
Abstract
Background:
The population in Latin America and Caribbean (LAC) has experienced a major demographic transition with increased numbers of older adults (OA). This change brings opportunities in the public health sector to implement health prevention interventions and delay the onset of geriatric syndromes. Micronutrients play an important role in the maintenance of biological function which contributes to longevity. Micronutrient deficiencies (MD) in OA increase the risk for onset of chronic comorbidities and geriatric syndromes.
Aim:
To review and summarize the existing data on micronutrient status in OA in the LAC region and discuss the gaps and challenges in public health approaches to address deficiencies.
Methods:
Literature review in Medline for records describing nutritional biomarkers in older adults (≥ 60y) from community dwelling and population-based studies in LAC.
Results:
Few countries (including Chile, Ecuador, Costa Rica, Brazil, and Mexico) have documented one or more nutritional deficiencies for OA in national health surveys, however across the entire region, evidence of micronutrient levels is scarce. Some surveys have documented a high prevalence and large heterogeneity in the prevalence of vitamin D followed by B12 deficiency, being the 2 MDs most studied due their effects on cognition, frailty, and bone mineral density in the OA population. Other MD including C, E, A, copper, zinc, iron, and selenium have also been reported.
Conclusion:
Information on the micronutrient status in OA from LAC is poorly documented. Research and capacity building initiatives in the region are crucial to develop tailored strategies that address the specific nutritional needs and challenges faced by the ageing population in Latin America.
Plain language title
Micronutrients Deficiencies in Older Adults in Latin American
Plain language summary
For the first time, there are more older adults (OA) than children worldwide. In the Latin America and Caribbean (LAC) region, OA represents 13.2% of the population, and it is projected to increase to 30% (220 millions) by 2030. This demographic shift represents an opportunity in the public health sector to implement health prevention strategies and public health policies to delay the onset of geriatric syndromes in the younger generation. Vitamins and minerals (micronutrients) are necessary in our body to maintain biological function. Deficiencies in older ages have been associated with the onset of geriatric syndromes (such as sarcopenia, frailty, cognitive impairment, and falls, among others). Therefore, it is relevant to understand the magnitude and distribution of micronutrient deficiencies in OA in the LAC region. This will help to inform decision-makers to further implement early actions to maintain good nutrition and health status in the population. In this narrative review, we highlight that few countries in the LAC region documented one or more nutritional deficiencies for OA in their national health surveys. Across the entire region, evidence of micronutrient levels in OA is scarce. Vitamin D and vitamin B12 are the 2 most reported micronutrients in the OA population. Research and capacity-building in the region are crucial to develop tailored strategies to address specific nutritional needs and challenges faced by the aging population in Latin America.
Introduction
