
Abstract
Background:
Maternal anemia continues to be a public health problem in India, despite existence of multipronged governmental programs to combat it.
Objective:
This study explores the determinants of persistent anemia in poor pregnant women in an urban population in Chandigarh, India.
Methods:
A mixed method approach was used to examine the causes of maternal anemia. Three focus group discussions with pregnant women from different socioeconomic groups and 2 with female health workers were conducted to explore their perceptions and beliefs about maternal anemia and iron folic acid (IFA) tablets in urban settings in 2009. This was followed by interviews of 120 pregnant women about their nutrition knowledge and practices. Food frequency questionnaires were used to estimate daily consumption of nutrients. Finally, a follow-up survey in health clinics explored issues of stock-outs of IFA.
Results:
Sixty-five percent of respondents had hemoglobin less than 11g/dL and were anemic. Only 35% respondents obtained free IFA through public health programs. While 53% of respondents knew that they should eat green leafy vegetables, only 8% reported daily consumption of these vegetables. Focus group discussions highlighted issues around lack of food, especially for slum women, and low decision-making power in the household. Stock-outs of IFA in facilities often pushed women to purchase IFA from chemist shops.
Conclusions:
Clear gaps emerged in pregnant women’s knowledge and practice regarding diet and IFA tablet use. Lack of control over decision-making due to their low status of women was also hindering IFA use and healthy eating.
Introduction
Anemia is a major health concern globally. Pregnant women are particularly vulnerable to anemia, and it is one of the major underlying cause of maternal mortality. 1 Maternal anemia is most often due to lack of appropriate nutrients, such as iron, folic acid, and vitamin B12 but can also be due to parasitic infections (helminthes and plasmodia) or indoor air pollution. 2,3 Maternal anemia is associated with an increased risk of maternal mortality, preterm births, low birth weight babies, fetal and newborn deaths, iron deficiency anemia in infants, and decreased mental and physical potential of children. 2,4 –9
There are a number of health and nutrition programs in India aiming to combating maternal anemia, including National Rural Health Mission and Integrated Child Development Scheme (ICDS). 10 One potential tool to combat nutrition deficiency-induced maternal anemia is iron folic acid (IFA) tablets, which are made up of 0.5 mg folic acid and 100 mg iron and are to be taken daily. 5 The Government of India mandates that all pregnant women receive 100 tablets of IFA to be taken daily throughout the course of their pregnancy. 5 If a woman is anemic, the policy states that she should receive 2 tablets per day. Iron folic acid has been shown to be effective in improving anemia status in young children and in adolescent girls in India. 11,12
Another method for improving maternal nutritional status, and subsequently reducing maternal anemia, lies in changing maternal diet. Past research has suggested that in poor rural areas of India, the vast majority of pregnant women have a low dietary intake of all micronutrients except magnesium. 13 One study found that the majority of pregnant women were deficient in more than 1 micronutrient, with women most commonly being deficient in zinc, iron, and folic acid. 13 Another study, in Haryana State, found that roughly 60% of pregnant women consumed less than 75% of the daily recommended number of calories, suggesting that low food intake could be part of the cause of nutrient deficiency. 13 Hence, pregnant women in India are eligible to receive dry goods to take home through the Supplementary Nutrition Programme, and in some states they can receive hot cooked meals some days a week in Aganwadi centers. 14 Additionally, pregnant women receive education at their antenatal visits about nutrition, such as the importance of eating green leafy vegetables.
Despite these programs and policies, the most recent National Family Health Survey (NFHS) indicated that maternal and child anemia remains high across India. 15,16 According to NFHS-III (2005-2006), 41% pregnant women in Punjab and 69.7% in Haryana were anemic. Past research in Chandigarh (which is the capital of both Haryana and Punjab and the study location) found that 94% of rural, 91% of urban, and 64% of slum pregnant women reported consuming IFA. 17 It is essential to look into why women continue to be anemic, despite the existence of the anemia control program. The objective of this study was to ascertain the determinants of persistence maternal anemia in Chandigarh. Specifically, we aimed to explore if women receive IFA, and if they receive it but do not take it, why do they not take IFA tablets. We also wanted to know if pregnant women receive information about iron-rich foods and what women eat and why. This study will help in targeting educational messages and improving the distribution of IFA in the specific population group studied.
Materials and Methods
This study was conducted in Chandigarh, Union Territory, which has a population of 1 055 450 (70% urban cities, 27% slum/resettlement colonies, and 3% rural) per the 2011 census. 18 The area is similar to other union territories in the country. It represents other small cities in the country, where most of the population has migrated from the neighboring states. The study received ethical approval from the Post Graduate institute of Medical Education and Research, Chandigarh. Verbal/written informed consent was obtained from the participants depending upon their literacy status. Data were collected from February to May 2009. A partial sequential mixed-method approach (qualitative study followed by quantitative study) was used to conduct the study. 19
Qualitative Study
Focus group discussions
First, 5 focus group discussions (FGDs) were conducted—3 with pregnant women and 2 with the health-care providers. Pregnant women were recruited from the antenatal clinics of government civil dispensaries in Chandigarh city. Health-care providers also worked at the same clinics. All participants completed an informed consent (either verbally or in writing, depending on literacy skills). The goal of the FGD was to elucidate themes and inform the creation of an individual survey. Focus group discussions with pregnant women revolved around their understanding of anemia, dietary habits and knowledge, and views about the IFA tablets. Pregnant women in the FGDs were grouped into socioeconomic groups so as to make respondents more comfortable. The 3 groups were from the slum population, lower/middle class, and middle/upper class. Upper class women do not attend civil dispensaries, and therefore they were not included in the FGDs. “Slum population” was defined as living in one of the sections of Chandigarh designated “slum” areas. One FGD was conducted with auxiliary nurse midwives (ANM) and the second with the Anganwadi workers (AWW). Anganwadi workers are part of the Indian Integrated Child Development Services Program, and they provide nutrition supplements, pre- and postnatal care, health-care check-ups, and referrals and contraceptive services, with a special focus on poor and underserved populations.
