
Abstract
Background:
Low birth weight is a significant risk factor in infant mortality and morbidity and the likelihood of chronic and clinical disease in later life.
Objective:
To identify reported associations between maternal dietary patterns and risk of low birth weight offspring.
Methods:
This article reviews some of the literature on this subject, with emphasis on maternal intake of dairy products.
Results:
Published data show a positive association between maternal dairy product intake and birth weight but are inconclusive with respect to fetal length. While data are limited, 2 studies have reported a positive association between maternal consumption of milk and yogurt and birth weight, but this association is not observed with respect to consumption of cheese.
Conclusion:
If correct, by deduction, this observation is suggestive that whey protein may be a contributing factor to birth weight. Indirect evidence supporting why this observation merits further investigation is presented.
Introduction
The adverse effects of low birth weight (LBW) cannot be overemphasized. There is a vicious, intergenerational cycle at play among the malnourished populations of the developing world. 1 Low birth weight infants are frequently stunted, meaning their height for age value is reduced by more than 2 standard deviations from the World Health Organization (WHO) Child Growth Standards median. Stunted, undernourished, young mothers have a high risk of delivering LBW infants. Infants of LBW, if also stunted, have great difficulty with catch-up growth and remain small for age. Stunted girls have a higher probability of becoming stunted mothers, and so the vicious cycle continues. The cycle is further compounded by pregnancy during adolescence. 2 Adolescent pregnancy occurs in all countries and cultures, especially within vulnerable populations, and brings its own set of additional risk factors for LBW. This cycle is dismal, but there is cause for hope. The WHO Multi Center Growth Reference Study Group indicated that short term nutritional improvement (during intrauterine life and childhood) can result, in just one generation, in a mean gain in adult height that is up to 8 cm greater than the mean parental height. 3
Definitions
Low birth weight is defined as a birth weight of less than 2.5 kg. Globally, there are approximately 20 million births every year that are classified as LBW, 95% of these occur in developing countries. 4 In both developed and developing countries, LBW is a critical factor in infant mortality and infant and childhood morbidity. LBW is influenced by a combination of the duration of gestation and intrauterine growth rates.
Prematurity refers to a gestational duration of less than 37 weeks, and while premature babies are generally small, they may well have average weights for their gestational age. In contrast, intrauterine growth retardation (IUGR) sometimes referred to as “small for gestational age” or “small for dates” is a combination of LBW and a gestational duration of greater than 37 weeks. 4 Intrauterine growth retarded infants fall into 2 categories: they can either be considered wasted, where they have average length but are thin (ie, disproportional) or their length and weight are proportionally reduced, in which case they are considered stunted. The latter category is critical to the vicious cycle. Premature babies with weight appropriate for gestational age along with disproportional or wasted IUGR infants, provided they receive the right nutrition, can catch up in their growth, whereas stunted IUGR infants do not.
Low Birth Weight Prevalence
There are multiple causes of LBW, and most of them are influenced directly or indirectly by nutrition. Maternal height, prepregnancy weight, paternal weight and height, gestational weight gain, and energy intake in developing countries are the main causes of IUGR. Poor gestational nutrition, low prepregnancy weight, and short maternal stature also result from inadequate nutrition. 4 Episodic illness, such as malaria, or excessive alcohol consumption or smoking by the mother also can contribute to LBW.
Low birth weight not only affects infant mortality and morbidity, but it also predisposes individuals to short stature, lower cognitive performance, and increased risk factors for chronic diseases, such as high blood pressure, reduced glucose tolerance, lung, kidney, and immune function later in life. In addition, LBW is also associated with increased clinical diseases such as diabetes, coronary heart disease, and increased all-cause cardiovascular mortality. 1
The WHO recommends that pregnant women consume an additional energy intake of 200 to 285 kcal per day and a somewhat modest increase in protein intake within that energy intake of 6 g per day. 5 This advice is in broad agreement with the findings of Kramer and Kakuma 6 who reviewed the outcome of balanced energy and protein supplementation during pregnancy in both nourished and undernourished women. They concluded that there was an association between the consumption of supplemental nutrition where protein contributed less than 25% of the energy and a reduction in still and small for gestational age births.
