
Abstract
Background:
School feeding programs (SFPs) can play a crucial role in the emergency food and nutrition response, but there is a dearth of information on how SFPs operate during emergencies.
Design and Methods:
A rapid comparative assessment of 11 SFPs throughout Latin America and the Caribbean during the COVID-19 pandemic. Data from (1) systematic document search and (2) surveys with key informants (n = 23) about barriers/facilitators to modifications were systematically analyzed using a multiple case study approach.
Results:
During the pandemic, all SFPs continued (although continuation plans varied from a few days in Chile to > 1 month in Puerto Rico) via food kits, food vouchers, and/or grab n’ go meals. The SFP implementation was highly dependent on the programs’ autonomy and financial support, which impacted their logistics to acquire and distribute foods during the pandemic. The types of foods offered in some SFPs suggest that established nutritional guidelines were not always followed. Key informants expressed concerns about the deterioration of the nutritional quality of foods offered during the pandemic and lack of community engagement that impeded distribution to the neediest.
Conclusions:
Results underscore the urgency for clear implementation guidance on how to modify SFP during emergencies. Public health implications include (1) allocation of autonomous resources to an intersectoral working group to safeguard nutritional benefits during emergencies, (2) strengthening efforts of SFP community engagement before and during emergencies, and (3) establishing guidelines of the types of foods that can be distributed to meet the nutritional needs of beneficiaries during emergencies.
Introduction
The arrival of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in March 2020 resulted in an unprecedented shock to the global food systems, 1,2 with the number of people living in acute hunger globally expected to double as a result of the pandemic, 3 and the most vulnerable being children. 4 Lockdown mandates and school closures during the pandemic were also expected to pose serious social and health risks, especially for children already living in poverty, who could be negatively affected by increased intake of unhealthy food, further exacerbating disparities in malnutrition in all its forms. 5 -8
School feeding programs (SFPs) are embedded into national protection systems and are essential components for national food and nutrition security policies, 9 playing an important role in improving nutrition in all aspects and serving as a social safety net for children who are most vulnerable to malnutrition. 10,11 The lockdown measures to contain the spread of the SARS-CoV-2 virus resulted in wide school shutdowns that abruptly stopped the established operation protocols for SFP, affecting approximately 87% of the global school population in 2020 12 with documented increased risks for food insecurity. 13 Specifically in the Latin American and the Caribbean (LAC) region, 85 million SPF beneficiaries were impacted by school closures, while governments struggled to continue their programs to mitigate food and nutrition insecurity in these populations while keeping to social distance guidelines. 14,15
The international debate about how to best assure that the food and nutrition needs of schoolchildren are met while containing the spread of the SARS-CoV-2 virus led to the international recommendations about national and subnational responses that could operate under different scenarios. 16 Nonetheless, how SFPs were able to follow and accommodate these recommendations during the pandemic has not been systematically assessed. Learning about the modifications made to SFP implementation during the pandemic, as well as the challenges faced during the pandemic to implement these adaptations, will inform a better response to address food and nutrition security needs during future emergencies.
This study aims to draw out policy lessons by examining how SFPs were redirected toward schoolchildren (6-19 years old) beneficiaries during the COVID-19 pandemic. We used a rapid comparative assessment of modifications made by 11 SFPs in LAC to describe changes made during the unprecedented school closures due to the SARS-CoV-2 pandemic and to document barriers and facilitators during the implementation of these modifications.
Methods
This rapid comparative assessment of SFP modifications employed a multiple case study approach, which guided the data collection, analysis, and interpretation. Case studies are the preferred method when the following 3 criteria are met: (1) The focus is on “how” or “why” questions; (2) an investigator has little control over the events being studied; and (3) the focus is on a contemporary phenomenon within a real-life context. 17
Case Selection
School feeding programs were purposefully selected to showcase a range in human development metrics and malnutrition prevalence, selecting sites where undernutrition coexists with increasing childhood obesity prevalence. 18 In addition, following the case study selection criteria proposed by Yin, 17 cases were finalized according to whether there was sufficient access to pertinent and reliable data to illuminate the research question. The sample thus consists of 10 SFPs in the following countries: Brazil, Chile, Colombia, Costa Rica, Ecuador, Guatemala, Mexico, Peru, Puerto Rico, Uruguay, and one subnational territory (Buenos Aires, Argentina).
Data Collection
The data were collected in 2 phases: (1) systematic document search and review of public information and (2) surveys with key informant/stakeholders in each country to triangulate the data collected from phase 1 and expand upon it with further details.
