
Abstract
Introduction: Vegetarianism in its various forms has gained global recognition in part because of the notion that it is healthier; however, associations between plant-based diets and selected lifestyle practices in Israel have yet to be clarified. Methods: A population-based sample consisting of 1396 Israeli adults was collected via telephone survey, between the years 2013-2014. Differentiation between self-defined and actual vegetarians was initially verified (based on food intake). Next, “actual” vegetarian status was studied in relation to demographics and health behaviors. Results: Approximately 5% (N = 65) of respondents (5.8% Jews and 3.0% Arabs) were “self-defined” vegetarians; but only about half (N = 33) adhered to genuine vegetarian diets. By contrast, nearly 2% (N = 26) of those self-identified as non-vegetarians were “actual” vegetarians; thus, 4.4% (N = 59) of the sample were verified “vegetarians.” And while socio-demographic features did not meaningfully capture differences by vegetarianism status, “actual” vegetarians were significantly more likely than non-vegetarians to be physically active (OR = 1.7), use nutritive supplements (OR = 2.4) and read food product labels (OR = 1.9; all P < .01). Conclusions: Aggregately, “actual” vegetarian participants were more inclined to have healthier lifestyle practices relative to their non-vegetarian counterparts. Forthcoming research using larger samples should however exploit constant assessment measures to validate the link between vegetarianism and health-promoting correlates.
“The findings strengthen the notion that vegetarians practice healthier lifestyles than non-vegetarians.”
Introduction
Vegetarianism is a broad term that encompasses a diverse array of nutritional practices that each involves, to some extent, the avoidance of meat, poultry, or fish.1,2 Vegetarians may be further sub-classified based on the inclusion of eggs (ovo-vegetarians), dairy (lacto-vegetarians), fish (pesco-vegetarians), poultry (pollo-vegetarians) or a combination of these foods in their diet. In fact, 2 common types of plant-based nutrition include “ovo-lacto-vegetarians” (those that refrain from meat and fish products but include eggs and dairy, and are often referred to as “vegetarians”) and “vegans” (those that refrain from eating any animal products, e.g., meat, fish, dairy and eggs).2,3
The majority of recent studies suggest that vegetarianism in its various forms is increasingly becoming a common dietary preference.4,5 This might be related with the motivations accompanying these diets; 6 for instance, the 2 principal impetuses involved in the adoption and maintenance of plant-based nutrition implicate ethical or moral concerns for animal welfare and environmental destruction associated with meat consumption7,8 as well as concern for improvement of personal health. 9
Further, a growing body of work suggests that plant-based diets (comprised of lower fat and cholesterol intake and higher fruits, vegetables and whole grains consumption) are healthier than those containing animal derived products.10,11 This is especially so, as vegetarians have been shown to have a lower prevalence of chronic disease-related risks (ischemic heart diseases, hypertension, cholesterol problems, type II diabetes and certain cancers) 12 and higher levels of overall health and longevity as compared with otherwise similar non-vegetarians.11,13 And although it is generally accepted that deliberate vegetarian diets are nutritionally adequate some concern remains over the possibility of induced health risks in energy restrictive and monotonous diets; for example, subclinical protein malnutrition and vitamin deficiency.14-16
Still, other researchers have focused on the overall health behaviors of those embracing a vegetarian diet to determine whether the observed advantageous health properties attributed to these individuals are also a by-product of social, demographic or lifestyle determinants commonly observed in health-minded individuals.17,18 These studies have demonstrated that vegetarians were more likely to be female,19-21 of a higher socioeconomic status (e.g., education level),2,3,20-22 with lower BMI 12 and healthier conduct (e.g., smoke less, exercise, and sleep more, adhere to healthy nutrition)2,6,20,23,24 in contrast to their omnivores counterpart.
In so far as estimating the prevalence of vegetarianism among Western nations, rates have ranged between 1 and 10%.3-5,20,21 This pattern of results might in part, be a function of the various methodologies employed in assessing vegetarianism such as: diverse operational definitions of the term and its’ application, as well as differences in sampling methods. For example, 1 notable discrepancy in research methodology pertains to how vegetarian status is determined, for example, by self-proclamation alone or ascertainment of genuine dietary practices (regular consumption or exclusion of animal-based products).
And while according to the Israeli Central Bureau of Statistics (ICBS), during the years 2014-2015, the rate of self-defined vegetarians reached 6.4% 25 these data do not capture the “true” (or actual) prevalence of vegetarianism in Israel, which to the best of our knowledge is presently unknown.
