
Abstract
Background:
In 2014, Ecuador became the first country in Latin America to adopt the nutritional traffic light labeling system as a public policy aimed at guiding informed food choices.
Objective:
To describe the differences in comprehension and use of the new nutrition label in 2 different ethnic populations residing in a limited resource area of central Ecuador.
Methods:
A total of 394 women (18-75 years, 54.8% indigenous and 45.2% mixed-race mestizas) were randomly selected in the Chimborazo Province and were requested by a questionnaire to provide information regarding their awareness and comprehension of the traffic light nutritional labeling system and personal use of the food label in food selection.
Results:
Indigenous women had a high percentage who lacked any formal education (43.5%) and a greater proportion were not aware of the labeling system when compared with the mestizas (84.3% vs 46%; P = .001). In both groups, the main reason for not reading labels was lack of understanding of its meaning (50% indigenous vs 32.7% mestiza; P < .05). The reported use of the labeling system for food choices was low—on average, 32% of the mestizas and 5% of the indigenous women reported using nutrition label information to guide their purchase and consumption of packaged food items.
Conclusion:
The use of nutritional labeling is low in both mestiza and indigenous Ecuadorians, although higher among the mestizas. Among the indigenous women, mostly likely owing to less education, limited nutrition-related health knowledge, and higher risk for food insecurity, the utility of the new traffic light food label is limited.
Introduction
Mandatory nutritional labeling for commercially prepared foods is a public policy approach implemented with the objective of providing nutrition information to consumers for their informed decision-making based on the nutritional quality of prepackaged food products. Such labeling aims to promote healthy dietary habits in an effort to reduce exposure of the population to risk factors related to the development of chronic, noncommunicable diseases. However, awareness and use of nutrition labels vary considerably among different population groups. The use of nutrition labels has been shown to be affected by geographical residence (urban and vs rural populations), age, socioeconomic status, education, and ethnicity. 1 –5 The latter may be associated with the understanding and use of nutrition labels 1,2,4,6 in some populations primarily due to its covariation with other determinants including socioeconomic status, language, and education.
The policies regulating nutrition labeling vary substantially between countries. 1 An increasingly popular approach is the use of the nutrition traffic light, in which specific nutritional constituents such as salt, sugar, and fat are labeled with traffic lights shining green, orange, or red in order to provide information about the appropriateness of such foods as part of a healthy eating pattern. 7 This format involves less information processing than is required of the nutrition table format and the guideline daily amounts format and thus may be effective in promoting accessibility to nutrition information across groups differing in education and levels of socioeconomic status. 1,2,7 –13
In August 2014, Ecuador became the first country in Latin America to adopt the nutritional traffic light system to go along with the Nutrition Facts portion of food labels as a mandatory public policy aimed at guiding the public toward informed decision-making in regard to their food consumption and health. 14 Total levels of salt, sugar, and fat are categorized as high, medium, and low, which are then associated with the colors red, yellow, and green, respectively, in order to provide consumers with information regarding the content of these food components in processed foods that when consumed in excess are related to compromised health and increased chronic disease risk.
Ecuador is a racially and ethnically diverse country—7% of the total population describes itself as indigenous, 72% as mixed race (mestizo), and the remaining 21% as Afro-Ecuadorian, white, or Montubios (a racial group unique to Ecuador). The recently published data from the Ecuador National Survey of Health and Nutrition 15,16 reveal significant differences in the prevalence of noncommunicable chronic diseases according to ethnicity. For example, in the year 2012, the prevalence of diabetes in the indigenous population aged 10 to 59 years was estimated at 0.9%, whereas the prevalence in the mestizo population was 2.9%. 15 The prevalence of hypertension in the indigenous population aged 10 to 59 years was 5.3%, whereas the prevalence was 9.0% in the mestizo population. 15 It is likely that differences in dietary patterns contribute to the ethnic differences in disease prevalence. Indigenous Ecuadorians primarily reside in rural areas with historically less access to commercially prepared foods, whereas mestizas more commonly live in urban areas where packaged foods are readily available. In the central highlands of Ecuador, carbohydrate consumption is typically high in both urban and rural areas owing to ingestion of white bread and potatoes, with white rice and simple sugars consumed in higher quantities in urban areas. 15 In addition to potatoes, commonly consumed foods among the indigenous population of the Andean region include beans, quinoa, vetch, barley, and vegetables such as chard, cabbage, and turnips. Dietary fat intake is typically low in this region. 17
Ecuador is now in the midst of a nutrition transition and rural indigenous populations are facing increased exposure to processed foods at early ages. For example, among indigenous children and adolescents aged 10 to 19 years, 69% reported consumption of soft drinks, energy drinks, and processed juices—not much lower than the 81% of mestizo reporting consumption of these sugary beverages. The prevalence of sweet or salty snack consumptions was 55% among indigenous adults compared to 65% among mestizo adults, whereas the prevalence of fast food consumption was 41.7% among the indigenous population and 52.5% among mestizos. 15
Given the newly enacted nutrition labeling in Ecuador and the current transition among both mestizo and indigenous populations in the country to the use of more commercially prepared, prepackaged food items, we sought to determine the extent of differences, if any, in awareness, comprehension, and use of nutritional labeling among these 2 groups living in the central Andes highlands of Ecuador. The information generated by this study contributes to understanding the applicability of this public policy as a strategy to guide informed decision-making on nutrition and health.