Four research assistants who were fully fluent in Spanish, English, and Portuguese were trained to systematically search for each country: (1) official national or territorial government web page; (2) official web page for the Department or Ministry of Education and/or Health; (3) social media accounts (Instagram, Facebook, Twitter) of each government and of the ministries mentioned above; (4) web pages of national mainstream newspapers in each country; and (5) social media accounts for national/local newspapers. They were instructed to list the web pages where the information was extracted from and to note if some information was not found.
The information compiled for each country was then discussed with the research team (coauthors) and with invited academics and high-level policy makers who had topical and regional expertise in each case and could verify, add insight, and suggest important secondary sources of information. This process was completed during weekly meetings for a 7-month period in April 2020 to October 2020.
Using an adapted snowballing sampling approach, the research team initially used their professional network, composed mostly of academics and policy makers, in each country to send the survey to (via email). This initial set of key informants was instructed to identify additional respondents who would be knowledgeable of the SFP in their countries and to send them the survey; this is how relevant SFP coordinators and managers in each case were identified. In addition, the research team also utilized data from the document search (phase 1) to identify additional potential respondents and to send them the survey. When needed, the research team followed up with stakeholders via email and phone calls to obtain further clarification.
The survey procedures were exempt from institutional review board under DHHS regulatory Category 2 at the authors’ institute. Survey data collection was completed between November 2020 and April 2021.
Subsequently, information collected during phase 2 was systematically compared to data from phase 1. If there was contradiction in the data collected between phase 1 and phase 2, the research team either recontacted key informants for further clarification or sought the perspective of an additional key informant within that case study. The research team analyzed each case seeking to reach saturation, which was defined as the point at which the collection of additional information (from public sources and from key informant surveys) did not contribute new data to the study and repeated what was obtained previously. 20
Finally, survey responses to the open-ended questions about challenges faced during the implementation of the modifications were compiled in a descriptive manner for each country. Coauthors analyzed these data according to common themes that emerged from the open-ended responses across all SFPs. These were used to triangulate and provide nuance to the information, as well as preliminary insights on the ground-level implementation of SFP.
Results
A total of 23 completed surveys from 11 SFPs across LAC were received (at least 2 surveys per site, except for Ecuador, where only 1 survey was received). Table 1 summarizes data from both phases about the modifications in the implementation of SFPs during the pandemic, and Table 2 shows the foods distributed in the modified SFPs during the pandemic. For all cases, reports of the first confirmed COVID-19 case spanned between February 26, 2020 (Brazil) and March 14, 2020 (Colombia and Guatemala). The number of days between school closures and authorizations to restart the SFP varied with the shortest adjustment period occurring in Chile (2 days) and the latest one occurring in Puerto Rico (44 days). The SFP modifications were supposed to follow the established nutritional regulations and guidelines that existed prepandemic, and some SFPs published pandemic guidelines on how to do this. For example, in Brazil and Uruguay, the SFPs published their national guidelines during the pandemic to inform local- and state-level governments how the new food kits should be delivered to children, emphasizing the need to maintain prepandemic nutritional and food group recommendations, including the restrictions for sugar-sweetened beverages, and other high-fat, high-sodium processed and ultra-processed foods. The case of Peru is worth highlighting because during the pandemic, the SFP provisions were actually bolstered by increasing the diversity of the types of foods provided compared to prepandemic SFP.
Modality of SFP During the Pandemic
Except for Puerto Rico and Uruguay, all other cases modified their SFP to provide food kits. These food kits contained ingredients and food items meant to be prepared/cooked and consumed at the home. In Puerto Rico and Uruguay, “meals” were provided instead of food kits. In the case of Puerto Rico, the SFP was eventually modified to a “grab n’ go” style in which school foods were prepared at some (not all) schools, primarily by school cafeteria personnel, and available for daily pickup. In Uruguay, although the schools were closed, the SFP was available to provide only the lunch portion (cooked) and excluded breakfast and snacks. Two additional modifications are worth mentioning: In rural areas of Uruguay, food vouchers equivalent to the daily cost of the school lunch and redeemable at supermarkets were provided to the families that requested it. This was operational until April 23, 2020, when the rural schools reopened. In Colombia, in addition to food kits, meals and food vouchers were provided. The meals were “ready-to-eat” individualized and prepackaged complementary rations available only for children 9 to 13 years old. The food vouchers were only available in established areas, with a value of $50.000 Colombian pesos (approximately $14 USD) per month and redeemable only for predetermined eligible foods (Table 1).