Dietary Pattern Studies
There have been a number of studies addressing dietary patterns during pregnancy. Data from New Zealand, Japan, the Netherlands, Spain, and Denmark were recently reviewed by Grieger and Clifton 7 and showed an association between “traditional” diets containing fish, low-fat dairy products, lean meat, fruit, and vegetables and higher birth weights and lower risk of IUGR. In contrast, “Western” diets predominantly composed of refined grains, processed meat, and confectionaries were associated with increased risks of small for gestational age and LBW babies. For example, in the Auckland Birthweight Collaborative study, which was included in the Grieger and Clifton review, 7 consumption of the traditional food pattern was associated with reduced odds for IUGR (odds ratio 0.86; 95% confidence interval [CI] 0.75-0.99) when compared to the Western food pattern.
Literature reviews of studies looking directly at dairy product consumption by healthy mothers and certain anthropometric parameters, such as fetal length and birth weight, have been published. A recent review by Brantsaeter et al 8 found associations between maternal dairy product consumption and fetal growth and infant birth weight. The data in the case of fetal length are rather inconclusive—2 studies they reviewed showed no associations between fetal length and maternal dairy product consumption, while another 2 showed a positive association. Cited studies with a positive association included that of Chang et al 9 who reported that in adolescent mothers, dairy intake had a positive effect on fetal femur growth (P = .001; R 2 = 0.97), and a dose–response relation was suggested in the intermediate dairy intake group (2-3 servings [1 serving = 260 mL]/d, P = .089. In addition, the study of Olsen et al 10 found an association with length at birth across the whole range of milk intakes with a total increment of 0.31 cm (95% CI: 0.15-0.46).
In contrast, birth weight data from the Brantsaeter et al 8 review suggested a more likely association with dairy product consumption. While 2 of the reviewed studies showed no association between dairy intake and birth weight, 4 prospective studies did show an association. The outcomes of these positive studies are summarized in Table 1. The positive effects were most pronounced with low to moderate milk intake levels, while excessive intake was associated with large for gestational age babies.
