
Abstract
Objectives:
To determine the prevalence of vitamin D deficiency in 6- to 23-month-old children from 4 different ethnic groups, Han, Lisu, Hani, and Bai, in Yunnan Province of China.
Methods:
A large cohort of 938 young children aged 6 to 23 months who were living in Yunnan, China (23°28′-27°52′ N), were selected and recruited in this study. Venous-blood sampling was conducted in all the participants, and serum 25-hydroxyvitamin D [25(OH)D] levels were measured. The children’s physical status was measured.
Results:
General mean serum 25(OH)D level was 21.46 ± 7.95 ng/mL, which was obtained from a total of 938 cases. No significant difference was found in age, gender, height, and weight of participants from different ethnic groups. The mean 25(OH)D level was significantly lower in children of Lisu ethnic groups compared with that of Han and Hani participants, respectively (P < .05). In addition, Bai children had lower 25(OH)D content than Hani children (P < .001). Among the children with 25(OH)D sufficiency, the number of Lisu participants was significantly lower than Han children (P < .001).
Conclusion:
The prevalence of vitamin D deficiency varied among the ethnically different children in Yunnan, China, and significantly fewer Lisu children maintained vitamin D sufficiency compared with other ethnic children. Recognizing these ethnic differences in treating children with vitamin D deficiency may improve the therapeutic outcome.
Introduction
Vitamin D is a steroid hormone with pleiotropic actions on most tissues and cells in the body. 1,2 The 1,25-dihydroxyvitamin D [1,25(OH)2D], the active form of the vitamin D, plays an essential role in phosphorus and calcium homeostasis, skeletal growth, and bone mineralization. Vitamin D status is linked to cancer, autoimmune disease and infection, and cardiovascular disease. Although optimal vitamin D concentration remains controversial, it was commonly recommended that 75 nmol/L (30 ng/mL) is the optimum level. If the level of 25-hydroxyvitamin D [25(OH)D], which is the predominant circulating form of vitamin D, is lower than the suggested optimum level, it reflects a major public health issue. 3 There is growing concern about the functional impacts of maternal vitamin D on their offspring. Low maternal levels of 25(OH)D have been suggested to be associated with some adverse outcomes for the fetus and neonate. 4 Numerous studies have reported a high prevalence of vitamin D deficiency among pregnant women and fetus and its association with sunlight exposure. 5 –7 However, low levels of vitamin D during critical phases of development, not only before being born, have crucial effects on the long-term risk of developing diverse disease outcomes. 8 Vitamin D deficiency among minorities is suggested to be ethnically specific. 9 Thus, question raised whether ethnicity is associated with low levels of 25(OH)D in children. A study demonstrated that black or Asian race are predictors of lower 25(OH)D levels. 10 In general, nonwhite race/ethnicity was found to be a high-risk factor for 25(OH)D deficiency. 11
Yunnan is one of the most ethnically diverse provinces of China, with ethnic minorities accounting for about 34% of its total population. Difference in vitamin D status may contribute to health disparities between race/ethnic groups among young children and influence the risk of some of the leading causes of health problem in China. In the present study, thus, we aimed to assess 25(OH)D levels among children of different ethnicity aged 6 to 23 months in Yunnan Province and to determine the prevalence of vitamin D deficiency and insufficiency among the different ethnic groups.
Participants and Methods
Study Design
This was a cross-sectional survey of initial 1200 children (6-23 months old) who were born in rural area of Yunnan Province of China. Both parents came from same background of ethnic minority who were volunteered to participate in this study. Our main exposure of interest was 25(OH)D concentration of participants. Our primary outcomes of interest were deficiency and prevalence of 25(OH)D among young children of different ethnic groups in Yunnan Province.
Study Site and Participants
The study was undertaken in 4 different counties in Yunnan province in China: Pu Er Mo Jiang county (northern latitude from 23°28′ to 23°41′, Hani ethnicity is dominant), Zhao Tong Yi Liang county (northern latitude from 27°41′ to 27°52′, Yi and Miao ethnicity is dominant), Lu Shui county (northern latitude from 26°00′ to 26°13′, Li Su ethnicity is dominant), and Jiang Chuan county (northern latitude 26°31′, Bai ethnicity is dominant). In this study, the Yunnan Province is divided into 4 types of districts according to the spatial distribution, where 4 ethnic groups were predominantly inhabited, respectively.