Methods
Design of the Study and Description of the Geographic Area
A descriptive cross-sectional study design was implemented during 2015 in the province of Chimborazo, situated in the center of the Andean region of Ecuador. The study was part of a larger project designed to examine blood pressure and anthropometric characteristics among urban- and rural-dwelling women in Ecuador (Melby et al, 2016) 18 . The Chimborazo Province (population 458 581) was selected as the geographic region of the study based on its ethnic composition (38% indigenous, 58% mestiza) and urban/rural population distribution (59% rural, 41% urban). Socioeconomically, Chimborazo is characterized as the province of the Andean region of Ecuador with the second highest rates of poverty in the form of unsatisfied basic needs (46%), with one of the highest rates of migration from the rural sierra to the urban areas, 19 with migrants primarily in search of work and improved economic status. This region also has a high percentage of functional illiteracy among the population (27.5%). 20 Agriculture has historically been the primary driver of the Chimborazo economy, with most rural families cultivating small plots of land—97% of small-scale farmers have less than 2.5 hectares under cultivation. Potatoes are the main staple crop in Chimborazo, grown for both local consumption and distribution to other parts of the country. 21 In the last decade, the increased growth of the economy of Chimborazo into other sectors has resulted a growing trade in processed food, introduction of large supermarket chains, and the construction of commercial centers, especially in Riobamba, the provincial capital.
This study was developed 3 months after the end of a national health campaign, “Choose Well to Live Well,” designed to introduce the Ecuadorian population to the traffic light nutrition label and promote its use in the selection of healthier foods. 22 The 3-month campaign used written and audiovisual media, with materials and media developed in Spanish with translation to Quichua, the primary language of the indigenous peoples in Ecuador. Our study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human participants were approved by the institutional review boards (Bioethics Committees) of the Universidad San Francisco de Quito and the Colorado State University, respectively. Written informed consent was obtained from all study participants. The consent form was read to potential participants and any questions and concerns were addressed before asking for their participation and signature of voluntary consent. In those cases in which women could not write, they provided consent by inked fingerprint on the consent form.
Sample Selection
The canton of Riobamba, the provincial capital of Chimborazo, has both urban and rural communities. From the total of 11 parishes in the canton, 3 urban parishes (communities) were randomly selected for the study—Calpi, Lican, and San Luis. Three remote communities—San Juan, Cacha, and Pungalá—were randomly chosen as representatives of the rural population. The presidents of each of these 6 parishes were contacted and then visited by trained public health research assistants. The purpose of the investigation was explained, permission for participation of each parish was secured from the president, and a list of families in each of these 6 parishes was obtained from the respective presidents. Households were then randomly selected from each list, in proportion to the number of families listed in each parish. Each randomly selected household was visited by the team of research assistants who invited the matriarch (18-75 years) from each household to participate. In the case that a potential participant was not available, participant replacement was performed by visiting the next dwelling to the right of the randomly selected one. The total sample was composed of 394 women, n = 216 indigenous women, mean age (standard deviation [SD]) = 47.6 (15.8) years, mean body mass index (BMI) = 25.0 (3.8) kg/m2 and n = 178 mestiza women, 43.3 (17.1) years; BMI = 26.8 (4.3).
Questionnaire
A survey instrument was developed by the investigators to obtain information regarding demographics, knowledge of nutritional labeling, the perceived capacity of labeling to provide information useful in making food choices, sources of foods consumed, and self-perception of health, among others. The questionnaire was prepared after considering similar questions in previous studies. 1,5,15 The initial draft of the questionnaire was developed by the investigators and then sent to several Ecuadorian public health researchers to examine the survey for clarity as well as content and construct validity. The survey was modified accordingly based on feedback received. Then each question was subjected to discussion in a group setting by 14 public health professionals, 11 of whom resided in various regions of the province, including urban and rural settings. Five of the professionals self-identified as being indigenous and spoke Quichua, the indigenous language of this geographical region. Special attention was devoted to framing the questions within the context of the provincial culture. Again, modifications were made based on these discussions. This iteration of the survey was then field tested in 20 urban- and rural-dwelling women randomly selected within the province, feedback was solicited from those tested and from the research assistants administering the questionnaire, issues were identified, and the final iteration of the instrument was then completed. The instrument was coded for all possible responses for each variable.
