
Abstract
Background:
Vitamin B12 deficiency in early life can adversely affect the growth of developing brain with myriad of neurodevelopmental manifestations. At this age, the deficiency is usually the result of low maternal levels.
Objectives:
To assess the vitamin B12 status of healthy exclusively breast-fed Indian infants aged 1 to 6 months and their mothers.
Methods:
One hundred term exclusively breast-fed infants aged 1 to 6 months attending pediatric outpatient department were recruited. Hemogram, serum B12, folate, and ferritin levels were obtained from each infant–mother pair.
Results:
The prevalence of B12 deficiency in infants was found to be 57%. Forty-six percent of mothers were deficient. There was a positive correlation (r = .23) between the B12 levels of the infants and their mothers.
Conclusion:
There is a high prevalence of vitamin B12 deficiency in Indian infants and their mothers. There is an urgent need to supplement our population with vitamin B12, and the best time to do this would be antenatal.
Introduction
Vitamin B12 deficiency has severe adverse consequences on the growing brain of the infant. 1,2 The infant may be unwittingly subjected to such harm as a result of low vitamin B12 status of the mother and this in turn is reflective of the widely prevalent vegetarian food habits of our people. 3,4 The nonvegetarians in our country too consume very little of nonvegetarian food per week, not enough to mitigate the effects. 5
The vitamin B12 status of an infant is largely determined by the B12 status of the mother. In an infant born to deficient mother, not only are the blood levels of B12 low, but the liver stores of the vitamin are also inadequate. 6 Further, a cobalamin-deficient mother is likely to produce breast milk having low levels of the vitamin. 7,8 Even though a deficient mother may not exhibit any hematological or neurological symptoms of B12 deficiency for several years, her exclusively breast-fed infant may develop symptoms as early as 3 weeks of age. 9,10 These are often subtle and difficult to detect because of the wide variation in the normal development in this age group. Such infants may have failure to thrive, irritability, apathy, anorexia, refusal to solid feeds, delay and regression of neurological development, hypotonia, seizures, and pancytopenia. 11,12
The disturbed neurodevelopment has a multifactorial etiology and includes delayed myelination. Both adenosylcobalamin and methylcobalamin are cofactors in enzymatic reactions, which impact myelin formation. The decreased S-adenosylmethionine to S-adenosylhomocysteine ratio impairs methylation reactions essential for the synthesis of proteins, lipids, and neurotransmitters in the central nervous system. 13,14
The data on the prevalence of B12 deficiency in the Indian population suggest a high prevalence, and among pregnant and lactating mothers, the figures range from 52% to 74%, which are significant and noteworthy. 3,4,15 There is a paucity of data on the prevalence of cobalamin deficiency in Indian infants and children, and to the best of our knowledge, no data are available for the 1 to 6-month age group. The current study was planned with the aim of assessing the vitamin B12 status of healthy exclusively breast-fed Indian infants of 1 to 6 months of age and their lactating mothers and establishing a correlation, if any. This is of vital importance as detection of asymptomatic deficiency can prevent the devastating consequences that may follow.
Materials and Methods
This cross-sectional study was conducted at a pediatric tertiary care hospital of North India over 2 years. As this institute is in the public domain with no user charges, it caters to mainly low to middle socioeconomic strata of the society with the daily outpatient attendance of around 600 patients.
For this study, term exclusively breast-fed infants aged 1 to 6 months attending pediatric outpatient department for immunization services, mild viral illness, or minor complaints were included. Those with weight less than third percentile for age as per World Health Organization charts, significant medical or surgical history and those who had taken multivitamin supplementation in the past were excluded. Hundred participants were recruited with an equal number below and above 3 months of age. The study protocol was approved by the institutional ethics committee.
After written informed consent from either of the parent of the included participant, a 3-mL venous sample was drawn aseptically for hemogram, serum B12, folate, and ferritin levels. A 3-mL venous sample of the mother was also drawn for the same hematological investigations. The serum B12, folate, and ferritin levels were measured by fully automated analyzer based upon chemiluminescence immunometric assay method.
The normal ranges were defined as: for serum B12—200 to 700 pg/mL, for serum folate—4 to 9 ng/mL, and for serum ferritin—12 to 95 ng/mL. For anemia, the definition was for 1-month age Hb <11.5 g/dL, 2-month age Hb <9.4 g/dL, and for 3 to 6 months of age <11.1 g/dL. For lactating mothers, Hb <12 g/dL was the criteria for anemia.