Quantitative Study
Individual survey
A cross-sectional study was conducted to estimate the prevalence of anemia among pregnant women and ascertain the dietary pattern of pregnant women. A sample size of 114 respondents was estimated to be sufficient for this study based on the prevalence of anemia among pregnant women in Punjab being 42%, an error of 10%, and precision of 95%. 15 Civil dispensaries located in 4 randomly selected sectors of Chandigarh were used to recruit participants. All pregnant women who attended in these clinics were eligible to participate if they were between 15 and 45 years of age and were residing in the urban area.
From these focus groups, a questionnaire was developed for interviewing pregnant mothers at their homes. In addition, a pretested and validated Food Frequency Questionnaire (FFQ) and standard 24-hour recall charts were used for collecting nutritional data during individual interviews. 20 In the FFQ, women were asked how often and what portion size they consumed of a list of items, which were culturally relevant to this population. Recall time frame was 1 month for FFQ. In the 24-hour recall chart, women were prompted to provide information about all food and drinks they ate or drank the day before and what quantity they consumed of each item.
Respondents were either visited in their homes or approached while waiting for their antenatal care visit. The research team comprised the lead author (ND) and 2 research assistants. Research assistants were females and of similar age to that of the respondents.
Health center follow-up survey
Finally, a short questionnaire was administered to ANMs in 3 civil dispensaries in which pregnant women were enrolled for this study. The questionnaire mainly focused on IFA supply issues.
Analysis
Focus group discussion data were analyzed manually using themes on knowledge of anemia, dietary habits, knowledge, and views about IFA tablets by the lead author (ND). Individual survey data were analyzed using Stata10, and the FFQ was analyzed using a formula pretested to calculate nutrient intake. 20 This formula estimates the calories and nutrient values of a variety of different foods, taking portion size and frequency of consumption into account. 20 The nutritive value of foods was calculated following the Indian Council of Medical Research (ICMR) recommendations. 21 Anemia status was defined per World Health Organization guidelines for pregnant women (hemoglobin [Hb]< 11.0 g/dL). 22
Hemoglobin testing was not available in any of the civil dispensaries in Chandigarh. Pregnant women were advised to get this investigation done from either secondary care hospital or private laboratories. Hemoglobin was estimated using an automated hemotology analyzer. Hemoglobin results were copied from the patient’s medical record card, which the patient keeps at home and brings to the dispensary at each visit. There is delay between the timing of Hb testing after being advised by the doctor on the antenatal card and actual testing being done, because this test is not done in the dispensary itself and women either have to go to secondary care hospital or get it done in a private laboratory. Hence, Hb levels were available for 87 pregnant women of 120 respondents. Hemoglobin was not specifically tested for this survey. If Hb was tested for more than one point of time per each pregnant woman, the most recent estimate was considered.
Results
Focus Group Discussions
There were 6 women in the slum socioeconomic group FGD, 6 in the lower/middle socioeconomic group FGD, and 5 in the middle/upper class socioeconomic group FGD. Participants of the lower/middle class and middle/upper class FGDs had similar knowledge about anemia, IFA, and nutrition. Most of the women in these 2 groups had heard about anemia and were aware that it can lead to adverse health consequences for the mother and the baby. One woman from the lowest income FGD explained that she had “heard that we should eat and drink more and take care of ourselves” and another from the lower/middle income FGD explained how they knew: “there are many times such meetings are held here in dispensary, from where I have heard about it.” Some knew that an Hb level below 11 g/dL was bad for the mother and baby and that it was associated with eating: “because of poor dietary intake we usually suffer from low hemoglobin” (woman from the upper middle income FGD). All women who participated in the FGDs knew about IFA and about the sources of the IFA, including the public source “these tablets are for treatment of anemia. It will increase Hb. It is good for child. It will not cause anemia.” (middle/upper income FGD). They were, however, not very clear about whether they should take these tablets with water or milk. Some women mentioned that they eat less during pregnancy, though most knew that they should eat more. All pregnant women in these groups knew that they should eat green leafy vegetables: “we should eat green leafy vegetables, milk and egg, so that our level should be higher” (lower/middle income FGD); however, some women had misconceptions about what should be eaten and reported high-fat foods: “taking good diet, ghee (purified cream), paneer (cheese)” (middle/upper income FGD).
There were marked differences between the women belonging to the lower/middle and middle/upper classes and the women from the slum area. In the slum FGD, women had not heard about “anemia,” but most had heard about IFA or government programs that provide food or IFA tablets. Some women did not know what green leafy vegetables were. The main topic of the discussion was about trouble with getting enough food: “we know that we should eat green leafy vegetables this but we don’t eat.” Most said that they eat only 2 times a day. They mentioned the prevailing practice of eating last of all in their family: “first my husband and in-laws eat, then children, then I.” Due to this practice, sometimes not enough food is left for them to eat: “sometimes it happens that food is finished when it’s our turn to eat.” They also mentioned that their mothers-in-law have control over what is cooked and how much they will have to eat: “whatever my mother in law cooks I take, my mother in law makes the decision about what should be cooked in the house.”