The demographic transition in most low- and middle-income countries (LMIC) has experienced rapid changes in the population age structure. 1 For the first time, there are more older adults (OA) than children worldwide. 2 The number of OA ≥60 years old in the Latin America and Caribbean countries (LAC) is around 88.6 million, representing 13.2% of population. The OA population in this region is projected to increase to 114.9 million (16.5%) by 2030, and to 220 million (30%) by 2060. By the end of this century (2100), OA aged 80 years and over will be the only population group that will continue to grow at the regional level. 3 All these projections represent an opportunity to develop public policies in anticipation of these population changes, to address inequalities in the public health sector, 4 and to implement preventive strategies to achieve healthy aging. At the same time, these predicted population shifts bring challenges in currently fragmented and segmented health care sectors when it comes to managing geriatric syndromes (such as loss of autonomy, frailty, sarcopenia, and dementia, among others), providing quality care and addressing overall inequity in access to health care without action at the public health level. 5
The change in the life expectancy at birth has increased an average of 6.9 years in the Latin American region over the last 30 years. In part, this is a result of the success of public health policies implemented several decades ago that focus on the early stages of life, including policies addressing micronutrient deficiencies (MD) in childhood (+0.3 years gained) and maternal and neonatal health coverage improvements (Figure 1). 6
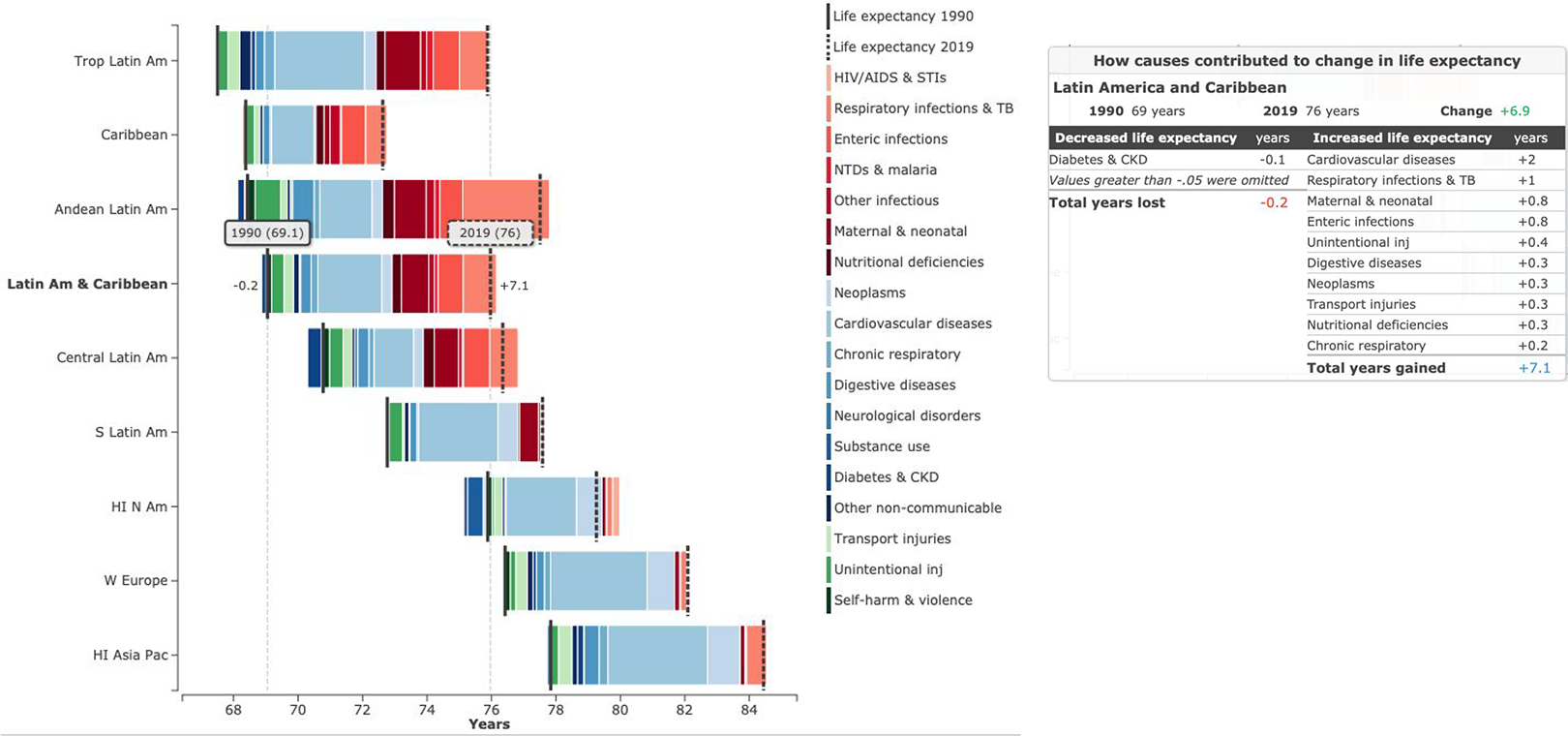
Change in sub-region life expectancy at birth from 1990 to 2019 in both sexes by broad cause group in selected regions. AIDS, acquired immunodeficiency syndrome; Am, America; CKD, chronic kidney disease; HI, high income; N, North; Pac, Pacific; S, south; STD, sexually transmitted infections; TB, tuberculosis; Trop, tropical; W, western; NTD, nontransmissible diseases.
Micronutrients such as vitamin B12, folate, vitamin D, iron, magnesium, and zinc (among others) play an important role in the maintenance of biological function, immunity, and functionality across the life span including in OA, which together contribute to longevity. 7 As a result of physiological changes that occur during the aging process, 8 MDs are common in OA and may pose a risk in the onset of chronic comorbidities, infection, and geriatric syndromes. 9 The causes of MD in OA are complex and quite often multifactorial and frequently relate to dietary deficiencies, malabsorption syndromes, polypharmacy, and comorbidities. Having a better understanding the complexities of MD in OA is essential to enable well designed preventive health interventions for OA to maximize functional independence and quality of life, in alignment with the UN Decade of healthy aging. 10
The United Nations has declared 2021 to 2030 the “decade of healthy aging.” As such, this represents an opportunity to focus efforts on improving quality of life for OA and to maximize our later years in a sustainable and healthy way, to benefit both for current and future generations. 10 Ongoing public health efforts in the region are addressing MD and anemia in children and women, with known deficiencies in indigenous populations and those living in poverty and in rural areas. However, our understanding of MD in OA is less well documented. 11 In this narrative review, we highlight what we know about common nutritional deficiencies and their role in the health of older Latin American adults. We discuss the gaps and challenges to address these deficiencies to achieve healthy aging.