The objectives of the current research were to estimate the nature and prevalence of “actual” vegetarianism in Israel and determine its potential link with health-promoting choices.
Methods
Study Population
A cross-sectional population-based telephone survey was carried out during the years 2013-2014. For purposes of the interview a random sample—with equal and proportional depiction among multiple geographic regions in Israel—was extracted from a computerized list of mobile telephone numbers derived from 6024 Israeli households (2998 Jewish and 3026 Arabs).
Inclusion criteria were households with residents aged 18 years and older, fluent in either Hebrew or Arabic, capable of understanding the content of the survey, and able to provide oral informed consent for participation. Excluded at the initial study phase were participants with telephone numbers that were not relevant for the purpose of the study (disconnected numbers, commercial and business numbers) as well as households that did not meet the aforementioned inclusion criteria (N = 1509). A total of 4515 individuals were contacted of whom 2694 were not accessible (subsequent to 2 additional out-reach attempts) and 425 refused participation. Accordingly, 1396 respondents met fully our inclusion standards (corresponding to a response rate of 30.9%) and were subsequently interviewed.
In accordance with Israeli legislation, the Ministry of Health is authorized to carry out telephone surveys in public health research, for regulatory purposes, as outlined in this manuscript, without the necessity of approval from a Human Research Ethics Committee/Institutional Review Board. 26 Likely related, prior to participation, each respondent provided oral informed consent after a brief explanation of the health survey and its purposes and importance. All data were gathered anonymously.
Instruments and Procedures
The interview was administered via a structured assessment measure, by trained surveyors in Hebrew or Arabic, using computer-assisted telephone interviewing. The questionnaire included 28-items (detailed below) were developed to assess participants’ backgrounds, diets, and health-promoting behaviors. These independent variables were selected based on the premise that they are linked with the vegetarian habit. 6
Background features assessed included sex, age, and years-of-education. Age and years-of-education were divided into categories to minimize the effects of extreme values. Categories were collapsed to stabilize associations when odds ratios did not differ meaningfully. As a result, for age, we used “early to middle-adulthood” (ages 18-49 years) and “middle to late adulthood” (ages 50+) years as it differentiates among the stages of adulthood.
Religious affiliation was determined based on participants’ self-defined classification as being either: secular (not religious at all); traditional (applies some religious rules); religious (applies most religious rules); or devout (adopts extreme religious rules)—religiosity was then grouped into “non-religious” (secular/traditional) vs “religious” (religious/devout) categories.
Body Mass Index (BMI) was also assessed and calculated by dividing the reported weight (in kilograms) by the square of the reported height (in meters) and evaluated as non-obese (less than 30) and obese (30 and above).
Self-perceived physical health (“are you, in general, satisfied with your physical health?”) and life satisfaction (“are you, in general, content with your life?”) were then determined—we note that both items were dichotomized into “satisfactory” (very well/well) vs “non-satisfactory” (not well/poor) groupings.
During the survey participants were also asked about their eating patterns—this was independent of self-proclaimed vegetarian identification. The first set of questions, was devised to assess differences among participants’ in the extent that they refrain from consuming animal-based food products (“do you refrain from eating beef, lamb, chicken, turkey, fish, eggs or dairy products?”).
Following this and consistent with methods previously reported, for example, by Valdes et al 3 those avoiding all animal-based food products (beef, lamb, chicken, turkey, and fish) but reported on no restrictions on eggs or dairy consumption were classified as “vegetarian”; whereas those avoiding all animal-based food products (beef, lamb, chicken, turkey, fish, eggs, and dairy) were classified as “vegan.” Due to the small number of cases within the vegan group (N = 13), these respondents were included within the “vegetarian” category.
All other variations in dietary exclusions that did not align with the above-mentioned vegetarian classification as well as those that did not report on any exclusions at all, were categorized as “non-vegetarian.” We note, that, this classification system, was designed to capture respondents according to their true eating habits (as opposed to self-proclaimed-status alone, see below) and served as the dependent variable for this study.
Succeeding the aforementioned tangible food consumption questions, participants were asked about self-identification concerning their vegetarian status (“do you consider yourself to be a vegetarian?”) for determining their “self-defined” vegetarian status. This was categorized as either “yes” (self-defined vegetarian) or “no” (self-defined non-vegetarian).