Summary of Studies Reviewed by Brantsaeter et al 8 Reporting a Positive Association Between Birthweight and Maternal Dairy Product Intake.
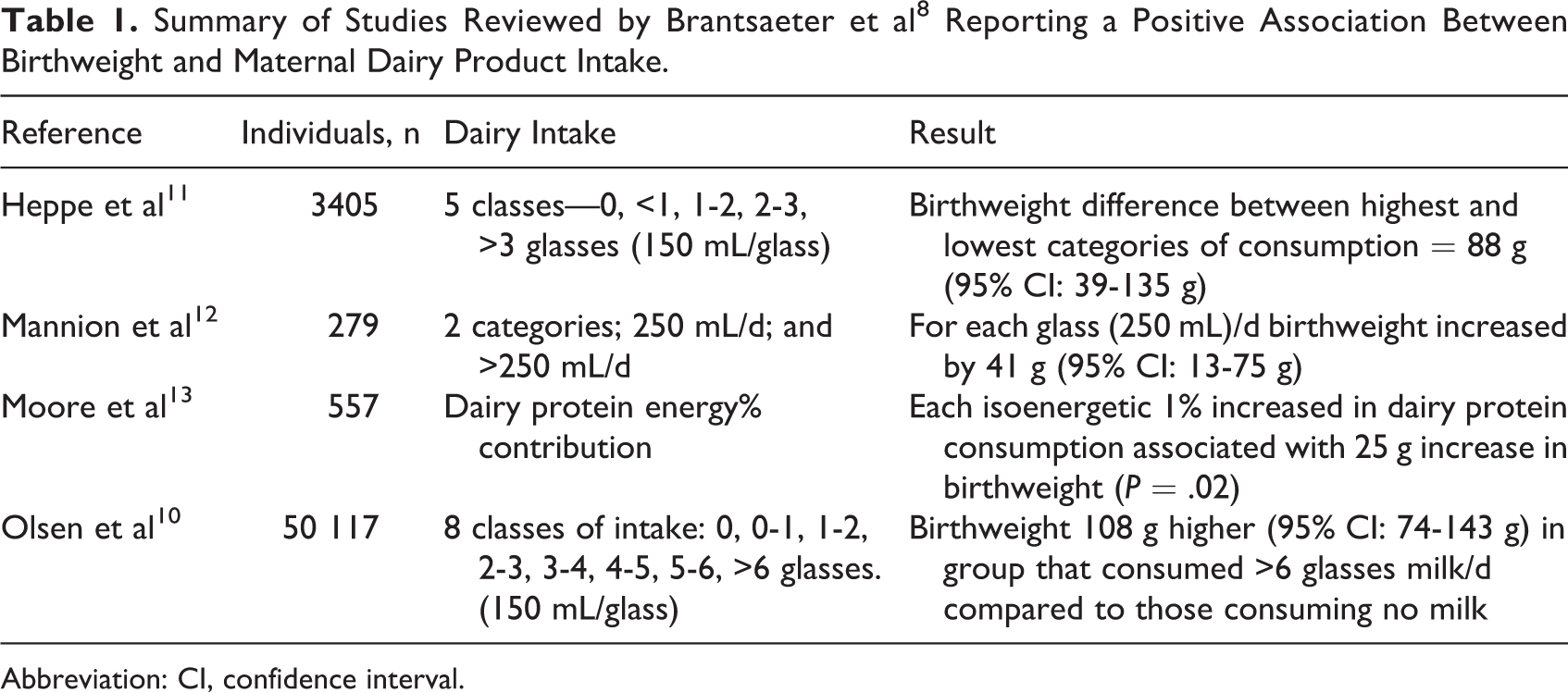
Abbreviation: CI, confidence interval.
One of the positive studies—that by Heppe et al 11 —examined data derived from the Generation R study in the Netherlands. This study investigated maternal diet, which was subsequently broken down into quintiles of consumption of different macronutrient types and sources. Some of their data are reproduced in Figure 1. Heppe et al 11 found a strong positive association between birth weight and maternal milk (milk and milk drinks) and dairy (milk, yogurt, cheese, butter, quark, milk pudding, dairy-based ice cream, and cream/creamers) protein consumption. The effect was most apparent at higher levels of milk and dairy product consumption, equivalent to 3 glasses (ie, 3 × 150 mL) of cow’s milk per day and was associated with greater fetal weight gain in the third trimester. In contrast, consumption of protein from nondairy sources had a negative association with birth weight, particularly at the highest quintile of consumption (Figure 1). The weight gain associated with the highest level dairy protein consumption was 88 g greater than that of babies whose mothers consumed low levels of milk (0 to 1 glass/d; 0-150 mL/d) during pregnancy. 11 Further analysis showed that higher birth weights were linked to the protein component of dairy products and not to the fat or carbohydrate constituents. (The negative association found with cheese consumption shown in Figure 1 will be addressed later in this article). These researchers also noted that head circumferences were increased with dairy product consumption, but there was no association found with fetal length. 11
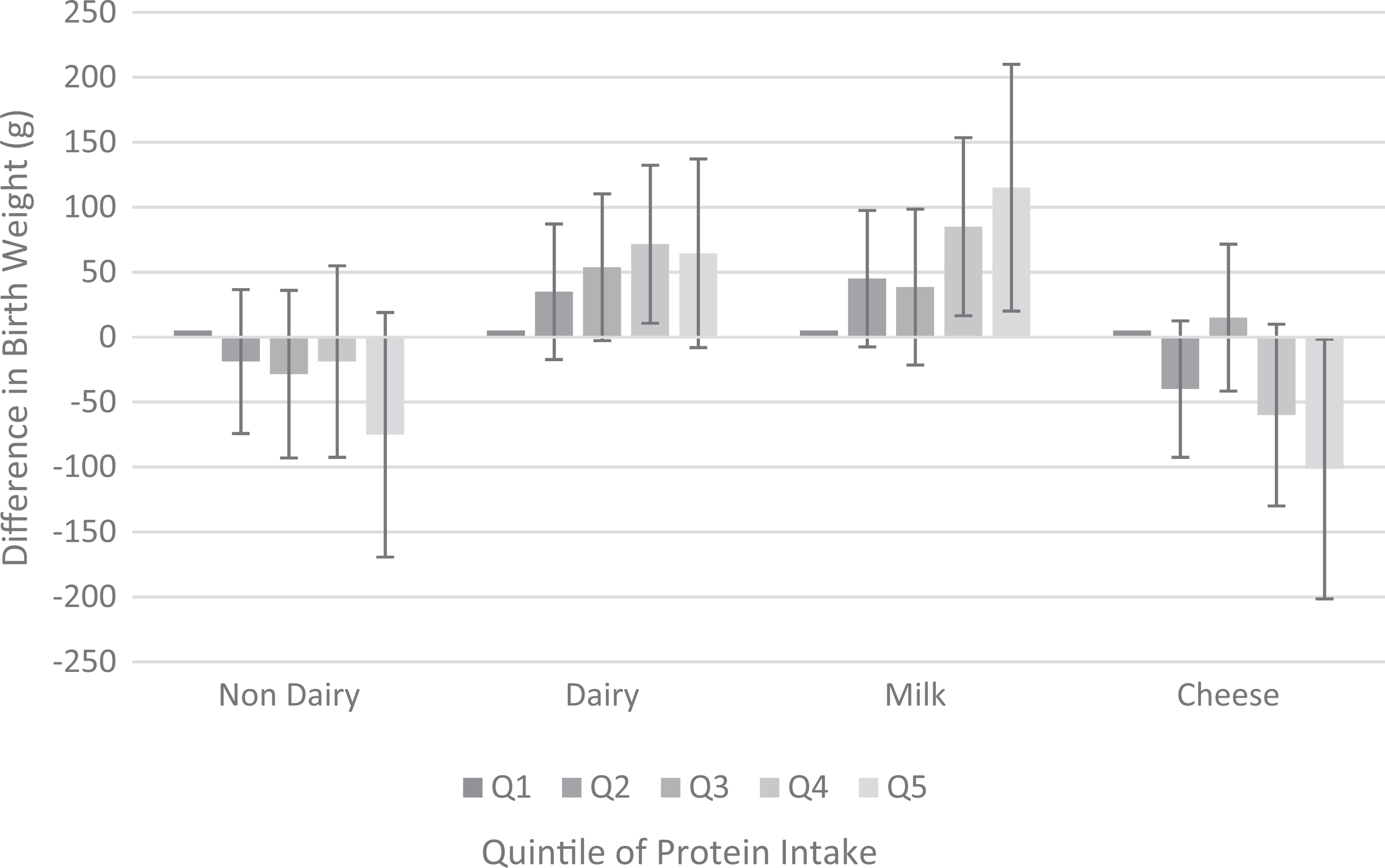
Associations of maternal protein intake with offspring birth weight: the Generation R Study, Rotterdam, The Netherlands. Results are based on multivariate linear regression models and reflect the difference and 95% Confidence Interval for each level of daily protein intake comprising non-dairy protein (P = 0.93), dairy protein (P = 0.01), protein from milk (P = 0.01) and protein from cheese (P = 0.24). Intake is expressed in terms of quintiles of consumption (Q) which are categorized as equivalent to 0, <1, 1-2, 2-3 and >3 glasses (150mL) milk/d. (Adapted from Heppe et al. 11 ).
