
Abstract
Background:
Micronutrient deficiencies in Latin America are a public health concern, nonetheless, lack of information still exists in many countries, so that the true magnitude of the problem remains uncertain.
Objective:
To summarise experiences that can inform the development of policies and programs to address micronutrient deficiencies throung supplementation in pregnant women and chlidren under five years of age in Latin American.
Methods:
Review of the most evidence on the effects of micronutrients supplementation, focusing on pregnant women and children under five years of age.
Results:
Certain population groups, as women of reproductive age and children under 2 years of age, are at increased risk for deficiency due to their high micronutrient requirements. This is compounded by the limited access to micronutrient-rich foods for many people living in vulnerable situations. Micronutrient supplementation is an effective intervention to prevent and treat deficiency and to mitigate its adverse effects on health, nutrition, and pregnancy outcomes in micronutrient-deficient populations. The potential benefits of supplementation programs, however, are realized only when they reach those who have the potential to benefit, that is, with inadequate intakes of micronutrients from dietary sources, and when the quality of design and delivery of the programs aresufficient to reach that population timely, regularly, and effectively to enable and motivate consumption.
Conclusions:
Several resources and experiences exist that can help favor the development of programs that can realize this biological and programmatic potential. There is need for continuous efforts to augment coverage and achieve results that can translate into economic benefits for individuals, families, and nations.
Plain language title
Correcting Vitamin and Mineral Deficiencies in Pregnant Women and Children in Latin America
Plain language summary
Previous articles in this supplement have highlighted the importance of micronutrient (vitamin and mineral) deficiencies in Latin America, their causes and effects in different population groups, and some alternatives for their prevention and control. At certain stages of life, particularly during the first 1000 days (from pregnancy to 2 years of age), high nutrient requirements predispose to nutritional deficiencies. This is exacerbated by the limited access to healthy foods for populations living in vulnerable situations. Dietary supplements are therefore an effective strategy for preventing and treating deficiencies and mitigating their adverse effects on the nutrition and health of the population. In this article, we review the most recent estimates on the prevalence of nutrient deficiencies, with a focus on pregnant women and children under 2 years of age; the types of supplements available, and the international recommendations for supplementation during this period of life. There is strong evidence for several benefits of short-term supplementation. In pregnant women, vitamin and mineral levels are improved and a healthy pregnancy is achieved. In children, vitamin and mineral levels are also improved, and some (such as iron and zinc) improve growth and development. In the long term, there are economic benefits for individuals, families, and nations. Several recommendations from studies and supplementation programs are also discussed. Although nutritional supplementation can be cost-effective, benefits will only be achieved if the types and formulations of supplements meet the assessed nutritional needs of the population and if a program is properly designed and implemented. Similarly, programs that include supplements need to be monitored and evaluated to ensure that supplements are taken regularly and for long enough to achieve these benefits.
Introduction
Vitamins and minerals (micronutrients) were first discovered as essential agents to address specific deficiency diseases and syndromes. These discoveries laid the foundation for growing evidence of the importance of micronutrients in a wide variety of biological processes and eventually for the setting of dietary requirements and development of interventions to address inadequacies such as food fortification and supplementation. 1
Micronutrient deficiencies are common in low- and middle-income countries (LMIC) and are not always clinically apparent nor dependent on food supply and consumption patterns, hence so-called “silent epidemics.” They are associated with physiological effects of added nutrients demands during pregnancy, lactation, and rapid growth stages, making teenage women, women of reproductive age (WRA), and young children high-risk groups. 2 Regional estimates showed that Africa has the highest prevalence of vitamin A deficiency (VAD; 1995-2005), zinc deficiency (2005), and iron deficiency (ID; 2011) (ie, 41.6%, 23.9%, and 20.2%, respectively); while Oceania has the lowest (ie, 12.6%, 5.7%, and 15.4% respectively) for same years. 3 A recent study, estimated that there are 1.2 billion (1.0-1.4) nonpregnant WRA and 372 million (95% uncertainty interval 319-425) preschool-aged children (aged 6-59 months) with one or more micronutrient deficiencies worldwide. 4 Current, representative data are unavailable for the region. Specific estimates based on pooled data from 5 Latin American countries showed that prevalence of deficiencies in one or more of 3 core micronutrients (ie, iron, folate, zinc) was 63% (47, 79) in nonpregnant WRA and 48% (38, 58) in preschool-aged children in the period 2003 to 2019. Prevalence varied widely among countries, for example among nonpregnant WRA, ID was 17% in Ecuador (2012), 16% in Guatemala (2013-2016), and 35% in Mexico (2006), while zinc deficiency was 57%, 25%, and 29%, respectively for same years. In preschool-aged children, ID was 14% in Colombia (2010), 11% in Ecuador (2012), 11% in Guatemala (2013-2016), and 35% in Mexico (2006), while zinc deficiency was 39%, 28%, 25%, and 27%, respectively for same years. 4
Lack of current information on micronutrient deficiencies still exists in many countries, so that the true magnitude of the problem remains uncertain, indicative of an insufficiently addressed or monitored public health problem, as noted in this supplement. Frequency of data collection in countries that have reported data is very low, even for micronutrients for which more information is available (ie, iron and vitamin A). Information for other population groups is often lacking too. Besides the high costs and logistical pressures involved in specimen collection, there is also limited understanding of the importance of micronutrients for health and use of this information for program planning. 5 As a result, the information available for most micronutrient status biomarkers is often outdated.