Adaptations in Coverage/Beneficiaries
During regular, prepandemic times, the age eligibility for enrollment in SFP included children aged 6 to 19 years old, except for the cases of Colombia and Peru, which included children as young as 3 years old, and Buenos Aires, which focused the SFP specifically for children 6 to 11 years old. During pandemic, Buenos Aires and Puerto Rico extended their programs to anyone who requested it (in Puerto Rico, anyone could request a meal regardless of whether or not they were enrolled in the educational system). In a similar manner, Peru passed a series of decrees to allow vulnerable populations of all ages (not just schoolchildren) to participate in the SFP during the pandemic. In contrast, Uruguay and Mexico restricted the use of its SFP during the pandemic to more targeted populations: In Uruguay, the modified SFP was available only to students whose families requested it; in Mexico, there was a recommendation to limit SFP to the most vulnerable families based on a needs and food security assessment made during the pandemic (Table 1).
Distribution Frequency
Table 1 displays the frequency with which SFP foods were distributed during the pandemic according to the type of modality. The frequency of distribution varied depending on the type of modality; for example, in Colombia, food kits and food vouchers were distributed every month, while meals were every 7, 15, and 30 days. Puerto Rico and Uruguay were the only cases to report daily distribution of meals during the pandemic, in agreement with the observation that these were cooked and available for pickup or delivery daily.
Modifications to the Implementation of School Feeding Programs (SFPs) in 11 Latin American and Caribbean Case Studies During the COVID-19 Pandemic.
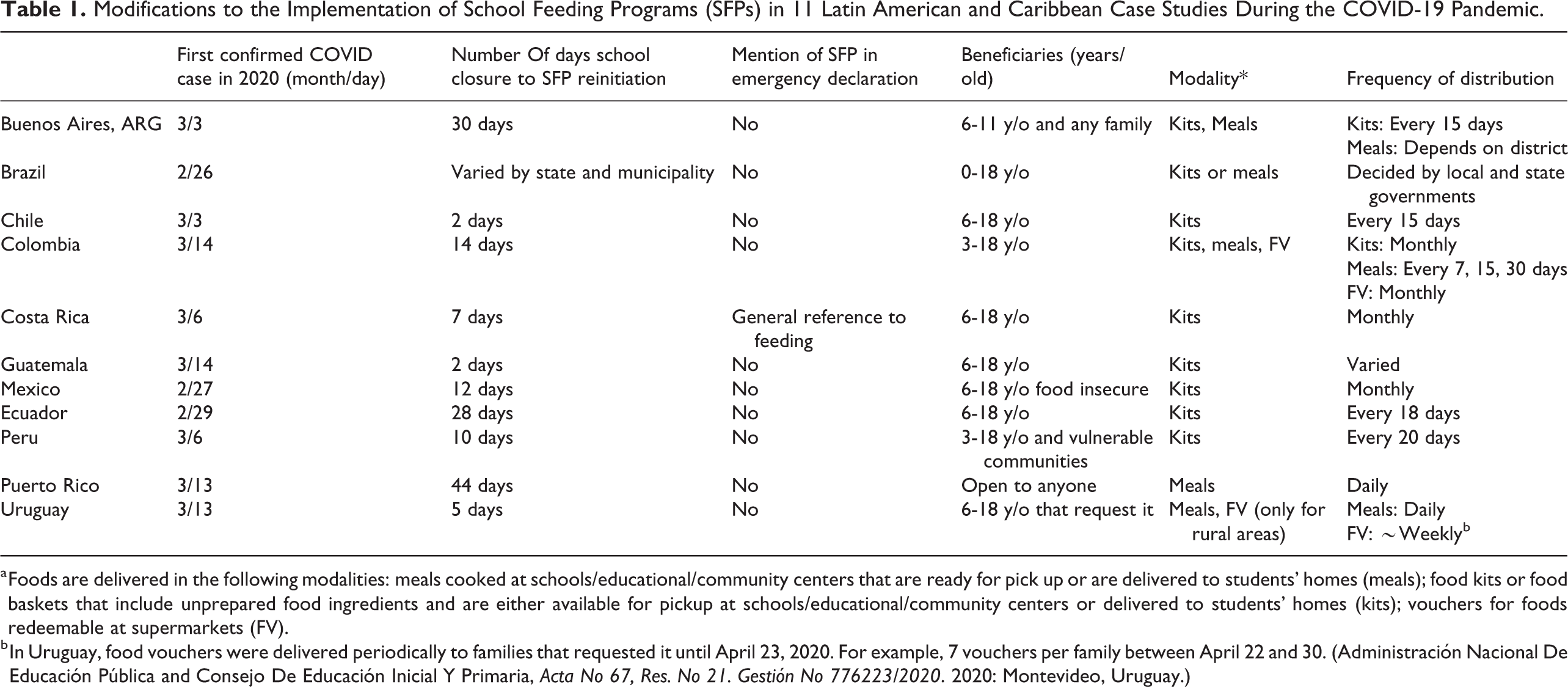
a Foods are delivered in the following modalities: meals cooked at schools/educational/community centers that are ready for pick up or are delivered to students’ homes (meals); food kits or food baskets that include unprepared food ingredients and are either available for pickup at schools/educational/community centers or delivered to students’ homes (kits); vouchers for foods redeemable at supermarkets (FV).
b In Uruguay, food vouchers were delivered periodically to families that requested it until April 23, 2020. For example, 7 vouchers per family between April 22 and 30. (Administración Nacional De Educación Pública and Consejo De Educación Inicial Y Primaria, Acta No 67, Res. No 21. Gestión No 776223/2020. 2020: Montevideo, Uruguay.)
