
Abstract
Background:
Maternal spot feeding programs operational in southern Indian States are providing a package of nutrition services (food, micronutrient supplementation, deworming, gestation weight gain monitoring, and fortnightly nutrition health education) to pregnant women. These remain to be evaluated.
Objective:
We evaluated the maternal spot feeding programs in 2 Southern Indian states.
Methods:
Study design was cross-sectional entailing primary data collection (July to November 2016) on 360 pregnant and lactating women (of infants aged 0-6 months) per state and a review of the scheme’s management information system (MIS) beneficiaries’ records for the time period April 2014 to August 2017. To gain program functioning insights, open-ended interviews (n = 252) with state, district, and block program managers a state-level open space technology workshop was conducted.
Results:
Average days of meal consumption ranged from 19 to 21 days per month; spot meal enhanced high dietary diversity (≥6 food groups; 57%-59%) and consumption of eggs and milk (74%-96%) among pregnant and lactating women. On-the-spot consumption of iron, folic acid, calcium, and deworming was 18%, 87%, and 56%, respectively; 94% attended at least 1 of the 2 nutrition monthly counseling sessions. Majority (68%) of the beneficiaries were motivated to enroll by self-help groups or family members, suggesting the crucial persuasive role of peers and family members.
Conclusion:
Maternal spot feeding schemes can potentially deliver nutrition interventions outlined in the World Health Organization antenatal care guidelines 2016 for a positive pregnancy outcome. Research on schemes’ impact on birth outcomes, maternal depression, social norms, and its cost-effectiveness is needed.
Introduction
Poor nutritional status of a woman before and during pregnancy is a major cause of fetal stunting. 1 In India, stunting affects approximately 47 million (38%) children younger than 5 years. 2 An estimated 5 million Indian children (19%) are born with low birth weight, approximately 4.4 million of whom are born small for gestational age. 2 Most Indian women enter pregnancy with poor nutrition—23% of reproductive-age women are too thin for their height with a body mass index less than 18.5 kg/m2 and 53% women are anemic, increasing to 58% among pregnant women. Additionally, 8% of pregnant women (approximately 4.5 million) are adolescents. 2 Diets of 71% of pregnant women in rural India are deficient in protein, while diets of 90% of pregnant women are deficient in iron. 3 The average weight gain in pregnancy is only 7 kg. 4
World Health Organization (WHO) antenatal care guidelines 2016 have placed substantially greater emphasis on maternal nutrition assessment and interventions during antenatal care. These guidelines specify balanced energy protein supplementation, micronutrient supplementation (iron folic acid [IFA], calcium), deworming, weight gain monitoring and counseling on nutrition and family planning, breast-feeding coupled with efforts to prevent and treat maternal infections, and anemia as core antenatal nutrition-related interventions to reduce risk of stillbirths and small-for-gestational-age newborns. 1
Schemes in India to deliver the abovementioned WHO 1 recommendations are largely delivered through flagship programs of 2 ministries: Women and Child Development and Health and Family Welfare. The Integrated Child Development Services (ICDS) scheme under the Ministry of Women and Child Development provisions for supplementary food as micronutrient-fortified food and/or energy-dense take-home ration for pregnant women and breast-feeding mothers at a unit cost of 9.5 Indian rupees (USD 0.14) per woman per day for 25 days a month. The supplementary food is intended to provide 600 kcal, 18 to 20 g protein, and 50% of the recommended dietary allowance of 9 essential micronutrients. 5 The Ministry of Health and Family Welfare delivers micronutrient supplements (IFA and calcium), deworming, weight gain monitoring, medicated mosquito nets (in malaria-prone areas), and counseling to pregnant women as part of antenatal care services on monthly outreach and facility-based antenatal contact points. 6 -9
However, the challenge has been to ensure these above-mentioned schemes reach an estimated 30 million pregnant women annually 10 and bundling the delivery of these schemes in one platform to ensure a compound effect of the WHO 1 recommendations. For example, receipt of balanced energy and protein supplementation from ICDS and consumption of IFA tablets in pregnancy have remained traditionally low at 51% and 30%, respectively. 2
In order to address these challenges, the state government of erstwhile Andhra Pradesh launched Indiramma Amrutha Hastham in 2013, a maternal spot feeding and counseling program in 102 high-risk administrative blocks (reaching out to 310 000 pregnant women and breast-feeding mothers across 23 949 Anganwadi centers [AWCs]–about 30% of total AWCs). Anganwadi center is village-level outpost for the ICDS program. Under this self-selective scheme, supplementary food of ICDS as dry ration was replaced with a hot cooked meal, to be consumed daily at a fixed time, normally between 11
As the scheme provides a platform to bundle various nutrition interventions, on request of the state governments of Andhra Pradesh and Telangana, we evaluated (1) on-ground implementation of components of this scheme (meal, health services, and counseling) and the recorded management information systems (MIS) data; (2) stakeholder perspectives on what’s working and what’s not; and (3) the potential for improving the nutritional profile of the enrolled women.
Key messages
Maternal short stature was 8%, wasting 19%, and severe wasting 8%. Maternal spot feeding meal enhanced maternal dietary quality and quantity; minimum dietary diversity was evident for the vast majority as was consumption of high-quality foods like eggs and milk. Self-help groups and family members played an important role to motivate the beneficiaries to eat the meal. The scheme has potential to be a platform for integrating nutrition and health interventions to ensure positive maternal health outcomes and could serve as a workable mechanism for identifying high-risk pregnancies.
Methods
The study was cross-sectional and used mixed methods comprising primary data collection (July to November 2016) and desk review of program MIS records for 3 years (2014, 2015, and 2016) and April to August 2017. Primary data were collected to assess uptake of various components of the scheme by eligible beneficiaries. Desk review of program MIS was used to assess effect of the scheme on pregnancy weight gain, birth weight, and hemoglobin levels. Using a participatory open space technology workshop method, views of diverse state stakeholders implementing the schemes were sought on barriers and enabling factors influencing implementation of the scheme (in December 2015), which was complemented with open-ended interviews of state, district, and frontline stakeholders (in July to November 2016).