The short- and long-term consequences of micronutrient deficiencies are well documented. Briefly, folate deficiency in women during the periconceptional period increases the risk of neural tube defects and other congenital malformations. 6 Anemia and ID during pregnancy are associated with low birth weight (LBW) and its consequences for infant survival and development, metabolic disease in adulthood, and when anemia is severe (Hb < 7.0 g/dL) 7 increased risk of maternal mortality. 8,9 Vitamin A, vitamin D, and zinc deficiencies increase susceptibility to severe infectious diseases. 10,11 Multiple micronutrient deficiencies, such as iron, iodine, thiamine, and B12, among others, rarely occur 12 and affect cognitive and motor development in children, and in some cases, these may also affect cognitive function in adults. 6 Because of the data limitations, the true burden of micronutrient malnutrition is not well quantified, limiting the ability to accurately estimate the related burden of morbidity and mortality. 13 Evidence on the complex relationship between nutrition during pregnancy and fetal and infant development continues to accumulate, and micronutrient deficiencies are only part of the picture, accounting for a wide range of adverse fetal outcomes. 14 For example, in undernourished populations, balanced energy and protein dietary supplementation is recommended for pregnant women to reduce the risk of stillbirths and small-for-gestational-age neonates. 15
The determinants of micronutrient deficiencies in pregnant women and children under 5 include their increased nutrient requirements, particularly during the first 1000 days, and their high susceptibility to inadequate diets leading to insufficiency of many nutrients. Complementary feeding practices in children aged 6 to 24 months may result in inadequate dietary intakes of iron, calcium, vitamin A, and zinc, among others. 16 Good nutrition during the first 1000 days of life is critical for long-term health and national economies. Well-nourished and active children are less likely to be overweight or obese, more likely to complete 4.6 extra years of schooling, earn 21% higher more as adults, and have a lower risk of preventable health problems as adults. 17,18
The importance of nutrition-related health outcomes and targets for assessing progress toward their elimination are captured in the Global Nutrition Targets (2025) 19 and Sustainable Development Goal 2 (2030). 20 According to the most recent assessment, most countries in the Region are currently off track to meet the Global Nutrition Target of 50% reduction of anemia in WRA (pregnant and nonpregnant women) by 2025. 17 Evidence also shows that the prevalence of LBW remains high in 360 cities in Latin America. 21 Several countries in the Region will not meet the goals for 2025, for example in terms of maternal mortality (World Health Organization). 22
Accelerating efforts to prevent micronutrient deficiencies and their consequences, such as spina bifida, through food fortification and/or micronutrient supplementation have recently been called for, 23 since usually no basic change occurs in the composition of pregnant women’s diets. 24,25 There are effective alternatives to improve health, nutrition, and pregnancy outcomes in micronutrient-deficient populations, such as iron and folic acid supplementation (IFAS) or multiple micronutrients supplementation (MMS). The potential benefits of these programs, however, are realized only when (1) they reach those who have the potential to benefit, that is, with inadequate intakes of micronutrients from dietary sources, and (2) when the quality of design and delivery of the programs is sufficient to reach that population timely, regularly, and effectively to enable and motivate consumption. In the next sections we review resources and experiences that can help favor the development of policies and programs that can realize this biological and programmatic potential.
