
Abstract
Background:
The current magnitude of folate and vitamin B12 deficiency in Latin America and the Caribbean is uncertain.
Objective:
To summarize data on plasma or serum vitamin B12 and folate concentrations in Latin America and the Caribbean reported since 1990, a period that covers the era before and after the introduction of folic acid fortification.
Methods:
A systematic review was conducted in 2012 and updated in 2014. Studies and surveys using biochemical biomarkers and conducted in apparently healthy individuals were identified.
Results:
Folate deficiency in Latin America and the Caribbean appears not to be a public health problem (prevalence < 5%) after the introduction of folic acid fortification. However, there is some indication that high rates of low or marginal vitamin B12 status remain in most locations and across population groups.
Conclusions:
Adding vitamin B12 as a fortificant with folic acid may be the best strategy in areas where vitamin B12 deficiency is an established concern.
Introduction
Vitamin B12 and folate are B vitamins with shared functions; both micronutrients participate in one-carbon metabolism. 1,2 Poor folate status in vulnerable fertile women increases the risk of neural tube birth defects. 3–5 As a measure to decrease the risk of this birth defect, folic acid has been added to staple foods such as wheat or maize flour. 6 Vitamin B12 deficiency is more frequent in populations with a low intake of vitamin B12–rich foods, most notably animal-source foods. 7 Older adults are also at high risk for vitamin B12 deficiency due to progressively impaired absorption of the vitamin from food with age. 7 More severe symptoms of deficiency of these two vitamins are associated with hematological disorders. 8 However, vitamin B12 deficiency can also induce clinical and subclinical neurological disorders in the absence of hematological impairment. 9 Poor maternal vitamin B12 status results in low levels of breastmilk vitamin B12 and subsequent vitamin B12 deficiency in the infant. Deficiencies of folate and vitamin B12 have the potential to be expressed as public health problems. In the past decade, alarmingly high prevalence rates of low plasma vitamin B12 were recognized to exist in the Americas, 10,11 while low plasma folate concentrations were less common. 10,11 Considering the strong interest in the potential benefits of folic acid fortification in the Americas and the few national programs existing to prevent or control vitamin B12 deficiency, updating existing data on folate and vitamin B12 status can provide valuable information in the fight to attain population adequacy of both vitamins. The purpose of this systematic review is to summarize available data on plasma or serum folate and vitamin B12 concentrations in Latin America and the Caribbean reported since 1990, a period that covers both the pre- and post-folic acid fortification eras.
Methods
A systematic review was conducted between July 2011 and April 2012 and updated in August 2014. All available evidence regarding folate and vitamin B12 status in apparently healthy populations in Latin America and the Caribbean since 1990 was included. PubMed, the Latin-American and Caribbean Center on Health Sciences Information (LILACS), Nutrinet, and Scielo were used to identify research articles by combining the terms “vitamin B12,” “folate,” and “folic acid” with the names of each country in Latin America and the Caribbean. Studies were not excluded on the basis of language. In addition, national surveys or national-level representative studies in apparently healthy populations were identified by accessing the websites of the Ministries of Health. Studies were classified according to national or local representativeness (small community, district, or province). A sample size of at least 50 per study was considered a minimum entry criterion for this review. Most of the available vitamin B12 prevalence data in Latin America and the Caribbean are based on serum or plasma vitamin B12. The values reported were standardized to picomoles per liter (picograms per milliliter converted to picomoles per liter by multiplying by 0.738). Plasma or serum vitamin B12 concentrations were defined as adequate (> 221 pmol/L), marginal (148 to 220 pmol/L), or low (< 148 pmol/L). 12 Low folate is mainly defined as serum folate < 3.2 nmol/L (converting nanograms per milliliter to nanomoles per liter by multiplying by 2.266). Since there were different criteria available and, in some cases, no standard cut point existed, the cutoff values expressed by each author were included. Prevalence data were described in percentages and confidence intervals. Figures were plotted using the software R studio (R Core Team 2014). 13
Results
A total of 817 articles were initially identified; 368 were excluded because of duplication. After review of the title and abstract, 606 studies were excluded because the information was not relevant to the purpose of the review. In the end, 8 national surveys and 41 studies were selected for this review.