Methods
A literature review was conducted in MEDLINE (PubMed) for records describing nutritional biomarkers and micronutrient deficiencies in OA (≥60 years) in outpatient clinical and field settings (community and population-based studies) where the crude prevalence was reported in the Latin American region, in the period 2000 to 2022. We excluded case reports, duplicates, theses, and studies that did not report prevalence, hospital-based settings and, where OA were in residential health care settings for specific medical conditions (heart diseases, hip fractures, COVID-19, etc).
Results and Discussion
Commonly Measured Micronutrient Biomarkers
A total of 28 studies reported one or more MDs in OA in Latin America in 8 Latin American countries (Table 1). National health surveys and aging surveys conducted in Chile, Ecuador, Brazil, Costa Rica, and Mexico reported MD in their OA populations. In addition, MD prevalence was reported through local (community-based) studies in the same countries, with the addition of Argentina, Peru, and Venezuela.
Summary of Studies Documenting the Prevalence of Micronutrient Deficiencies in Older Latin Adults.
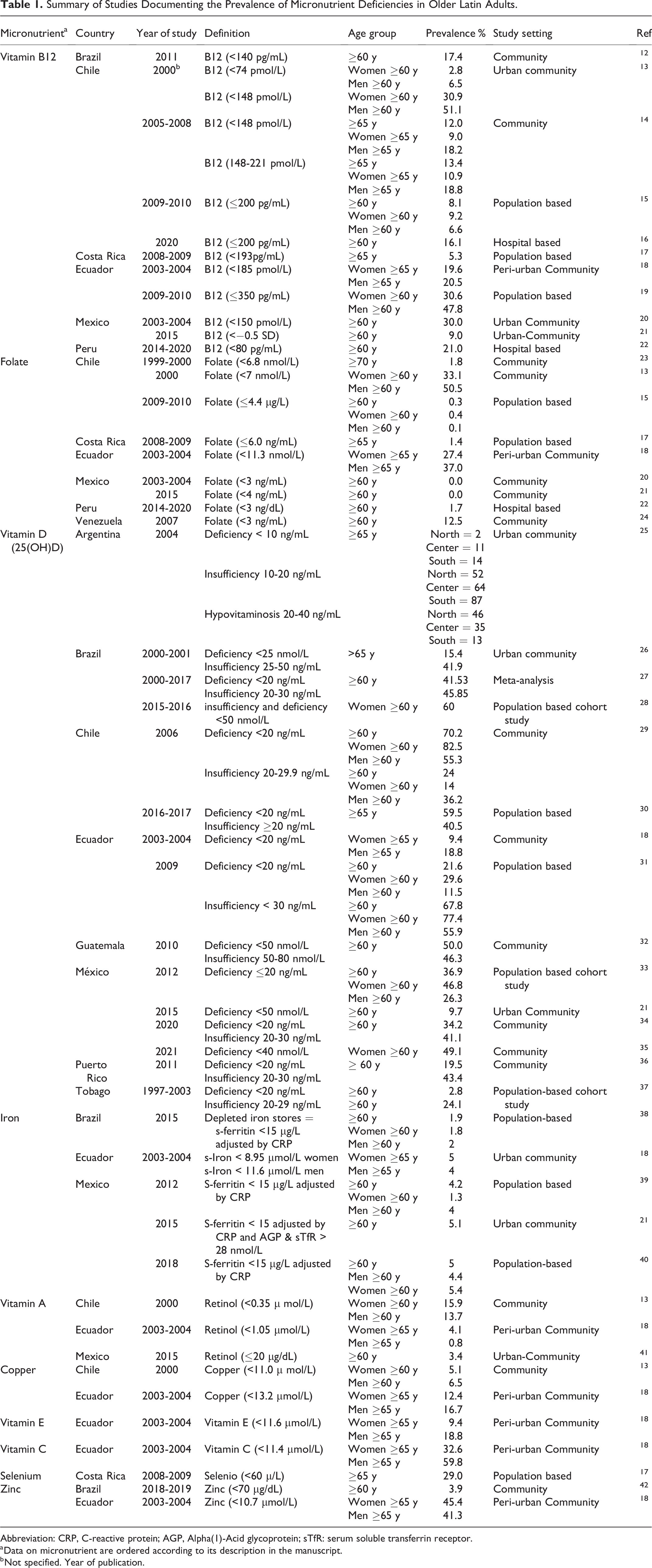
Abbreviation: CRP, C-reactive protein; AGP, Alpha(1)-Acid glycoprotein; sTfR: serum soluble transferrin receptor.
a Data on micronutrient are ordered according to its description in the manuscript.
b Not specified. Year of publication.