Specific Information Regarding Nutrition Label Comprehension and Use
In relation to the commercially processed foods consumed by study participants, in a section of the questionnaire, the participants were asked whether they knew of the nutrition labeling system used in Ecuador and whether they were accustomed to reading such labels. If answering affirmatively to the latter question, participants were asked about the frequency with which they read the labels as well as reasons why they read the nutrition labels. For those individuals who reported not reading labels, again reasons were explored for this response.
The participants were also queried about the type of label, if any, they used when buying commercially available food, with the following options: “the traffic light colors,” “the label where nutrition information is written,” “the traffic light colors in addition to the nutrition facts label,” and “any label.” With regard to the nutritional traffic light, respondents were tested as to their comprehension of the information it provided. Three sets of visual cards were developed for hypothetical foods with differing amounts of sugar, salt, and fat contained in each food item displayed by different colors of the traffic light. Participants were asked to explain the meaning of the colored lights in regard to the levels of these food constituents in a single serving of the respective food item. Incorrect or “don’t know” responses were coded as 0 and correct responses as 1. Information from participants was also requested (using a Likert format) as to their frequency of use of each of the colored traffic lights for fat, salt, and sugar when considering buying commercially processed foods. Additionally, the participants were asked questions regarding relationships between the salt, fat, and sugar consumption and specific health outcomes.
Data Collection
Six research teams, each composed of a female and a male public health professional, were trained in principles of research bioethics, appropriate procedures for obtaining voluntary informed consent, interviewing skills, and specific methods for valid data collection and recording. These research assistants participated in numerous practice sessions over a 1-week period under the supervision of the study investigators. The assistants were approved to collect data for this study only after providing evidence of satisfactory skills under the observation of the principal investigator. Individual research teams then traveled to the randomly selected parishes and individual households for data collection during the months of March and April 2015. For the 3 rural areas composed primarily of indigenous Ecuadorians where Quichua is the primary language spoken at home, research teams included at least 1 indigenous research assistant fluent in the Quichua language.
Data Analysis
From the total of 400 study participants, 6 were eliminated from the analysis—2 for having missing values and 4 because they ethnically self-identified as neither indigenous nor mestiza (n = 1 Afro-Ecuadorian, n = 2 white, and n = 1 other). Thus, the total number of observations for analysis was 394. The questionnaire variables were coded and entered into the CsPRO2 program, and the information was reviewed and checked for accuracy. Statistical analyses were performed using the STATA version 12.0 package. Analyses of simple frequencies and test comparisons of frequencies (percentages) were conducted through χ2 and Fisher exact tests, which were dependent upon the number of observations. The level of significance was set at P < .05 and the analysis of inference was 2 tailed.
Results
Of the total population, 54.8% of the women identified themselves as indigenous and 45.2% as mestiza. The mestiza compared to the indigenous participants were slightly younger (mestiza: 72% ≤55 years; indigenous: 63.4%, ≤55 years), resided mainly in urban areas (mestiza: 98.9% vs indigenous: 8.3%), and had a higher level of education than the indigenous population (mestiza: 55.6% >6 years vs indigenous: 13.4%). A higher percentage of illiteracy (43.5%) was observed among the indigenous women compared to the mestizas (4%). The food consumed by the mestizas was based primarily on purchase from commercial markets (95%), whereas 66% of the indigenous women reported consuming foods primarily from their own cultivation, mostly potatoes and vegetables. As shown in Figure 1, there were differences in self-reported health status, with a higher percentage of indigenous women reporting poor to average health compared with the mestizas. A higher percentage of the latter reported good to excellent health.
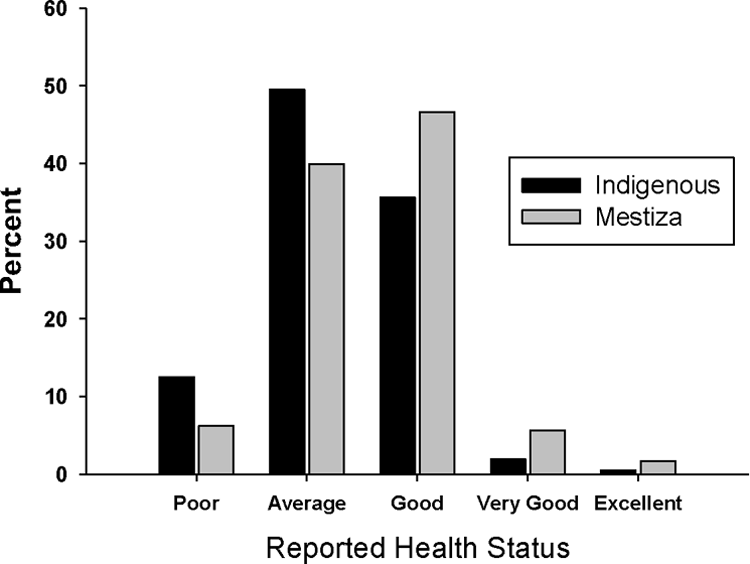
Self-reported health status among the indigenous and mestiza study participants. χ2 = 14.3, df = 4, P = .006.