Prevalence of Folate Deficiency in Latin America and the Caribbean
Figure 1 shows the prevalence of folate deficiency in Latin America and the Caribbean. Before folic acid fortification started, children from Mexico (< 12 years) 14 and Costa Rica (< 7 years) 15 had rates of folate deficiency of 2% (plasma folate < 2 nmol/L) and 7% (stated as plasma folate < 6 ng/dL), respectively, while children from Venezuela 16,17 had a 32% rate of folate deficiency. Mexican 14 and Costa Rican 18 fertile women had rates of folate deficiency of 5% and 4%, respectively (stated as plasma folate < 57 ng/dL and < 6.8 nmol/L, respectively), while a rate of 35% was reported in lactating women from Costa Rica (stated as < 6 ng/dL). 19 In local studies, Mexican children presented with a 3% prevalence of deficiency (< 3 ng/dL), 20 while in Venezuela, 54% of children and 64% of adolescents were classified as deficient (< 6.6 nmol/L). 16 Indigenous children from Venezuela presented with a 12% rate of deficiency (≤ 3 µg/L). 21 Local studies conducted in pregnant women from Mexico, Venezuela, and Brazil reported a range of prevalence rates from 0% to 36%, 22–25 while a rate of 0% (< 6.1 nmol/L) was reported in pregnant women from Mexico. 22 Among lactating women, a local study conducted in Guatemala indicated a 3% prevalence of low plasma folate (< 6.8 nmol/L). 