
Abstract
Background:
Food insecurity and malnutrition present challenges to HIV management, but little research has been done in Latin America and the Caribbean (LAC).
Objective:
To assess levels of food insecurity and malnutrition among people living with HIV (PLHIV) across multiple countries in LAC to inform pilot projects and policy.
Methods:
Through interinstitutional collaboration, we collected data on sociodemographics, household food security, anthropometry, and commonly consumed foods among adults seeking care at HIV clinics in Bolivia, Honduras, and the Dominican Republic (DR; N = 400) and used the results for pilot projects.
Results:
Most PLHIV had moderate or severe household food insecurity (61% in Bolivia, 71% in Honduras, and 68% in DR). Overweight and obesity were also highly prevalent, particularly among women (41%-53% had body mass index ≥25). High body fat was also prevalent, ranging from 36% to 59%. Among salient foods, fruits and vegetables were lacking. Country-specific pilot projects incorporated locally tailored nutrition counseling with a monthly household food ration, linkage to income-generating projects, or urban gardens. Nutritional counseling was conducted initially by professionals and later modified for peer counselors given the lack of nutritionists.
Conclusion:
High levels of food insecurity and overweight among PLHIV in LAC have important implications, since prior interventions to address food insecurity among PLHIV have focused on underweight and wasting. Formative research and intersectoral collaboration facilitated locally appropriate nutritional materials and interventions, enhanced local capacities, and helped incorporate nutritional guidelines into policies and practice. Addressing human capital constraints in resource-poor settings and developing complementary strategies were key recommendations.
Highlights
Documenting high levels of food insecurity and overweight among people with HIV in Latin America and the Caribbean and highlighting food gaps have important implications for interventions, since prior efforts to address food insecurity among people with HIV have focused on underweight and wasting.
Introduction
Food insecurity and HIV pose severe and interrelated problems in Latin America and the Caribbean (LAC). Over the past decade, LAC has experienced a dramatic scale-up of antiretroviral therapy (ART), reaching the highest average coverage among regions of low- and middle-income countries. 1 However, food insecurity has emerged as a barrier to ART utilization and adherence among people living with HIV (PLHIV), especially in low-resource settings. 2 -5 Food security has been defined as “the limited or uncertain availability of nutritionally adequate, safe foods or the inability to acquire personally acceptable foods in socially acceptable ways.” 6,7 Most national AIDS strategic plans in LAC emphasize integrated support services (including nutrition) that promote access and adherence to treatment in low-resource settings, but there has been little research in LAC to guide culturally relevant nutritional advice and food insecurity interventions for PLHIV, and availability of such support services is often lacking. 8
Food insecurity has been found to be highly prevalent among PLHIV in low-resource settings, but research in LAC has been limited. 2,9 -11 In LAC, widespread inequalities and poverty shape the HIV epidemic, as one of the regions with the highest levels of income inequality. 12,13 However, to date, most of the evidence regarding the relationship among poverty, food insecurity, and HIV has been conducted in sub-Saharan African countries and among vulnerable populations in the United States. 14 -17 Additional work is needed to explicate factors affecting PLHIV’s ability to access and utilize food resources across the LAC region.
Food insecurity has been found to be associated with poor ART adherence in resource-poor regions such as sub-Saharan Africa 3 -5 and South America, 2 as well as among vulnerable populations in resource-rich settings such as the United States 18 -20 and France. 21 Across economic contexts, food insecurity among PLHIV has also been associated with worse virologic and immunologic outcomes, 22,23 higher morbidity 10 and mortality, 24,25 and increased likelihood of depression. 26,27 Promoting food security and effective nutritional support is crucial to ensuring optimal ART uptake, adherence, and outcomes. Nevertheless, there is little research on effective strategies for promoting food security and nutritional support among PLHIV in LAC. 28 -33
Motivated by the need to address this gap, the UN World Food Programme Regional Bureau for Latin America and the Caribbean (WFP-LAC) formed a partnership with the RAND Corporation, a nonprofit research organization, to develop and evaluate pilot projects that address the food insecurity and nutritional needs of PLHIV in LAC. A first step was to conduct formative research across various LAC countries to help inform these pilot projects. Our overall approach was driven by the idea that context-specific formative work can help better align interventions with the needs and preferences of potential “users.” This is true especially when trying to address food insecurity, since, as noted in the above definition, acceptability plays an important role.
The purpose of this article is to assess levels of food insecurity and malnutrition among PLHIV across multiple countries in LAC (Bolivia, Honduras, and the Dominican Republic [DR]) to inform the development of pilot interventional projects and policy. We discuss how these informed the pilot projects that resulted, as well as policy and practice around addressing food insecurity and nutritional needs of PLHIV. Lessons learned from our cross-country experiences can guide others wanting to use interinstitutional approaches and applied research to inform the development of policies and programs to address food insecurity and nutritional needs of vulnerable populations.
Methods
Overall Approach
The WFP-LAC Regional Bureau and the RAND team selected countries to represent a range of Latin American regions (Central America, South America, and the Caribbean) and overall high levels of poverty. Although HIV prevalence was not the main driving factor, it played a role when deciding to include the DR and Honduras, which, at the time we began our partnership in 2008 to 2009, had among the highest overall HIV prevalence in Spanish-speaking Latin America. 34 Perhaps the most important feature across all 3 countries was that their WFP country offices had expressed interest in partnering to conduct the formative research and were committed to working with local stakeholders to develop strategies to address food insecurity and nutritional needs of PLHIV.