With respect to awareness, comprehension, the utility of nutritional labeling, and the utility of the traffic lights system, there were numerous significant differences (P < .05) among the indigenous and mestiza population (Table 1). Figure 2 shows that a higher percentage of the indigenous population was unaware of the existence of labeling of processed foods in comparison with the Mestiza population (84.3% vs 46%; P < 0.001). Among those who said that they knew about nutritional labeling, a greater proportion of the mestizas were accustomed to reading labels than the indigenous population (39.9% vs 11.1%; P = 0.00; Figure 3). However, in the 2 groups, when food labels were read, the frequency of reading was “always/almost always,” and the main reason for doing so was wanting to be healthy (average total 85%; Table 1). Other options for reading labels such as “having diabetes,” “having hypertension,” “being overweight,” or “following a special diet” were not mentioned as a reason for the reading of labels. Among the indigenous and mestiza women who were not accustomed to reading labels, the main reason for not doing so was “do not understand what the labels mean” (50% vs 32.7%, P > .05) and to a lesser extent because they are not interested (13% vs 16%, P > .05).
Nutrition Label Use and Comprehension Among Indigenous and Mestiza Women in the Province of Chimborazo, Ecuador.a
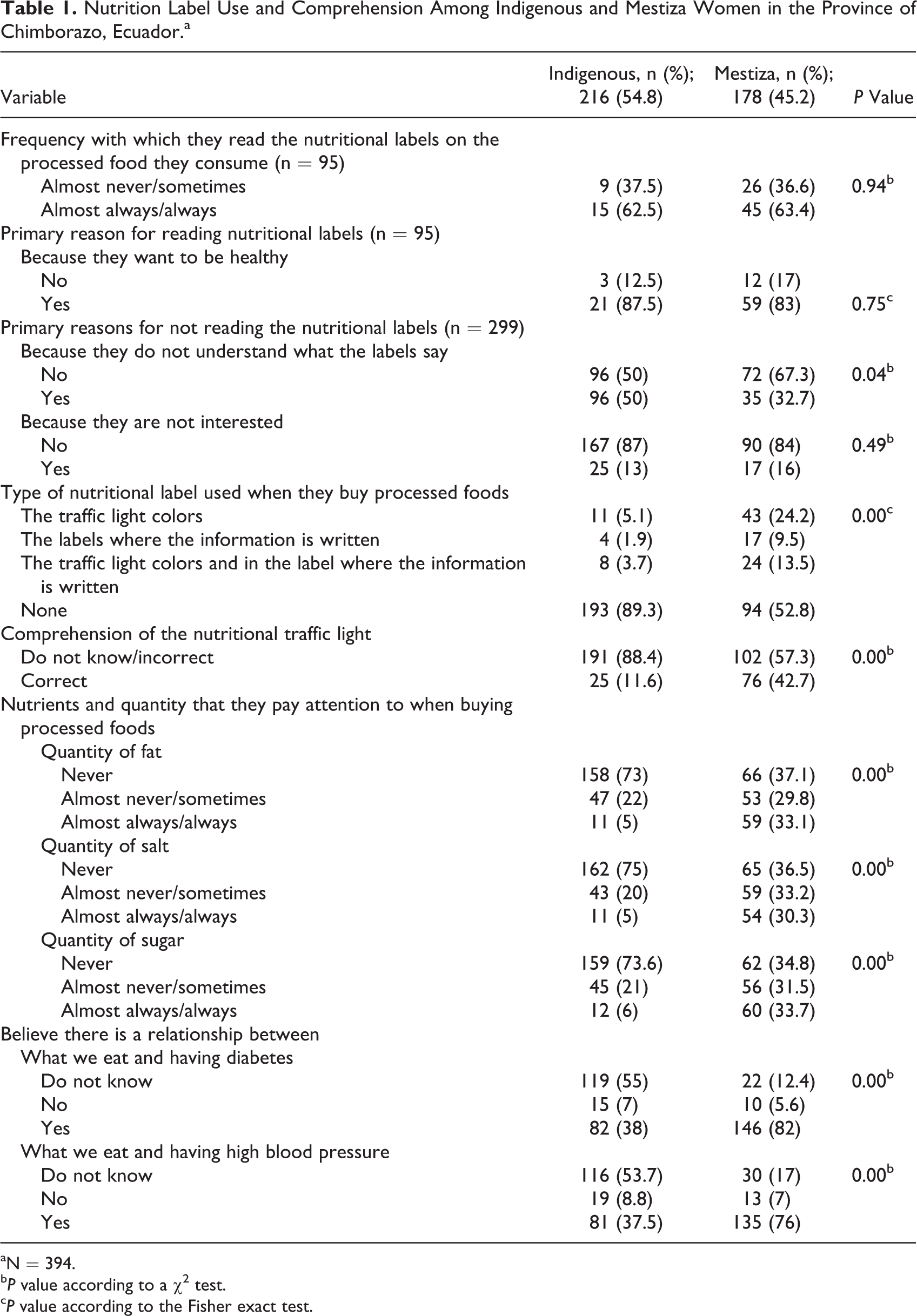
aN = 394.
b P value according to a χ2 test.
c P value according to the Fisher exact test.