Sampling
The study population was divided into 3 different age groups (6-11 months, 12-17 months, and 18-33 months age groups). The ethnicity was categorized as follows: Han, Lisu, Bai, and Hani. This study was conducted between October 2014 and November 2014. Serum 25(OH)D was measured using automatic chemical luminescence immunity analyzer and reagent kit (LIAISON, Diasorin, Italy) by strictly following manufacturer’s instructions. The criteria for degree of serum vitamin D level were as follows: 25(OH)D level <10 ng/mL for vitamin D deficiency, 10 to 30 ng/mL for vitamin D insufficiency, 30 to 100 ng/mL for vitamin D level sufficiency, and >100 ng/mL for vitamin D poisoning. Children anthropometric and developmental measurements were performed using YSC-2 horizontal length-measuring device and TZ-530 portable children body weighing scale.
The blood samples were collected from the Eppendorf tube at −20°C, and the serum 25(OH)D was measured by chemiluminescence method.
Ethics Statement
The study design and protocol were approved by the Ethics Committee of Kunming Medical University. Written consent was obtained from each participant.
Statistical Analysis
Data were analyzed using SPSS version 17. Means with standard deviations were presented for measurement statistics while medians with interquartile range (IQR) were presented for descriptive statistics. Comparison for general means between multiple groups χ2 test was applied, and comparison between 2 groups was analyzed with q test. Pearson’s correlation coefficient was used for estimating the correlation between maternal and children 25(OH)D concentrations. Multiple linear regression analysis was used to identify predictors of vitamin D status. We adjusted the confidence intervals and P values for the cluster design of the study.
Results
General Characteristics
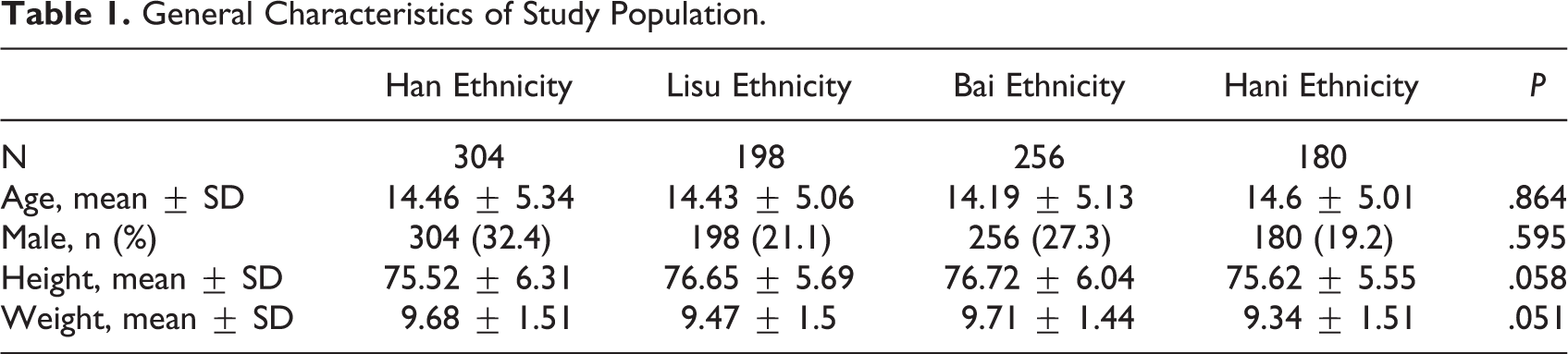
A total of 938 participants were selected and recruited with blood samples from young children of Han (n = 304), Lisu (n = 198), Bai (n = 256), and Hani (n = 180) ethnic groups. The mean age of young children from Han ethnic group was 14.46 ± 5.34, from Lisu ethnicity was 14.43 ± 5.06, from Bai ethnicity was 14.19 ± 5.13, and from Hani ethnicity was 14.6 ± 5.01. There was no obvious age difference between ethnically/racially different young children in our study (P < .05). In addition, no significant difference was found in gender, height, and weight of participants from different ethnic groups (P < .05; Table 1).
General Characteristics of Study Population.