Primary Data Collection
Data were collected in the months of July 2016 (in Telangana) and September 2016 (in Andhra Pradesh) by a trained team of 6 postgraduate nutritionists cum researchers who were supervised by a team of 3 senior researchers. In each state, the districts, blocks, and sectors considered the oldest geographies where the scheme was first introduced in 2015 were selected. In Andhra Pradesh, data were collected from 4 districts (Kadapa, Krishna, West Godavari, and Vishakhapatnam) across 5 ICDS projects (3 rural and 2 tribal), encapsulating 29 ICDS supervisory areas and 60 AWC. In Telangana, the districts of Karimnagar, Khammam, and Warangal were selected, covering 5 ICDS projects (3 rural and 2 tribal), 30 ICDS supervisory areas, and 60 AWCs.
A computer-generated random system was used to select blocks, sectors, and 12 AWCs per project per state. In each state, 360 pregnant and lactating women were enrolled in the scheme from the selected 60 AWCs. These women were interviewed for their sociodemographic information, receipt of scheme’s services, and experience of food insecurity conditions and coping mechanisms during that time. Anthropometry and maternal dietary diversity were ascertained on half the sample (n = 180), while 24-hour dietary recall was done on 15% of the sample (n = 57).
The interview was done using a pretested semi-structured bilingual (English and Telugu) questionnaire. Questions included age of the woman, status (pregnant/lactating), age at marriage, age at first pregnancy, religion, caste, women who never attended school, practiced open defecation, unprotected drinking water source, and self-help group membership. Services received by the women from the scheme were also recorded, such as mother and child protection card, antenatal checkups, deworming, IFA tablets and calcium tablets, medicated mosquito net, and counseling on family planning and nutrition. Household food insecurity experiences were captured using the standard 8-item Food and Agriculture Organization scale 12 using 12-month recall period. Household food security responses were categorized as follows: (1) never: not even once in past year; (2) rarely: only once or twice in past year; (3) sometimes: in some months but not every month; and (4) often: almost every month. “Sometimes” and “often” were treated as affirmative responses, and the household food insecurity score was calculated based on that. Summed affirmative responses were calculated for each household based on the household food insecurity score (0-7). Households with 0 to 3 affirmative responses were classified as “food secure households,” those with 4- to 6 affirmative responses were classified as “moderately food insecure,” and those with 7 affirmative responses were classified as “severely food insecure households.”
Anthropometric measures included height and mid-upper arm circumference (MUAC). Height was measured using the UNICEF SECA microtoise (model 216, range 20-205 cm, records variation up to 0.1 cm). Mid-upper arm circumference was measured using a MUAC tape with measurement range of 0 to 59 cm to the nearest 0.1 cm. Women were considered short stature when their height was below 145 cm. Mid-upper arm circumference <23 cm and MUAC <21 cm were used as cutoffs for wasting and severe wasting, respectively. 13,14
Micronutrient adequacy was ascertained using the Minimum Dietary Diversity–Women (MDD-W) list-based method. 15 A score consisting of simple count of 10 food groups: (1) grains, roots, and tubers; (2) pulses; (3) nuts and seeds; (4) dairy; (5) meat, poultry, and fish; (6) eggs; (7) dark leafy green vegetables; (8) other vitamin A–rich fruits and vegetables; (9) other vegetables; and (10) other fruits, consumed over a 24-hour recall period. A score less than 3 indicated low diet diversity, 4 to 5 as medium diet diversity, and more than 6 as high diet diversity. Women who consumed at least 5 of the 10 possible food groups were classified as having minimal diet diversity. Additionally, dietary intake was assessed using the 24-hour dietary recall method on the subset of 57 beneficiaries. The amount of raw food used for cooking the family meal, the total volume of food cooked, and volume of cooked food consumed by the participant (beneficiary), and the raw weight of the food ingredients was calculated by using standard tools (utensils). The data so obtained were utilized for calculating the approximate amount of raw food consumed by the participant. Data collection for dietary recall was assisted by showing models, pictures, or standardized utensils (bowls, glass, spoon, and clay models) to the participant. Subsequently, the nutrient intake of each participant was calculated. The nutritive value of food was obtained from the food composition data published in the Indian Food Composition Table, Indian Council of Medical Research, 16 New Delhi. Recommended dietary allowances suggested by the Indian Council of Medical Research 17 were utilized to assess the calorie intake of the participant manually.
Data Triangulation From Program MIS
Data from the 3 years (2014, 2015, and 2016) were collected from the program MIS. Data for 520 beneficiaries were reviewed for each financial year from the same 60 AWCs where the primary data were collected. The sample size of 520 for each year per state was calculated to be representative for each year (384; taking a design effect of 1.35 for clustering effect, a total sample size of n = 518 [rounded to n = 520] per state per year was arrived at). Additionally, MIS data (n = 566) for April to August 2017 were also collected.
The program MIS components that were captured for the purpose of the desk review included (1) identification details; (2) beneficiary profile (name, age, date of registration, migrant, caste, and religion); (3) last menstrual period; (4) gravida; (5) weight, month of pregnancy, and hemoglobin at the time of registration in AWC; (6) weight gain by month of pregnancy; (7) hemoglobin level by month of pregnancy; (8) IFA consumption by month of pregnancy; (9) number of antenatal checkups; (10) days of attendance (number of days attended for One Full Meal by month); (11) weight of child at birth and first 2 years (1, 2, 3, 4, 5, 6 and 18, and 24 months); and (12) overall attendance of the scheme and for Nutrition and Health Days.
Open Space Workshop and Informal Interviews
Views of different stakeholders (n = 252) were sought using a participatory approach workshop methodology, Open Space Technology, 18 in which the central question addressed the factors constraining and enabling the functioning of the scheme and how best the barriers could be overcome. In addition, 1-to-1 open-ended interviews were conducted with stakeholders (consultant: n = 2, state: n = 3, district: n = 5, and field level: n = 242) to find out what worked, what did not, and recommendations for the future.