Vitamin B12 and Folate Deficiency
Ecuador, 19 Chile, 15 and Costa Rica 17 reported the prevalence of low vitamin B12 levels in OA from representative surveys (Table 1), with a large heterogeneity in the prevalence of Vitamin B12 deficiency (B12D) by sex, and when data was gathered from local studies.
The active forms of Vitamin B12 are methylcobalamine and adenosylcobalamin, they act as cofactors in 2 separate metabolic reactions, with cytosolic methionine synthase and mitochondrial methymalonyl CoA mutase. The disruption of either of these reactions can lead to B12 deficiency. In B12D, decreased levels of adenosylcobalamin lead to an increase in methylmalonyl-CoA, which affects synthesis of neuronal myelin in the developing central nervous system; while decreased levels of methylcobalamine leads to the functional deficiency of folate and accumulation of homocysteine. 43,44 B12 metabolism is linked with folate-mediated one-carbon metabolism due to the utilization of 5-methyltetrahydrofolate as a methyl donor. 44 Both, B12 and folate deficiency (FD), affect DNA synthesis with resulting macrocytic anemia. B12D increases cellular inflammation (hypersegmented neutrophils) and the synthesis of intermediate metabolites such as homocysteine and methylmalonic acid (MMA). 44 Increased levels of homocysteine and MMA can result in severe damage to the brain and spinal cord, particularly in the corticospinal and spinocerebellar tracts, resulting in ataxia, neuropathy and in later life, cognitive decline. 45 There are numerous studies exploring B12D in older populations due to the association with cognitive decline, impaired executive function, and the risk of dementia. The OA population is at higher risk of B12D due to malabsorption secondary to gastric atrophy, diminished intrinsic factor and hydrochloric acid. 46 In Latin America, B12D has been widely studied in the Chilean population, with the Government responding with public health initiatives to address deficiencies. 47 Along with Chile, 48 Ecuador, 19 and Peru 22 have also documented the role of subclinical B12 deficiency on cognitive function in OA, with contradictory findings. In a cross-sectional study of older Cuban adults, higher homocysteine levels and FD but not B12D were associated with mild cognitive impairment. 49 Daily fluctuations of B12 levels in serum may not properly reflect the true B12 status. What might be useful are combinatory approaches for measuring multiple, related indicators of VB12 levels in OA. For example, measuring the intermediate metabolites homocysteine and MMA, or others involved in the transport of B12 such as holotranscobalamin, which when combined, might improve sensitivity in the diagnosis of B12D. 50
Since the introduction of the mandatory folate fortification in wheat and corn flour in some Latin American countries, 51 FD has dropped below 1% prevalence in OA. As such, FD is no longer considered an ongoing public health challenge in those countries. 51 Only a few studies have documented FD in OA. However, supraphysiological levels of folate have been reported in older Chilean and Mexican populations (Table 2). Elevated folate levels have been implicated in exacerbating B12D. 52 The mechanism of folate-VB12 interaction is not well understood; however, there is some evidence that high folate levels (HFL) decrease the effectivity of vitamin B12 treatment in B12D. 53 In some studies, HFL and low vitamin B12 has been linked to impaired cognition in OA, 54,55 but in other studies, authors have documented high folate levels associated with higher score in cognitive function, independent of B12 levels. 56,57 More research is needed to better understand how low levels of vitamin B12 (subclinical deficiency) interact with high levels of folate in the progression of cognitive decline.
Supraphysiological Levels of Folate and Iron in Older Population From Selected Studies in the Latin American Region.