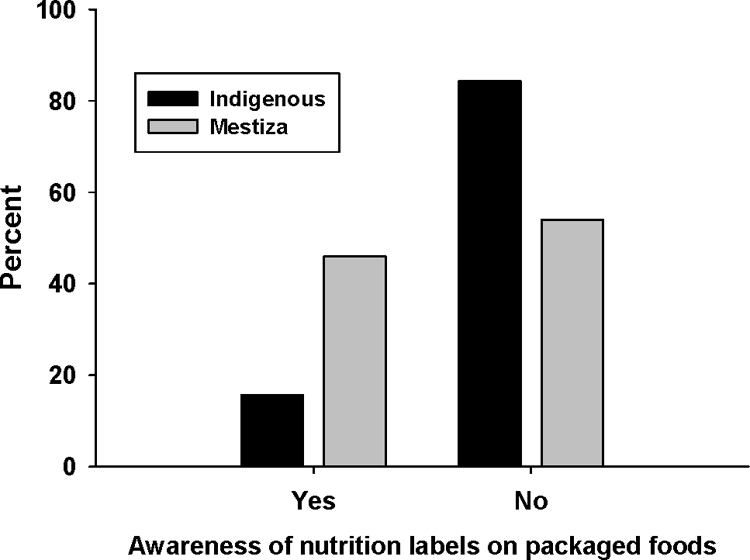
Awareness of nutrition labels on commercially available prepackaged food items among indigenous and mestiza study participants. χ2 = 64.8, df = 1, P < .0001.
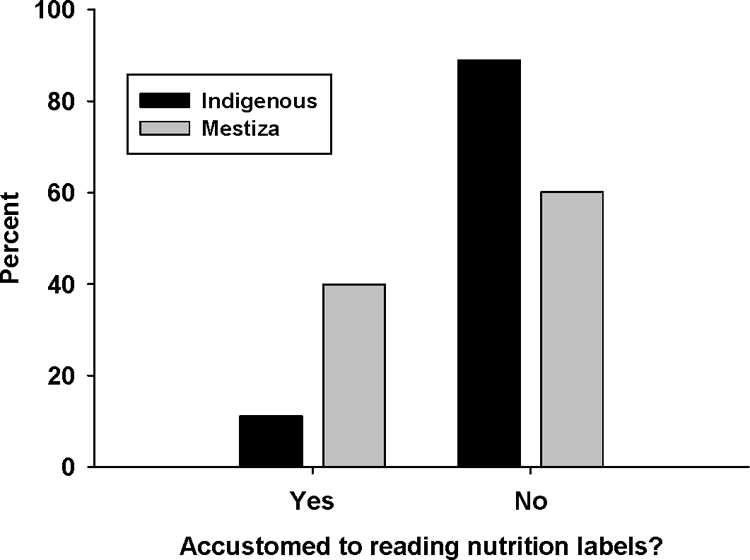
Self-reported reading of nutrition labels on commercially available prepackaged food items among indigenous and mestiza study participants. χ2 = 44.5, df = 1, P < .0001.
Among those who were aware of the nutritional labels used on commercially prepared foods, the nutritional traffic light was mentioned most frequently by the 2 groups as the format they used the most. The proportion of those who specifically used the nutritional traffic light was higher among the mestizas than the indigenous population (24.2% vs 5%; P < .001). Based on the test of knowledge regarding the meaning of the various colored traffic lights on the 3 different hypothetical label examples, on average only 42.7% of the mestiza women exhibited correct understanding of the information given by the nutritional traffic light. Among the indigenous population, this percentage was even lower (11.6%; Table 1).
Participant use of labels to provide information for nutritional decision-making was low for both groups. Only 32% of the mestiza participants and 5% of the indigenous participants reported they “almost always/always” use the label to observe the amount of salt, sugar, or fat when they buy processed food; no differences were observed in the 2 groups on the basis of the 3 individual nutrients (sugar, salt, and fat). However, a significantly higher percentage of the mestizas compared to indigenous women thought that there was a relationship between “what you eat and having diabetes or hypertension” (82% vs 38%).
Table 2 shows that the level of education and the area of residence were both related to knowledge of the nutritional labels on prepackaged foods in the 2 populations of women, more so in the indigenous population. Among the indigenous women who had no knowledge of nutrition labels (n = 182), 50.6% had no formal education, whereas among the indigenous women who reported awareness of nutrition labels, 94% had at least 6 years of formal education (P < .001). With respect to the place of residence, among the indigenous peoples in the urban area (n = 18), 23.5% had knowledge of the labels, of which 88.9% had at least a primary school education (information not presented in tables). Lack of education was also important for the comprehension of the traffic light nutritional labeling system; among the indigenous women, 48% of those who did not understand this format were illiterate versus 6.8% in the mestiza (information not provided in tables).