In all 3 settings, we followed the following pattern: (1) identified local partners, including government and nongovernment organizations, with whom we conducted formative research consisting of qualitative and quantitative methods and assessed dietary patterns, nutritional status, and levels of food insecurity among PLHIV, as well as obtained important contextual information for developing pilot programs; (2) reviewed findings with local stakeholders and developed context-specific nutritional counseling and other strategies for addressing food insecurity and nutritional deficiencies in this population; and (3) implemented and evaluated pilot programs to address food insecurity and nutritional needs of PLHIV, with the aim of improving ART adherence and overall health. The resulting multicomponent food security and nutrition strategies were designed taking into consideration World Health Organization (WHO) treatment recommendations and local priorities and capacity. These recommendations are aimed at improving nutrition and food security for PLHIV through improved dietary habits and quality, with due consideration to local food availability, cultural acceptability, and family budgetary constraints. 35
Partnership Structure
The overarching structure of partnership to carry out the formative research included a lead from each partner agency (RAND, WFP-LAC) and leads from each WFP country office, supported by proper contacts within relevant HIV programs in the respective countries’ Ministries of Health. The leads were responsible for coordinating with other colleagues in their agencies on partnership research activities. Within each country, we worked closely with WFP country personnel and HIV clinic staff to execute all study activities. We also met with other key stakeholders such as national AIDS program personnel and national associations of PLHIV at key points, for example, before starting the study and during the formative research phase, to review preliminary findings and discuss implications. Additionally, in one country, we hired members of the National Association of PLHIV as data collectors. Bilingual researchers from RAND trained data collectors to administer all study protocols under the direct supervision of the in-country lead (WFP staff or consultant). Researchers also provided ongoing support and supervision to country leads to ensure consistent implementation of data collection instruments.
Study Sites and Sampling
The WFP country offices selected study sites within each country to represent a range of geographic regions, populations, and types of HIV clinical settings (eg, government hospital, government clinic, and nongovernmental organization). Table 1 provides an overview of HIV and socioeconomic indicators for each study country. Fieldwork was staggered across the selected countries, covering Bolivia (2008-2009), Honduras (2009-2010), and the DR (2011-2012). Clinic sites were in primarily urban/peri-urban areas: La Paz and Santa Cruz (Bolivia); Tegucigalpa, San Pedro Sula, Progreso, and Tela (Honduras); Santo Domingo, Higuey, Puerto Plata, and San Juan (DR). Local data collectors screened patients who sought care at study clinics on the designated recruitment days for eligibility and, if eligible, invited them to participate. Eligibility criteria included ≥18 years of age, resident in the area for at least 1 year prior, Spanish speaker, and registered in clinic (with confirmed diagnosis of HIV). Pregnant women were excluded because of the influence of pregnancy on nutritional outcomes. We aimed to sample 35 to 40 participants per site within each country, guided by the number required to reach saturation on the free listings (see below).
Selected Demographic and Health Indicators for Study Countries (2012-2015).a
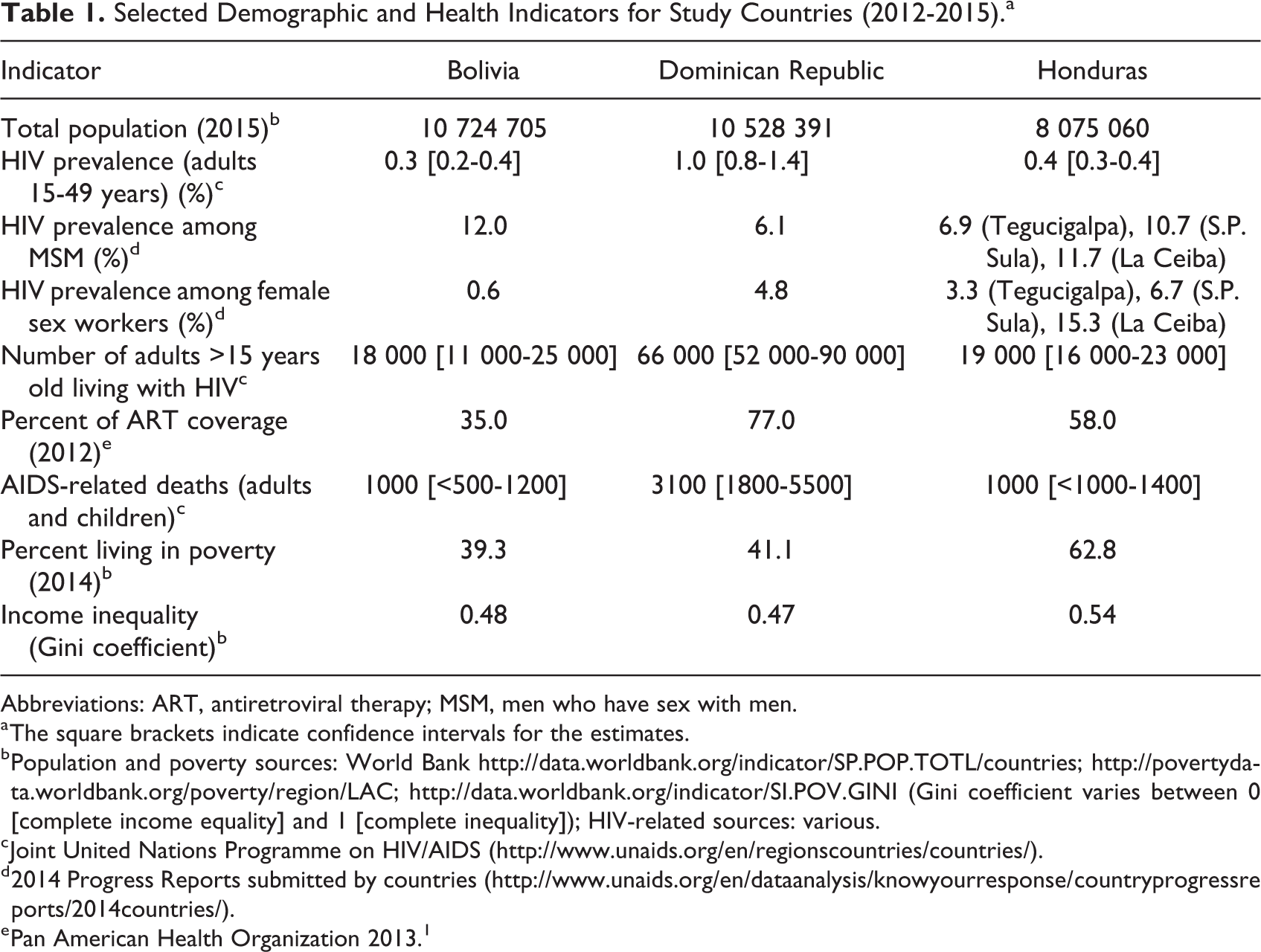
Abbreviations: ART, antiretroviral therapy; MSM, men who have sex with men.