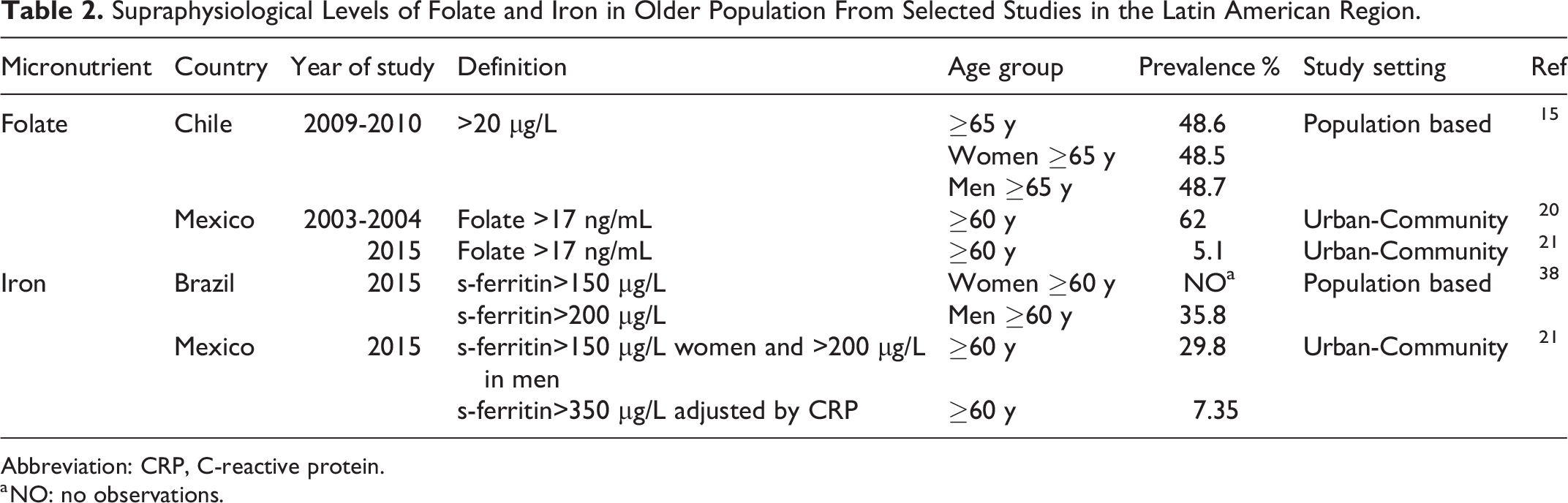
Abbreviation: CRP, C-reactive protein.
a NO: no observations.
Vitamin D Deficiency
Brazil, 28 Chile, 30 Ecuador, 58 and Mexico 33 reported the prevalence of low vitamin D levels in OA from representative surveys (Table 1). Vitamin D (VD) status is the most reported micronutrient in the LAC region. Both, VD insufficiency and deficiency (VDD) are highly prevalent in OA, reaching a prevalence (25[OH]D <20 ng/mL) higher than 50% in Brazil 28 and Chile, 30 which is comparable with other LMIC. 59 Most studies have used 25[OH]D levels for classifying VDD in OA populations. 60
At the community level, the VDD prevalence in OA varied, probably due to sample characteristics, seasonality (more prevalent in winter), and latitude (Table 1). Two metanalyses 27,61 have been conducted to estimate VDD in the region, showing a prevalence of 41.5% (95%CI: 27.6, 55.4) in older Brazilian adults, and 34.8% (95%CI: 29.7, 40.2) in all age groups in the South-American Region.
Sun exposure is the primary source of vitamin D for the human body 60 with dietary intake of VD making a smaller contribution to VD status. 62,63 Advanced age has been associated with a lower capacity for the body to synthesize vitamin. 64,65 In addition, OA with chronic comorbidities (such as obesity, diabetes, kidney disease) 66 have impaired absorption and metabolism of vitamin D. 67,68 Therefore, supplements of VD are often required to reach the daily intake recommendation.
Vitamin D (along with vitamin A) regulates gene expression and acts as transcription factor for multiple genes that modulate the immune response. 69,70 VD is essential for maintaining bone, muscle health, and erythropoiesis, therefore, its deficiency can have a significant impact on quality of life for OA. 71,72
Vitamin D deficiency increases the risk of osteoporosis, bone fractures, type 2 diabetes, respiratory diseases, sleep disorders, depression, impaired cognition, cardiovascular disease, autoimmune diseases, and some types of cancer. 69,72,73 Older adults with VDD have a higher risk of falls, sarcopenia, and decreased functional capacity, which can in turn lead to increased frailty, dependence, and disability. 71,73
Recent systematic reviews and meta-analysis has suggested a correlation between low Vitamin D and impaired cognitive function. 72,74,75 Evidence from a number of observational studies is contradictory, possibly due to residual confounding. For instance, in one study, VDD was not associated with cognitive function in OA from Ecuador. 19 In other studies, metanalysis exploring supplementation of VD did not show any effect on cognition or depression. 76,77
During the COVID-19 pandemic, VD was studied in several populations due its role in strengthening the immune system by modulating the inflammatory response during infection. For all age groups, including OA, VDD was associated with COVID-19 severity and mortality 78,79 Supplementation with VD may contribute to the prevention and management of COVID-19 infection. 79 Nonetheless, a causal relationship between vitamin D status, VD supplementation, and COVID-19 (incidence, severity and progression) has not been established due to methodological differences in those studies.