Awareness of Nutrition Labels on Packaged Foods by Area of Residence, Education, and Reported Health Status According to Ethnicity.
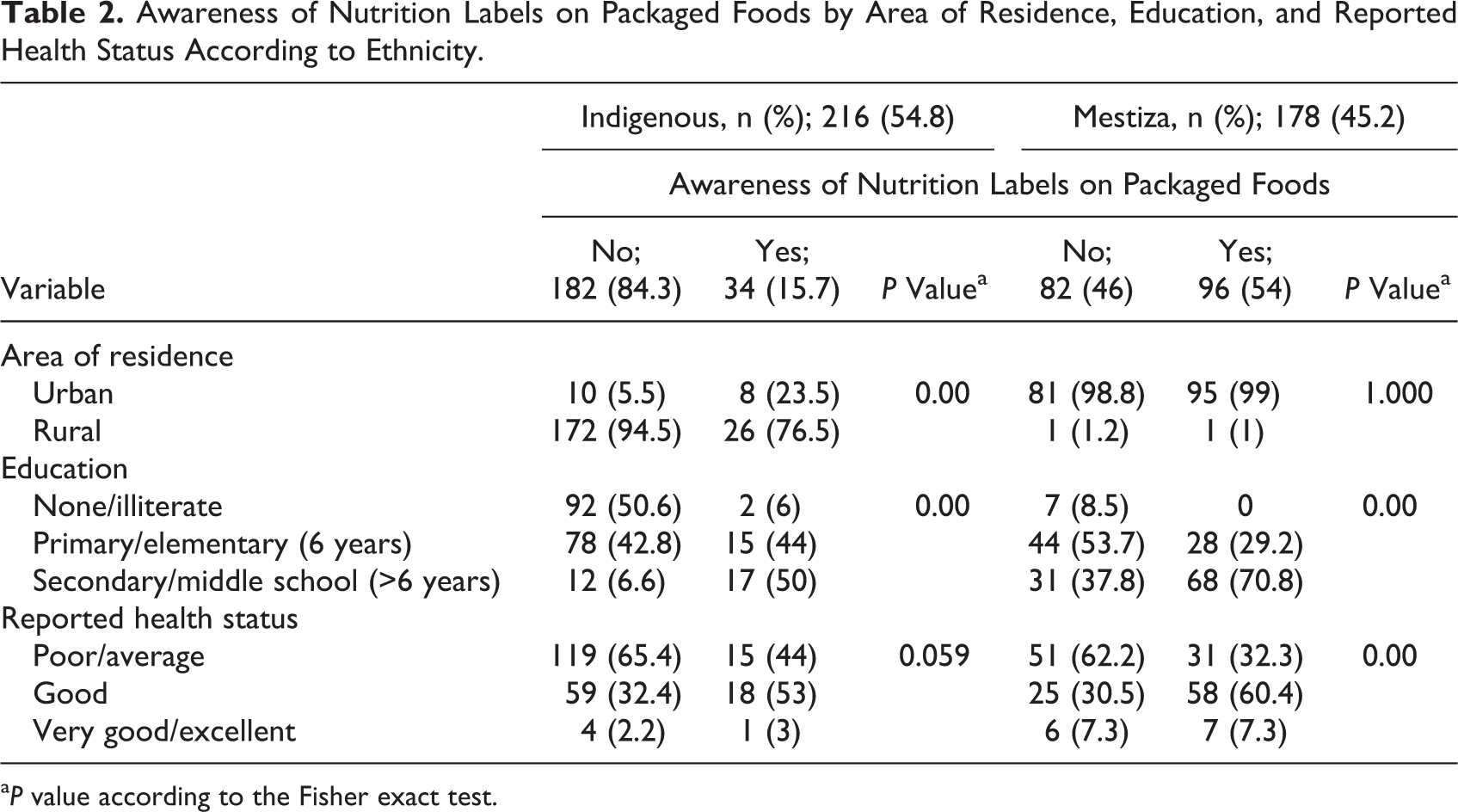
a P value according to the Fisher exact test.
Self-reported health status was also associated with awareness of nutrition labels among both groups of women. A greater percentage of both indigenous and mestizas who perceived themselves as in poor to average health lacked awareness of nutrition labels (average of 63.8% for both groups; Table 2)
Discussion
The findings of this study show that in the Chimborazo region, a geographic area characterized by significant agriculture, increasing urbanization, and increasing availability and consumption of processed foods in both urban and rural areas, the awareness and use of the nutrition labels as a tool for decision-making about food purchases is quite limited. This is evident from the fact that more than 50% of the study participants reported not using any of the nutrition label information when purchasing processed foods.