a The square brackets indicate confidence intervals for the estimates.
b Population and poverty sources: World Bank http://data.worldbank.org/indicator/SP.POP.TOTL/countries; http://povertydata.worldbank.org/poverty/region/LAC; http://data.worldbank.org/indicator/SI.POV.GINI (Gini coefficient varies between 0 [complete income equality] and 1 [complete inequality]); HIV-related sources: various.
c Joint United Nations Programme on HIV/AIDS (http://www.unaids.org/en/regionscountries/countries/).
d 2014 Progress Reports submitted by countries (http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2014countries/).
e Pan American Health Organization 2013. 1
Data Collection Methods
Demographic and Household Characteristics
These data were obtained through structured individual interviews. We adapted specific measures from prior health and family surveys within Latin America (Demographic and Health Surveys) and included age, sex, ethnicity, residential area, education, marital status, household composition, housing type, income, and employment.
Anthropometry (height, weight, body mass index [BMI], and body fat): Local data collectors recorded participants’ weight and height per technical standards of the Instituto de Nutrición de Centroamérica y Panamá (Institute of Nutrition of Central America and Panama). Using these measures, we calculated BMI as kg/m2 and categorized each participant as underweight (<18.5), normal weight (18.5-24.9), overweight (25.0-29.9), and obese (≥30) using WHO classifications. 36 Local data collectors also measured body fat composition using bioelectrical impedance analysis with a portable body fat analyzer (Model HBF 306; OMRON Healthcare, Vernon Hills, Illinois).
Food Security
Data collectors assessed household food security using the Escala Latinoamericana y Caribeña de Seguridad Alimentaria or Latin American and Caribbean Food Security Scale. This 15-item scale was developed to assess household-level food security in Latin America (based on experiences in Brazil, Colombia, and the United States) and has been validated in several regional studies. 37,38 Using the total score (0-15), we classified participants into 4 categories of household food insecurity as recommended by scale developers 38 : no food insecurity (0), mild food insecurity (1-5), moderate food insecurity (6-10), and severe food insecurity (11-15).
Free Listing of Frequently Consumed Foods
Free lists are often used by ethnographers to explore a semantic domain, especially at the initial stages of research. 39 As we were interested in learning about foods commonly consumed by PLHIV, data collectors asked participants to list “all the foods they usually consume.” Their individual answers were recorded taking care to list food items in the order they were mentioned. 40
Data Analysis
We analyzed the data for each country using descriptive techniques (eg, frequencies, means, or medians). Given the importance of sex for anthropometric outcomes, 41 we present results by sex within each country. For the free listing data, it is important to consider both frequency of mention of the different items and the order in which they were listed. Items that appear closer to the top of the list, as well as that are listed more frequently, better define the domain shared by the group (ie, cultural domain). 42 For this analysis, we used Smith S index, a salience measure that considers both rank order and frequency. 43 The higher the Smith S index, the earlier and more frequently the item was mentioned—on average—in free lists generated by informants. 43 Therefore, we interpreted foods listed first to reflect those items most important among those mentioned, and repetition of food items across different informants provided information about foods most commonly mentioned by the population of interest.
Application of Findings to Develop Pilot Projects
After collecting data in each country, we reviewed preliminary findings first with WFP and RAND staff and local data collectors and then with a larger group of stakeholders (eg, representatives of the national AIDS programs in each country, ministries of health, networks of PLHIV, etc). In these meetings, we discussed overall findings and how these could inform pilot programs to address food insecurity and nutritional needs of PLHIV in each country. Subsequent stakeholder meetings were held to design, implement, and evaluate the pilot programs.
Results
A total of 400 participants were included. Table 2 provides sociodemographic characteristics of participants across the 3 countries. Over two-thirds of participants in the DR and Honduras were women, whereas less than half were women in Bolivia. Mean age was slightly lower in Bolivia and Honduras (36.4 and 38.8 years, respectively) compared to the DR (40.0 years). Participants in the DR had the lowest levels of education: 72% with primary school or less in the DR, compared to 59% for Honduras and 23% for Bolivia. Participants in the DR also had higher levels of food insecurity, with 57% of the DR sample having severe food insecurity, compared to 34% in Bolivia and 45% in Honduras. A smaller proportion of the DR and Honduras samples reported receiving any income from formal or informal sector work activities (60% and 62%, respectively) than the Bolivia sample (77%).