Data Entry and Analysis
Primary and secondary (MIS) data were entered in CS-Pro version 4.1. Double data entry was done at the end of day by teams, verified by supervisors. Logs of indicators with errors were generated. Descriptive statistics were generated using SPSS version 12. Qualitative data were triangulated thematically.
Ethical Clearance
Ethical approval was obtained from the Amaltas Ethics Board and permission to conduct the research was obtained from the state governments. Verbal consent was obtained from each respondent before administering the questionnaire. Utmost confidentiality of information obtained was ensured by anonymizing the questionnaires and data to prevent linking to any individual.
Results
A total of 360 respondents were interviewed in Andhra Pradesh and Telangana, respectively. The sociodemographic characteristics of the respondents were reflective of underprivileged populations. The average age of respondents was approximately 23 years with slightly more pregnant women (Andhra Pradesh 57%, Telangana 51%) than lactating women. Nearly 45% belonged to scheduled castes or tribes, and 30% to 43% reported having their first pregnancy experience while they were in their teens. Mean age at first pregnancy was 19.1 (2.4 years). The prevalence of maternal low stature (height less than 145 cm) was 8%, respondents with MUAC <23 cm was 15% to 22%, and those with MUAC <21 cm was 4% to 12% (Table 1).
Sample Characteristics and Receipt of Services.
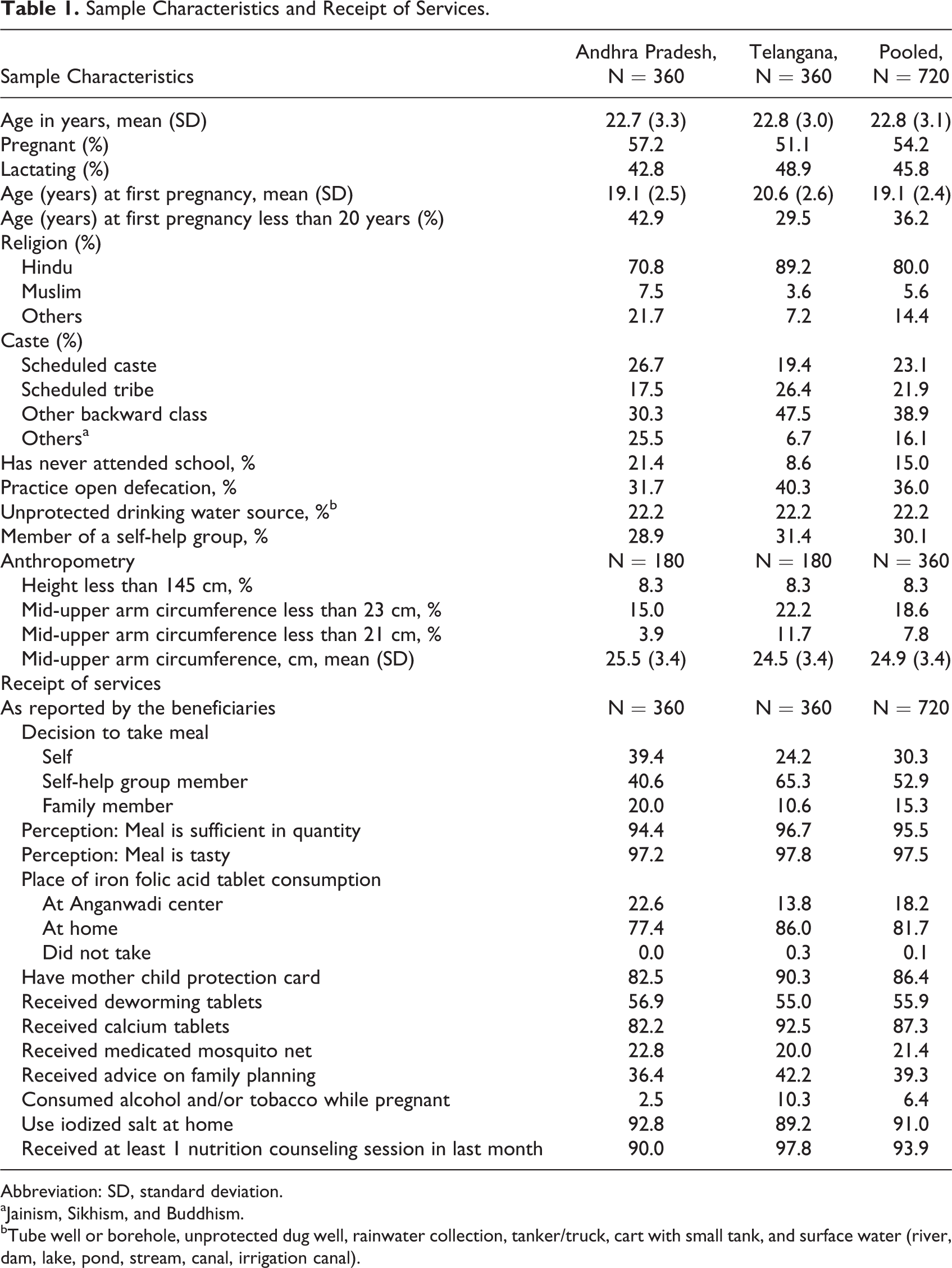
Abbreviation: SD, standard deviation.
aJainism, Sikhism, and Buddhism.
bTube well or borehole, unprotected dug well, rainwater collection, tanker/truck, cart with small tank, and surface water (river, dam, lake, pond, stream, canal, irrigation canal).