Data were entered in Microsoft Excel sheets and analyzed using Epi info version 7.1.4. and computed as percentages. Pearson correlation coefficient was used to find correlation between maternal and infant B12 levels.
Results
The sociodemographic profile of the study population is as shown in Table 1. The hematological profile of the infants and their mothers is shown in Table 2. Overall, 69% infants were anemic with the predominant type being normocytic (46%) and others being less frequent (microcytic—36% macrocytic—15%, dimorphic—3%). The prevalence of B12 deficiency was found to be 57% (62% in less than 3 months). Two infants had levels less than 50 pg/mL with the lowest being 6.6 pg/mL (Figure 1).
Demographic Profile of the Study Population.
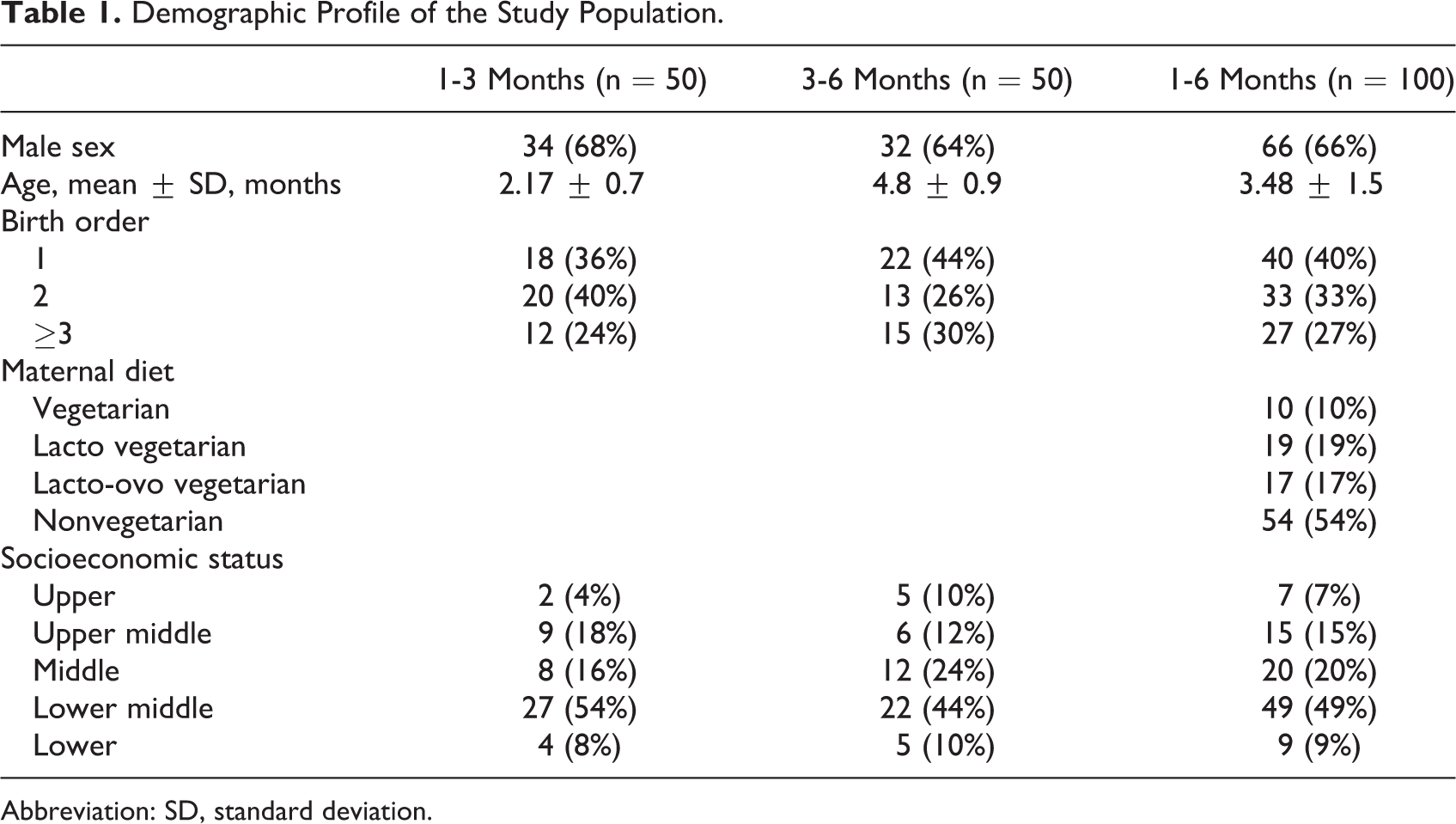
Abbreviation: SD, standard deviation.