26 Among adult women, there was a wide range of rates of folate deficiency, from 0% to 43% in Mexico (< 6.1 nmol/L), 22,27,28 Cuba (< 9 nmol/L), 29 and Chile (< 3.2 nmol/L). 30 Among adults, there was a large range of rates of folate deficiency, from 0% to 80% in Mexico (< 6.1 nmol/L), 22 Cuba (< 7 nmol/L) 31 , and Peru (stated as < 3.5 ng/mL). 32 Rates of folate deficiency in the elderly were reported to be 9%, 13%, 31%, and 39% in Guatemala, 33 Venezuela, 34 Ecuador, 35 and Chile, 36 respectively.
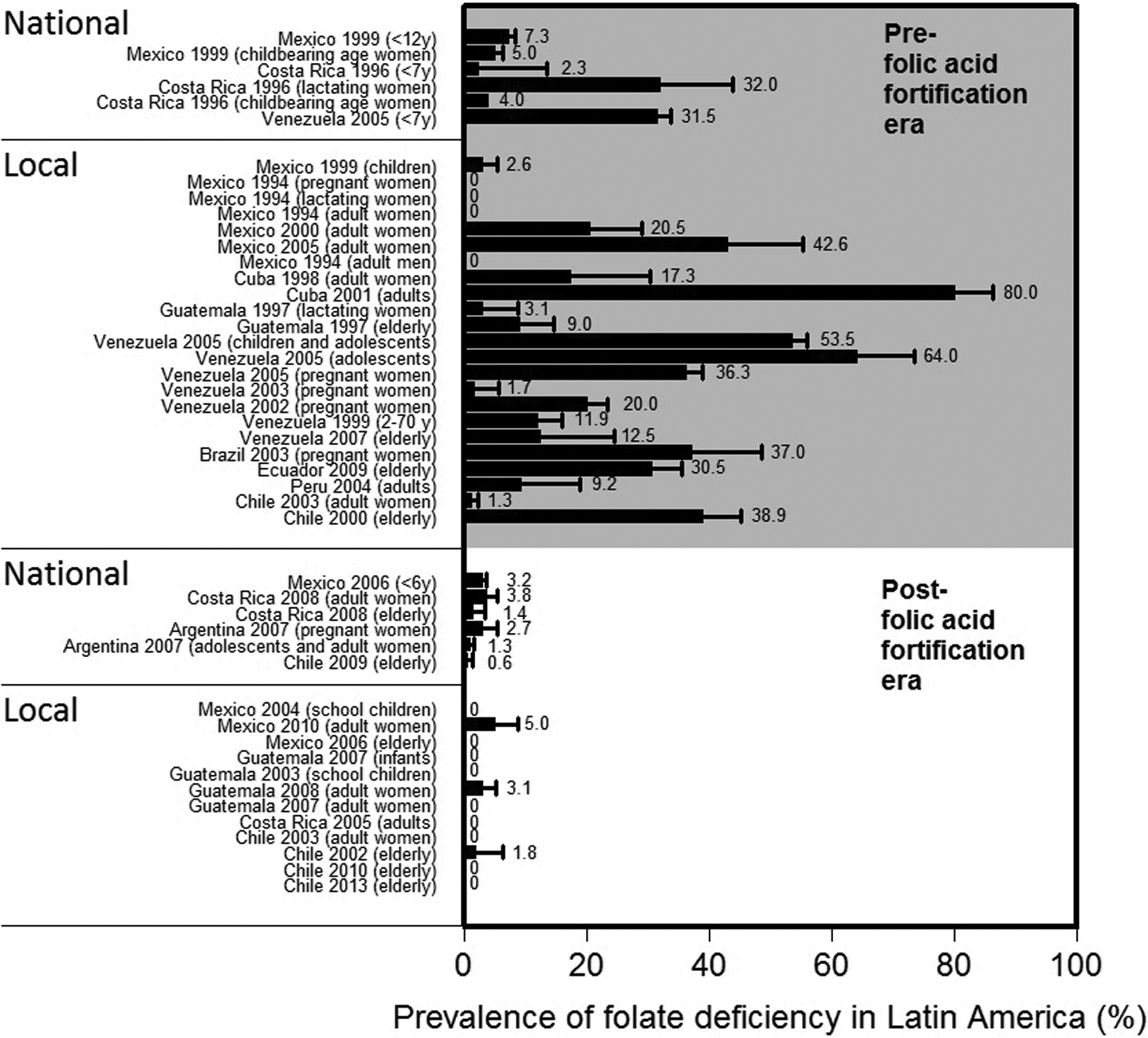
Prevalence of folate deficiency in Latin America and the Caribbean before and after folic acid fortification.
After folic acid fortification started, national data show that in Mexico, 37 Costa Rica, 38 and Argentina 39 there was a low prevalence of folate deficiency (3% in children under 6 years of age, 4% in adult women, 3% in pregnant women, and 1% in fertile women). Among the elderly, the prevalence of deficiency was only 1.4% and 0.6% in Costa Rica 38 and Chile, 40 respectively. Local studies also indicated the same pattern of the prevalence of folate deficiency, with rates of 5% among Mexican adult women, 41 3% among Guatemalan adult women, 42 and 2% among Chilean older people. 