Iron Deficiency
Information about iron deficiency (ID) in OA is scant. In those studies that report it (Mexico and Brazil), the prevalence of ID was around 5% or less. 38,40 Low iron stores, and ID, are typically defined by measuring s-ferritin levels (an acute phase protein). However, established thresholds for defining ID are based on adult populations that do not take into account any normative changes that might occur in OA. 80 The diagnosis of ID is challenging in OA since low grade inflammation secondary to the aging process (inflammaging), infection and chronic comorbidities may all increase ferritin levels. Functional ID can be the result of inflammation (for example caused by infection, cancer, rheumatoid arthritis, autoimmune disease or, chronic disease), 81 as a result of increased hepcidin, a protein that blocks iron export from ferroportin in the epithelial cells thereby limiting iron availability in the bone marrow. In the presence of infection, the body reduces circulating iron in an attempt to combat pathogens. 82 Consequently, prolonged iron deprivation (referred to as functional iron deficiency) can lead to anemia of chronic diseases or anemia of inflammation. 83 To improve diagnosis specificity for ID, the use of s-ferritin as an indicator should be used in conjunction with inflammatory biomarkers to generate a more reliable indicator of overall iron status. 84 Iron deficiency and anemia are detrimental to health. Iron deficiency is the main cause of anemia in younger populations in LMIC 85 and it is estimated to be the second leading cause in OA. 86 Few studies have documented the causes of anemia in OA in Latin America. 21,87,88
Iron deficiency leads to poor quality of life and disability. 89 It has also been established that ID anemia (IDA) increases the risk of morbidity and mortality in OA. 90,91 The causes of ID in OA are usually associated with gastrointestinal blood loss (caused by varices in portal hypertension, gastritis, ulcers, inflammatory bowel diseases, among others) which can lead to IDA. In addition, alcohol abuse, malnutrition, and chronic diseases as chronic renal failure and inflammatory diseases can also result in ID and lead to IDA.
Iron is a trace mineral essential for maintaining normal physiological processes involved in the electron transport chain, mitochondrial respiration, DNA synthesis, and synthesis of heme, myelin, and neurotransmitters. Due to its role in redox activity, iron is tightly regulated in the body. Excessive iron results in catalyzed oxidative reactions that generate reactive oxygen species (ROS). ROS (oxidative stress) causes DNA damage, lipid peroxidation, and aberrant posttranslational modification of proteins. 92 In mitochondria, energy production generates ROS. Iron utilization in the mitochondria requires proteins to regulate iron homeostasis (frataxin, mitoferrin) since it is vulnerable to iron-induced oxidative stress. The loss of mitochondrial iron homeostasis in combination with iron accumulation, may contribute to mitochondrial decay, which is characteristic of aging. 93 These mitochondrial changes may be involved in the pathogenesis of age-related neuro-muscular degeneration (muscle atrophy, sarcopenia). 93 As part of normal aging, the central nervous system shifts into a pro-inflammatory state, with increases in glial cells numbers and increased permeability of the blood–brain barrier. These ageing-related changes can lead to regional increases in brain iron 94 which in turn has been correlated with the presence of neurodegeneration. 95,96 To date, this correlation has not been shown to be causal. 95,97 Evidence from observational studies linked high ferritin levels and neurodegeneration has been inconclusive. High ferritin levels have been linked to cardiovascular disease, diabetes, and increased mortality in the older adult population. 98,99 Two studies in the Latin American region (Brazil and Mexico) reported a higher prevalence of increased ferritin levels in OA. To better understand the nature of the relationship (correlation, cause, or consequence) between increased iron levels and aging, more research in the LAC region is needed.
Vitamin A Deficiency
Few countries (Chile, Mexico, and Ecuador) have reported the prevalence of Vitamin A (VA, also known as retinol) deficiency in older Latin America population, with estimates of less than 5% prevalence (Table 1).
Vitamin A is a liposoluble vitamin that plays an important role in gene expression, transcription, stem cell differentiation, cell proliferation, vision, growth, maintenance of epithelial cellular integrity, and immune function. 100 Vitamin A deficiency leads to a depleted immune system, night blindness, altered bone metabolism, 101 and increased risk of respiratory infections. 102 Retinoic acid (the main metabolite of VA) has been reported to have neuroprotective effects in the amyloid signaling cascade, as well a role in synaptic plasticity, associated with memory. 103,104 We previously reported a cross-sectional association of low serum retinol with lower verbal fluency in older Mexican adults. 41 In older Cuban adults, vitamin A deficiency was cross-sectionally associated with increased risk for mild cognitive impairment. 49 Moreover, higher retinol levels have been associated with higher adverse events in other OA populations (lower bone density, cardiovascular risk, and mortality). 101,102
Copper, Zinc, Vitamin E, Vitamin C Selenium, and Magnesium Deficiencies
There are very few reports of levels of copper, zinc, vitamin E, vitamin C, or selenium in Latin American populations. One study in a subset of OA Ecuadorians in a low-income peri-urban community in Quito, documented a cross-sectional association of low levels of vitamin C, E, copper, and zinc with anemia and respiratory infections via negative impacts on immune function. 18 Costa Rica is the only country in the region that has published evidence of low levels of s-selenium in OA. 17 Deficiency of all these micronutrients in OA from other populations has been associated with a deprived immune system, 105 oxidative stress, 106 anemia, 107 cardiovascular disease, 108 and impaired cognitive function, 109 among others.