Only 24% to 39% beneficiaries had enrolled on their own initiative, while the majority were motivated by self-help groups or family members. Nearly all the beneficiaries perceived the meal to be adequate in quantity and taste (Table 1). Minimum dietary diversity (≥5 food groups) was documented in 78% to 95% of respondents (78%-95%), dietary diversity (≥6 food groups) was documented in the 57% to 59% of respondents, as also consumption of high-quality foods, such as eggs and milk (69%-99%; Table 2). Based on the 24-hour dietary recall, which was conducted in 15% of sample, in comparison to Sundays when the meal was not provided, the computed dietary energy and protein intake was mostly higher on days when the scheme’s meal was consumed. For example, in Andhra Pradesh, for the pregnant women, the mean (standard deviation [SD]) energy intake was 2669 kcal (866.6) and mean (SD) protein intake was 79 g (26.6) based on the meal eaten at site and at home. On Sunday, the mean (SD) energy intake was 2244 kcal (964.7) and mean (SD) protein intake was 72 g (43.1). For the lactating women, the mean (SD) energy intake was 2690 kcal (631.0) and mean (SD) protein intake was 78 g (17.6). On Sunday, the mean (SD) energy intake was 1946 kcal (493.7) and mean (SD) protein intake was 53 g (25.1). In Telangana, for the pregnant women, the mean (SD) energy intake was 2650 kcal (810.9) and mean (SD) protein intake was 78 g (26.7) based on the meal eaten at site and at home. On Sunday, the mean (SD) energy intake was 2464 kcal (778.5) and mean (SD) protein intake was 82 g (38.1). For the lactating women, the mean (SD) energy intake was 2816 kcal (658.8) and mean (SD) protein intake was 84 g (21.3). On Sunday, the mean (SD) energy intake was 2547 kcal (797.7) and mean (SD) protein intake was 72 g (28.2; Table 3).
Maternal Dietary Diversity.
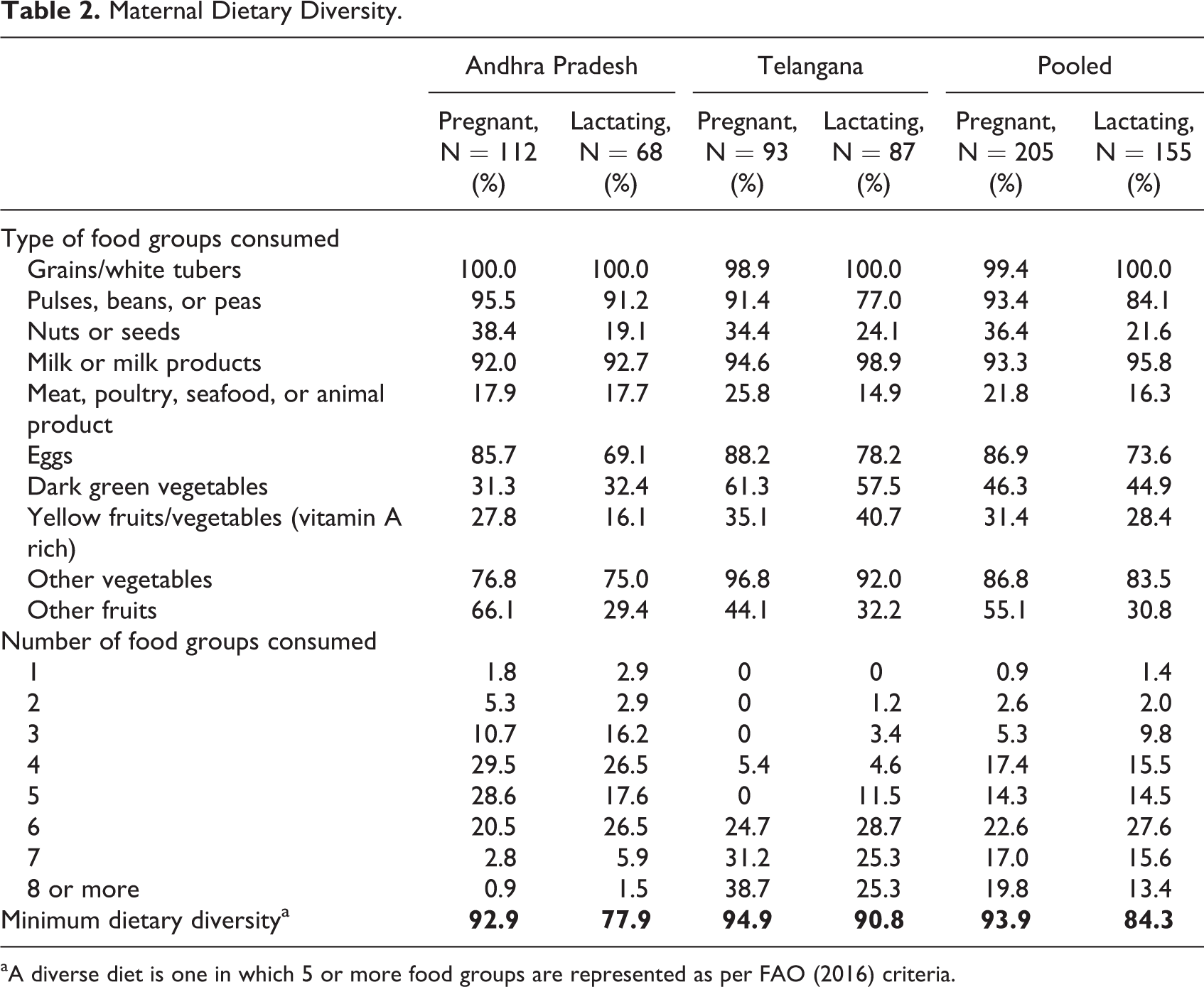
aA diverse diet is one in which 5 or more food groups are represented as per FAO (2016) criteria.
Protein and Energy Consumption of Women Based on 24-Hour Dietary Recall Method.