Contents of Food Kits
For the cases that provided food kits, these were supposed to follow the nutritional guidelines established for the SFP prepandemic. Results show that all kits included some form of dairy and grain. Except for Ecuador, all countries also provided fruits and vegetables in the kits, and most (except for Buenos Aires) specified that all or some of these must be fresh. Except for Ecuador, all countries provided pulses/legumes and animal-based proteins; the latter were typically eggs and/or meats/fish, which were often either frozen, canned, or delivered in a pouch format. With the exception of Ecuador, kits also included vegetable oils. In addition, sugar was included in the kits for Buenos Aires, Brazil, Colombia, Chile, Guatemala, and Peru; and salt included in kits for Brazil, Chile, Costa Rica, and Peru. Beverages with added sugars (ie, flavored milks or fruit-flavored beverages) were included in Ecuador and Peru. Sweets and desserts (ie, gelatins, cookies, sweet cereal bars, flans, cakes) were part of the food kits in Buenos Aires, Ecuador, and Peru. In Chile, some kits included artificially sweetened dairy products and beverages (Table 2).
Content of Meals/Grab and Go During the Pandemic
Although the actual implementation or preparation of hot meals and snacks provided by Uruguay, Puerto Rico, and Colombia is unknown, Table 2 documents the menus that existed during the pandemic for Uruguay and Colombia. For Uruguay, this included fruits and vegetables while sugary drinks and desserts were prohibited; for Colombia, the snack guidelines detailed that the provision of a dairy product accompanied with a sweetened grain product or dessert, and a seasonal fruit only if available.
Characteristics of School Feeding Programs (SPFs) Modalities in 11 Latin American and Caribbean Case Studies During the COVID-19 Pandemic.a
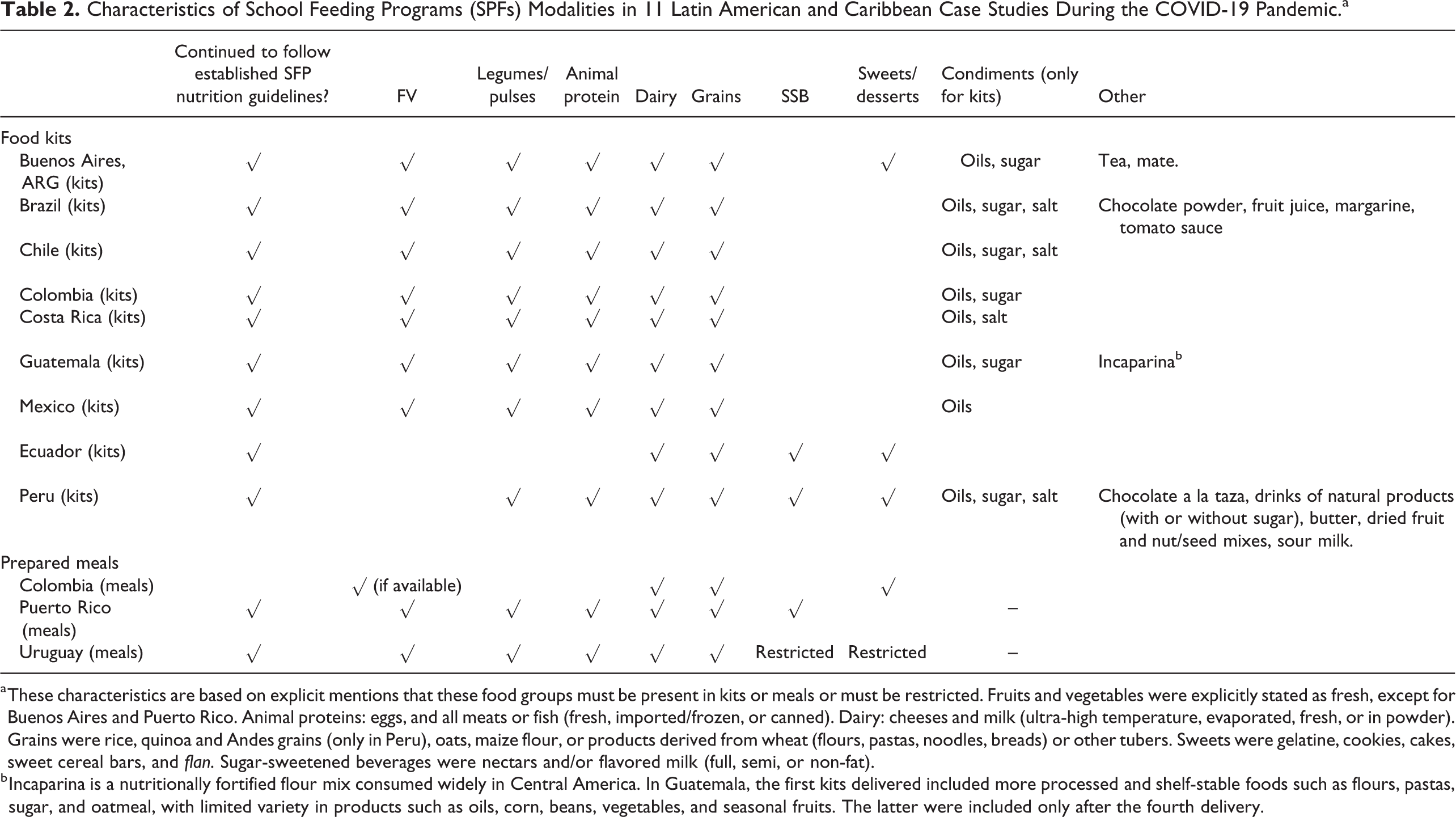
a These characteristics are based on explicit mentions that these food groups must be present in kits or meals or must be restricted. Fruits and vegetables were explicitly stated as fresh, except for Buenos Aires and Puerto Rico. Animal proteins: eggs, and all meats or fish (fresh, imported/frozen, or canned). Dairy: cheeses and milk (ultra-high temperature, evaporated, fresh, or in powder). Grains were rice, quinoa and Andes grains (only in Peru), oats, maize flour, or products derived from wheat (flours, pastas, noodles, breads) or other tubers. Sweets were gelatine, cookies, cakes, sweet cereal bars, and flan. Sugar-sweetened beverages were nectars and/or flavored milk (full, semi, or non-fat).
b Incaparina is a nutritionally fortified flour mix consumed widely in Central America. In Guatemala, the first kits delivered included more processed and shelf-stable foods such as flours, pastas, sugar, and oatmeal, with limited variety in products such as oils, corn, beans, vegetables, and seasonal fruits. The latter were included only after the fourth delivery.