Supplementation During the First 1000 Days in the Context of Global Recommendations
The WHO has developed a variety of recommendations for consideration by countries depending on the specific issues prevalent in their context. Of relevance to the region, for example, WHO recommends daily IFAS for all pregnant women as part of standard antenatal care (ANC). However, a recently updated WHO recommendation
26
is to provide multiple micronutrient supplementation (containing iron and folic acid) or IFAS on an intermittent basis, in the context of rigorous research (note 1) in LMICs. Intermittent IFAS is associated with fewer side effects and reduced the risk of high levels of Hb in mid and late pregnancy, although the risk of mild anemia near term was increased.
27
The updated recommendation draws on new evidence on MMS in pregnancy and showed a reduction in LBW and probably a reduction in small for gestational age (SGA) babies and preterm births in some contexts
28
but also recognizes that further research is needed. Such research may include controlled clinical trials in which early pregnancy ultrasound is used to establish gestational age with certainty, with assessment of critical maternal and perinatal outcomes, and follow-up of infants sustained into childhood; and where programs of MMS are being considered, implementation research to establish the impact of switching from IFA supplements to MMS, including evaluation of acceptability, feasibility, sustainability, equity, and cost-effectiveness. Other WHO recommendations for pregnant women include: Daily or weekly vitamin A supplementation during pregnancy in areas where VAD is a severe public health problem (if 5% or more of women in a population have a history of night blindness in their most recent pregnancy in the previous 3 to 5 years that ended in a live birth, or if 20% or more of pregnant women have a serum retinol level below 0.70 µmol/L)
29
to prevent night blindness.
24
Zinc supplementation only in the context of rigorous research (not as a routine part of antenatal care [ANC]) to improve our knowledge of its effect in pregnant women, particularly on how zinc status is affected by other nutritional supplementation (eg, iron and/or calcium) given as part of routine ANC. Research is also needed on the effects of zinc supplementation on maternal and neonatal outcomes.
30
Daily calcium supplementation for the prevention of hypertensive disorders that complicate pregnancy such as preeclampsia and eclampsia, major causes of maternal and perinatal mortality and morbidity.
31
Daily vitamin D supplementation for pregnant women with suspected vitamin D deficiency; vitamin D supplements may be given at the current recommended nutrient intake (RNI) of 200 IU (5 µg) per day. This may include women in populations where sun exposure is limited.
32
Disadvantaged pregnant women and adolescent girls in humanitarian and emergency settings may also benefit from individual or MMS to improve their overall nutritional status and to address maternal and neonatal health inequalities.
24
There are also several WHO recommendations for infants and young children to help countries achieve global targets and to improve children’s health and well-being
33
: Daily iron supplementation is recommended as a public health intervention in infants and young children aged 6 to 23 months and preschool-age children aged 24 to 59 months, living in settings where anemia is highly prevalent, for preventing ID and anemia.
34
Twice-yearly high-dose vitamin A supplementation for infants aged 6 to 23 months in settings where vitamin A is a public health problem.
35
Point-of-use fortification of complementary foods with multiple micronutrient powders (MMP) for infants and young children aged 6 to 23 months is recommended by WHO to improve iron status and reduce anemia.
36
Anemia is usually caused by ID, but deficiency of other micronutrients may also contribute such as folic acid, and vitamin B12; or factors such as malaria, soil-transmitted helminths, other infections, and inherited hemoglobin disorders may also contribute. There is not enough evidence, or the existing has not been reviewed yet, to make a global recommendation for the use of lipid-based nutrient supplements,
37
or for preventive or therapeutic supplementation with vitamin D
38
or zinc.