Zinc plays a pivotal role in maintaining health and well-being in OA. In the region, Brazil 42 and Ecuador 18 are the only countries that have reported serum zinc concentrations in OA. Low zinc levels affect T cells and cytokines activity, wich impairs the immune response. 110 Consequently, OA with zinc deficiency (ZD) might experience a higher incidence and longer duration of respiratory diseases, as shown in the study with Ecuadorian OA. 18 Intervention studies with zinc supplementation have shown that an increase in serum zinc levels boosts T cells, enhancing immune system function. 111 Zinc is also involved in preserving bone integrity by controlling bone resorption and deposition, with low levels of zinc being a risk factor for osteoporosis. 112 Furthermore, the brain contains the highest zinc concentration compared to other organs. Zinc acts as a modulator for neurotransmitters such as glutamate, and γ-aminobutyric acid (GABA), is involved in glycinergic synaptic transmission. 113 ZD can impair enzyme metabolism in the brain, leading to an accumulation of pathological proteins linked to Alzheimer’s disease. 114 In older Brazilian adults, ZD has been associated with cognitive decline. 42
So far, no countries in the region have studied the role of Magnesium (Mg) and health in OA. Mg has a pivotal role in aging and longevity since it modulates both the innate and the acquired immune response acting as anti-ROS preserving genomic stability, 115 and as a cofactor for multiple proteins reactions (eg. muscle synthesis ATP, vitamin D synthesis among others). 116 In the brain, Mg preserves the integrity and stability of the cell membrane, reduces neuroinflammation, is involved in neural maturation and clearance the proteins and toxins from the brain. 117 Deficits of Mg have been associated with insulin resistance, diabetes, cardiovascular disease, cancer, hypertension, asthma, psychiatric disorders, osteoporosis, cognitive decline, and Alzheimer´s disease. 116,118 -120 Epidemiological studies in OA (from North America, Japan and Australia) have shown that low intakes of Mg are associated with a higher risk of cognitive decline and dementia of all types, including vascular dementia. 121 -123 Further research is needed to better understand the role of Zn, Mg, and others MD in health and disease, in order to design effective strategies to achieve a healthy aging in the region.
The Gaps and Challenges
To date, information on the micronutrient status in older populations is scarce in most Latin American countries. Information that is reported comes from representative surveys and local studies (which are not representative of the national population within each country). Most of the aging surveys used in Latin America do not collect enough information about nutritional biomarkers to accurately characterize the micronutrient status of the population, and these biomarkers are not routinely measured. The assessment of the micronutrient status at a population level in OA requires investment, a coordinated approach to data collection, as well the appropriate equipment and certified laboratories to process biological samples. Moreover, there are no universally agreed serum/plasma micronutrient thresholds to define deficiency in OA. 124 A variety of cut-off points to define micronutrient deficiencies are used which makes comparison across the Latin American region difficult. Some existing thresholds used to define “deficiency” are based on data from younger adults and do not consider age-related changes. This brings challenges when interpretating the “deficiency status” in this age group, including in the identification of deficiencies in the subclinical range, which might represent the best opportunity for timely intervention. Malabsorption syndromes, polypharmacy, and chronic comorbidities are common conditions of OA, which in themselves can exacerbate micronutrient deficiencies. Additionally, the effect of low-grade inflammation during aging might mask underlying deficiencies in micronutrients such as retinol, iron, and zinc. With all of this in mind, it is likely that micronutrient deficiency is underestimated in OA in LAC. Micronutrient deficiencies tend to disproportionately affect underrepresented and vulnerable groups, such as black, indigenous, rural populations, and those with lower socioeconomic status, where health inequities persist. 125 More research is needed to better understand the long-term risk of MD and the inherent inequities in the LA region, before it can be effectively addressed. 125
The lack of information about MD in most countries across the region make it challenging to respond adequately and comprehensively to the UN declaration of the decade of healthy aging. Regular data collection is crucial for surveillance of micronutrient levels in OA population. In addition, longitudinal studies in OA are needed to accurately describe trends in MD and to identify the window of opportunity where nutritional intervention would be most effective. Revising and agreeing on recommendations of micronutrient levels in OA, and including consensus criteria for diagnosing deficiencies, are both needed to allow comparison within and between countries as well as to evaluate the response to any interventions. Without this, the existing gaps in our understanding continue to limit opportunities to address inequities in nutrition to improve the nutritional status of the older population and achieve healthy aging.