Challenges to Implementing the Modifications to the SFP
Table 3 summarizes descriptions of the themes that emerged among key informants from each SFP when they were asked about challenges or facilitators that they faced during the implementation. One of the factors that was explicitly mentioned as facilitating the continuation of the SFP during the pandemic was that the universal laws of their countries protected the SFP. This is important because stakeholders joined that idea to intersectoral efforts that enabled the SFP modifications to roll out quickly, facilitating the rapid reach of remote and hard-to-reach populations. For example, in Costa Rica, key informants highlighted the collaborative approach taken within institutions to act in a quick manner to modify the SFP. In contrast, in Peru, a challenge was that the SFP is administered under a different ministry than the Ministry of Education, and the uncertainties of school closures and reopening were mentioned as a challenge.
Summarized Themes From the Perspectives From Key Informants/Stakeholders From 11 Governments in Latin America and the Caribbean About the Principal Barriers and Facilitators Faced During the Modifications to the SFP Implementation During the COVID-19 Pandemic.

A shared barrier to the implementation of SFP modifications was flexibility and autonomy allocated to the SFP during prepandemic times, in the face of exacerbated needs during the pandemic. This barrier emerged clearly in various ways in Brazil and Ecuador (budgetary constraints vis-à-vis the needs of the population), in Uruguay (given the deficiencies in equipment and infrastructure) and in Costa Rica (a limited budget could not cover the increase in beneficiaries that happened when schoolchildren from private schools moved to public schools during the pandemic). The SFPs, which were already strained for resources before the pandemic, were required to continue to follow national regulations during the pandemic without provision of additional resources. In addition, they faced price gouging, limited food supplies, and interruptions in food transportation. Key informants related how these challenges impacted the provision of nonperishable fresh foods, increased provision of processed, shelf-stable foods potentially high in added sugars, saturated fats and salt, and compromised the nutritional quality of the foods delivered during the pandemic.
Further, key informants across sites described the importance of relying on local entities and community engagement to reach beneficiaries, especially if these beneficiaries lived in rural and indigenous communities. For example, Uruguay and Guatemala explicitly identified teacher and parent engagement as a critical strength to facilitate the success of the program modification, whereas Puerto Rico and Ecuador mentioned low parent participation and absenteeism from the school personnel as major challenges to implementing the modifications.
