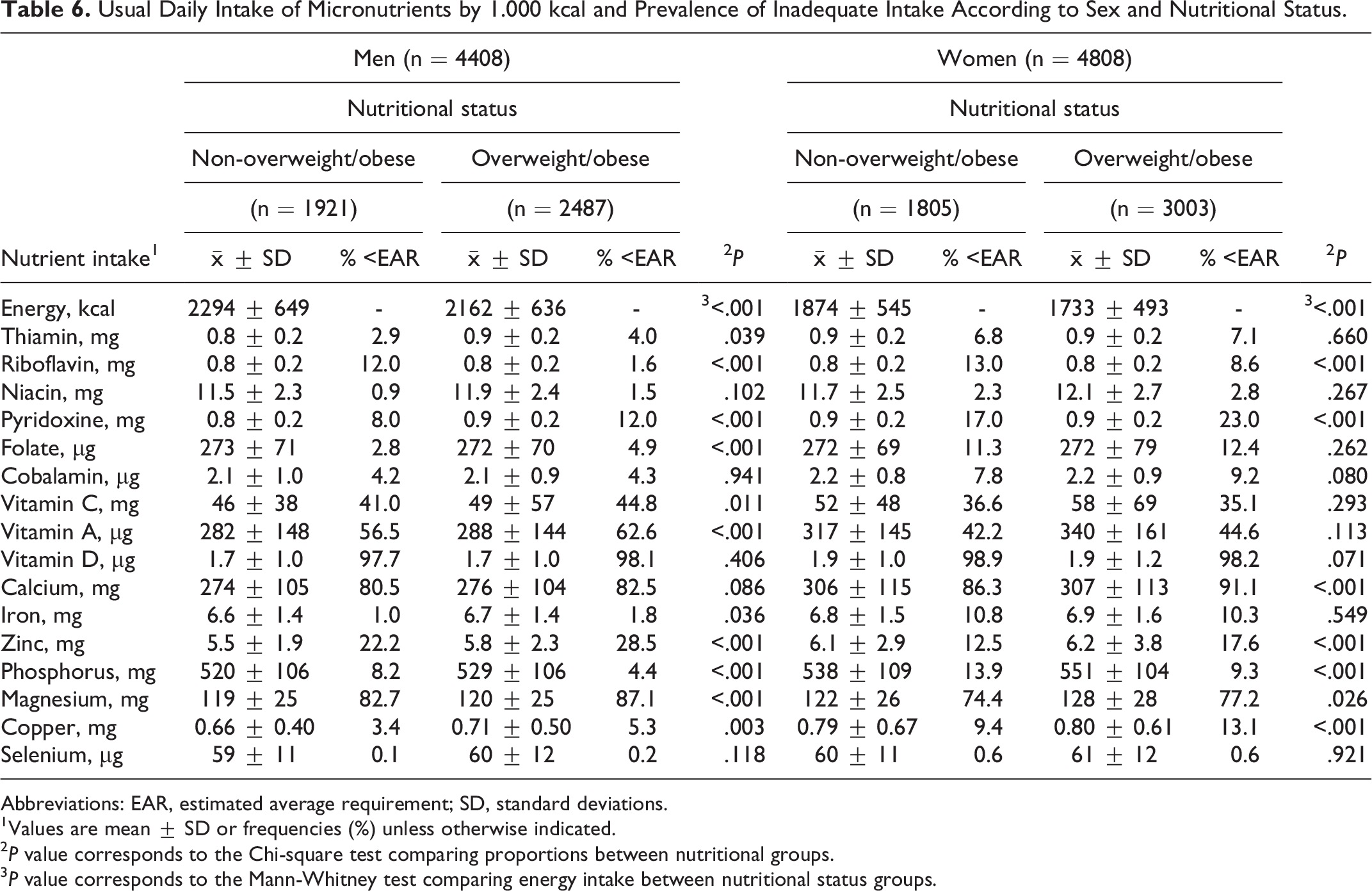
Abbreviations: EAR, estimated average requirement; SD, standard deviations.
1Values are mean ± SD or frequencies (%) unless otherwise indicated.
2 P value corresponds to the Chi-square test comparing proportions between nutritional groups.
3 P value corresponds to the Mann-Whitney test comparing energy intake between nutritional status groups.
Overweight/obese women had higher inadequate intakes of vitamin A (44.6%), calcium (91.1%), and magnesium (77.2%) than non-overweight/obese women. The prevalence of inadequate intakes of vitamins C, A, and D was similar in women, regardless of nutritional status. However, the inadequate intake of vitamin D was greater than 98%.