Serum 25(OH)D level of young children from different ethnic groups in Yunnan
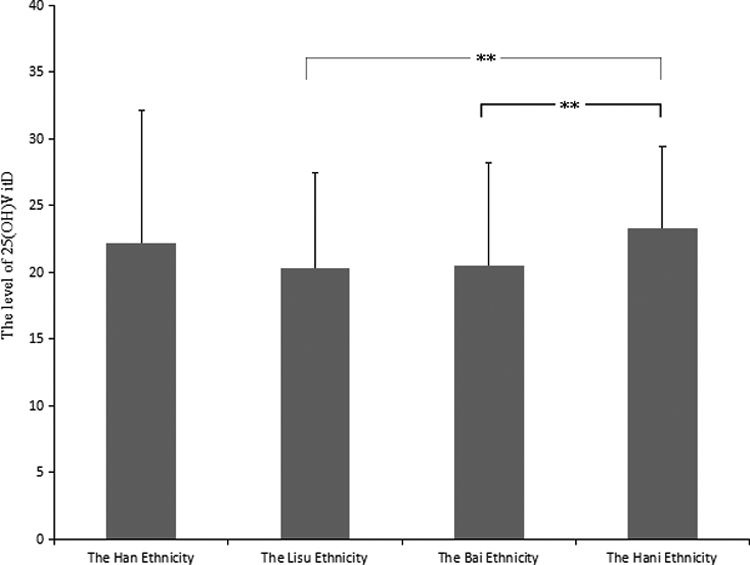
General mean serum 25(OH)D level was 21.46 ± 7.95 ng/mL, which was obtained from a total of 938 cases. The mean serum 25-(OH)D level was 23.31 ± 6.07 ng/mL in young children from Hani ethnicity, was 22.19 ± 9.91 ng/mL in participants of Han ethnicity, was 20.48 ± 7.72 ng/mL among children of Bai ethnicity, and was 20.29 ± 7.16 ng/mL in children from Lisu ethnicity (Table 2). The mean 25(OH)D level was significantly lower in children of Lisu ethnic groups compared with that of Han and Hani participants, respectively (P < .05). In addition, Bai children had lower 25(OH)D content than Hani children (P < .001). In order to further clarify the vitamin D status among ethnically/racially different children, we conducted subgroup analysis based on 25(OH)D content classification—sufficient, insufficient, and deficient. Results showed that among the children with 25(OH)D sufficiency, the number of Lisu participants was significantly lower than Han children (P < .001). There was no significant difference between different ethnic groups in insufficient and deficient subgroups (Figure 1).
Serum 25(OH)D Status of Young Children Among Different Ethnicity in Yunnan.
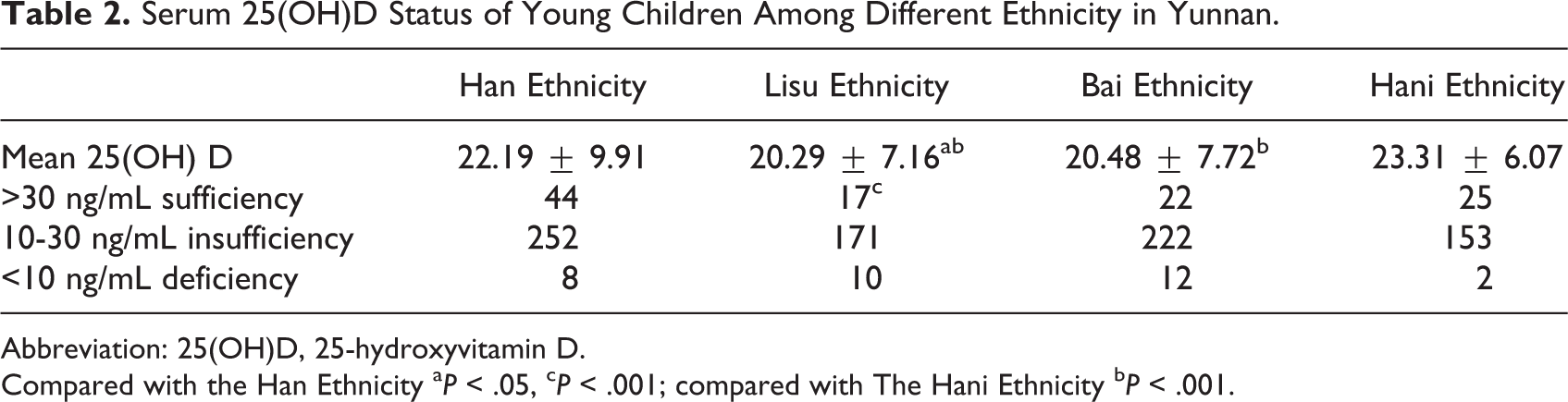
Abbreviation: 25(OH)D, 25-hydroxyvitamin D.