Hematological Parameters of the Infants and Their Mothers.a
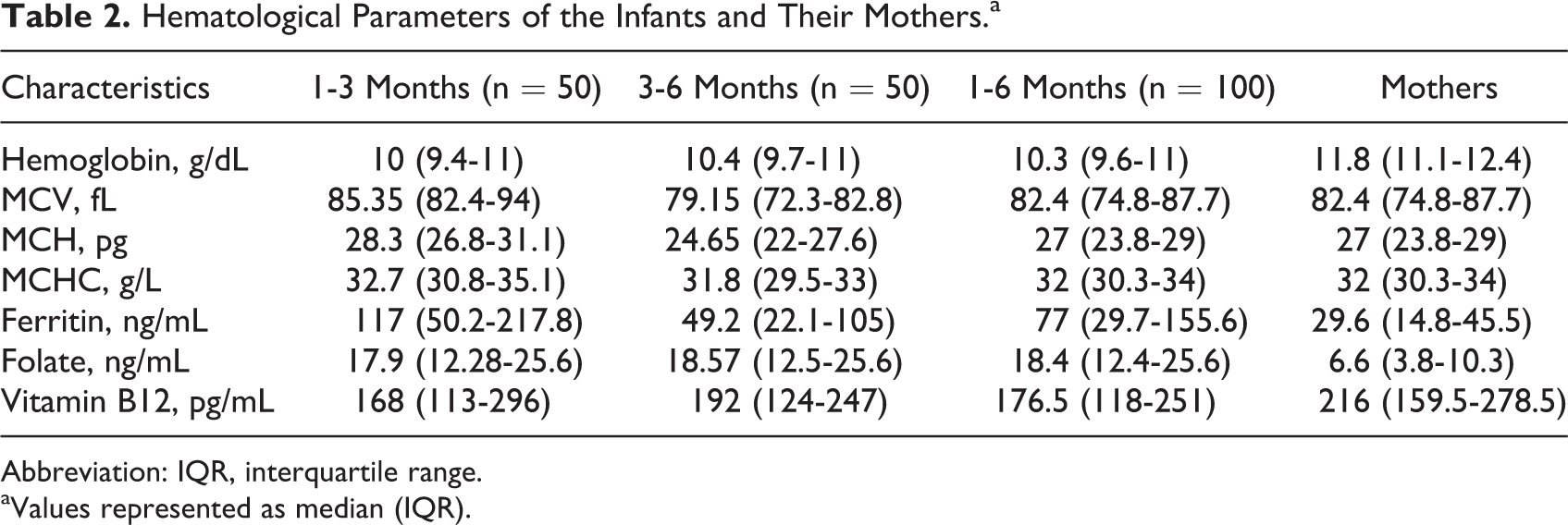
Abbreviation: IQR, interquartile range.
aValues represented as median (IQR).
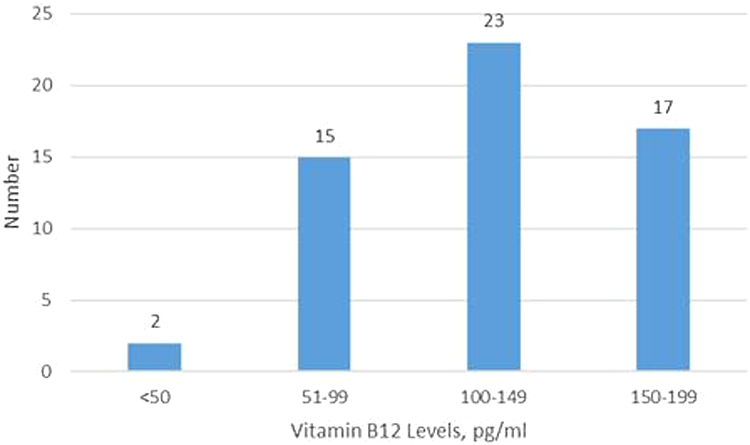
The distribution of vitamin B12 status in the deficient infants.