Among the indigenous women in the Chimborazo Province, more than 80% lacked awareness of nutrition labeling and only about 10% were accustomed to reading nutrition labels. This may not be surprising, given that the majority of foods consumed by indigenous women came from their own cultivation and thus their contact with nutrition labels on prepackaged foods would be limited owing to lack of access to a large array of prepackaged foods with food labels. However, during data collection, the investigators noted that in the 3 rural areas surveyed (where most of the indigenous women lived), small convenience markets were present with prepackaged foods available including chips, crackers, cookies, soft drinks, and candy. Thus, despite the lower use of processed, commercially available food items among the indigenous population, these women still had some exposure to food items with food labels.
Other factors that likely contribute to the low awareness and use of nutrition labels among the indigenous women include the lower level of education and the associated high rate of illiteracy. As observed by other authors, education is an important determinant of the understanding and use of nutritional labeling. 1,3 –5,23 In Ecuador, the indigenous population has the highest percentage of illiteracy (20.4%) in comparison with mestizos (5%), with functional illiteracy proportionately higher among indigenous women (40.1%) than men. 19 In the current study, almost 44% of the indigenous women had no formal education, a phenomenon that would clearly limit understanding of the label’s meaning. Lack of understanding was the primary reason mentioned by the study participants for not reading the nutritional labels. Even so, among the small percentage of indigenous women who were aware of nutrition labeling, the traffic light format was identified as the nutritional label used most frequently when buying processed food. Previous studies 1,7,9,11,12 highlight the use of the simple traffic light format in contributing to informed decision-making for selection of food items. This simple format may be especially important among populations with limited education, although a lack of education could even detract from comprehension of the nutrition traffic light.
Although the mestizas exhibited higher education levels and were more cognizant of the Ecuadorian nutrition labels than their indigenous counterparts, almost half of the mestiza population also reported being unaware of the nutrition label. Less than 40% were accustomed to reading nutrition labels, despite living in urban areas where prepackaged commercially prepared foods are widespread. Despite greater access to such food items, many of the women residing in urban areas still purchase many of their foods in local markets where the items are not prepackaged and thus have no nutrition labels. This phenomenon could limit the understanding and use of nutrition labels. Our findings are discordant with those of Freire et al, 12 who, based on focus group interviews, reported a high level of awareness of the traffic light label among Ecuadorian children and adults. Reasons for the disparate findings are unclear but may be related to differences in the sampling frame and educational level, with the focus group interviews of Freire et al 12 taking place in large, medium, and small cities, often in schools.
Another factor that has been identified as a determinant of nutrition label use is concern for one’s health. 24 In our study, among the relatively low percentages of both indigenous women and mestizas who were aware of nutrition labels, the primary reason for reading these labels was the desire to be healthy. This association between using nutrition labels and health concerns in some women has been shown previously. 2 However, the impact of the nutrition labeling system for decision-making was significantly greater among the mestiza population, indicating this policy was not equally effective in guiding the decisions of consumers in these different population groups. Overall, the indigenous women reported lower health status compared to the mestizas, but obviously this did not translate into a greater use of the nutrition labeling system driven by health concerns. The large difference between awareness of the nutritional labels in both groups and their actual use to determine the content of fat, salt, and sugar of commercially available foods has also been reported by other authors. 2,3,11 –13,23 There are numerous intervening variables that could contribute to this disconnection between knowledge and actual use of nutrition labels, including lack of understanding as to the relationship between salt, fat, and sugar intakes and health status as well as intransigent habits, taste preferences, and preferred food brands that may be intrinsically more important to a consumer than the nutritional quality of a food item. 12 There were marked differences observed between the indigenous and mestiza women in their knowledge of the relationship between food consumption/nutrition and risk for developing diseases such as diabetes or hypertension. The greater understanding of this relationship among the Metizas is likely associated with urban residence with greater access to health-care services and health education.
Chimborazo has historically been one of the provinces of the central Ecuadorian sierra with the highest prevalence of chronic malnutrition, with 24% to 40% of children exhibiting stunting. 25 –27 This high prevalence of malnutrition among both children and adults, especially in rural areas, has been related to an agricultural production system characterized by lack of diversity in crops grown, with little or no crop rotation from year to year. 25 Although intake of carbohydrates is high in this region, 25 deficiencies in consumption of fat, protein, and specific micronutrients including vitamins A and B12, iron, zinc, and calcium are common. 25 This phenomenon of undernutrition is especially problematic, given the high caloric intake requirements necessary to support the extreme physical demands of manual farming at high altitudes. 17 Thus, within the context of limited resources and greater food insecurity among indigenous Ecuadorians in the region, the focus of the food label on avoiding excess salt, sugar, and fat would limit its utility. Rather than limiting fat intake as proposed by the traffic light label, higher fat intakes among the indigenous farmers may be advisable in order to meet their higher energy requirements. Thus, faced with the reality of a double burden of disease risk in Ecuador characterized by overnutrition in some individuals and population groups and undernutrition in others, 28 the focus of the current nutrition label on avoiding excesses must necessarily be complemented with food security policies as well. Possibly including a green light on the label for those foods higher in protein and selected micronutrients would enhance the use of the food label in this population, especially in future years as the nutrition transition continues with increasing access to processed foods in rural areas.