Dietary deficiencies are considered to be the main causes of MD, which are intimately linked to food insecurity and poverty. 7,126 Data exploring the link between dietary practices and geriatric syndromes are scarce, and where is does exist, is poorly documented across the region. In addition, national diet and food policies vary across Latin American countries, which may contribute to the prevalence of MD, where known. Fortification of staple foods such as wheat and maize, with critical micronutrients including iron, vitamin A, zinc, calcium, and vitamin D, is a strategy that has been successfully used to address MD at the population level. 127 However, surveillance in the adherence to fortification guidelines is necessary in counties where fortification is not mandatory. For example, a study in 2018 conducted in Mexico City reported that only a low proportion of flours were adequately fortified, despite national policy recommending fortification. 128,129
Most countries in the region have implemented food fortification programs, such as adding folic acid to wheat and corn flours which explains the decline in the prevalence of FD in the region. 51 What is perhaps missing is research into the effects of supraphysiological levels of some micronutrients, such as folic acid and vitamin A, and their effect on outcomes in OA, some of whom may also be participating in the supplementation programs.
Supplementation strategies have been effective when designed to target specific populations. For example, in Chile the program “Complementary Feeding for older adults” was designed to address VB12 deficiencies in the Chilean OA population. This program supplemented 58% of the daily recommended intake of B12 130 but previous reports had already shown that this dose would be insufficient. 47 When safely implemented targeted population strategies are cost-effective approaches to improve micronutrient status, health, and aging-related outcomes. 131
Final Remarks
Micronutrient deficiency is detrimental for health across the whole lifespan. The risk of MD increases with age. A more comprehensive understanding of the main drivers of MD in LAC is needed in order to generate public health-level solutions that improve overall health, independence, and quality of life for OA. The OA population is projected to grow in Latin America which brings challenges to the health system unless early nutritional interventions are delivered to maximize healthy aging. Effective screening of MD will be a critical step to maintain biological function and preserve functionality for at-risk populations. Public health policies focusing on the prevention of malnutrition offer an economic alternative to costly treatment of potentially preventable chronic conditions.
Investment in research and capacity building in the region is crucial to identify equitable solutions to enable healthier populations. By investing in targeted research, we will gain valuable insights into factors contributing to micronutrient deficiencies in OA in LAC. Such insights will inform the development of targeted interventions, policy recommendations, and educational programs aimed at promoting healthy aging and improving the overall well-being of OA. Concurrently, building capacity among health care professionals, policymakers, and community stakeholders will foster a collaborative environment for effective implementation and sustainability of interventions.
Studies that adopt a life-course perspective will enable better understanding of early social determinants, nutritional interventions, long-term outcomes 132,133 and identification of the most cost-effective strategies for the prevention and treatment of age-related diseases associated with MD.
Conclusions
This narrative review describes the reported prevalence of micronutrient deficiencies in OA in Latin America. Only a small number of countries in the region (Brazil, Chile, Ecuador, Costa Rica, and Mexico) have reported any micronutrient data for their populations through representative surveys. These countries are among the highest development index rankings for the region (in the top 10) with minimal Caribbean representation (Tobago). Vitamin D and B12 are the most studied micronutrients in this population, being Vitamin D deficiency reported as the most prevalent. Other micronutrient deficiencies (Vitamin C, E, A, copper, zinc, iron, and selenium) are reported with lower frequency, while others such as magnesium are not reported at all. The limited availability of data, lack of standardized criteria for acceptable micronutrient levels in OA, and the need for biomarker infrastructure in the region, pose significant obstacles to the accurate determination of MD prevalence and to design and implement targeted interventions. Future research and public health efforts should prioritize addressing these challenges to improve the nutritional status and overall health of OA in the Latin American region.
Footnotes
Acknowledgments
The authors thank Alison Canty for critical revision of the manuscript.
Author Contributions
The main author of this work declares that all authors have contributed and work on the development of it as follows. VDG: Conception and design, literature search, analyses, and interpretation of data, writing manuscript. RPG: Literature search, analyses, and interpretation of data, drafting manuscript. ODF: Literature search, analyses, and interpretation of data, drafting manuscript. All authors: Read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the publication of this article from Fundación Iberoamericana de Nutrición (FINUT). The funders of the publication had no role in study design, data collection, data analysis, data interpretation, or writing of the report.