Participant Sociodemographic Characteristics and Food Insecurity.a
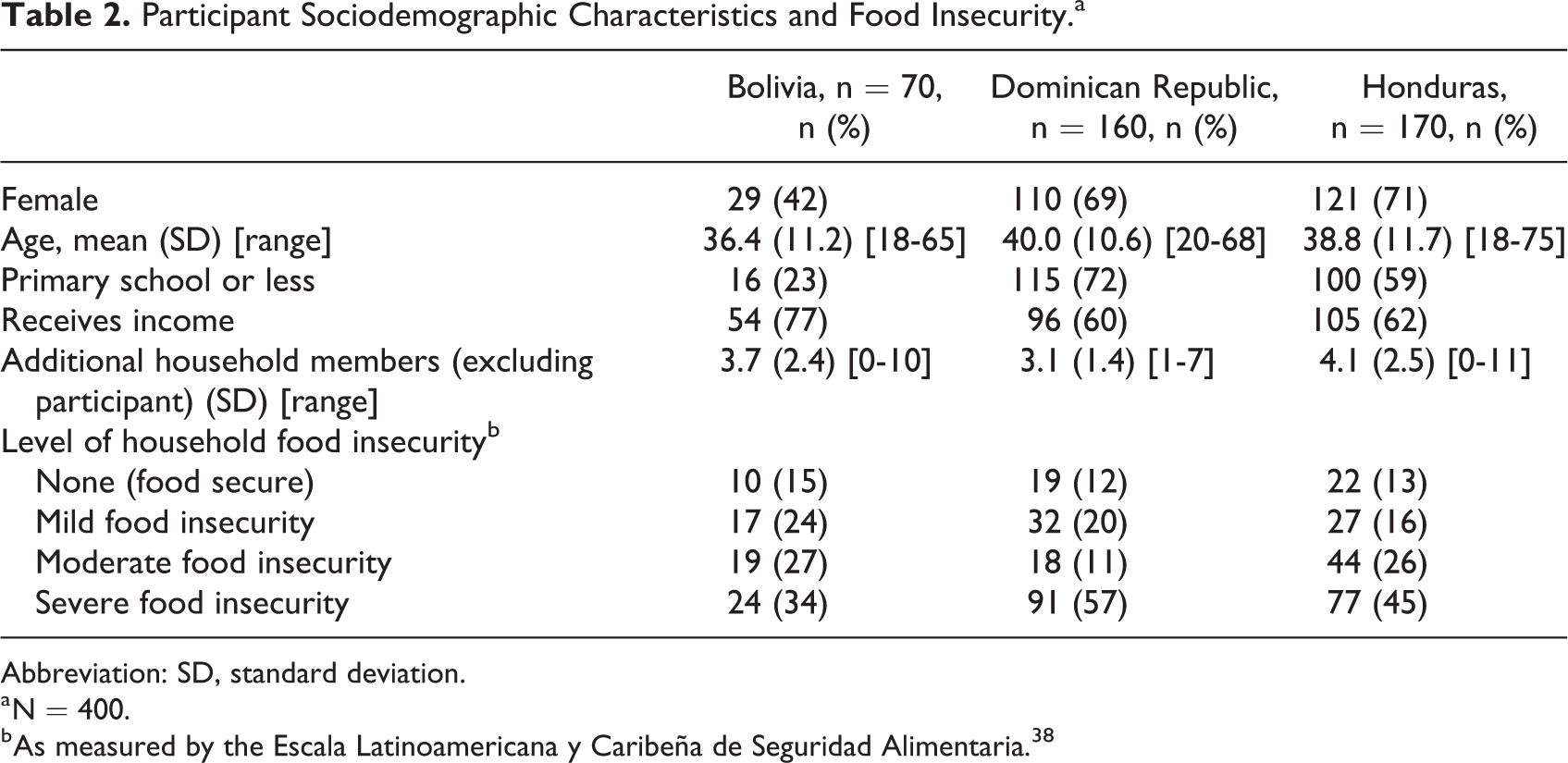
Abbreviation: SD, standard deviation.
a N = 400.
b As measured by the Escala Latinoamericana y Caribeña de Seguridad Alimentaria. 38
Table 3 provides nutritional status (BMI and body fat) by country and sex. “Normal” was the predominant category of BMI for men (75% in Bolivia, 54% in DR, and 86% in Honduras), but substantial proportions of women in each country were either overweight or obese (53% in Bolivia, 41% in DR, and 42% in Honduras). However, it is also important to note the presence of underweight, most notably in the DR (19% of women and 14% of men). With respect to body composition, more than one-third of men and women across all 3 countries had high and very high body fat (ranging from 36% among men in Honduras to 59% among men in DR). The presence of low body fat was more apparent in Honduras (14% of women and 35% of men) and the DR (31% of women and 17% of men).
Participant Nutritional Status by Study Country and Sex.