Three women participated in the FGD for AWWs and 6 in the FGD for ANMs. In the FGDs with ANMs and AWWs, the respondents stated that they provided IFA to all pregnant women, educated them about how to take IFA, and about eating green leafy vegetables. Providers felt that they themselves were victims and blamed both the patients and other forces out of their control for pregnant women’s for low use and knowledge of IFA. They felt that the pregnant women did not always listen to them and many just throw away the IFA tablets, as 1 AWWs explained “they don’t really listen to us and they usually visit dispensary and follow the instructions of the doctor.” The AWWs were also afraid of the husbands of pregnant ladies and therefore were unable to tell the women what they should do. The respondents also discussed gaps in the health-care delivery system and understanding of the needs of pregnant women. Interestingly, many of the FGD participants in this group, all of whom were educated health-care providers, had not taken IFA tablets while they themselves were pregnant. Auxiliary nurse midwives and AWWs suggested supervised administration of IFA like the Directly Observed Therapy program of tuberculosis, where health-care providers watch the women take their IFA daily. An ANM suggested providing with the free food program “supply IFA to Anganwari where food is supplied, so with every plate of food they should give iron capsules.” This strategy would require providing IFA tablets through the AWWs (rather than through only the ANM). All FGD participants thought that this change in strategy would improve the anemia prevention program.
Individual Survey With Pregnant Women
One hundred and twenty women were administered the individual survey which included survey questions as well as an FFQ. Most of the pregnant women interviewed were young (mean age 25 and range 18-35 years) and had mean family income of Rs 7375 rupees (range Rs 600 to Rs 50 000). On average, they lived in households with about 5 family members (range 2-12). Most of them were literate (86%) and Hindus (80%). Forty-seven percent were graduates (equivalent to 3 year diploma after high school). About 33% belonged to lower social caste groups. Over 75% of the respondents were pregnant either for the first time (40%) or for the second (35%) time, and most of them were in the second (44%) or third (38%) trimester of pregnancy (Table 1). Eighty-seven (72.5%) women had had their Hb tested. Sixty-five percent of these pregnant women tested for Hb were anemic (28.7% moderately, 37% mildly, and none severely anemic; Table 1). Women who had not yet had their Hb measured did not differ from women who had in terms of age, caste, or religion; however, women who had not had their Hb tested were significantly less educated than women who had (t test, P = .034). Some women were too early in their pregnancies to have gotten the Hb test yet, however, some women who should have been tested had not done so.
Background Characteristics of Individual Questionnaire Respondents.a
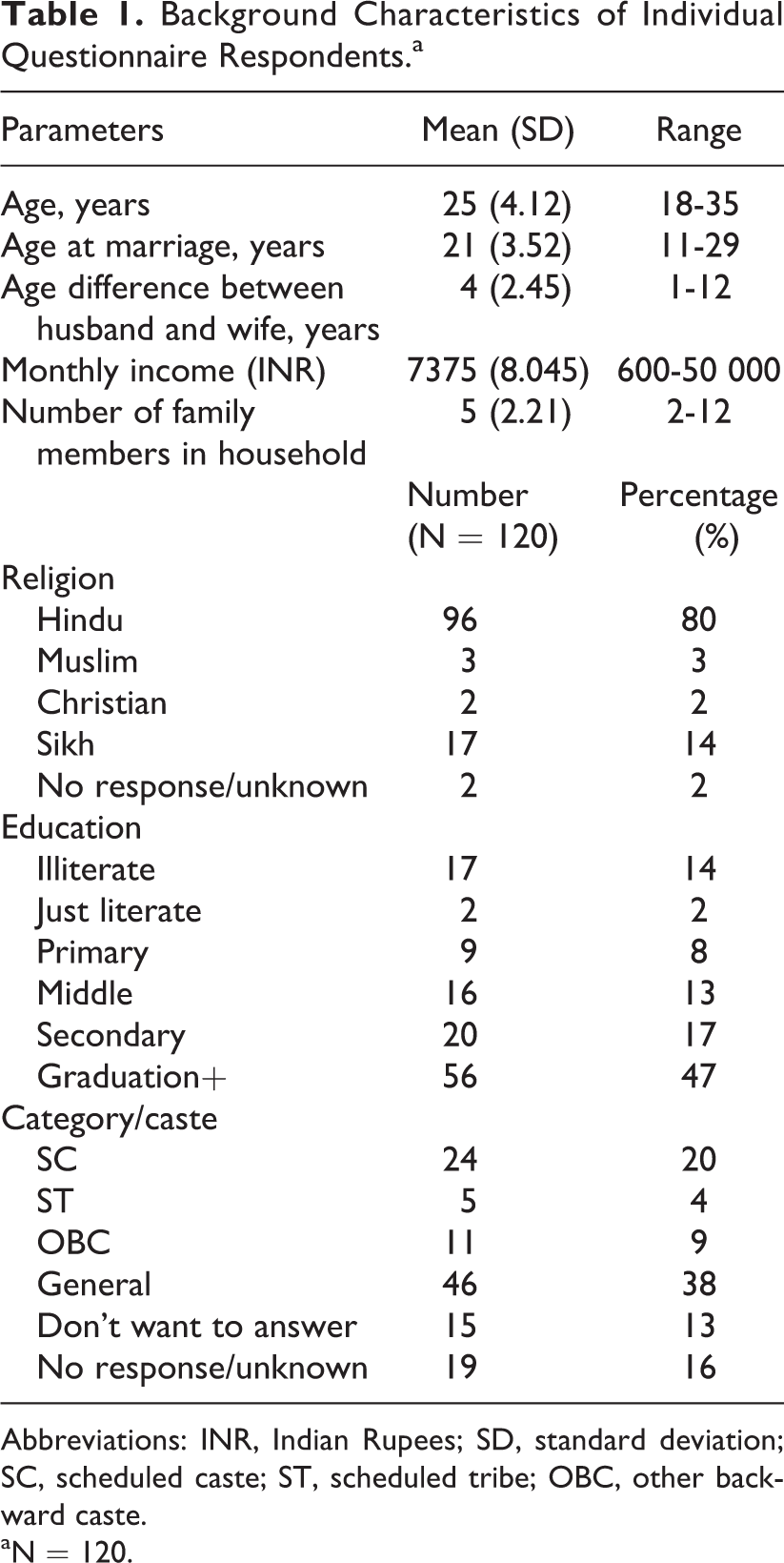
Abbreviations: INR, Indian Rupees; SD, standard deviation; SC, scheduled caste; ST, scheduled tribe; OBC, other backward caste.