43 A series of studies conducted across age groups indicated no folate deficiency in schoolchildren and older people in Mexico 44,45 ; infants, schoolchildren, and adult women in Guatemala 46,47 ; adults in Costa Rica 48 ; and adult women and older people in Chile. 30,49,50
Prevalence of Low Vitamin B12 in Latin America and the Caribbean
Figure 2 shows the prevalence of low vitamin B12 in Latin America and the Caribbean. Before folic acid fortification started, national data from Mexican preschoolers, schoolchildren, adolescent girls, and women reported rates of low serum vitamin B12 (< 148 pmol/L) of 24%, 27%, 36%, and 23% and rates of marginal vitamin B12 values (between 148 and 221 pmol/L) of 16%, 20%, 22%, 24%, respectively. 14 Eleven percent of lactating women in Costa Rica and 5% of preschoolers in Venezuela had low vitamin B12 values. 16,17,19 In local studies, the range of low and marginal vitamin B12 values was 0% to 61% and 13% to 33%, respectively, in populations of all age and physiological groups from Mexico, Venezuela, Guatemala, Cuba, Chile, and Peru. 20–22,26,27,29,34,46,51,52
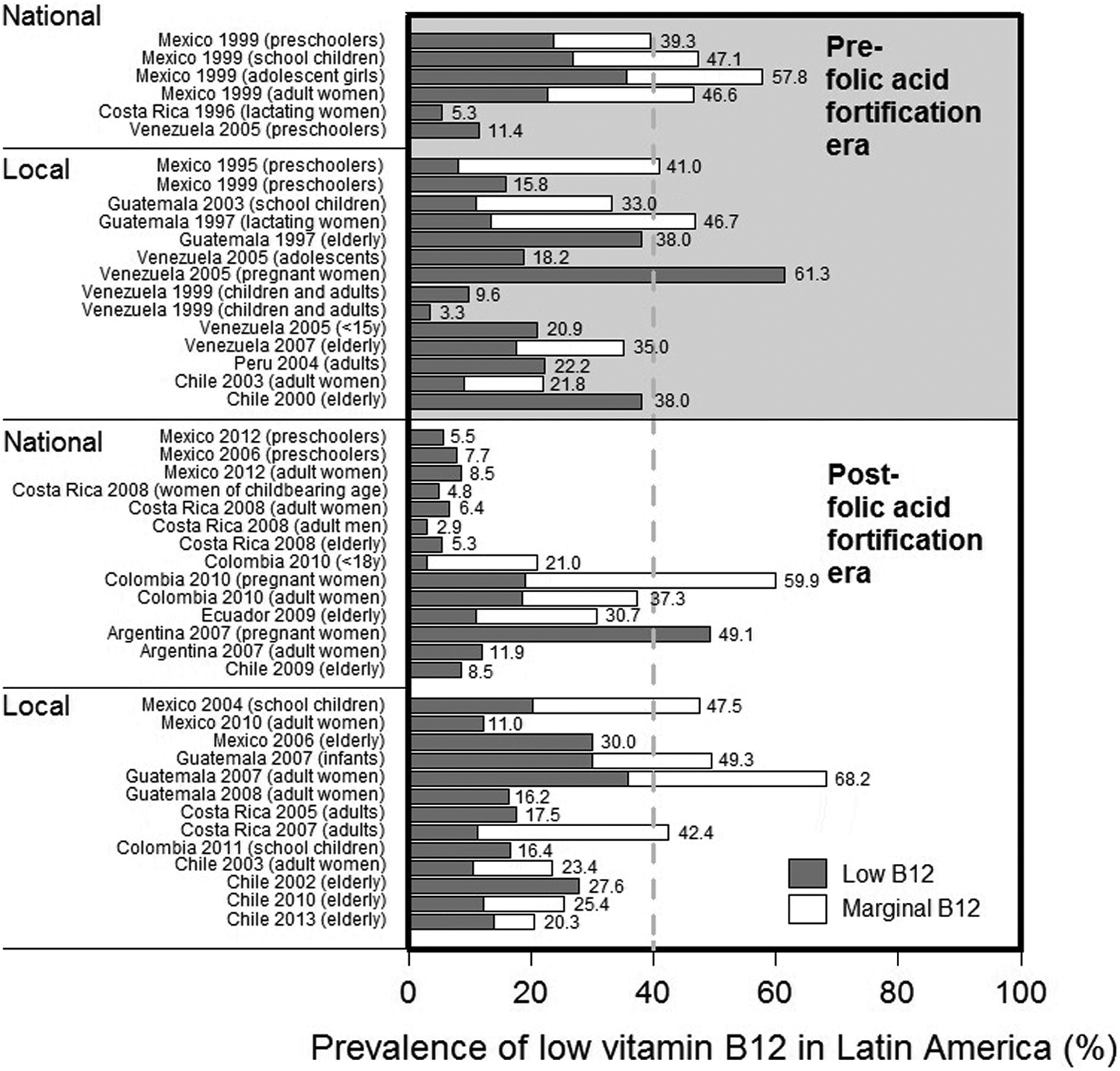
Prevalence of low vitamin B12 before and after folic acid fortification in Latin America and the Caribbean. Low vitamin B12 was defined as vitamin B12 < 148 pmol/L and marginal vitamin B12 status as vitamin B12 between 148 and 221 pmol/L.