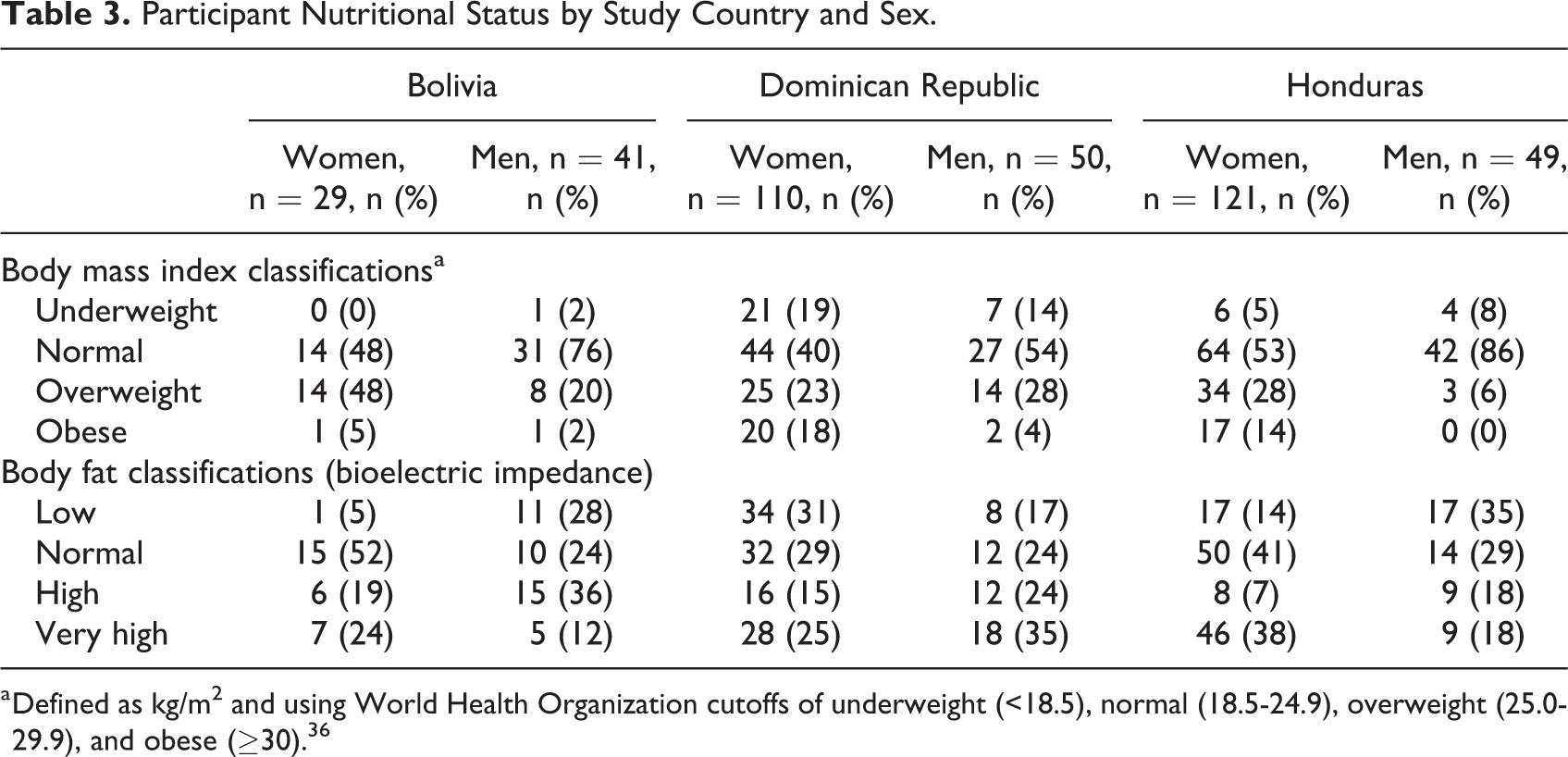
a Defined as kg/m2 and using World Health Organization cutoffs of underweight (<18.5), normal (18.5-24.9), overweight (25.0-29.9), and obese (≥30). 36
Table 4 provides the Smith S index for the salience of foods in the free listing. Across all 3 countries, rice had the highest salience. Further, foods listed in the top 10 tended to be sources of carbohydrates or protein, including animal sources (eg, chicken, egg) as well as vegetable sources (eg, beans). No green leafy vegetables and no fruits except tomatoes made it into the top 10 listed foods for any of the countries.
Foods Most Commonly Mentioned in Free Listings as Being Usually Consumed, by Country, Ordered According to Smith Salience Index.a
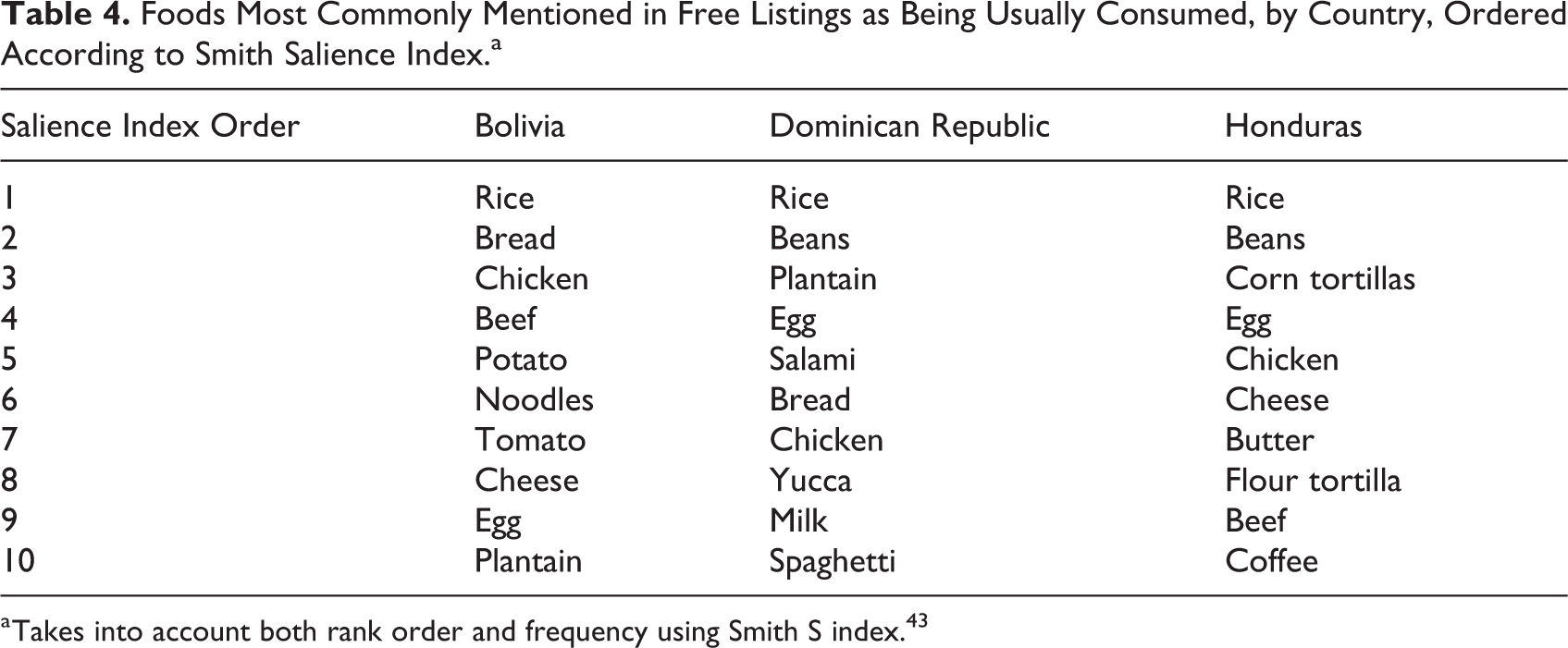
a Takes into account both rank order and frequency using Smith S index. 43
Design, Implementation, and Evaluation of Pilot Programs
We discussed the findings from the formative phase with local WFP country offices, governmental agencies, associations of PLHIV, and HIV clinics, to identify the most relevant issues that would help design pilot projects tailored to each context. Across all 3 countries, there was a general lack of knowledge regarding the nutritional needs of PLHIV—including among the limited number of professional nutritionists and the physicians providing the bulk of care to PLHIV—and few nutrition training programs. Therefore, nutritional counseling was identified as a priority focus across all sites to address the wide range of nutritional statuses identified—from underweight to overweight and obesity. The formative research helped to guide the nutritional counseling and resultant curricula that were developed to facilitate it. In addition, there was special care to address the high levels of food insecurity in tangible ways, but the nature of the proposed strategies varied across contexts.