Discussion
Our results showed that micronutrient intake in urban areas of LAC fails to meet the recommendations for the majority of nutrients. Although the prevalence of inadequate intake is quite low for some nutrients, it is alarmingly high for others. Differences in inadequate micronutrient intake between men and women may reflect gender variations associated with gender stereotypes about food. However, as this study did not collect information on that specific topic, there are no arguments to explain these results. Future analyses of the influence of psychosocial aspects on the different micronutrient intakes between men and women may provide inputs that can guide the design of strategies to improve public health. 37
Variations in micronutrient intakes according to SES have been widely documented globally, 10,38 as diet cost is a mediator of the relationship between SES and micronutrient intake. 39 In addition, a displacement of micronutrient-rich foods by ultra-processed foods has been documented, mainly when SES increases. 6,40 Likewise, educational level generates significant disparities in micronutrient intakes. Early childhood education is not only a determining factor in future employment and income but it also affects the ability to understand and implement dietary guidance messages and risk-reducing dietary behaviors. 41 Because educational level has been generally recognized as a proxy of SES, 42 -44 it is possible that collinearity between these variables exists, but this was not significant for this study given the descriptive scope of it. In light of this, future studies including multivariate analysis aiming to predict the effect of sociodemographic variables on nutrient intakes should consider this possible collinearity.
Inadequate intake of micronutrients in overweight/obese people can have important repercussions for their health. Micronutrients are involved in the regulation of fat, carbohydrate, and protein metabolism, and as such, micronutrient deficiency worsens the course of obesity and further exacerbates the deficit. 45 This is of particular concern in Latin America where there is an epidemic of overweight/obesity.
Inadequate Intake of B-vitamins
Latin America has a long history of fortification policies and programs aimed at eradicating deficient micronutrient intakes. 46,47 The low prevalence of inadequate intakes of thiamine, riboflavin, niacin, and folate in urban areas may be a reflection of these policies. The fortification of wheat flour with thiamine, riboflavin, niacin, and folate is mandatory in the 8 countries included in the study. 48 In addition, other countries also fortify corn flour (Costa Rica) and rice (Costa Rica, Peru, and Venezuela) with these nutrients.
The moderate prevalence of inadequate pyridoxine intakes is consistent with the low intake of legumes, vegetables, and non-citrus fruits observed in urban areas of LAC, 49 suggesting the impact of the nutritional transition in replacing traditional diets. This finding highlights the need for public health initiatives that promote the recommended consumption of those food groups (100 g/day of legumes and 400 g/day of fruits and vegetables). 50,51
Inadequate Intake of Vitamin C
The high prevalence of inadequate vitamin C intake is noticeable in Latin America, where the main sources of this nutrient (fresh fruits and vegetables) are widely available. 52 Unfortunately, a previous study showed that the consumption of both food groups is considerably low in the countries participating in the ELANS. 49 Multiple campaigns and policies have been implemented to encourage fruit and vegetable consumption in LAC, but numerous barriers to intake remain. The high cost of whole fruits and vegetables, particularly fresh produce, is an oft-cited barrier. 14,49,52,53 Furthermore, as has been reported in several studies, 54 -56 the low fruit consumption may be a consequence of its displacement by the consumption of energy-rich and nutrient-poor foods, like ultra-processed foods. Therefore, policymakers should develop targeted nutritional policies to improve access to fruits and vegetables, which are available in all LAC but inaccessible due to cost, especially in populations with low SES and educational level. 49 In addition, public health strategies aimed at reducing the consumption of ultra-processed foods must be promoted, to avoid the displacement of minimally processed food consumption (e.g., fruits and vegetables) by these.
Inadequate Intake of Vitamin A
Although vitamin A intake is not related to serum levels of retinol, 57 it has been shown that inadequate vitamin A intake for 4 months can lead to the depletion of liver reserves and subclinical deficiency. 58 On the other hand, there are no Latin American studies that provide information on the status of serum levels of retinol in adolescents and adults.
The consumption of vitamin A-rich foods (liver, organ meats, and certain fruits and vegetables) is considerably low in urban areas of Latin America. 59 Policymakers should consider the need to fortify staple foods with vitamin A. However, fortification should not only be used as a means to reduce the risks associated with inadequate vitamin A intake in pregnant women and children (as has been done traditionally). 60 Other important biological functions of this vitamin are continually discovered in new fields, such as lipid metabolism, insulin response, cardiovascular disease, and obesity. 61
In Costa Rica, as in other Central American countries, sugar for household consumption has been fortified with vitamin A since the 1960s. 61 Nevertheless, currently, sugar may not be the best fortification vehicle due to the high prevalence of overweight/obesity in Latin America, 19 high sugar consumption in urban areas of LAC, 62 and the strategy of the WHO to reduce the sugar intake to less than 10% of daily total energy intake. 63 Edible oils are an ideal vehicle for vitamin A fortification 64 ; and would encourage the consumption of a healthy fatty acid profile. In the last decade, several countries around the world have initiated mandatory national programs to fortify cooking oil with 15 to 30 µg/g vitamin A. 65 However, the excessive use of fortified edible oils could increase the risk of obesity in the population.