An increased risk of LBW infants among adolescent mothers has also been reported. Adolescent growth is usually complete only 4 years after the beginning of menstruation, and concern has been expressed about potential competition between mother and fetus for nutrients in pregnant adolescents. 2 Data from studies in both developed 9,14 and developing 15 countries show that fetuses grow slower in younger mothers (10 to 16 year olds) compared to older mothers. The widely quoted study by Chang et al 9 showed there was a positive association between adolescent maternal dairy product intake between 20 and 34 weeks gestation and femur length, and this effect seemed to be dose-responsive, with optimum results between 2 to 3 servings per day (2-3 × 260 mL milk/d).
Studies investigating associations between LBW and dairy product consumption are rather difficult to carry out in developing countries. The health care infrastructure can be quite limited, there are difficulties following up longitudinal studies, and individuals frequently have to be excluded due to concerns about accuracy of birth weights or gestational age. Available studies frequently have been performed in the more affluent areas of developing countries. For example, the Barros study was conducted in the city of Pelotas, a relatively wealthy area of South Brazil. 16 The 9% of babies of known gestational age that were found to have IUGR exhibited growth retardation that was significantly associated with maternal height, prepregnancy weight, birth interval, and maternal age. This study also reported that preterm infants caught up in growth, if they were of appropriate size for gestational duration, whereas the IUGR infants did not. 16
A small study of affluent, well-nourished Indian women by Borazjani et al 17 showed that maternal high milk (>465.17 mL/d) and high protein (>70g/d) intakes were positively associated with head and abdomen circumferences and femur lengths of their babies. An earlier study by Rao et al 18 addressing a low-income group in India, where mothers were considered to be short and low on energy and protein intakes, found that birth size was strongly associated with the frequency of maternal consumption of milk, fruit, and green leafy vegetables.