It is also important to note that some key informants explicitly mentioned additional feeding services to most the vulnerable populations, such as the case of Uruguay that provided a Copa the Leche program (Glass of Milk) to children who requested it, and for the first time in its national history, the SFP operated even during the school break.
Discussion
Our findings illustrate how 11 SFPs in LAC modified their implementation strategies during the school closures resulting from the COVID-19 pandemic. It also describes the challenges and facilitators that these SFPs faced during the uncertain times that the pandemic created. All SFP made extraordinary efforts to face existing and new hurdles associated with the delivery of SFP to keep feeding schoolchildren during the pandemic. The number of days that transpired between school closures and reinitiation of SFP modalities (ranging from a couple of days in Chile to more than a month later in Puerto Rico) underscore the urgency for strong clear implementation guidance on how to modify SFP during future emergencies to continue to feed schoolchildren. Eventually, all SFP devised and implemented new modalities, which included a mixture of packaged foods in the form of “food kits” for preparation at home, food vouchers to be redeemed in supermarkets, and prepared/cooked meals and snacks that could be picked up by parents in central locations (grab n’ go style). The success of new modalities of the SFP implementation seemed to depend on prepandemic resources, with emphasis on financial support for, and autonomy of, SFP. These resources impacted the success of remaining nimble and navigating logistics to acquire and distribute foods to beneficiaries. Key informants were concerned that, given these logistical challenges, the nutritional quality of the SFP deteriorated during the pandemic.
Considering the recommendations of international organizations to mitigate food and nutrition insecurity during the pandemic, 16 our results can be contextualized to illustrate several broader public health implications for the SFP implementation during future emergencies: (1) the allocation of immediate resources dedicated to safeguarding nutritional benefits during emergencies, (2) strengthening efforts of community engagement before and during emergencies, and (3) establishment of clear guidelines of the types of foods that must be distributed to beneficiaries to meet the emerging nutritional needs during emergencies.
1. Allocation of resources to safeguard nutritional benefits during emergencies
Emerging from the international debate about how to mitigate food and nutrition insecurity during the pandemic, international organizations put forth recommendations for national and subnational governments to establish an intersectoral working group (ie, sectors of health, social protection, education, agriculture) to address the food and nutrition insecurity during this emergency. 16 Our results evidence that a few SFP (Costa Rica, Colombia, Guatemala, Mexico) were involved in intersectoral efforts and collaborations, most notably with the agricultural sector, that facilitated procurement and transportation of foods during the pandemic and enabled some countries to meet the guideline that a percentage of SFP purchases come from local agriculture in order to guarantee income for family farmers. Although some countries created agencies to deal with the public health emergency (see, eg, 21 ), these were not provided independent funds to handle the new feeding emergency and the design of the SFP did not allow or provide guidance for health emergency exceptions. Therefore, as evidenced by our findings and those of others, 22,23 during the very first months of the pandemic, SFP struggled to determine the best way to address nutrition gaps among schoolchildren, especially if they needed to provide fresh produce, suggesting a lack of established guidelines to modify and implement SFP during this emergency. The mention of barriers related to budgetary constraints: limited budget during prepandemic, and no financial autonomy for SFP before or during the pandemic, made it more difficult to quickly respond to the sudden new challenges of food acquisition and distribution. These challenges are not specific to LAC: In Canada, feeding scholars have noted that the SFPs have been chronically under resourced prepandemic and that these programs lack ownership and an institutional home that would allow them for flexibility to act and to advocate for additional resources. 24 The limited autonomy and resources, compounded by the lack of guidance from a central entity, obligated the SFP to figure out the logistics on their own to continue to ensure nutritional benefits. This seemed to be a shared barrier in the published literature on SFP during the pandemic, which is mostly coming from the United States and Europe. To illustrate, in the United States, there was no federal guidance on best practices to encourage continued participation in SFP during the pandemic, resulting in a temporary patchwork of emergency feeding programs that risked leaving the most at-risk populations without coverage. 25 The UK government was also heavily criticized as being unprepared for this emergency, compared to, for example, food distribution before the Second World War, which had placed value on nutritional quality of food and policy intervention across the food chain to ensure equitable distribution. 26
School feeding programs are naturally intersectoral, with roles and responsibilities that range from mitigation of food and nutrition insecurity, improving education, and implementing nutrition and health policy. We agree with other scholars that the unprecedented context of the pandemic opened the room for questions on how to resource and reimagine SFPs as platforms to mitigate food security in the context of future emergencies. 27 Cross-sector collaboration has been identified as a factor that affected the effectiveness of local feeding approaches to serve children and families in the United States during the pandemic. 25 In addition, although not investigated systematically in this study, SFPs have been able to support communities in their food security response to the COVID-19 pandemic in the United States, 28 and in Peru, with the SFP Qali Warma being leveraged to feed communities. 