Engagement with health-related activities and lifestyle factors were then evaluated. These included assessment of whether the participant currently smokes cigarettes—“yes” (smoker) or “no” (non-smoker); compliance with recommended guidelines for physical activity (engagement in at least 150 minutes per week of moderate intensity activity, 75 minutes per week of vigorous intensity or an equivalent combination)—rated as being physically “active” or “non-active”; and adherence with recommendations for appropriate sleep duration (
Other question items related to nutritive intake. Respondents were asked whether they take nutritional supplements, use food product labels or consume organic foods. These 3 items were dichotomized into “yes” (most often/usually) vs “no” (rarely/never) classifications.
The last segment of the interview included questions that explored attitudes about vegetarianism. Accordingly, respondents were asked if they accept as factual that a diet based on plants promotes one’s health—rated as “yes” “no” or “do not know.” Participants that answered this question positively (yes) were also asked about specific health food beliefs. That is, whether consuming a vegetarian diet is beneficial because it is perceived as (containing at least one of the following properties): (1) less industrial and more natural; (2) enriched in vitamins and minerals; (3) contains more fruits and vegetables; (4) contains less fat, cholesterol, sugar and salt; (5) improves body function, alertness and energy; (6) precludes disease and increases longevity; (7) reduces weight and body fat; (8) prevents killing of animals; (9) contains less hormones, antibiotics and bacteria.
Statistical Analyses
In preliminary considerations for this research, the method used to estimate statistical power was adopted from Rosner 27 we thus relied on our observed crude rates of “actual” vegetarians (4.2%), the sample size (consisting of 1396 participants) and a maximum two-sided Type I error rate of 5%. And aligned with prior research 20 statistical power was computed and estimated at 84%.
At the first stage of analysis, the prevalence of “self-defined” and “actual” vegetarians among the complete sample were estimated and weighted to create alignment with rates of Israel’s general population. For this purpose, “actual” vegetarian status was verified from within the broader self-proclaimed vegetarian category. Those truly adhering to plant-based diets were then studied in unison independent of whether they were self-defined vegetarians or not and these participants are at the forefront of this work.
To study the extent to which the above-depicted independent variables successfully captured potential cases contingency tables were conducted for which “actual” vegetarian status was the primary dependent variable, and background details, health-related behavior and nutrition practices were entered as independent variables. The two-tailed Chi square test (χ2) was the primary technique used to study bivariate associations, generating crude Odds Ratios (ORs) and 95% Confidence Intervals (CIs). At the multivariate level, the significant variables from the above models were studied using logistic regression.
Lastly, graphical depictions concerning attitudes on adherence to plant-based diets by “actual” vegetarian status as well as benefits of vegetarianism were plotted. A P value of .05 was set as the level of significance. All analyses were conducted using SPSS (version 24.0).
Results
Sample Characteristics
The sample was comprised of 1396 participants, 53.4% (N = 745) of whom were male and 55.0% (N = 768) were Jewish. Study participants were between ages 18 to 90 years (mean = 41.9; SD = 15.3 years; median = 39.0). Most participants were younger than 50 years of age (N = 976, 70.0%), had more than 12 years of education (N = 811, 58.6%), self-identified as non-religious (N = 989, 72.9%), and married (N = 985, 70.7%). We note, that the age distribution of the sample, and thus its representativeness, was similar to that of the general population during the study frame.