In Bolivia, WFP implemented nutritional counseling via professional nutritionists and a monthly household food ration and partnered with RAND to explore the feasibility of transitioning recipients off food support and into income-generating projects. 44 The formative research also influenced the National AIDS Program to include nutrition as a focus in its national plan. Nutritionists trained through these efforts were hired by the Ministry of Health to support nutritional care at government HIV clinics. Municipalities that had participated in the formative research included a line item in their budgets for nutritionists at their HIV clinics.
In Honduras, RAND and WFP partnered to implement culturally tailored nutritional counseling (via professional nutritionists) and a monthly household food ration in a pilot cluster randomized controlled trial (RCT) with funding from the US National Institutes of Health (NIH). The objective was to compare the effect of nutritional counseling plus food assistance on ART versus nutritional counseling alone in a cluster RCT of 4 clinics. After finding that both interventions (nutritional counseling plus food assistance and nutritional counseling alone) decreased food insecurity 33 and improved ART adherence, 32 we conducted a supplemental study whereby the nutritional counseling component was successfully transferred to peer nutritional counselors to scale up the intervention. This strategy allowed us to scale up from an initial 4 clinics up to 14 clinics, covering 80% of patients attending government-supported HIV clinics in the country. 30 The nutritionists trained through our NIH-funded study were later hired by the Ministry of Health after the conclusion of study activities to support nutritional care at government HIV clinics. Further, many of the peer nutritional counselors that we trained through the extension project in Honduras were also hired by the HIV clinics after the study. Thus, the project contributed to development of human capital to support Honduras’ efforts to address the food and nutrition security of PLHIV. Further, these activities were supported by the training manuals and intervention materials developed during the study, which were officially transferred from the research team to the Ministry of Health for use in HIV care.
In the DR, a slightly different approach was taken due to factors related to WFP food assistance policy as well as learning from the earlier pilots in Bolivia and Honduras. Since around 2008, when the DR became a middle-income country, WFP has not provided food assistance except in emergencies. Thus, coupling nutritional counseling with food assistance was not an option. Together with local collaborators and stakeholders, we brainstormed on possible strategies and identified urban gardens as a potential way to support improved food security in a sustainable fashion. We then conducted additional formative research through in-depth interviews 45 and focus groups to inform this strategy and developed a partnership with the Dominican Ministry of Agriculture to conduct pilot urban garden projects in 3 communities. Currently, we are conducting an NIH-funded trial to assess the feasibility, acceptability, and preliminary effectiveness of an integrated peer nutritional counseling and urban garden intervention on HIV adherence and viral suppression (evaluation ongoing). In addition, at the policy level, our formative research finding of high levels of food insecurity, coupled with advocacy by key partners like the Dominican National AIDS Council (known by its Spanish acronym, CONAVIHSIDA), influenced policymakers to expand eligibility among PLHIV for existing social protection programs. The WFP DR country office has also made nutritional counseling and urban gardens a focus of their HIV programs in the country, in collaboration with CONAVIHSIDA.
Discussion
Our formative research across various countries and regions in LAC identified high levels of food insecurity coinciding with overweight and obesity, particularly among women. Most PLHIV in our study had moderate and severe household food insecurity (ranging from 61% to 71%). Comparatively, studies among PLHIV in the United States and Canada have identified rates of food insecurity ranging from 48% to 65%, 19,23,46 -48 while 89% were identified as having severe food insecurity in Haiti. 49 At the same time, across the 3 countries in our study, between 41% and 53% of women were overweight or obese per BMI and 40% and 45% had high or very high body fat. These findings motivated context-specific combination intervention approaches led by WFP and in-country stakeholders intended to address the dual concerns of food insecurity and diverse manifestations of poor nutrition in each of the 3 countries. This is one of the first studies reporting on formative research driven by local needs and context, using rigorous scientific methods, to inform the integration of HIV and nutrition for LAC.