29 This underscores the urgency to examine more systematically how the SFP intersectoral infrastructure can be strengthened and focused to mitigate food and nutrition insecurity during future emergencies. The pandemic offered an opportunity to reflect how we can do better in future emergencies: Given the challenges faced of autonomy and financial flexibility, a financially independent intersectoral working group with the authority and mission to address food and nutrition needs and to provide guidance on best practices for effective feeding of schoolchildren during future emergencies is an important first step. It is important to bear in mind that intersectoral management may introduce multiple and rigid bureaucratic processes that may limit rapid response and action to quickly alleviate the deleterious effects of an emergency. 30 For example, in Brazil, the process of purchasing food from local farmers during the pandemic was reported to be bureaucratic and complicated, despite the fact that there is a legal obligation to do so as part of supporting SFPs. 23 This intersectoral work during emergencies would require processes that encourage iterative problem solving and innovation and stay away from politicking. 31 Creating and strengthening partnerships with existing non-governmental organizations may be a strategy to increase resilience and preparedness for future pandemics. Empirical research will be crucial to examine how such an intersectoral working group would work to implement top-down policies and practices while also remaining nimble to allow for quick local problem solving and consideration of cultural local adaptations, tailoring guidance for locally-driven implementation strategies and drawing from local community knowledge and support. This leads us to our second policy implication:
2. Strengthen efforts of community engagement before and during emergencies
International organizations recommend that these intersectoral working groups evaluate the rapidly evolving situation so that they can provide options for viable responses and engage communities. 16 Our results show that family and community engagement were factors considered to significantly impact the success or failure of reaching the intended SFP beneficiaries during the pandemic. This is an integral aspect of the redesign and delivery of the SFP modality during emergencies. In the United States, a study that examined the effectiveness of emergency feeding approaches in 5 cities reported the need to establish trust and good relationships in order to reach the targeted communities, especially given the fact that most emergency food services were located in predominantly racial/ethnic minorities communities. 25 Our results illustrate the successful establishment of trust with the beneficiary communities, which facilitated the implementation of the new modalities: For example, in Guatemala, parents were part of a legally recognized organization that received financial resources to purchase and deliver foods prepandemic; hence, during the pandemic, these organizations continued to operate and participate and were a key to the success of the modifications.
Although not examined in the current study, it would be critical to assess how the SFPs may complement other community food security responses, especially to mitigate the gaps in feeding that may result from SFP as others have proposed 21,30 and from intrafamilial distribution of foods. In LAC, several countries discussed the inevitable intrafamilial distribution of food kits spurring concerns about whether SFP foods were still meeting the nutritional needs of schoolchildren during the pandemic. 31,32 During the pandemic, some SFPs were leveraged to either complement existing whole community feeding efforts. Three concrete examples come to mind: in Mexico, with the Programa de Asistencia Social Alimentaria a Personas en Situación de Emergencia o Desastre 33 ; in Peru, where Qali Warma resources and infrastructure were also redirected to feed others beyond schoolchildren 29 ; and the case of Puerto Rico where foods were diverted to food banks, at least initially. 19 Part of the efforts to mitigate food and nutrition insecurity in future emergencies must examine emergency feeding from a systems perspective to understand how feeding networks can be activated and work together for the whole family and community, rather than as temporary patchworks that may leave out those who need it most.
3. Establish clear guidelines of the types of foods that must be distributed to beneficiaries to meet their nutritional needs during emergencies.
During the pandemic, international organizations recommended, as much as possible, the avoidance of foods with low nutritional content, including juices with high sugar content, packets of sugar, prepackaged snacks with high saturated fat, and sugars and oil, among others. 16 Although the current study did not conduct an assessment of the nutritional content of foods offered during the pandemic, we found that in some of the studied countries, desserts, sweets, sugary beverages, sugar, and salt were provided to students’ families, suggesting that established guidelines were not followed. These foods may have been distributed during the pandemic because they were already offered to students before the pandemic hit, despite the vast array of evidence that links foods high in added sugars with increasing risk of obesity in LAC. 34,35 Clear guidelines on what foods to provide during emergencies are critical because, in previous emergencies where these did not exist, emergency food assistance was saturated with calorie-rich nutrient-poor foods, which are known risk factors for diet-related chronic diseases. 36 Food corporations may have also leveraged the vulnerability of governments during the emergency to boost sales of ultra-processed products during the pandemic. 37 These foods tend to be shelf-stable and can be prepackaged for individual consumption during emergency responses without an assessment on how they meet the established nutritional guidelines. 36
The results from the current study underscore the importance of considering the nutritional quality of foods during emergencies, not only because the needs of beneficiaries and the circumstances in which they live may be different than from normal times (ie, heightened nutritional needs, family sharing of foods) but also because of the additional challenges related to logistics in acquisition, transportation, and distribution of foods that emergencies often pose, and that may be a risk to maintaining the quality of fresh produce and other products. The literature on nutritional quality of emergency foods in regions that have mostly overnutrition and diet-related chronic diseases, rather than from undernutrition, is sparse and has only recently come into attention of some countries (see, eg, 38,39 ). Our results join the call to urgently consider nutritional quality in feeding programs during emergencies with a focus on providing foods with high nutritional content that do not exacerbate the risk of overweight and obesity.