Compared with the Han Ethnicity a P < .05, c P < .001; compared with The Hani Ethnicity b P < .001.
General characteristics of study population.
Discussion
Our study investigated the vitamin D status among young children aged 6-23 months from 4 different ethnic groups in Yunnan, China. The mean serum 25(OH)D level of young children was lower in Lisu ethnicity compared with Han and Hani ethnicity, respectively, and it was lower in Bai ethnicity compared with Hani, but not Han, ethnicity. Significantly fewer Lisu children were subjected to vitamin D sufficiency compared with other ethnic children. No substantial difference in age, gender, height, and weight was found. This means that difference in vitamin D status among young children may be ethnic-specific.
Multiple factors likely contributed to race/ethnic vitamin D differences including economic status, reduced nutrient intake, and the skin pigmentation. 12 Minority groups are more likely to have lower incomes compared with Majorities 13 and their access to nutritious food may be too expensive or limited, therefore contributing to nutrient health disparities. 14
Han ethnicity has been referred as majority in China, accounting for 92% of total population. The total population of Hani ethnicity was up to 1.63 million, and they are living in isolated geographical conditions, mostly riverside of Naban River. 15 This makes Hani ethnic group unique and genetically homogeneous due to a relatively low rate of migration and intermarriages. 16 Lisu ethnic group has population of 1.26 million and mostly living in Yunnan and border land of Burma, Thai, and East India. Unlike Hani ethnicity, Lisu people have higher migration rate and generally have darker skin. 17 Bai ethnic group ranked the 15th largest of the 56 ethnic groups, accounting for 1.9 million population, in China, and they live in concentrated communities in Yunnan Province. 18
The distribution of vitamin D status varies in different regions according to the duration of sunlight exposure, dietary habit, maternal vitamin D status, and ethnicity. A study conducted in Italy showed that Caucasians had higher median 25(OH)D levels than sub-Saharan Africans (P < .001), North Africans (P < .001), and Indians (P < .001), and for children older than 1 year, they found significant differences in 25(OH)D levels in the different ethnic groups, compared to Caucasians. 19 A study on 218 children aged 6 to 35 months in Jos, Nigeria, showed that no children had a serum 25(OH)D concentration <10 ng/mL (the generally held definition of vitamin D deficiency). 20 In 325 children (white race 95%, boys 56%, mean age 20.7 months), the overall prevalence of vitamin D deficiency was (25(OH)D concentration <20 ng/mL) 22.8% in Western Europe. 21 In Wuxi, China (31°57′ N), a study showed that serum 25(OH)D levels of young children at the age of 1 to 3 years ranged from 20.6 to 132.9 nmol/L (Median: 71.5 nmol/L). Among which 16.1% of the population had vitamin D deficiency (<50 nmol/L), while 38.8% of the subjects had a sufficient (50-74.9 nmol/L) vitamin D level. 22 A study reported the vitamin D status among children in Yunnan Province. It was described that serum 25(OH)D levels ranged from 7.70 to 58.50 ng/mL, with a mean concentration of 26.61 ± 7.26 ng/mL. Sufficient concentrations of 25(OH)D were found in 29.4% of all cases. A total of 125 (70.6%) children presented with low blood levels of 25(OH)D, with 29 (16.4%) children exhibiting 25(OH)D concentration of <20 ng/mL. No significant difference in the 25(OH)D concentration was found between the boys and girls (P > .05). 23 However, this study did not evaluate 25(OH)D concentration in specific regions of Yunnan Province where highly multi-ethnical area and no impact factors on 25(OH)D concentration were studied. In conclusion, this study is the first to report vitamin D status of young children from 4 different ethnical/racial backgrounds in Yunnan Province. Better understanding the ethnic-specific disease prevalence may have substantial value for health care and managements of young children in Yunnan.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Public Health and Disease Prevention and Control of Collaborative Innovation Subproject in Yunnan Province (Grant No.: 2014YNPHXT10) and National Natural Science Foundation of China in 2017 (Grant No.: 81760593).