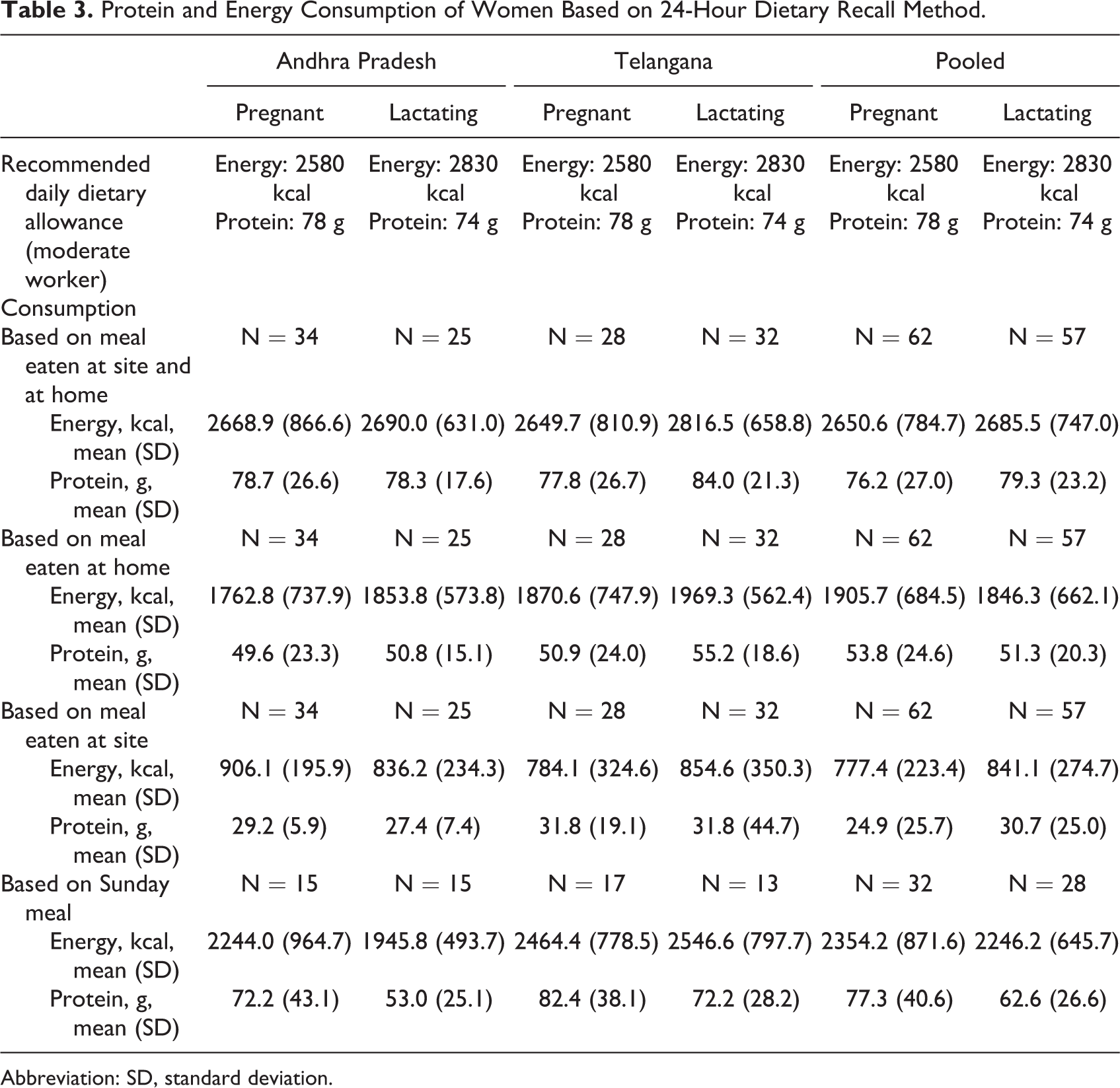
Abbreviation: SD, standard deviation.
On-the-spot IFA pill consumption was poor (14%-23%). Nutritional counseling had been imparted to nearly all, but only 36% to 42% had received family planning counseling. Severe (Andhra Pradesh 2.5%, Telangana 3.9%) and moderate (Andhra Pradesh 10%, Telangana 8.3%) household food insecurity was uncommon as assessed by raw scores. Coping mechanisms adopted by the families included household head working overtime (46%-50%), females starting to work outside home (39%-45%), and migration of a family member (11%-19%; Table 4).
Food Security and Coping Mechanisms.a
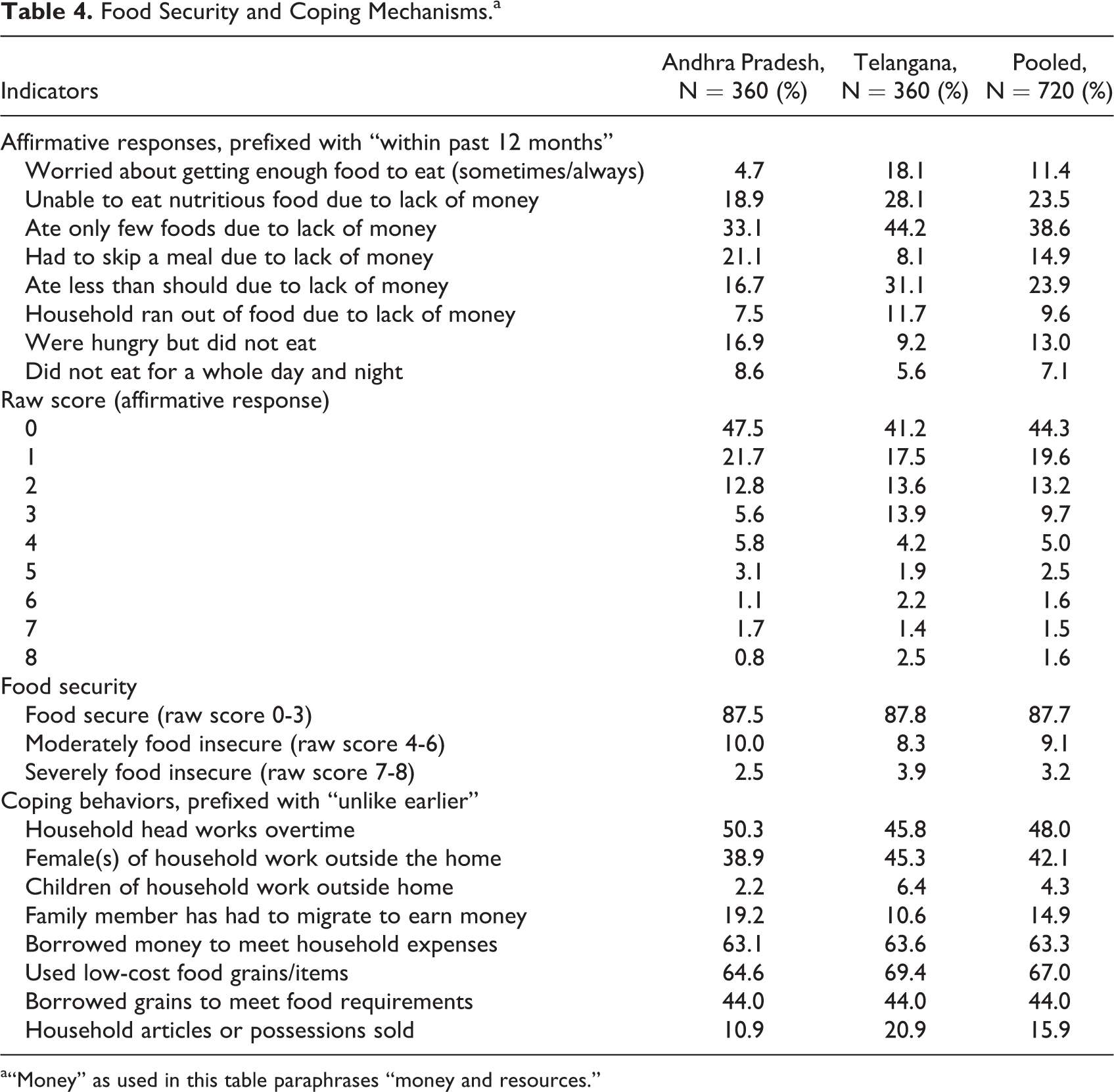