Verification of Vegetarian Status
As shown in Figure 1, vegetarians are depicted based on self-definition and verified vegetarianism status. Overall, 5.3% (N = 65) of the participants (N = 1396) self-identified as vegetarian (weighted based on the above-mentioned criteria); of whom only 50.8% (N = 33) adhered to a vegetarian diet pattern and were deemed true vegetarians. Flow chart of study population.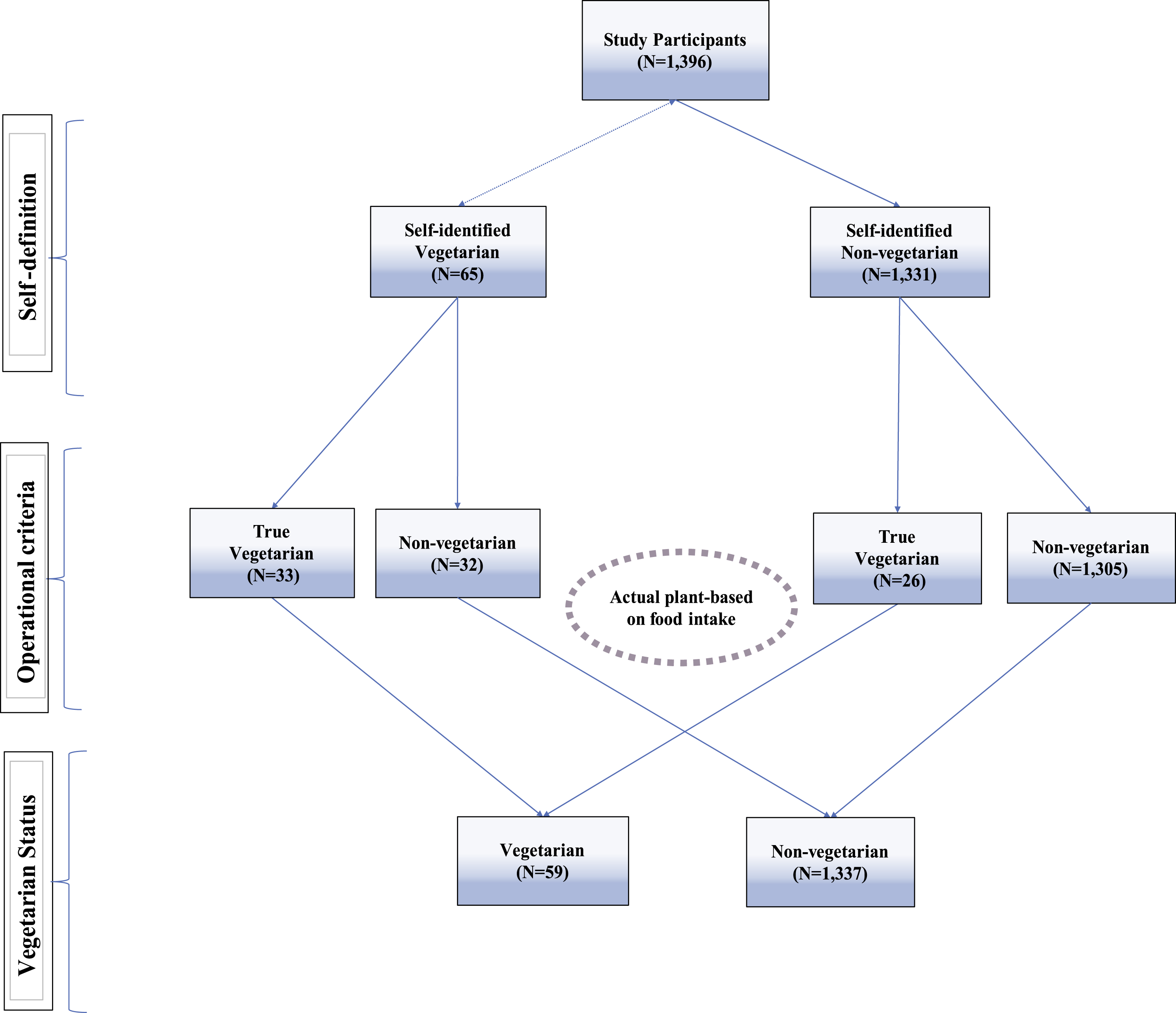
By contrast, of the participants who were self-identified non-vegetarians (N = 1337) as many as 2.0% (N = 26) were reconsidered as true vegetarians based on their actual eating habits. In fact, 4.4% (N = 59) of all respondents were considered: true vegetarians and are referred to throughout as “actual vegetarians.”
We note that in preliminary analyses self-identified non-vegetarians that were reclassified as true vegetarians (based on tangible plant-eating habits) (N = 26) were found to be less educated and more religious than self-defined authentic vegetarians (N = 33). Inversely related, participants erroneously self-regarded as “vegetarian” (N = 32) were more similar to the general population of non-vegetarians (N = 1305) than to actual plant-eaters as per health-related indices. Thereby supporting the use of operational criteria for purposes of vegetarian groupings (results available upon request).
Determinants of Vegetarian Status
Univariable Associations of Background Features and Health-Related Exposures Among the Study Population by Actual Vegetarian Status.