The study was conducted 7 months after the country adopted the traffic light nutrition label. During this time period, a 3-month public health campaign was initiated to introduce and orient Ecuadorians to the new label. Possibly the length and/or the intensity of the campaign were not entirely adequate to reach the more remote areas of the country where there is a higher prevalence of illiteracy and fewer processed foods are consumed. We made no attempt to determine whether the study participants remembered seeing or hearing information from the campaign, so this is only speculation.
Strengths and Limitations of the Study
The sample of the study participants was chosen randomly from among rural and urban communities that were also chosen randomly from those in the Chimborazo Province. Thus, the results of this study are likely to be representative of women living in this region of Ecuador. However, one cannot extrapolate these findings to the country as a whole, as other regions differ substantially in geography, agriculture and staple crops available, climate, and ethnic diversity. We chose to include only women in this study because women compared to men have shown to be more attentive to nutrition labeling and consequently their decisions in regard to food consumption. 3,5,23 Thus, we cannot extrapolate our findings to indigenous and mestizo men or to other ethnicities in Ecuador. The sample of indigenous women was slightly older than the Mestizas and this difference in age between the 2 population groups could have contributed to the differences seen in these groups. Young adults have been shown to have greater knowledge and use of the nutrition labeling system compared to older adults. 2 As with any self-reported questionnaire data, confirmation bias could have occurred wherein the responses of the study participants were influenced by the questionnaire itself. 11 Finally, our study did not directly seek to observe the study participants’ use or nonuse of nutrition labels at the point of processed food purchase. Despite these limitations, our findings contribute to the scarce literature on this topic in Ecuador, the first Latin American country to implement the nutrition traffic light system.
Conclusion
In this descriptive study in the Chimborazo Province of Ecuador, we found that the labeling system as a public policy strategy for directing informed decision-making regarding the use of processed foods in Ecuador is principally known by the mestiza population but is barely known and used among the indigenous population of this area. The limited access to prepackaged foods with nutrition labels in rural areas, the lower level of education in these areas, the usual dietary patterns of consumption, food insecurity, and the apparently low awareness of the relationship between food and chronic diseases are likely contributors to the lack of awareness and use of nutrition labels among the indigenous women. However, even among the mestizas, almost all of whom resided in urban areas with convenient access to nutrition-labeled packaged foods, approximately half reported being unaware of nutrition labeling and less than half were accustomed to reading nutrition labels. The nutritional traffic light was the most well-known part of the nutrition labeling system, but a large proportion of indigenous and mestiza participants did not correctly understand the information presented in this system. The implementation of the nutritional labeling system in the form of the nutritional traffic light may be an important policy for the prevention of noncommunicable chronic diseases. However, for this approach to be more effective, it must go hand in hand with other strategies including literacy campaigns, especially among indigenous and other rural-dwelling women of Ecuador, among whom the lower level of education likely interferes with their awareness and comprehension of the nutritional traffic light system. A complimentary communication strategy for providing information about the risk factors associated with food consumption may also help this population perceive and better interpret the nutritional information conveyed within the nutritional labeling system. Also, given the high risk of food insecurity in limited resource populations, a traffic light system focused on increasing micronutrients and protein rather than solely focused on limiting intake of salt, sugar, and fat would appear to be very important.
Footnotes
Authors’ Note
FO helped formulate the research questions, design the study, collect, analyze, and interpret the data, and write the manuscript. DO helped formulate the research question, design the study, collect the data, and write the manuscript. MM helped formulate the research question, design the study, collect the data, and write the manuscript. MP helped design the study, collect the data, and write the manuscript. CLM helped formulate the research questions, design the study, collect, analyze, and interpret the data, and write the manuscript. All authors have read and approved the final draft of the manuscript.
Acknowledgments
The authors thank the study participants for their generous donation of time and information and the following research assistants for their help in data collection and management: Pablo Barrionuevo, Evelyn Ponce, Myrian Moyón, Diego Peñafiel, Cristina Ramos, Diana Orozco, Paola Inca, Alex Cuvi, David Janeta, Elena Bacuy, Franklin Bautista y Lucía Chávez, Fabian Muñoz, Jessica Dueñas, and Rocio Soria.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an internal grant from the Colorado School of Public Health at Colorado State University. While conducting this study, Christopher L. Melby was funded by a fellowship from the Fulbright Foundation. Neither source of funding had any role in the design, analysis, or writing of this article.