Studies in Brazil have documented high levels of central obesity (58%) and high BMI (36% BMI ≥25) among women living with HIV 50 but have not documented levels of food insecurity. Studies of PLHIV on ART in Africa are also beginning to see similarly increasing levels of overweight and obesity 51,52 ; however to date, most studies about food insecurity among PLHIV focus on the association between food insecurity and underweight. 53 Similarly, the study in Haiti that reported 89% moderate or severe food insecurity among PLHIV found that only 20% had BMI ≥25 kg/m2 and food insecurity was negatively related to BMI. 49 In contrast, our pilot research in Bolivia, Honduras, and the DR found high levels of both food insecurity and obesity. Further, additional analyses of the DR data found a positive relationship between severe household food insecurity and BMI of PLHIV, even after controlling for age, sex, income, having children at home, education, and ART status. 54
We should also highlight that although overweight and obesity were more common in our samples than other forms of malnutrition, we also found some degree of underweight, most prominently in the DR, which was also the country with the highest overall level of severe food insecurity. Taken together, these findings confirm the “dual burden” of obesity and undernutrition among PLHIV in low- and middle-income countries and its co-occurrence with food insecurity. 55 It is, therefore, imperative going forward to develop interventions in resource-limited settings that address both overweight/obesity and undernutrition and food insecurity.
In terms of other commonalities among our sites, analysis of free listings of foods commonly consumed highlighted several interesting points. Among the most salient foods, there was a shared pattern represented by rice, egg, and chicken. Beef, beans, plantain, bread, and cheese were commonly mentioned in 2 of the 3 countries. Each country had some foods that represented low cost and ease of access: noodles in Bolivia, yucca and spaghetti in DR, and tortillas (corn or flour) in Honduras. On the other hand, among the top 10 most frequently mentioned foods, there was only 1 fruit (tomato) and no green leafy vegetables mentioned. While this procedure does not provide precise dietary information, it does reflect features shared by this domain of “foods most commonly consumed” and raises points of interest to address with more specific methods of dietary evaluation. Fruits and vegetables are important sources of vitamins and minerals, and it has been well-documented that micronutrient deficiencies increase risk of poor ART outcomes. 56 Also, food insecurity among PLHIV has been found to be associated with low dietary diversity, which is correlated with poor nutrition. 49 Therefore, although our free listing data do not allow us to determine the actual level and types of macro- or micronutrient deficiencies that may be present among the populations that participated in our study, they suggest the need for future research to assess quality of diet and, if found to be deficient, develop appropriate interventions to address it.
A critical aspect of our formative research and pilot projects was the involvement, at various stages, of specific community-based stakeholders, especially national and regional networks of PLHIV. For example, individuals from networks of PLHIV were involved in data collection (Bolivia and the DR). This aspect is important because we were particularly interested in involving these groups in implementing the pilot projects that we proposed. Following this strategy, we relied on networks of PLHIV to help distribute food baskets to participants (Bolivia and Honduras) and serve as peer counselors (Honduras and the DR). Although stakeholder involvement in HIV-related efforts is not unusual and often promoted through national AIDS councils, the focus on food insecurity and nutritional needs brought together additional cross-sectoral partnerships with local health officials and other governmental agencies such as the Ministry of Agriculture in the DR. The active involvement of PLHIV in designing and implementing the resultant strategies (eg, peer nutritional counseling, urban gardens) was essential for the success and sustainability of these initiatives and, in some cases, contrasted with the more passive roles that sometimes characterize recipients of government social assistance programs.
Finally, our interinstitutional approach—led by a specialized UN agency in WFP and involving international researchers, local research collaborators, civil society, health-care providers, and government agencies—led to a robust response and culturally tailored programs. Further, the work influenced national policies and programs because of the key actors involved. Nevertheless, this broad partnership also required that different actors adjust their own expectations at times. For example, after completing the qualitative research in the DR on the acceptability of urban gardens as a strategy to address food insecurity, WFP, the Ministry of Agriculture, and other local partners were ready to begin a demonstration project in the communities where we had done the qualitative research. However, it would take time to get research funding to test the effectiveness of urban gardens in addressing food insecurity and improving ART adherence and decreasing viral load (an important goal of adherence). Thus, the team agreed to initiate a demonstration project to be responsive to community needs, and that once research funding was obtained, the research project would need to be conducted elsewhere in the country. This tension between action and research is likely to exist between organizations whose missions are oriented toward operations and relieving human suffering versus producing evidence to inform policy.
Several limitations should be noted regarding our findings. First, our opportunistic sampling from HIV clinics meant that it did not capture PLHIV who have abandoned treatment or are not engaged in care; these individuals may have even higher levels of food insecurity. Second, our sample generalizability both within countries and across the region was further restricted given its nonrandom approach. Third, we do not have HIV-related outcome data, which is a weakness in terms of being able to understand clinical relevance of the high levels of food insecurity and overweight and obesity. Fourth, we did not collect data on depression, which is often correlated with food insecurity. Fifth, when examining body fat, we did not control for ART status, time on ART, or treatment regimen, and these have been associated with fat deposition, including loss/accumulation and redistribution. 57 Further, there is some evidence that body composition changes due to HIV status and treatment differ between men and women. 58 Finally, the time frames for data collection varied across several years, diminishing our ability to directly compare findings across the 3 countries. Nevertheless, our standardized training and data collection procedures enhance comparability and, given the lack of research on food insecurity and nutritional status among PLHIV in the region, our findings provide important trends to explore in population-based studies.