a“Money” as used in this table paraphrases “money and resources.”
In general, sociodemographic characteristics, maternal nutrition, diet diversity, on-the-spot consumption of IFA, and counseling were poorer in tribal projects. Overall, maternal nutrition and diet diversity were poorer in tribal projects. For example, 19% to 24% of women in tribal project sites were wasted compared to 12% to 21% in rural project sites. Pregnant women consuming minimum diet diversity was lower in tribal sites (79%-98%) than in rural (89%-96%; Table 5).
Comparison of Selected Indicators of Tribal and Rural Sites.
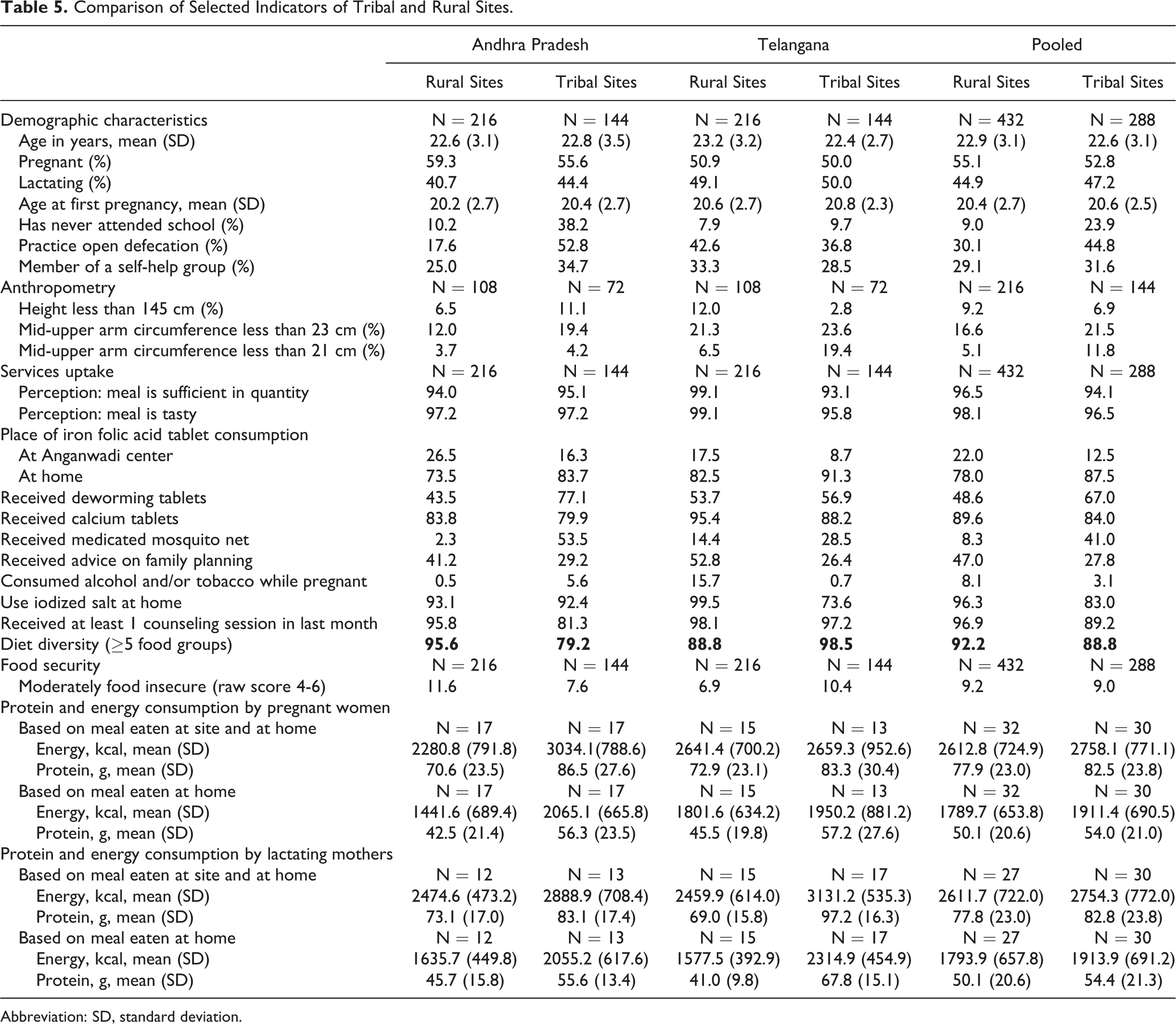
Abbreviation: SD, standard deviation.