aN = 120.
Level of Anemia, Diet, and Iron and Folic Acid Tablet Intake of Pregnant Women in Chandigarh, 2009.
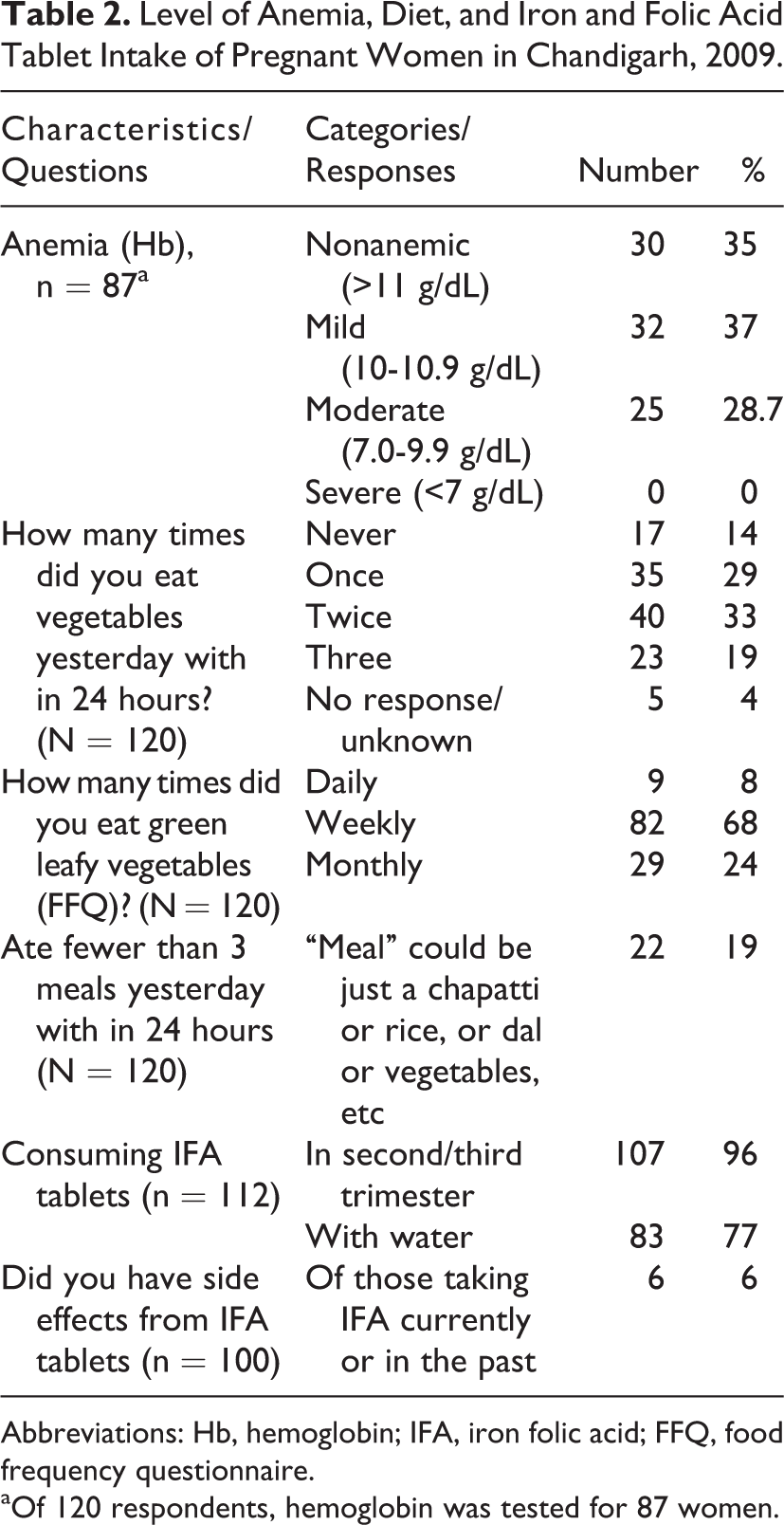
Abbreviations: Hb, hemoglobin; IFA, iron folic acid; FFQ, food frequency questionnaire.
aOf 120 respondents, hemoglobin was tested for 87 women.
Very few (6%) respondents who had taken IFA in the past reported side effects. Although 96% of respondents reported that they took IFA, only 35% were taking the IFA provided through the civil dispensary by the government program. Dispensary supplied pills were not available in 48% of households. More than 50% of them were taking multivitamins or calcium supplements in the place of IFA tablets. About 25% of them were taking IFA with milk or tea. Forty percent of respondents did not know reason to take these tablets.