On univariate analysis, none of the sociodemographic factor was significantly associated with vitamin B12 deficiency (Table 3). Among the infants with multiple birth order, 60% were deficient, whereas among the ones with first birth order, 52.5% were deficient. In infants with mothers who were nonvegetarian, deficiency was found to be 52.1%, whereas those born to vegetarian mothers had prevalence of 68.9%. Those born in lower socioeconomic status families (as per Kuppuswamy scale) were deficient to the extent of 60%, whereas 52.3% of the others were deficient. 16 Though these differences were not statistically significant, they do reflect the effect of birth order, maternal diet, and socioeconomic status on the B12 levels in the infant.
Factors Associated With Vitamin B12 Deficiency in Infants and Mothers.
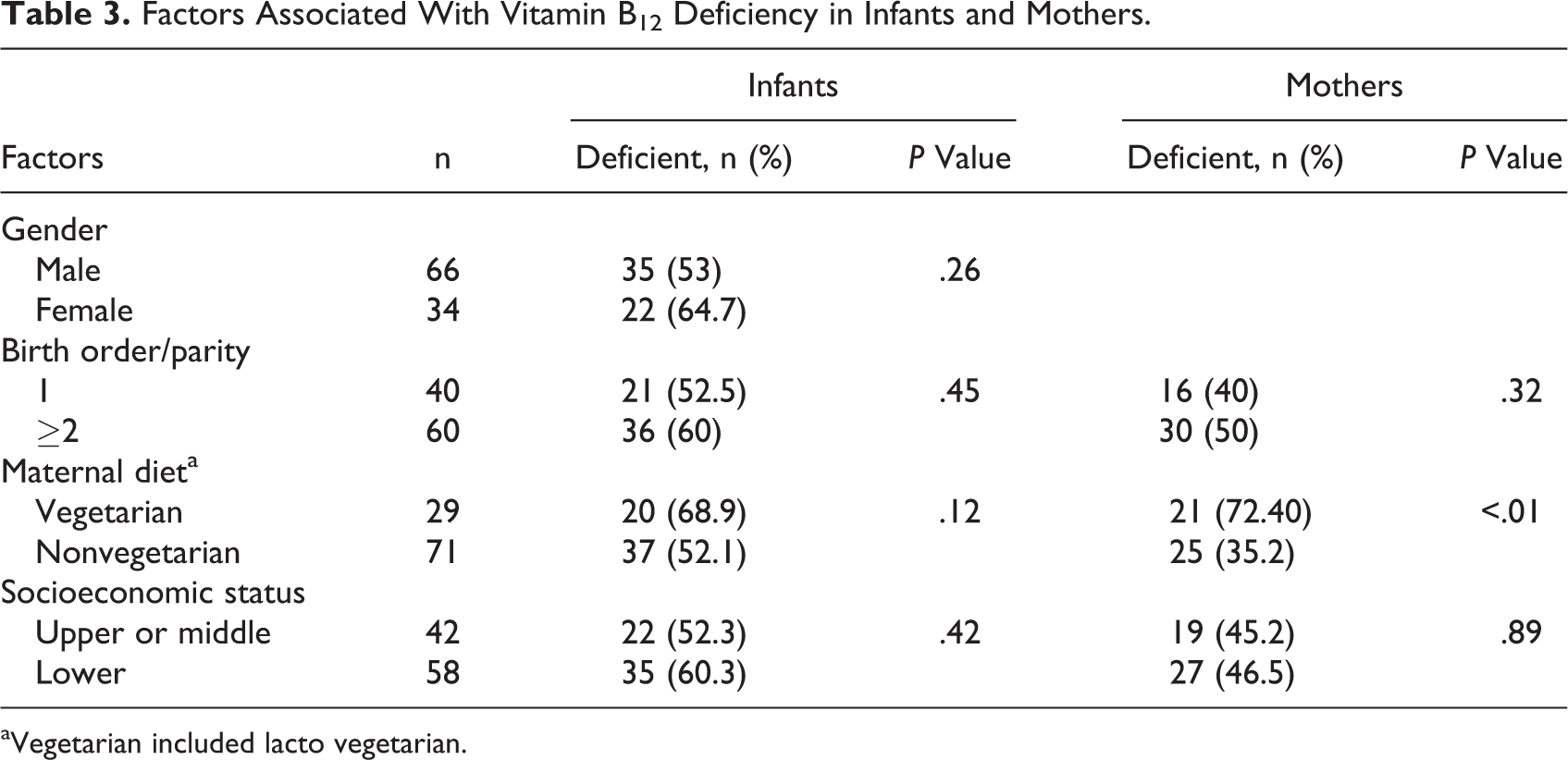
aVegetarian included lacto vegetarian.