Data retrieved from the MIS of the 3 years indicated that the average days of consumption of the scheme’s meal in a month ranged from 17 to 22 days, against the targeted 25 days. The estimated mean weight gain between the second and the ninth month of pregnancy ranged from 8.3 to 9.7 kg. The mean hemoglobin level was low. The vast majority (≥90%) of the AWCs had organized at least 1 nutrition and health day session during the past 1 month (Table 6).
Secondary Data on Program Performance Indicators.

Abbreviation: SD, standard deviation.
aDisaggregated data not available.
The resounding consensus from the qualitative survey of various stakeholders was that this is a useful program, which is well accepted by beneficiaries, with several aspects making it attractive, but some areas requiring improvements to enhance performance. These included increased ownership of local groups for community audit/review of quality of services; ensuring basic cooking, water, and sanitation infrastructure; availability of proper weighing scales; motivating beneficiaries who attend irregularly and women in high-risk pregnancy to avail themselves of the scheme; greater and functional linkage with health services, including counseling; and strengthening nutrition and health day counseling sessions through mass and mid-media, with one dedicated session for newly wed women.
Discussion
This study is one of very few formal operational evaluations of a large-scale maternal spot feeding–based integrated maternal nutrition promotion program employing mixed quantitative and qualitative techniques with due diligence for sampling methodology and quality assurance. The sociodemographic and maternal nutrition profile setting was similar to rural and tribal underserved populations of several states of India; these findings may, therefore, be relevant for such states, if they are contemplating adopting and adapting similar schemes. The primary objective was implementation research, namely, to gain insights into ground realities of the functional scheme and stakeholder perspectives to provide relevant input for improving program performance. These have been discussed below.
First, not all vulnerable groups may be covered by the scheme and greater efforts are needed to include them. The study design does not permit an estimate of the proportion of eligible beneficiaries from the region participating in this facility-based maternal nutrition program. Often, the marginalized and vulnerable segments (extreme poverty, illiteracy, lower castes or tribes, and diseased) remain divorced from such schemes. In this data set, although scheduled castes and tribes comprised approximately 45% of beneficiaries, a smaller proportion could be classified as vulnerable (stunted, wasted, or households with moderate or severe food insecurity). The scheme is therefore partially addressing social inequity through participation of some deprived beneficiaries. However, the proportion of such vulnerable pregnant women is substantially lower than that documented in recent large population-based surveys from Bihar, Chhattisgarh, and Odisha—stunted 9.8% to 13.4%, wasted 35.8% to 53.9%, households with moderate food insecurity 21.0% to 44.4%, and households with severe food insecurity 6.3% to 20.1%. 19 -21 It is therefore entirely conceivable that not all marginalized and deprived beneficiaries are reaping the benefits of this program. There is thus an urgent need for dedicated efforts to search for and enroll such beneficiaries through multiple channels, including health workers, self-help groups, and local leaders. On average, the enrolled beneficiaries availed themselves of the scheme’s meal between 70% and 85% of the targeted 25 days. Thus, they need constant education and motivation for continued attendance to reap maximal benefit. Real-time MIS use could prove helpful in tracking and reminding defaulters. Stakeholders’ suggestion to allow home delivery of food packets to physically disabled or ill beneficiaries and those residing in remote or inaccessible areas needs careful evaluation to prevent potential misuse and leakages. The majority (68%) of the beneficiaries were motivated to enroll by self-help groups or family members, suggesting the crucial persuasive role of peers and family members. Constant efforts through these and similar channels, including media and mobile phones, may be required to increase attendance and prevent default. Obviously, greater efforts and intensity would be required for the relatively underprivileged, illiterate, and those in inaccessible tribal regions.
Second, maternal diet may have been enhanced, but ground-level management is needed to improve benefits. In this setting, the scheme is operationalizing an important recommendation from the recent WHO guidelines for a positive pregnancy experience 1 : “In undernourished populations, balanced energy and protein dietary supplementation is recommended for pregnant women to reduce the risk of stillbirths and small-for-gestational-age neonates (context-specific recommendation).” Nearly all the beneficiaries perceived the meal to be sufficient in quantity and tasty. Although causal inferences are suspect with this study design, it is likely that the meal enhanced maternal dietary quality and quantity. First, minimum dietary diversity (≥5 food groups) was evident for the vast majority (78%-95%) as also consumption of high-quality foods like eggs and milk (69%-99%). This dietary diversity is substantially better than that documented in recent large population-based surveys on pregnant women from Bihar, Chhattisgarh, and Odisha, where the minimum dietary diversity was 33.5% to 57.3%, egg consumption 8.7% to 10.7%, and milk consumption 12.8% to 32.5%. 19 -21 Second, in comparison with Sundays when the scheme’s meal was not served, the computed dietary energy and protein intake was mostly higher on days when the scheme’s meal was consumed, which helps in bridging the gap in the beneficiaries’ recommended dietary allowance. Third, nutritional counseling had been imparted to nearly all beneficiaries, which may have translated into better utilization of household dietary resources. Fourth, severe (Andhra Pradesh 2.5%, Telangana 3.9%) and moderate (Andhra Pradesh 10%, Telangana 8.3%) household food insecurity was uncommon, which could either be an effect of additional food availability through the scheme or a reflection of participant bias. Qualitative data suggested that apart from the sufficient quantity of a tasty meal, providing eggs and milk added substantial value to the acceptability by beneficiaries. At some centers, there was interruption in the regular supply of eggs due to contractor problems. Moreover, beneficiaries preferred polished rice to the unpolished rice they were served. Regular managerial problem-solving at a micro level would be important to address these issues to ensure regular supply of high-quality foods in conformity with local food preferences.