39
Using Global Supplementation Recommendations and Existing Evidence to Select the Right Supplement
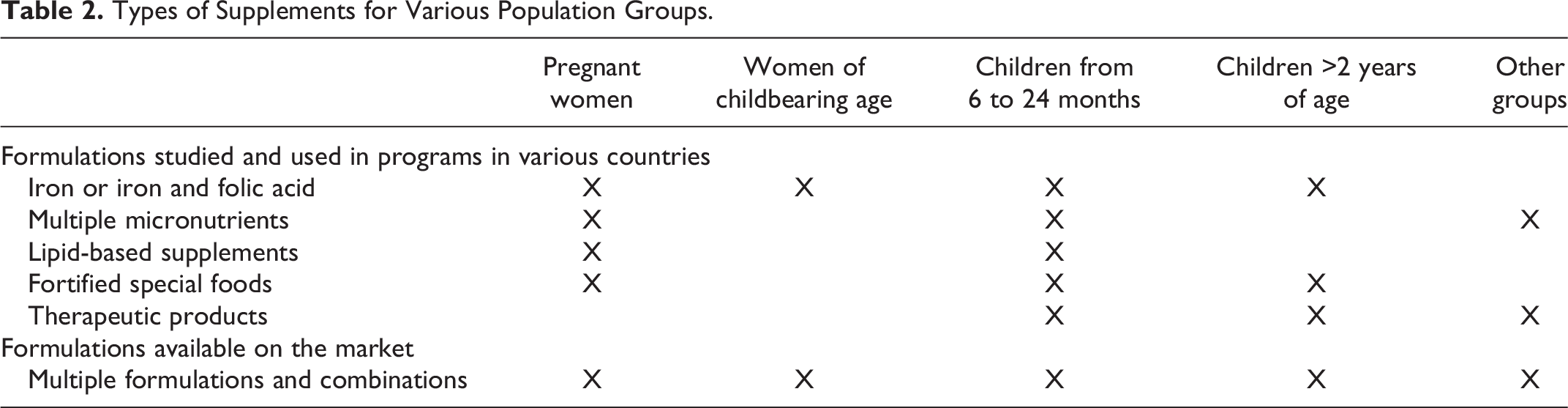
While an essential first step is to critically review available national or local data and global recommendations, the desired outcomes (ie, low-birth weight or growth) and reference points should also be identified. Data to assess the nutritional status of children and WRA may include the prevalence of deficiencies and their co-occurrence, the coexistence of diseases, and dietary intake of energy and other macronutrients and their adequacy. Several nutrients tend to be deficient in the diets of children between the aged 6 and 24 months in many LMICs (Table 1). 15 A comprehensive analysis of types of supplementation (Table 2) and schemes, including a combination of doses, compounds, duration, and target population for implementation, should follow.
Deficient Micronutrients in the Diets of Children 6 to 24 Months of Age in LMICs.a
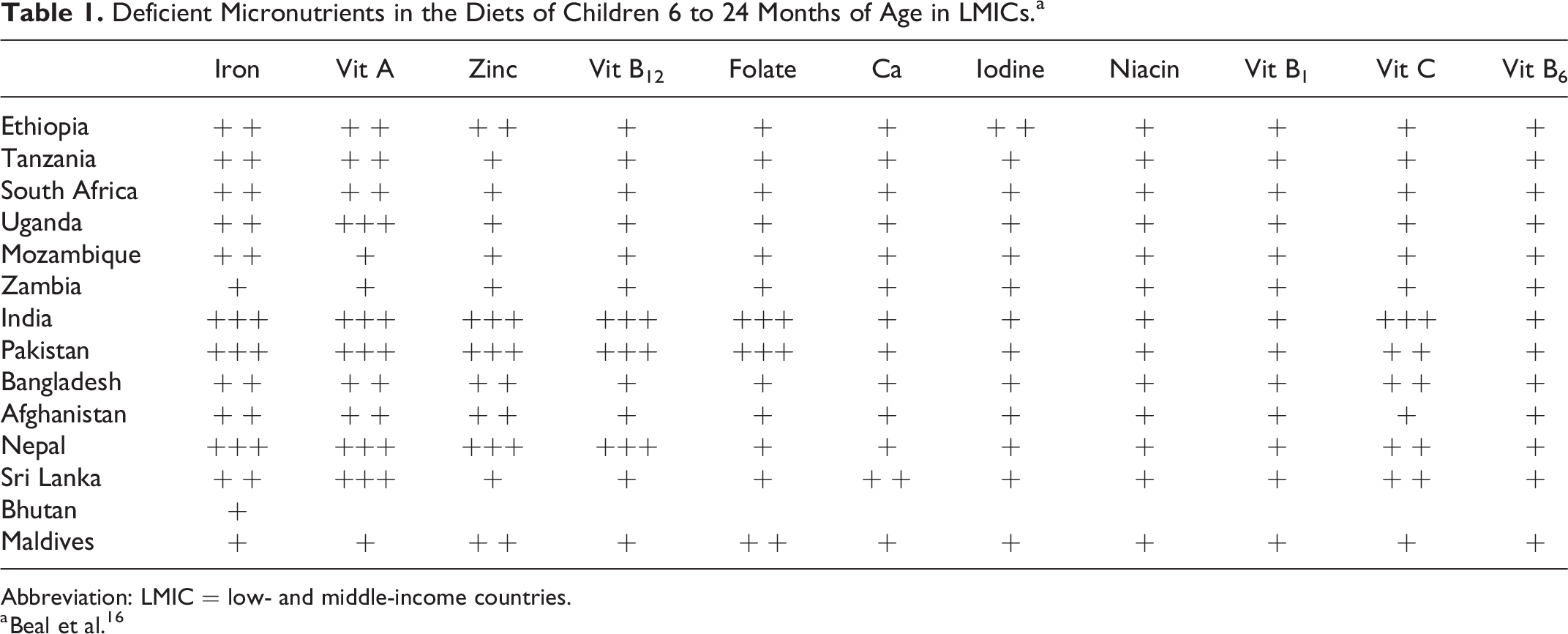
Abbreviation: LMIC = low- and middle-income countries.
a Beal et al. 16
Types of Supplements for Various Population Groups.
The effectiveness of previous supplementation programs and trials can also support the selection of an appropriate supplementation intervention in each context. Pilot programs among pregnant women in LMICs have used MMS containing 13 to 15 micronutrients (including iron and folic acid) and the widely available United Nations International Multiple Micronutrient Antenatal Preparation (UNIMMAP), which contains 15 micronutrients, including 30 mg of iron and 0.4 mg of folic acid. 40 UNIMMAP is a MMS tablet available from the United Nations Children’s Fund (UNICEF) that was specifically designed to improve pregnancy outcomes or supplement treatment of moderate acute malnutrition in women and not for use in children, as it contains high levels of vitamin A and iron. 41 Results using UNIMMAP-MMS have shown a 13% reduction in the risk of LBW and 9% reduction in the risk of SGA babies compared with IFAS. 42 Iron doses in MMS are lower compared to the recommended dose for IFAS, which has potential implications for the expected outcomes and side effects (eg, nausea, vomiting, among others). However, outside the places of detention conditions, logistics and investment in securing a threshold of compliance that would achieve an acceptable proportion of the “ideal” results must be considered, piloted, and budgeted for if justified by results. Multiple micronutrients supplementation can be part of comprehensive ANC or targeted at vulnerable groups, both of which require awareness raising, effective delivery, continuous quality care, counselling and support for women. 43
Evidence of a direct effect for MMS from 3 meta-analysis showed mixed results. Of 6 trials included in a meta-analysis, only 1 showed a smaller increase in vomiting in the MMS group compared with the IFAS group, and in 10 trials the difference in adherence between the MMS and IFAS groups was similar between groups (less than 2%). 30 Using individual patient data in another meta-analysis, subgroup analysis on several outcomes with MMS compared with IFAS showed a reduction in neonatal mortality in women, greater birth outcome benefits for infants born to undernourished and anemic pregnant women, and greater overall benefits for women who started supplementation early in pregnancy (ie, before 20 weeks’ gestation) and had higher adherence. 44 Another meta-analysis of data from pregnant women in Sub-Saharan found an overall prevalence of compliance to IFAS among pregnant women of 39.2%. This high adherence was further favored by counseling on IFAS during pregnancy, which resulted in women being 1.96 times more likely to adhere to IFAS than women who did not receive counseling. 45