Over half of the respondents specifically mentioned that pregnant women were supposed to eat green leafy vegetables and some type of calcium-containing food such as milk, curd, cottage cheese, and so on. Three percent said that pregnant women were supposed to eat meat, and 3% had no idea what pregnant women were supposed to eat. Over 30% of respondents said that someone else in the family decided what they ate and that person was the mother-in-law in 22% cases.
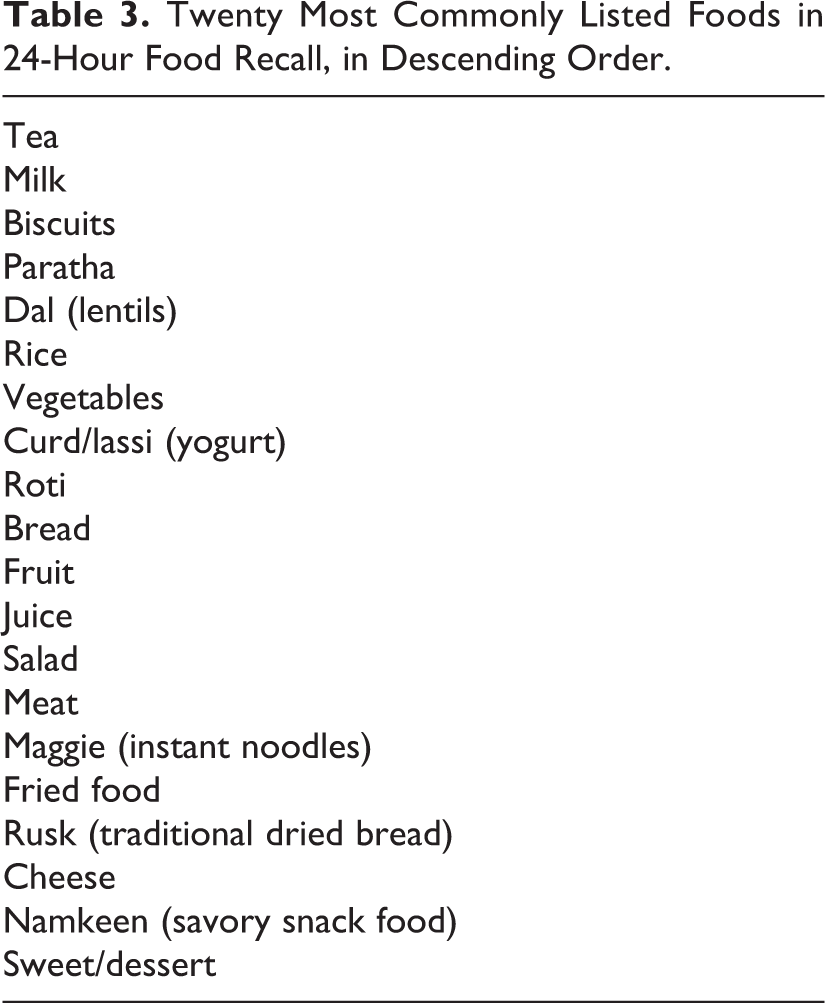
Responses from FFQ suggested that 8% of pregnant women reported of eating green leafy vegetable daily, 76% weekly, and 87% monthly. The 24-hour recall asked respondents what they had eaten yesterday (24-hour period). About 85% of respondents reported that they had eaten vegetables at any meal the day before. The 20 most commonly listed foods consumed the previous day are listed in Table 3. Some of the most commonly mentioned foods were tea, milk, biscuits, paratha/roti (wheat flat bread), rice, and vegetables (including all vegetables, not just green leafy vegetables). Almost 25% of respondents had eaten fewer than 3 meals the day before.
Twenty Most Commonly Listed Foods in 24-Hour Food Recall, in Descending Order.
Respondents were deficient in all relevant micronutrients and proteins except for fat intake, which was above the recommended daily allowances (RDAs) for pregnant women. .As can be seen in Table 4, respondents recorded below the RDA of nutrients for all nutrients except for fat and vitamin B12, based on their reporting of food intake the day before. Respondents reported a mean daily intake of 22 mg of iron, 338 μg of folic acid, 937 μg of calcium, 2360 kcal for energy, 65 g of protein, 72 g of fat, and 2 μg/d of vitamin B12.