Third, the scheme has potential to be a platform for integrating nutrition and health interventions to ensure positive maternal health outcomes. This scheme represents a unique opportunity to amalgamate nutrition and other health-related preventive and promotive activities to ensure a positive pregnancy outcome, especially through daily interaction with health functionaries and peers. Among several potential inputs, frequency of nutritional counseling seems reasonable, with almost all beneficiaries receiving counseling within the past month; however, the quality cannot be commented upon with this study design. Conversely, only 40% were counseled on the crucial aspects of family planning, which needs to be addressed on a priority basis. The poor on-the-spot consumption of IFA tablets (Andhra Pradesh 23%, Telangana 14%) was disappointing and may be partially contributing to low hemoglobin levels, even at near term. Stakeholders blamed infrequent and incomplete drug supplies for this situation. Apart from ensuring regular and adequate supplies, providing storage facilities for IFA tablets at the AWC, monitoring and reporting on IFA administration postmeal and IFA-focused counseling need attention. In the absence of storage facilities at the AWC, pregnant and lactating women can be encouraged to carry a blister pack of their tablets daily to the AWC. The IFA tablet consumption postmeal can then be monitored and recorded in the register by the AWW/AWT. It was reassuring that on-the-spot consumption of calcium tablets (Andhra Pradesh 82%, Telangana 92%) and periodic deworming (Andhra Pradesh 57%, Telangana 55%) were much better but still inadequate.
Fourth, the potential of MIS is not fully utilized and should be explored. Plausible and consonant data were retrieved from the MIS for 3 years and April to August 2017 for almost all the variables (meal consumption days, pregnancy weight gain, hemoglobin, nutrition, and health days), which suggests reasonable programmatic quality. However, the low birth weight prevalence from MIS indicating below 5% is implausible and may be biased, as the data pertain to the subset with birth weight records. The study design does not permit inferences about the practical use of this data set, which could be used for action to improve program outcomes. The opportunity presented through the daily presence of pregnant and lactating women at AWCs can be utilized to create an effective integrated health and nutrition monitoring system. A robust monitoring and reporting framework can quantify programmatic progress and provide input for remedial actions. The monitoring matrix should include indicators to track maternal and child health and nutrition. It seems likely that the potential of MIS is not being fully exploited for logistical aspects and for individual beneficiary use (eg, identifying high-risk individuals on basis of pregnancy weight gain, low hemoglobin level, tracking and reminding defaulters, referral). Implementation research is desirable to examine the validity of the MIS data and its potential utility for individual beneficiaries in real time.
Fifth, insights from stakeholders can improve program efficiency. The study’s qualitative methods yielded valuable insights from stakeholders into factors that are working, those that are not working, and recommendations for future. The resounding consensus was that this is a useful program, which is well accepted by beneficiaries, and several aspects are making it attractive, but some areas require early improvement to enhance performance. Some important suggestions included increased ownership of local bodies for community audit/review of quality of services; ensuring basic cooking, water, and sanitation infrastructure; motivating beneficiaries who attend irregularly; availability of proper weighing scales; and greater and functional linkage with health services, including counseling. Moreover, tribal projects need sustained efforts because these populations have poorer sociodemographic and health indices are more marginalized, illiterate, and difficult to reach.
Strengths and Limitations of the Study
The following limitations of the study merit consideration. The study was focused on a functional program, which precluded the conduct of an experimental randomized controlled design or evaluation of the entire population covered by the feeding center. Thus, the observational study design around a functional program in conjunction with the secondary analysis from the MIS does not permit robust causal inferences due to potential biases. A relatively small sample size is a further limitation. Nevertheless, some inferences, particularly from a program strengthening perspective, seem plausible. The sampling framework was based on the ICDS classification of rural and tribal projects. However, this may not be concordant with the demographic classifications of rural and tribal populations. The ability to draw conclusions on marginalized groups, like scheduled class and scheduled tribe populations, may therefore have been compromised. We also did not have data for physically disabled or ill beneficiaries who may be potential left out groups. Logistic considerations resulted in a modification of the 24-hour diet recall protocol according to the context and information correctness on availability of working condition of weighing scales, or its periodicity of calibration was not asked. Diet recall studies are typically conducted at home to make use of similar cooking ingredients and utensils, allowing for better accuracy. However, as the primary focus was documentation of program functioning in relation to the diet of pregnant and lactating women, accurate capture of food consumption at the AWC was prioritized and 24-hour dietary recall done with utensils brought by data collection teams.
Conclusion
The scheme has the potential to become an efficient and cost-effective platform to deliver amalgamated nutrition and non-nutrition interventions outlined in the WHO 1 guidelines for a positive pregnancy outcome. It could also serve as a workable mechanism for identifying high-risk pregnancies (eg, malnutrition, inadequate pregnancy weight gain, and pregnancy-related disease) and facilitating priority referral to the next level of health care. However, it is evident that the nonfood component is functioning poorly at ground level, and urgent, relevant, and perseverant efforts are necessary to ensure efficient convergence with the health system and functionaries. More studies related to the impact of such scheme on birth outcomes, cost of inaction, contribution of self-help groups coming on maternal depression, and social cohesion needed.
Footnotes
Acknowledgments
We are grateful to Shivanshi Kapoor and Anjali Krishan (Amaltas India) and Centre for Economic and Social Studies and National Institute of Nutrition in Hyderabad for data collection, data entry, and inputs for tool development. Harriet Torlesse (UNICEF Regional Office for South Asia, Nepal) reviewed initial drafts. Advisory support of Geeta Trilokh Kumar (Institute of Home Economics, New Delhi, India) and Jim Levinson (Independent Consultant) during the conduct of this study is duly acknowledged.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The three authors are employed with UNICEF. However. the views expressed are those of authors and not necessarily those of UNICEF.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This study was supported by UNICEF India.