The Role of Dairy Proteins
Dairy proteins are recognized as having high quality whether assessed using the Protein Corrected Amino Acid Score (PDCAAS) or the now preferred Digestible Indispensible Amino Acid Score (DIAAS) methods. Indeed, it is difficult to distinguish between different dairy fractions based on either of these quality scoring methods, as both demonstrate the superiority of dairy protein quality compared to nonanimal protein sources, such as soy, other legumes, and grains. 19 However, it is important to recognize that the DIAAS method delivers a true quality score, without the truncation of PDCAAS, thus emphasizing how dairy proteins can be used to compensate for the essential amino acid deficiencies of other protein sources by blending.
There are interesting questions that remain to be explored about the apparent protective effect that consumption of dairy proteins during pregnancy appears to offer against LBW in infants. Answers to these questions will help determine which dairy ingredients are optimal for different situations. Today, skimmed milk powder is a critical ingredient in Ready-to-Use Therapeutic Food. However, if the total protein content of dairy products is important, then milk protein concentrate obtained via ultrafiltration could be a more desirable choice. Alternatively, if certain nutritional attributes are derived from the whey protein fraction of milk, then whey protein obtained from the cheese manufacturing process can be concentrated by ultrafiltration. This latter process also removes a significant proportion of the lactose. Whey protein contains high levels of all the essential amino acids, particularly the branched chain amino acids. It is considered a “fast” (ie, quickly digested) protein and promotes muscle protein synthesis in inactive individuals. 20
As mentioned above, the study by Heppe et al 11 found that maternal consumption of dairy protein in the form of milk or dairy products had a positive association with infant birth weight (Figure 1). In contrast, Heppe et al 11 found that maternal consumption of dairy protein as cheese exhibited the opposite effect, that is, a negative association with birth weight. By deduction, this observation would suggest that maternal consumption of whey protein could be an important contributing factor to birth weight, since cheese is predominantly composed of the casein protein part of milk and contains minimal levels of whey protein. Heppe et al 11 are not the only researchers to observe conflicting effects between cheese and other dairy sources of protein, a similar effect was reported by Olsen et al. 10
Despite the need for further research to substantiate a possible role for whey, it is tempting to speculate further about why whey protein may indeed be protective against LBW. There is indirect evidence from other areas of research that could explain how whey protein affects fetal growth. These include (1) animal studies that show leucine is responsible for attenuating fetal growth restriction caused by a protein restricted diet in rats 21 ; (2) based on breast milk intake, young infants’ requirement for indispensable amino acids is most acute immediately after birth 22 ; the infant requirement in month 1 is twice that of month 4 on a mg/kg body weight basis, and there is reason to assume that the fetal requirement is similarly acute, a demand that could be in part met by maternal whey protein consumption; (3) human breast milk, the first food consumed by the newborn, is rich in whey protein, containing 3 times the level found in cow’s milk; (4) the protein concentration (predominantly whey protein) of human breast milk is significantly higher in mothers of preterm babies 23 suggesting that the youngest infants have the highest demand; and finally, (5) whey protein is considered a “fast” protein and promotes muscle protein synthesis in the inactive individuals, both elderly and young adults. 20 Given these observations, it is apparent that a potential association between maternal whey protein intake and birthweight should be investigated further.
Conclusion
Low birth weight is linked to infant mortality, morbidity, and other risk factors. Maternal nutrition and dietary patterns are highly relevant in the prevention of IUGR. There is evidence that moderate dairy product intake is associated with reduced risks of LBW infants and IUGR infants. While further research is necessary, data have been published which suggest that whey protein may be implicated in the positive association observed between dairy protein consumption and birth weight.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support from the U.S. Dairy Export Council for the research, authorship, and publication of this article.