Other Considerations to Address Micronutrient Deficiencies
In settings where micronutrient deficiencies and dietary inadequacies exist or coexist, supplementation of pregnant women has been shown to be the best bet for development and to improve several maternal and child outcomes. 46 However, making informed decisions to select the right supplement from available options, establishing expected outcomes, and designing and implementing the intervention are likely not enough, as other complementary considerations such as cost-effectiveness, evidence-based advocacy for policy change and government commitment, behavior change communication, serious monitoring/surveillance and evaluation for program management, and securing financial resources are crucial. The WHO/Centers for Disease Control and Prevention Logic Model for Effective Project Management and Monitoring and Evaluation for Micronutrient Interventions can be useful to incorporate all the necessary components. 47 According to the model, most micronutrient programs are expected to follow certain intervention processes. It has been suggested that, at a minimum, most programs should include indicators related to the monitoring of supply, coverage, and adherence of supplementation, and that policy indicators are also critical when transitioning from an IFAS to MMS program. 48
Other existing interventions such as dietary diversification, through education and dissemination of food-based dietary guidelines, 49 staple crop biofortification (eg, zinc-maize, iron-beans, zinc-rice, etc), 50 and large-scale food fortification, 51 for example with some vitamins such as folic acid and vitamin B12, may also be considered as some have already been implemented in the Region. 35 In some cases, supplementation may not be sufficient or timely for some outcomes, that is, to prevent neural tube defects 52 or even anemia in many pregnant adolescent girls, and LSFF may be effective in these scenarios. In other cases, micronutrient intake may improve among children who consumed fortified foods, but the pattern of use may limit frequency and quantity consumed or there may be substantial diversity in the prevalence of undernutrition combined with an increased risk of overweight and obesity among women. In these contexts, fortified foods may be substituted for MMS, 53 to reduce costs without compromising the potential for impact in pregnant women and children under 24 months of age. 54
Micronutrient supplementation can also be integrated into or indirectly influenced by existing programs. For example, micronutrient supplements can be used to motivate women to attend antenatal and postnatal care, promote growth monitoring visits, be distributed through school programs, or be included in food assistance programs or social protection programs that may have well-established delivery systems that can be leveraged to provide supplements to eligible WRA and children.
Conclusions