Ideally, before promoting the consumption of sugar or oils fortified with vitamin A, it is necessary to conduct educational campaigns to reduce the consumption of these foods and then adjust fortification levels. In this way, a public health strategy could be established to ensure the adequate intake of vitamin A through the consumption of sugar and fat compatible with the prevention of obesity.
Inadequate Intake of Vitamin D
Vitamin D intake demands urgent and immediate attention from decision-makers due to the very high prevalence of inadequate intakes, which could negatively affect serum levels of 25-hydroxyvitamin D. Low vitamin D status has been associated, although not consistently with an increased risk of type 1 diabetes, cardiovascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy. 66 -69 On the contrary, several studies point out the relevant role of vitamin D in bone health. 70 -73 Dietary vitamin D intake is low in many countries worldwide, especially because very few food sources are rich in this nutrient. 74,75 Mandatory food fortification represents the best opportunity to increase vitamin D intake in the Latin American population, which has been analyzed previously. 75 -78 Unfortunately, in Latin America, no studies have been carried out to determine the potential vehicles for vitamin D fortification.
Vitamin D fortification of foods in the United States and Canada has significantly affected the average daily intake of vitamin D in adults; however, it has been suggested that the fortification level is insufficient to achieve adequate intakes. 79 Nevertheless, well-designed and sustainable fortification strategies using a variety of foods to accommodate diversity have the potential to increase vitamin D intakes. A voluntary, government-driven vitamin D fluid milk and fat spreads fortification policy in Finland provides a useful example. Following its introduction in 2003, the percentage of the population with a 25(OH)D concentration <30 nmol/L decreased from 12% in 2000 to <1% in 2011. 80
Currently, a controversy exists about the recommended vitamin D intake suggested by IOM in 2011, 81 therefore a panel of Latin American experts is required to carefully review the most recent information on the dietary intake recommendations for vitamin D issued by different organizations, before establishing a fortification program with this vitamin.
Furthermore, it is important to consider that using a different vitamin D recommended intake than the one suggested by the IOM could increase the prevalence of inadequate intake of this nutrient in Latin America because vitamin D recommended intake by other international instanes 81,82 is higher than the one proposed by IOM.
Inadequate Intake of Iron, Zinc, and Magnesium
The fortification of wheat flour with iron in most countries (except Chile) could help explain the low levels of inadequate intakes of this nutrient because the consumption of foods that are natural sources, such as legumes, is notably low in the countries included in the study. 49 Promoting the consumption of legumes could contribute, with a low environmental impact, to improving iron intake and reducing the significantly inadequate intake of zinc and especially the low magnesium intake, since this food group contributes a high content of these nutrients. 83 However, this is only possible in countries like Costa Rica, Brazil, Colombia, and Venezuela where beans consumption is part of their food culture. Therefore, other alternatives must be required to increase the availability of zinc in the diet of the Latin American population. Agronomic biofortification of different cereals with zinc has been shown to offer a practical and cost-effective option to address the problem of zinc dietary intake deficiency. 84 -86
Since there are important differences among the zinc dietary recommendations set by the WHO, the IOM, the International Zinc Nutrition Consultative Group, and the European Food Safety Agency (EFSA), 87 it is necessary to carry out an analysis of these recommendations in the Latin American context, in order to identify the most appropriate one to assess the zinc dietary intake in the region.| However, it is important to consider that the adoption of new recommended values for dietary zinc intake may influence the assessment of the prevalence of inadequate intake of this micronutrient.