In the lactating mothers, anemia was found in 58%, 72% being normocytic, 4% microcytic, 7% macrocytic, and 17% dimorphic. Of the 100 mothers, 46% were deficient in B12 and all were asymptomatic. Of these deficient mothers, 3 had levels less than 100 pg/mL, 20 had levels between 100 and 149 pg/mL, and 23 had levels between 150 and 199 pg/mL. On univariate analysis, maternal diet was the only factor with significant influence on the B12 deficiency (Table 3). Among the nonvegetarian-consuming mothers (n = 71), 35.2% were deficient, whereas 72.4% of the vegetarian ones were deficient.
There was a positive correlation (r = .231, P = .021) between the B12 levels of the infant and the mother with much better correlation in those below 3 months (r = .55 vs r = .14). A scatter plot of infants and maternal levels is shown in Figure 2. There was poor correlation between the age and vitamin B12 levels of infants (r = .165, P = .10).
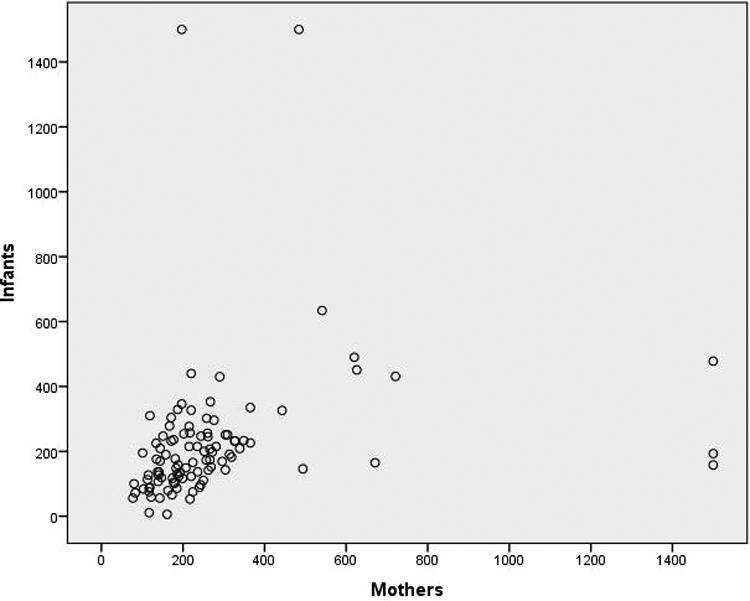
Scatter plot of infants and maternal vitamin B12 levels (pg/mL).
Discussion
Our study has found an alarming rate of vitamin B12 deficiency in young Indian infants (57%) and their mothers (46%). This crucial age group of 1 to 6 months studied has been simply unexplored in the previous studies. Poor cobalamin status of the mothers must have led to low fetal stores and low cobalamin content in their breast milk, thereby impoverishing the infants. It is important to pick up deficiency at this early age, as treating it may prevent the devastating consequences that may manifest later.