After folic acid fortification, national data from Mexico indicated rates of low vitamin B12 of 6% in 2012 and 8% in 2006 among preschoolers, and 9% in 2012 among adult women 37 (Dr. Salvador Villalpando, personal communication). In Costa Rica, the prevalence of low vitamin B12 values (< 148 pmol/L) was 5%, 7%, 3%, and 5% among women of childbearing age, adult women, adult men, and the elderly, respectively. 39 In Colombia, the prevalence of vitamin B12 values < 221 pmol/L was 21%, 30%, and 37% among people < 18 years of age, pregnant women, and adult women, respectively. 53 In Ecuador, the prevalence of vitamin B12 values < 221 pmol/L was 31%. 54 In Argentina, 49% of pregnant women and 12% of adult women presented with low vitamin B12, while in Chile 9% of older people presented with vitamin B12 < 148 pmol/L. 39,40,55 Local studies in Mexico, Guatemala, Costa Rica, Colombia, and Chile conducted on multiple age groups indicate a range of rates of low and marginal vitamin B12 status of 11% to 68%. 30,41–45,47,48,50,51,56,57
Discussion
The intention of this review is to provide an indication of folate and vitamin B12 status in Latin America and the Caribbean covering the pre- and post-folic acid fortification era. Our interpretation is based substantially on national or state-level data collected in Argentina, Chile, Colombia, Costa Rica, Mexico, and Venezuela. No representative data were found from the Caribbean, with the exception of Cuba. The prevalence data indicated that folate deficiency is not a public health problem in Latin America, thereby suggesting the successful provision of folic acid to women of childbearing-age. In addition, there is a reasonable amount of evidence that low or marginal vitamin B12 status still remains in most locations and across population groups.
In 1998, the United States and Canada started mandatory folic acid fortification programs to prevent neural tube birth defects. At least 81 countries have adopted this intervention 58 , including most of the countries in Latin America. Today the high rates of low and marginal vitamin B12 status still remain during this time of high implementation of folic acid fortification among Latin American countries. Although the consequences of the interaction between vitamin B12 and folate status are not yet fully understood, high folate status has been implicated as exacerbating vitamin B12 deficiency. Analyses of National Health and Nutrition Examination Survey (NHANES) data in the United States have shown a higher risk of anemia and cognitive impairment among the elderly in the highest and lowest extremes of the distributions of serum folate and vitamin B12, respectively. 59 Data from NHANES showed that in the elderly, 59 as well as specifically in elderly Hispanics in California, 60 the combination of low serum vitamin B12 and elevated serum folate was associated with higher concentrations of methylmalonic acid and homocysteine. This may suggest that high folate status results in more pronounced vitamin B12 deficiency. There is also some evidence that high folate status negatively affects the response to vitamin B12 treatment among those who are vitamin B12 deficient. For example, in asymptomatic Chilean elderly with poor vitamin B12 status whose conductivity in myelinated peripheral nerves improved after vitamin B12 treatment, there was a weaker improvement in vitamin B12 status biomarkers when serum folate values were higher than the median at baseline (≥ 33.9 nmol/L). This baseline value is less than the serum folate cut point used to indicate high status in most of the studies focused on interactions between folate and vitamin B12. 61 Concerns about excess folic acid exposure have also been extended to further investigate the influence of unmetabolized folic acid and are not only limited to exacerbation of vitamin B12 deficiency, but also extend to other conditions such as the promotion of cancer progression and impaired immune function. 62–64 It must be recognized, however, that none of these possible negative effects have been definitively proven, unlike the indisputable benefits of preventing neural tube defects by increasing the folic acid supply. Meanwhile, a logical strategy may be to include vitamin B12 along with folic acid in flour fortification programs, where a need for additional vitamin B12 has been established. This could have multiple benefits, including further reduction in neural tube defects, improved vitamin B12 levels in breastmilk and among mothers and young children, and prevention of cognitive decline in the elderly. 65
Folate and vitamin B12 status has been extensively studied in some other countries. One of the largest representative samples available is that which was collected by NHANES. Data from NHANES 2003–2006 indicated that the adjusted geometric mean concentrations of serum folate and vitamin B12 were 21.3 nmol/L (95% CI, 20.8 to 21.8) and 304.1 pmol/L (95% CI, 295.9 to 312.2), respectively, among adults aged 19 years or older who had a regular intake of enriched cereal grain products. 66 In this group, 21.9% (95% CI, 19.1% to 24.7%) had serum vitamin B12 values under 221 pmol/L, a lower percentage than many of the available values from Latin America. These data suggest that the current situation in many Latin American countries is not dissimilar to that of North America.