Inadequate Intake of Calcium
The high prevalence of inadequate calcium intake suggests an aspect that public health authorities should consider immediately due to the association between calcium intake, reaching peak bone mass at around 30 years, 88 and osteoporosis prevention in adulthood. 89 However, there is robust agreement in the literature that approximately 80% of peak bone mass is determined by genetics and the remaining 20% is influenced by environmental factors such as diet and physical activity. 88,90 Although calcium intake plays an important role in bone health, its inadequate intake may not be an urgent public health problem, as it could be attributed in part to the high calcium requirements proposed by the IOM/NAM of the United States, which are difficult to attain, as previously has been suggested. 88 Evidence from high-income countries suggests that intakes below 800 mg/day in adults are suboptimal although most populations in low- and middle-income countries have intakes close to 400 to 500 mg/day with no solid evidence that these intakes cause adverse bone health outcomes. 88,91 Paradoxically, many low- and middle-income countries with low calcium intakes have lower rates of osteoporotic fractures compared to high-income countries. 88 Physical activity could explain this paradox because: (1) increased physical activity (mainly leisure-time activity or moderate or vigorous physical activity) is associated with a 1% to 40% lower risk of hip fractures and all fractures, 92 and (2) the prevalence of physical inactivity in high-income countries is higher than in low-income countries. 93
It is essential that decision-makers in Latin American public health carefully analyze the dietary reference intake values established by the IOM/NAM for North America (United States and Canada) 94 and make comparisons with the recommendations for calcium defined by other organizations (including the EFSA, 95 the Scientific Advisory Committee on Nutrition of the United Kingdom, 96 and the Working Group on Food, Diet, and Toxicology of the Nordic Countries 97 ) before making decisions regarding the promotion of calcium consumption for the prevention of osteoporosis, pregnancy complications, cancers, and cardiovascular diseases. However, the new proposed recommendations on calcium must be analyzed in light of the critical prevalence of inadequate intakes of vitamin D, because the role of vitamin D in bone health and the prevention of osteoporosis are well-documented. 98
This study has several strengths and limitations that should be considered when interpreting its results. Strengths include (1) the method used for food intake data collection (24-h recall) is more accurate than the food frequency questionnaire used in studies with similar objectives. (2) The adequacy of micronutrient intakes was evaluated using the usual intake, which minimizes the methodological bias associated with intrapersonal variability. (3) The large sample size provided more precise mean values, identified outliers that could skew the data in a smaller sample, and provided a smaller margin of error, allowing better estimations of the micronutrients intake in Latin American urban areas. Limitations include (1) The study only included urban areas of 8 LAC without considering rural areas or all the countries in the region, so the data cannot be generalized for all areas of Latin America. (2) The study did not consider the consumption of vitamin and mineral supplements, but this will most likely not affect the results as it has been shown that the use of these supplements is low in LAC. 99
Conclusion
This study showed a relevant inadequacy intake of micronutrients in urban areas of 8 LAC countries, particularly zinc, magnesium, vitamin C, calcium, and vitamin D. There is an urgent need to define direct regional actions and strategies in Latin America aimed at improving micronutrient intake, either through staple food fortification programs, agronomic biofortification, or through food policies that facilitate economic access to micronutrient-rich foods such as legumes, fruits, and vegetables, particularly for low SES and low educational level groups. In addition, public health policymakers must promote robust and continuous nutrition education campaigns and develop policies for agricultural production and food marketing consistent with healthy and sustainable dietary recommendations. Currently, LAC are focusing their attention on the epidemic of overweight/obesity and its associated metabolic complications. However, this problem coexists with the deficient dietary intake of micronutrients, therefore it is necessary systematic monitoring and surveillance of dietary intake of these. Realistic nutritional policies and appropriate intervention programs can improve both conditions for Latin American urban populations. Political and civil society support is necessary for any defined action to be effectively implemented.
Supplemental Material
Supplemental Material, sj-docx-1-fnb-10.1177_03795721231215267 - A Landscape of Micronutrient Dietary Intake by 15- to 65-Years-Old Urban Population in 8 Latin American Countries: Results From the Latin American Study of Health and Nutrition
Supplemental Material, sj-docx-1-fnb-10.1177_03795721231215267 for A Landscape of Micronutrient Dietary Intake by 15- to 65-Years-Old Urban Population in 8 Latin American Countries: Results From the Latin American Study of Health and Nutrition by Rafael Monge-Rojas, Rulamán Vargas-Quesada, Agatha Nogueira Previdelli, Irina Kovalskys, Marianella Herrera-Cuenca, Lilia Yadira Cortés, Martha Cecilia Yépez García, Reyna Liria-Domínguez, Attilio Rigotti, Regina Mara Fisberg, Gerson Ferrari, Mauro Fisberg and Georgina Gómez in Food and Nutrition Bulletin
Footnotes
Authors’ Note
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
The authors would like to thank the staff and participants from each of the participating sites who made substantial contributions to ELANS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the publication of this article from Fundación Iberoamericana de Nutrición—FINUT. This research was performed using the database of the ELANS study. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The original methods and funding information for the ELANS fieldwork are published elsewhere. 22
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.