Studies from India consistently show that there is high prevalence of vitamin B12 deficiency in our population, though the studies are few in number and many regions are unrepresented. This deficiency spans the life course from pregnant women to children to adults. In a large study from Pune (Pune maternal nutrition study), 71% of pregnant mothers at 28 weeks period of gestation had low vitamin B12 levels. More than 90% mothers had elevated urinary methylmalonic acid (MMA) levels, a functional marker of vitamin B12 deficiency. 17 In a longitudinal study from Mysore, 42% mothers were deficient in vitamin B12 and there was positive association between maternal levels and that of their children sampled at 9.5 years of age. 18 In an interventional study from Bangalore, around 50% pregnant women sampled before 14-week period of gestation were deficient in vitamin B12 deficiency. 19 Pathak et al found 74% of pregnant women deficient in vitamin B12 in a rural area of Haryana (North India), and a similar figure of 52% was reported by Yusufji et al in a previous study from Vellore in South India. 3,4
Among the other studies, in a study from Pune on 224 adult participants, the prevalence of cobalamin deficiency was 47% with 73% having elevated MMA levels. 20 A similar study from the same region showed low vitamin B12 concentration in the 67% of 441 middle-aged men studied. 21
There are 2 population-based studies in children from India. Taneja et al studied B12 levels in a community sample of infants aged 6 to 30 months from New Delhi and found a deficiency prevalence of 28%. A large sample size of 2261 makes their results noteworthy. The deficiency was attributed to prolonged breast-feeding, delayed introduction of complementary feeding, and high rates of gastrointestinal infections interfering with the absorption of the vitamin. 22 The other study is that of Hanumante et al from Pune who studied B12 levels and homocysteine levels in toddlers with mean age of 2.4 years. They found a prevalence level of 14% and attributed it to the impoverished diet of the urban slum population. Their sample size of 51 was, however, small. The homocysteine levels were high, as expected. 23
Studies from many other third-world countries also indicate high prevalence of vitamin B12 deficiency in childhood. In a study from Turkey, 180 pregnant women and their term babies were sampled. Seventy-two percent mothers and 41% babies were deficient. 24 In a large interventional study on micronutrient supplementation in pregnancy from Bangladesh, 31% of 1033 infants sampled at 6 months of age were deficient. 25 Casterline et al in a similar study to ours evaluated the status of vitamin B12 in 113 lactating women and their infants at 3 months of lactation in Guatemala. A total of 33.3% mothers had low plasma B12 levels, and 12.2% infants had elevated urinary MMA levels. 26
The maternal vitamin B12 levels are associated with cord blood/infants levels, and there is much higher prevalence in breast-fed infants as compared to nonbreast-fed infants. Most of case series describing neurological manifestations in infants with vitamin deficiency show these associations. In a longitudinal study from Norway and in the prevalence study from Turkey, there was good correlation between maternal and cord blood levels of vitamin B12. 24,27 In the prevalence study by Taneja et al from Delhi, the median level of cobalamin was much lower in breast-fed children as compared to nonbreast-fed children. 22 In the prevalence study from Bangladesh, 31% breast-fed infants were deficient as compared to 9% nonbreast-fed infants. 25 This difference is due to negligible levels of B12 in breast milk; breast milk contains 0.4 μg/mL of B12, whereas cow milk has 4 μg/mL. 8 In the present study, there was positive correlation between maternal and infant levels. However, as only exclusively breast-fed infants were enrolled, the comparison based on breast-feeding status could not be done.
Low levels of maternal vitamin B12 are linked to a variety of medical conditions in the fetus with long-term effects. Studies have shown an association between high folate to vitamin B12 ratio in pregnancy with small-for-gestational age at birth. 28,29 A meta-analysis has shown an increased risk of fetal neural tube defects in mothers with low vitamin B12 levels. 30 In Pune maternal nutritional status study, low B12 levels in mothers predicted higher insulin resistance in the offsprings at 6 years of age. 17
The present study had a few limitations. It was conducted in patients attending outpatient services of a tertiary care center in a public domain. It is likely that lower sections of the society were overrepresented in this study, and the results may not be fully representative of the population. Urinary MMA, often considered as an important functional marker of B12 deficiency, was not measured in this study.
To conclude, it may be said that there is a high prevalence of B12 deficiency in our infants and their mothers, and there is an urgent need to supplement our population with vitamin B12 and the best time to do this would be antenatal.
Footnotes
Authors’ Note
M.M. and R.J. conceptualized the study. V.B., M.M., and R.J. designed the study. V.B. collected the data. P.K.D. did biochemical tests. M.M. and R.J. did data interpretation. V.B. and M.M. prepared the initial draft of manuscript. M.M., R.J., and P.K.D. revised it for important intellectual contents. All authors did data analysis and approved the final manuscript. The requirements for authorship as stated earlier in this document have been met, and each author believes that the manuscript represents honest work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.