The indicators currently in use to define folate status in Latin America and the Caribbean have limitations. Concerns exist over assay variability and validity for serum or plasma folate. 67 Despite these concerns, blood folate concentrations are the most commonly used indicators at the population level. Most of the identified studies in Latin America and the Caribbean define folate status based on single measurements of serum or plasma folate. Few studies have incorporated red blood cell folate measurements. This is regrettable, since it has recently been established that a red blood cell folate concentration above 1,000 nmol/L is optimal for the prevention of neural tube defects. 68 It is suggested that this value be used in the future to evaluate the need for folic acid fortification and the impact of fortification programs. An equivalent cut point for serum folate could not be established. Vitamin B12 status in Latin America and the Caribbean and elsewhere is predominantly assessed by total serum or plasma vitamin B12 because of the simplicity and low cost of the method. However, the sensitivity and specificity of this method are also questionable. Today it is possible to measure other biomarkers of vitamin B12 status, such as methylmalonic acid (MMA), holotranscobalamin (holoTC), and total plasma homocysteine (tHcy). In general, vitamin B12 deficiency results in low concentrations of total serum vitamin B12 and holoTC, accompanied by high MMA and tHcy. The use of these biomarkers has not been extensively applied to evaluating vitamin B12 status in Latin America. The “combined indicator of vitamin B12 status” 69 is a novel approach to defining vitamin B12 status more accurately, based on combining two, three, or four biomarkers (out of total vitamin B12, MMA, holoTC, or tHcy) into one value.
It is necessary to be cautious with our preliminary conclusions from this systematic review, because the available data are limited and in most cases are not representative of the national situation within each country. Moreover, there are no recommendations as to how to define the prevalence of folate or vitamin B12 deficiency as a public health problem, or on the cut point for serum or plasma folate that defines a high level. Therefore, presentation of the available evidence is centered on deficiencies more than on the entire distribution of folate or vitamin B12 status. Some studies utilized data as a linear variable and prevalence data were therefore missing. In many cases, the reason for this was that there are less well-defined cut points for deficiencies of vitamin B12 and folate in specific age and physiological groups, such as children or pregnant women. Although we classified the studies according to whether they were conducted in the pre- or post-folic acid fortification era, the nature of the data does not allow exploration of changes over time. The review is limited to descriptions more than comparisons due to the few available studies that included follow-up data, as well as multiple factors such as different laboratory methods and age differences, among others.
In summary, the present computer-based systematic search of studies, complemented by national health data, updates the current picture concerning folate and vitamin B12 status in Latin America. It is important to note that there were few studies assessing folate and vitamin B12 status in the Caribbean. This review finds that folate deficiency is no longer a public health problem; however, poor vitamin B12 status seems to remain a public health problem. Better national data to clarify folate and vitamin B12 status in Latin America and the Caribbean are needed. In the case of folate, we recommend reporting the distribution of folate status, rather than focusing entirely on rates of deficiency, and adding red blood cell folate as a status measure. The definition of vitamin B12 status should be based on the inclusion of at least one extra biomarker (preferably holoTC or MMA) in addition to total serum vitamin B12, since recent research indicates that the use of combined indicators can more accurately assess vitamin B12 status. The information to be collected still needs to be focused on the entire life span, especially in groups at risk, such as older people, infants, and pregnant and lactating women. Consensus is needed to define the public health problem of deficiency for these two vitamins. Also required are cut points for deficiency in different age and physiological status groups, a cut point for elevated serum or plasma folate, and scientific bases to define excess.
Conclusions
Folate deficiency in Latin America and the Caribbean appears not to be a public health problem after the introduction of folic acid fortification. However, there is some indication that high rates of low or marginal vitamin B12 status remain in most locations and across population groups. Adding vitamin B12 as a fortificant with folic acid may be the best strategy in areas where vitamin B12 deficiency is an established concern.
Footnotes
Authors’ Contributions
Alex Brito, Manuel Olivares, Daniel López de Romaña, and Lindsay H. Allen designed the study; all authors interpreted the data and helped to prepare the manuscript; Lindsay H. Allen and Alex Brito had primary responsibility for the final content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Héctor Cori is Nutrition Science Director in Latin America for DSM Nutritional Products.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DSM Nutritional Products provided funding for this study.