There is considerable evidence of the diverse and profound benefits of micronutrient supplementation in WRA and children, particularly during the first 1000 days of life. Evidence on the magnitude and distribution of micronutrient deficiencies is sparse and insufficient to make a statement about the public health importance of most, if not all, micronutrient deficiencies in the Region. Given their potential impact, a call to urgent action, leading off with the strengthening of monitoring and evaluation systems (for existing national programs with supplementation, LSFF, etc) and micronutrient deficiencies indicators added ex officio to regular national surveys is a moral responsibility of governments and development agencies. To waste resources on unnecessary or ineffective interventions is just as bad as neglecting the problems.
In the short term, supplementation improves WRA micronutrient status and pregnancy outcomes, and in children, also improves micronutrient status, and growth and development (depending on the type of supplement). In the long-term, these results translate into economic benefits for individuals, families, and nations.
Today, MMS is the international recommendation for addressing micronutrient deficiencies in at risk settings for vulnerable pregnant women, and point-of-use fortification of complementary foods with MMP for vulnerable infants and young children aged 6 to 23 months.
Supplementation interventions have been sporadic, and there is lack of comprehensive and continuous policy to address micronutrient deficiencies. However, a supplementation program should be properly designed, implemented, monitored, and evaluated when there is supporting evidence of single or multiple micronutrient deficiencies in the population, not because the intervention exists or can be claimed to exist. The benefits of micronutrient supplementation will only be realized if products and formulations and delivery platforms are tailored to the micronutrients gaps to correct in the target population. There is a “biological potential” to respond to supplementation and a “programmatic potential,” if programs are designed to fully cover the target population, to achieve regular supplementation supply and consumption from those who will benefit, and for an adequate period to achieve these benefits.
As a result, some supplementation programs have been successful, but others have not, generally due to limited access, low coverage, and reduced adherence to the recommended regimens and counseling. There is a need for capacity to address the challenges of planning, implementing, and monitoring a micronutrient supplementation program and to assess the impact of these interventions on the population.
Footnotes
Authors’ Note
This report was presented at the seminar “Micronutrientes en América Latina” organized by the Fundación Iberoamericana de Nutrición—FINUT. The manuscript is an original work and has not been submitted for publication elsewhere. The views expressed in this publication are those of the author(s) and do not necessarily reflect the views of FAO.
Author contributions
LMN contributed to conception and design; ACFG, LNM, and AGG contributed to analysis and interpretation, draft manuscript, critically revised manuscript, gave final version and agree to be accountable for all aspects of work ensuring and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the publication of this article from Fundación Iberoamericana de Nutrición -FINUT-.