Strengths and Limitations
Limitations of this study are related to case selection, potential gaps between formal policy guidelines and actual implementation, and the limited scope of the rapid assessment. Our findings are not representative of the region and excluded countries that are also facing crises in food acquisition and security (primarily Venezuela where the food security and political crisis precede the COVID-19 pandemic). Implementation at the local level was not observed, and although many of the key informants surveyed were at the front lines of national SFP, this rapid assessment did not evaluate the impact of SFPs on any outcomes and did not examine actual implementation of modification strategies, quality of foods, or delivery to the most vulnerable populations. We are aware of the existence of other studies that propose such analysis on a national scale (see, eg, 40 ). This study is a first of its kind comparing modifications of SFP in LAC during the pandemic, expanding and contributing uniquely to the existing literature on this topic, which comes mostly from examples in Europe and the United States.
Conclusions
Although there is still much to be learned about the role of SFP in helping to protect children and adolescents' food and nutrition security during periods of economic and/or food supply shocks, the findings from this study highlight key measures that can help inform governments and the civil society future decisions to more readily face the challenges associated with similar emergency and/or economic and supply shock periods. Drawing from the lessons learned about challenges and facilitators of the modifications implemented during the COVID-19 pandemic in 11 SFPs in LAC, the findings underscore the following policy implications that deserve our immediate attention to mitigate schoolchildren’s food and nutrition insecurity during emergencies: (1) the allocation of immediate resources for an intersectoral working group dedicated to safeguarding nutritional benefits during emergencies, (2) strengthening efforts of community engagement before and during emergencies, and (3) establishment of clear guidelines of the types of foods that must be distributed to beneficiaries to meet their nutritional needs during emergencies.
Significance for Public Health
School feeding programs (SFPs) can play a crucial role in the emergency food and nutrition response, but there is a dearth of information on how SFPs operate during emergencies. This study elucidates lessons learned about modifications that SFPs in LAC made during the COVID-19 pandemic to continue to keep schoolchildren fed and to contribute to inform food and nutrition responses in future emergencies. Our results suggest that there is an urgency for clear implementation guidance on how to modify SFP during emergencies.
Our findings also underscore the need to: Allocate resources to an intersectoral working group dedicated to safeguarding nutritional benefits during emergencies. Strengthen efforts of community engagement before and during emergencies. Establish of clear guidelines of the types of foods that can be distributed to meet the nutritional needs of beneficiaries during emergencies.
Footnotes
Acknowledgments
The authors thank the directors of the different SFPs in Latin America and the Caribbean who provided information, as well as for Emma Creamer, from the George Washington University, who assisted with the initial document search. The authors also thank Dr. Carolina Batis Ruvalcaba for her insight, the Grupo de Estudios Políticas Alimentarias (GEPA), and Mercedes Leiva and her team for their insight into interpretation of results and connection in several countries. The authors also thank the “Childhood Obesity Prevention Across Borders” workshop series organized by the Center for Global Health Studies, Fogarty International Center, National Institutes of Health of the United States, and for the Programa De Liderazgo Latinoamericano En Nutrición (LiLaNut) organized by the Latin American Society of Nutrition, whose networks facilitated this cross-country collaboration.
Ethical Approval
All protocols were exempt from IRB review under DHHS regulatory Category 2 (IRB# NCR202820) at the George Washington University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JGW and FOG from Chile were supported by the Agencia Nacional Investigación y Desarrollo (ANID)/Fondecyt de Iniciación en Investigación 11180717 (Chile’s National Agency for Research and Development grant no. 11180717). Diana C. Parra was supported by the Centers for Disease Control and Prevention (number U48DP006395) and the Foundation for Barnes-Jewish Hospital. MFG was granted a Masters' scholarship from the Brazilian Coordination for the Improvement of Higher Education Personnel (CAPES). The findings and conclusions in this paper are those of the authors and do not necessarily represent the official positions of the Centers for Disease Control and Prevention.