Implications of Our Findings for Programs and Policy
High levels of both food insecurity and overweight and obesity among PLHIV have important implications for food security and nutrition interventions in resource-poor settings. To date, such interventions tend to focus on food supplementation and safety nets (food, cash, or vouchers) for food insecure, underweight individuals, with the goal of promoting weight gain. 59,60 Food supplementation and assistance has been the most studied, generally demonstrating positive effects on nutrition status, quality of life, 61 and household food security among PLHIV, 59,62 as well as retention in care and adherence to treatment outcomes. 9,10 Two caveats should be noted related to this intervention: food supplementation is often not sustainable, and of the few previous interventions tested among PLHIV in low-resource settings, most have focused primarily on undernutrition. 63 However, there is a growing burden of overweight and obesity among PLHIV, which can lead to increased risk of other chronic conditions including diabetes and cardiovascular disease. 64 In our evaluation of the intervention developed in Honduras, food support was more effective in reducing food insecurity than nutritional counseling alone; however, it had the undesired effect of increasing weight significantly among already overweight and obese patients, whereas counseling alone led to weight loss among overweight and obese participants. 27 This may not be all that surprising given that the food basket, as typical of such support, contained items high in calories (maize, rice, beans, corn-soy blend, and vegetable oil). Additional work is needed to identify effective and sustainable strategies for addressing food insecurity among PLHIV of diverse nutritional statuses, including promoting the consumption of fruits and vegetables. Dietary diversity and food choice are an important component of food security.
Nutrition education and counseling for PLHIV, which takes into consideration the local availability and cultural acceptability of foods as well as issues relevant for management of HIV disease, may be more effective and sustainable than long-term food support. Nevertheless, reviews of nutritional interventions for PLHIV have noted that nutrition education and counseling have been weak components. 59,65 In fact, in a review of nutrition assessment, counseling, and support interventions among PLHIV in resource-limited settings, 65 of the 21 studies included, only 2 included a nutritional counseling component. Development and rigorous assessment of culturally tailored nutritional counseling interventions among PLHIV in resource-limited settings are therefore needed to address both food insecurity and the diverse nutritional statuses found in this population. Additionally, addressing the human capital constraints regarding nutrition care in many such settings is important, as we found in our pilot studies, which prompted us to develop some creative interventions (i.e., training of peer nutritional counselors).
In addition to nutritional counseling, complementary strategies are needed to fully address food insecurity and poor nutrition among PLHIV. A recent pilot cluster RCT in Kenya found that an agricultural intervention for PLHIV (including water pump, microfinance loan, and education in sustainable farming) significantly increased CD4 cell counts and odds of viral load suppression at 12 months, 66 but the focus was on undernourished individuals and there were no statistically significant effects of the intervention on BMI. Our integrated urban gardens and nutritional counseling intervention being implemented in the DR among food insecure PLHIV of diverse nutritional statuses aim to fill this research gap of other sustainable interventions to address food insecurity among PLHIV with varied nutritional statuses. The research conducted through the WFP-RAND partnership across various LAC countries was key in helping to (1) identify the high levels of food insecurity and diverse nutritional statuses, (2) develop culturally tailored nutritional counseling and provide curricula for use by ministries of health, (3) identify the need to better tailor food aid in the region to a diverse range of nutritional statuses, and (4) establish the acceptability and feasibility of peer nutritional counselors and urban gardens as alternative and sustainable strategies to address both food insecurity and nutritional issues among PLHIV and complementary strategies to robust nutritional counseling as part of integrated care.
Conclusion
The effects of food insecurity and nutrition on HIV outcomes are of increasing concern across a variety of settings. Effective, locally tailored, and sustainable approaches to improving food insecurity and nutritional status among PLHIV are critical to improving their health outcomes. Through our interinstitutional partnerships and implementation of formative research on food insecurity and nutritional needs of PLHIV in Bolivia, Honduras, and the DR, we found consistently high levels of food insecurity among PLHIV and, in contrast to previous work on food insecurity among PLHIV in resource-poor settings, a range of nutritional statuses. In fact, the most common forms of malnutrition in this population were overweight and obesity, not underweight. We learned that, especially going forward, food insecurity interventions need to develop strategies that account for this range of nutritional statuses, such as tailored nutritional counseling, while at the same time facilitating a supply of nutritious foods. We also highlighted the need for properly trained paraclinical staff to support nutrition interventions and provided evidence on how to address limitations in human resources. Our experience of moving from nutritional counseling plus traditional types of food support to nutritional counseling plus urban gardens reflected not only the realization that diverse nutritional statuses were at play but also the critical need for sustainability. We emphasize that formative research and intersectoral collaboration evolved dynamically, supported the design of locally appropriate nutritional interventions for PLHIV, enhanced local nutritional and research capacities, and helped incorporate nutritional guidelines into national policies and clinical practice. Further, our partnership progression—and the methods and programs that resulted—demonstrate how such applied research and collaboration among a UN agency, a nonprofit research organization, and local partners can lead to useful tools for assessment and planning around food and nutritional needs of PLHIV and, potentially, other vulnerable populations.
Footnotes
Authors’ Note
K.P.D., J.A., and H.M. conceived the study. H.M., K.P.D., and K.P. designed the study materials, supervised data collection, and analyzed the data, while H.F. and J.A. provided critical input throughout all phases of the research. K.P.D. wrote the first draft of the manuscript, K.P. and H.M. contributed to significant revisions, and J.A. and H.F. provided subsequent critical revisions. All authors have read and approved the final manuscript.
Acknowledgments
The authors are deeply grateful to the participants in the formative research in Bolivia, Honduras, and the DR, who gave so generously of their time and personal information. The authors also thank various colleagues from WFP country offices, especially Blanca Joice Ramírez (Honduras), Ximena Rojas (Bolivia), and Altagracia Fulcar (DR), who were key to carrying out this work. In addition, Dr Salvador Quiñones managed data collection in the DR. We also acknowledge the support of RAND colleagues, especially Alexandria Smith for data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection was supported by a grant from the OPEC Fund for International Development (OFID) to the UN World Food Programme Regional Office for Latin America and the Caribbean. The formative research in Honduras was supported by grant number R34MH084675 (Martínez) from the National Institute of Mental Health (NIMH). Additional support for drafting and revising this manuscript came from grant number R34MH110325 (Derose) from NIMH and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK; grant number K01DK107335 [Palar]. The contents of this article are solely the responsibility of the authors and do not represent the official views of OFID, WFP, NIMH, or NIDDK.