Daily Nutrition Intake of Pregnant Women in Chandigarh, 2009.a
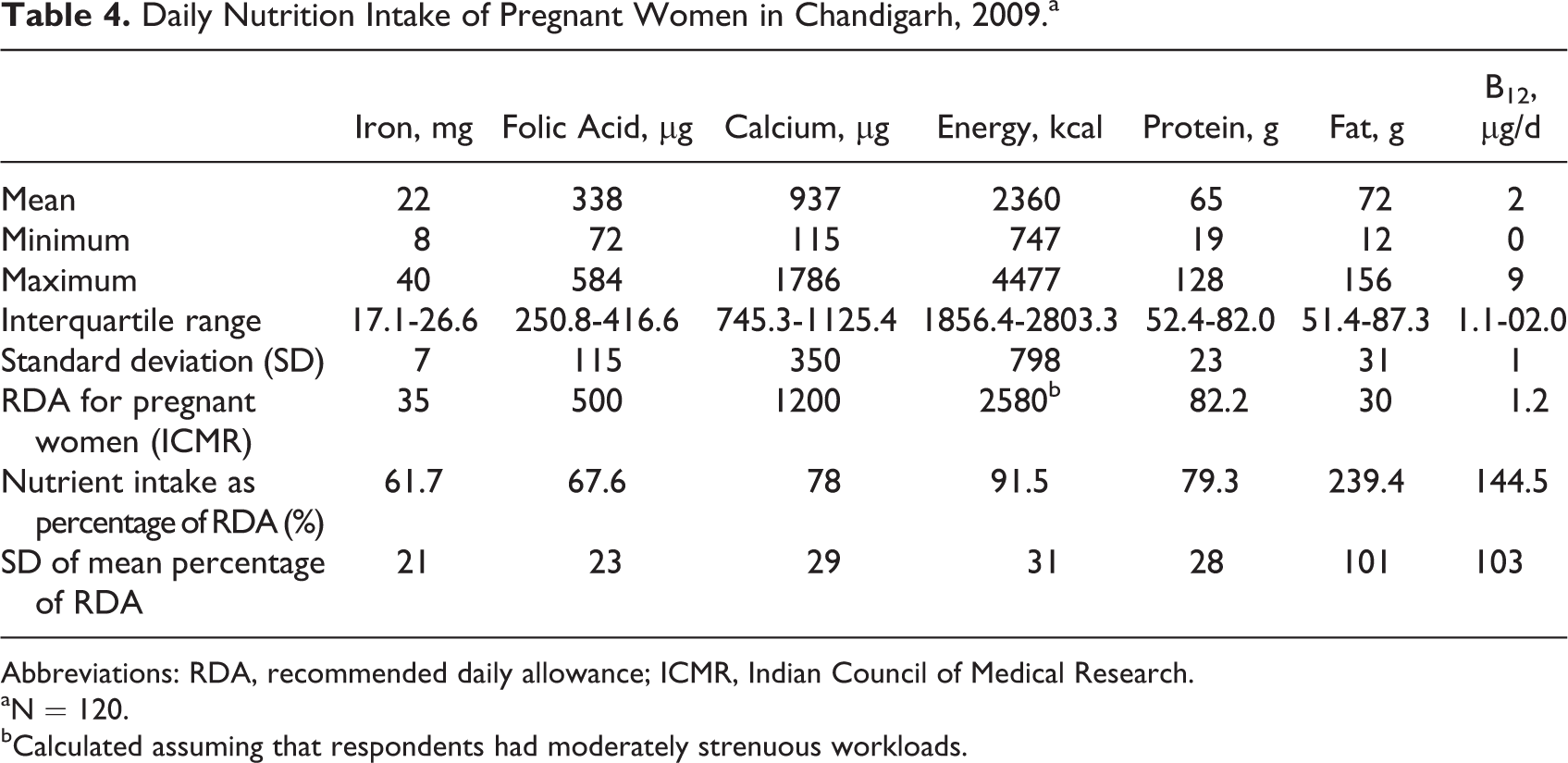
Abbreviations: RDA, recommended daily allowance; ICMR, Indian Council of Medical Research.
aN = 120.
bCalculated assuming that respondents had moderately strenuous workloads.
Thirty percent of the respondents were registered at the Anganwadi centers. Of these, roughly half said that they sometimes ate food provided by the Anganwadi centers. When asked why they did not eat the food provided at the Anganwadi centers, the most common reason was that the food was “not good” or “not tasty,” followed by the Anganwadi center being “too far away” and “not having enough time to go” there.
Health Center Follow-Up Survey
Although all 3 health centers in which we did follow-up surveys served the same patient population and were all under the auspice of the same government structure, there were marked differences in terms of how often they had stock-outs of IFA and what they did when this occurred. It appears that there is a problem of the stock of IFA running out, and overall, health centers did not know how to best handle this type of situation. In some centers, dispensary staff do tell pregnant women to buy medicines from the local chemists (when there is no supply at the dispensary), which explains why many of the respondents did not have the dispensary-supplied IFA tablets at home. Other centers had created systems where they could borrow IFA from neighboring health centers when they encountered stock-outs.
Discussion
The results of this study show that there are a multitude of factors leading to the persistence of anemia in Chandigarh. These include direct factors, such as the lack of iron and other nutrients in the diet, irregular supply of IFA in government centers, and lack of awareness about the reason of taking IFA tablets, and indirect factors that constitute larger societal factors including low status of women, poor communication between health-care providers and pregnant women, poverty, and illiteracy. These factors combine to make pregnant women less likely to get the health care and education they require to not become anemic.
The level of anemia in the study population was similar to the findings in the NFHS-3’s in this area, suggesting that the study population was representative (in terms of anemia). 15 No woman was found to be severely anemic, suggesting that better consumption of IFA in this area has prevented severe anemia. Twenty-nine percent of women surveyed has not had their Hb tested. It was not clear whether they had not been advised Hb test or they had been advised but did not agree for the test (Table 2).
Although most respondents knew that they should eat green leafy vegetables and eat more while pregnant, this was not reflected in their diet. While 53% of respondents specifically mentioned that pregnant women were supposed to eat green leafy vegetables and 85% said that they ate vegetables of some type “yesterday” in the 24-hour food recall, only 77% reported they ate green leafy vegetables weekly and only 8% reported that they ate green leafy vegetables daily. These figures are lower than the NFHS-3 findings for Punjab and Haryana, which were 85.2% and 90.0%, respectively. 15 This shows that though women are eating vegetables frequently, they do not eat green leafy vegetables, despite having relatively high knowledge that pregnant women are supposed to eat green leafy vegetables. This lack of green leafy vegetable intake was also reflected in the daily iron consumption of respondents, which was 58% of the RDA set for Indian pregnant women by the ICMR. 23
Eating green leafy vegetables only is not sufficient to prevent or treat iron deficiency anemia because of the bioavailability issues of dietary iron. Dietary iron contains 2 types: heme (derived from Hb and myoglobin from animal meat) and nonheme iron (derived mainly from cereals, fruits, and vegetables). Heme iron accounts for only 10% to 15% of total iron intake even with high meat content diets. However, heme iron is better absorbed than nonheme iron. Its absorption is not affected by iron status of the individuals and other food components except meat/fish and calcium. Nonheme iron does get affected by the iron status of the individuals, with more absorption in severely iron-deficient individuals, and presence of phytates, polyphenols, calcium, and proteins in diet inhibits its absorption, while ascorbic acidenhances its absorption. Diets in developing countries including India contain negligible amounts of heme iron, and nonheme iron is the main (90%-95%) source of dietary iron. The iron bioavailability factors for mixed diets in industrialized countries range from 14% to 18% for individuals with no iron stores, and for vegetarian diets it ranges from 5% to 12%. 24,25 In pregnancy, iron absorption increased from a mean of 7% to 30% and to 33% at gestational weeks 8 to 16, 27 to 32, and 36 to 39, respectively. 26 The absorption of iron was better among those with a lower percentage of transferrin saturation than in women with a higher percentage of transferrin saturation. 26 In theory, as much as 58% of 30 mg of dietary iron ingested per day could be absorbed (17.5 mg) by an iron-deficient, full-term pregnant woman. Thus, consuming IFA tablets is much more reliable option for treating anemia in pregnancy than just eating iron-rich diet.
Of concern is the large daily fat consumption (on average 240% of the RDA value). This particular finding can be explained by the nature of cultural preferences and beliefs of the society to which these pregnant women belong to. Eating ghee (oil made from cream) in Indian settings is quite common, as it is energy rich and especially recommended for pregnant women. Also, the way food is being cooked in most of the north Indian homes, that is, in the oil, could be the reason for excess fat and energy.
Throughout the developing and developed world, changes in diet and exercise are leading to an obesity epidemic. For example, the recent NFHS-3 data found that 29.9% of women in Punjab were obese (body mass index [BMI] < 25 kg/m3). 15 Recent research has suggested that young women who are obese are less able to absorb iron and therefore more likely to be anemic. 27 This is particularly worrisome in this setting, where pregnant women are already consuming less than the required daily iron intake and are concurrently having fat-rich diets. Unfortunately, our study did not include data on BMI, and future research could look at the correlation between BMI and anemia in pregnant women in this setting.
Respondents were also lacking in folic acid intake; however, it is reassuring to see that women were getting almost enough protein, calcium, and energy. The pregnant women in our study were getting enough vitamin B12. Only 30 (25%) women were nonvegetarian, and 9 (7.5%) were actually eating red meat; thus, the main source of vitamin B12 in this group was animal milk (81.6%), tea (82%), and yoghurt (50%). Also, there is strong evidence that small intestine of humans harbors considerable microflora (like Psedomonas and Klebseilla species), which is much more extensive in healthy Indian individuals, which synthesize significant amounts of vitamin B12. 28 This could be the reason for high levels of vitamin B12 among women in this study.
The mean iron and folic acid intake per 1000 kcal per pregnant women in this study was 11.6 mg and 132.3 μg, respectively. Iron density for pregnant women was high, as they consume greater portions of their iron and energy from vegetables, fruits, and cereals. Recommended iron density for Indian pregnant women has been revised from 14.4 mg/1000 kcal to 7 to 9/1000 kcal per nutritive value of Indian foods, ICMR, considering dietary iron content, bioavailability, and factors affecting iron status. 23,29 Only 30 (25%) women were nonvegetarian, therefore, the main source of vitamin B12 in this group was animal milk (81.6%), tea (82%), and yoghurt (50%).
Almost all (96%) of respondents in this study reported that they were taking IFA, which is higher than the NFHS-3 findings for Punjab and Haryana (65.5% and 61.1%, respectively). 15 However, only about 50% of respondents in this study were actually able to show us their IFA tablets. Thus, the actual IFA tablet consumption figure is much lower (50%) than the self-reported figure (96%) and is more similar to the state-level estimates. A large percentage of respondents did not know why they were asked to take IFA tablets. Not knowing the importance of taking IFA for their own and their baby’s health could affect their behavior toward taking the IFA regularly as is reported in study conducted in Uttar Pradesh. 30 Another major barrier to IFA use is irregular availability of IFA tablets from the government supply, as only 35% were taking IFA provided by the dispensary, and health-care staff did not know what to do when there is a shortage of IFA. It was clear from the follow-up survey with health centers that stock-outs of IFA occur not infrequently, and there is no set way for facilities to handle this situation. Some facilities reported directing women to buy IFA themselves from chemists, and many women interviewed had IFA that was not from the government. However, some women showed us “IFA” which was actually calcium or some other ayurvedic medication. Lack of regulation of the private sector and chemists, combined with low literacy and education, is putting at risk of not receiving the medicines and health care they think they are receiving. Improvements in the supply chain are essential as is regulation of chemists providing IFA and other medications.
Galloway et al 5 found various barriers in IFA use such as side effects (mostly gastrointestinal upset), deficient counseling and distribution of IFA, poor access to and quality of health services, cultural beliefs against using medications in pregnancy, and nonrecognition of signs of maternal anemia (fatigue is considered normal sign during pregnancy). Their synthesis of studies in several countries found that 30% of women reported side effects from IFA, but only 10% stopped taking IFA due to side effects, if they were counseled about how to manage side effects. 5 Side effects in our population appear to be lower, at 6%. Perhaps the higher than usual consumption of IFA in this study population is associated with low rates of side effects. To increase the compliance of IFA tablets, intermittent IFA tablets supplementation has also been explored as an alternative option in India and started under national program for weekly supplementation of adolescents but not as yet included under maternal health component. 10
Another area of concern is that almost a quarter of the respondents said that they took their IFA tablets with milk or tea. Tea is known to contain tannins, which interfere with absorption of iron. 31,32 Additionally, calcium (found in milk and often tea) can interfere with the absorption of iron. 32 Therefore, although such a large percentage of women were taking some type of iron and/or folic acid tablet, it is possible that the effect of the tablets was diminished by co-consumption of milk or tea.
In the FGDs with the slum population, the issue of lack of food due to being the “last to eat” was repeatedly raised. Individual interviews showed that about 20% of respondents ate fewer than 3 meals a day. It is important to note that in this case, a “meal” just means that they ate something (could be that they ate a chapatti or some rice only). Furthermore, over 30% of respondents did not make the decision for themselves about what to buy and eat. Anecdotal evidence from the interviews suggests that in many families, the pregnant women had little autonomy. These findings suggest that education of pregnant women alone about diet (and IFA) may not be sufficient to lead changes. It is essential that other family members should also be informed and engaged in improving pregnant women’s nutrition. Exacerbating this, many families had low incomes and could not afford to eat 3 meals daily or purchase specific foods.
A very small proportion of respondents were aware of and using the free lunches provided to low-income pregnant women through the Anganwadi centers. The most common complaint against the food provided at the Anganwadi centers was that the “food was bad,” although many of these respondents had not even tried it themselves. This suggests that there are prejudices against the program that are inhibiting use and success. Better awareness about the free food program, perhaps with a rebranding of its image, could improve the nutritional intake of pregnant women.
There was considerable difference in the knowledge, attitudes, and behaviors between the city and the slum dwellers. The lower income pregnant women in the focus groups, who were overall less well educated, had poor knowledge of nutrition, anemia, and IFA. These women were, unsurprisingly, not eating well and were also not taking their IFA as regularly as the more educated and higher social class women. This supports past research that social class and education level affect women’s health knowledge and actions. Agarwal et al 2 has also reported low literacy, poor standard living index of women, lack of awareness about anemia, and its prevention by regular consumption of iron folate tablets as contributing factors for maternal anemia.
Studies have suggested that in poor rural areas of India, vast majority of pregnant women have a low dietary intake of all micronutrients except magnesium. 33 Improvements in diet (diets rich in milk and high micronutrient foods such as green leafy vegetables and fruits) were found to be associated with larger sized babies (at birth) as well as reductions in anemia. 34 Individual counseling of underprivileged pregnant women in New Delhi, in addition to weekly reinforcements of knowledge, has been shown to improve nutritional status. 35 Other studies in India have found that pregnant women respond best to education about their nutrition when they receive education where they live, by someone who they are familiar with and in the company of others familiar to them. 36
Based on the results of this study, it is suggested that supply issues of IFA should be addressed with increased education of the staff and pregnant women. Coverage of women taking 100 tablets needs to increase to at least 80% if there is going to be a shift in maternal anemia. Having women take IFA in front of the AWW and giving IFA directly to the AWW for distribution among pregnant women could improve the program. Targeting husbands and mothers-in-law, who often have more influence in household decision-making, in addition to pregnant women, could help improve both nutrition and IFA uptake. Full utilization of existing community-based programs such as ICDS can also improve the situation. To truly increase the coverage of IFA, gaps in the supply chain to the dispensaries must be addressed. Given that the Government of India aims to provide IFA to all pregnant women, there is no reason that women should be sent to local pharmacies with mixed reputations to purchase IFA for themselves. Full utilization of existing community-based programs like ICDS can also improve the situation.
Limitations
This study has several limitations. First, the sample for the survey was comprised of women who sought care of government health facilities in Chandigarh and may not be representative of Chandigarh as a whole or other parts of India. There are also limitations to some of the tools used. The FFQs ask questions about what the woman ate the previous day, which might not reflect her usual daily consumption and is prone to recall bias. A food diary where the respondent wrote down everything she ate for a day or collecting FFQs for a few days of eating patterns could have collected more representative and less biased data, however, due to constraints on time and resources for data collection and not wanting to burden respondents, we were unable to use these methods. Another limitation is that we were not able to directly collect data on Hb, rather, we relied on measures of Hb recorded on women’s health cards. This led to some missing data and also a possible time lag between women’s measure of Hb and the data collected on eating behaviors.
Conclusion
This study used both quantitative and qualitative methods together to better understand the complex interactions between the health-care providers, individual pregnant women, and the governmental program and policy on maternal anemia and its prevention. A complex interplay of a multitude of factors is leading to persistent anemia in Chandigarh. Irregular supply of IFA, lack of awareness about the reason for taking IFA tablets, and lack of iron and other nutrients in the diet lead to anemia. Larger societal factors, such as the low status of women in this setting, poor communication between health-care providers and patients, and general issues of poverty and illiteracy, combine to make pregnant women more likely to not get the health care and education they require to avoid maternal anemic.
Footnotes
Acknowledgments
We would like to thank Ms Parampreet Kaur and Ms Luxmi Kanojiya for their work as interviewers. We would like to thank Nidhi Goyal and Rupali Mahajan for their advice about qualitative data analysis and research on nutrition specifically. We would like to thank the staff at civil dispensaries in Chandigarh for their support in recruiting patients from their clinics. Finally, we would like to thank the women of Chandigarh who gave us their valuable time and shared their experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study received ethics approval from Post Graduate Institute of Medical Education and Research’s (PGIMER) Ethics Committee, Chandigarh. Verbal/written informed consent was obtained from the participants depending upon the literacy status.