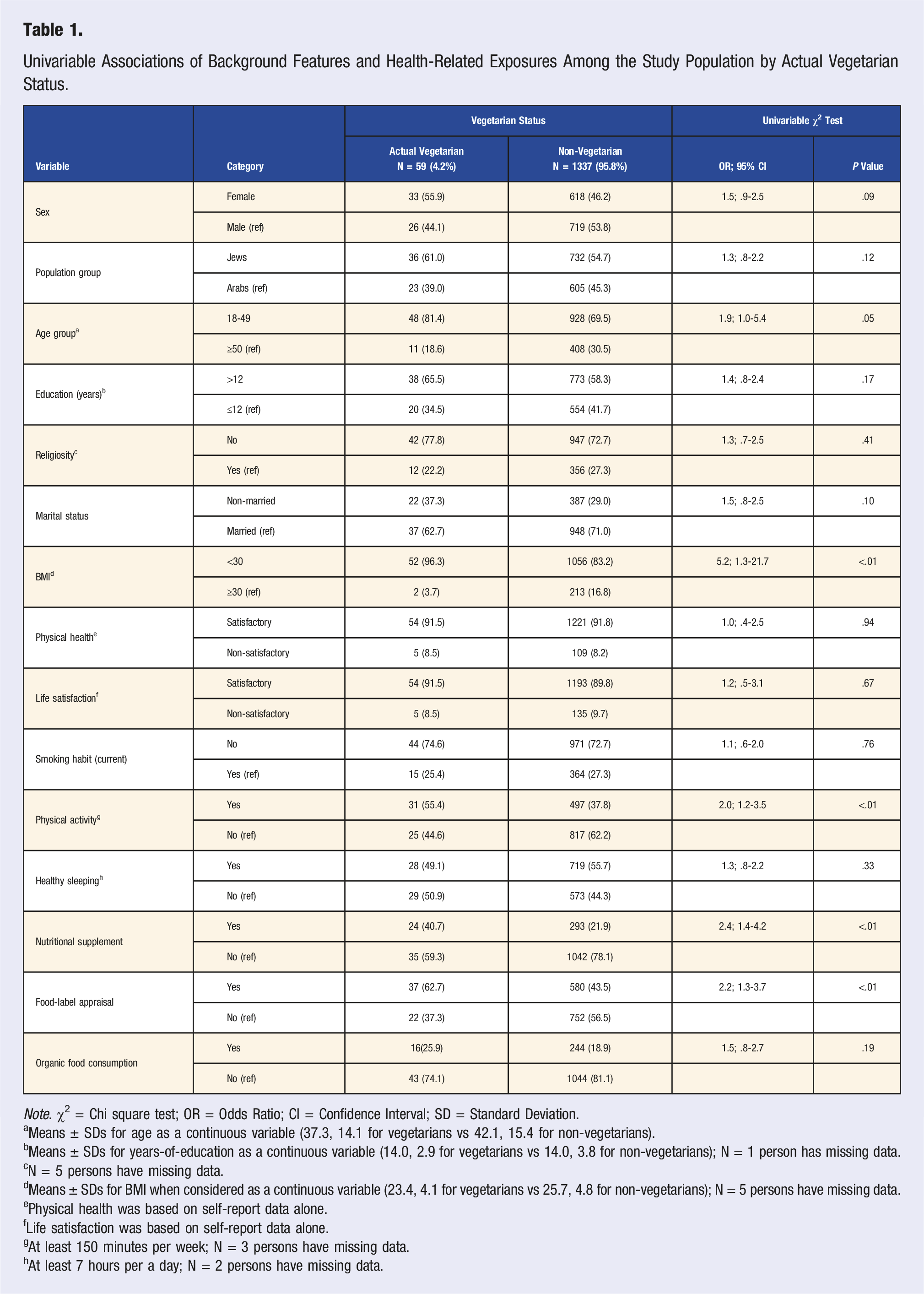
Note. χ2 = Chi square test; OR = Odds Ratio; CI = Confidence Interval; SD = Standard Deviation.
aMeans ± SDs for age as a continuous variable (37.3, 14.1 for vegetarians vs 42.1, 15.4 for non-vegetarians).
bMeans ± SDs for years-of-education as a continuous variable (14.0, 2.9 for vegetarians vs 14.0, 3.8 for non-vegetarians); N = 1 person has missing data.
cN = 5 persons have missing data.
dMeans ± SDs for BMI when considered as a continuous variable (23.4, 4.1 for vegetarians vs 25.7, 4.8 for non-vegetarians); N = 5 persons have missing data.
ePhysical health was based on self-report data alone.
fLife satisfaction was based on self-report data alone.
gAt least 150 minutes per week; N = 3 persons have missing data.
hAt least 7 hours per a day; N = 2 persons have missing data.
We note that in supplementary analyses when age group, BMI, and years-of-education were studied as continuous variables in relation to vegetarian status a similar pattern of results emerged to those reported here (results are available upon request).
Multivariable Associations of Background Features and Health-Related Exposures Among the Study Population by “Actual” Vegetarian Status.
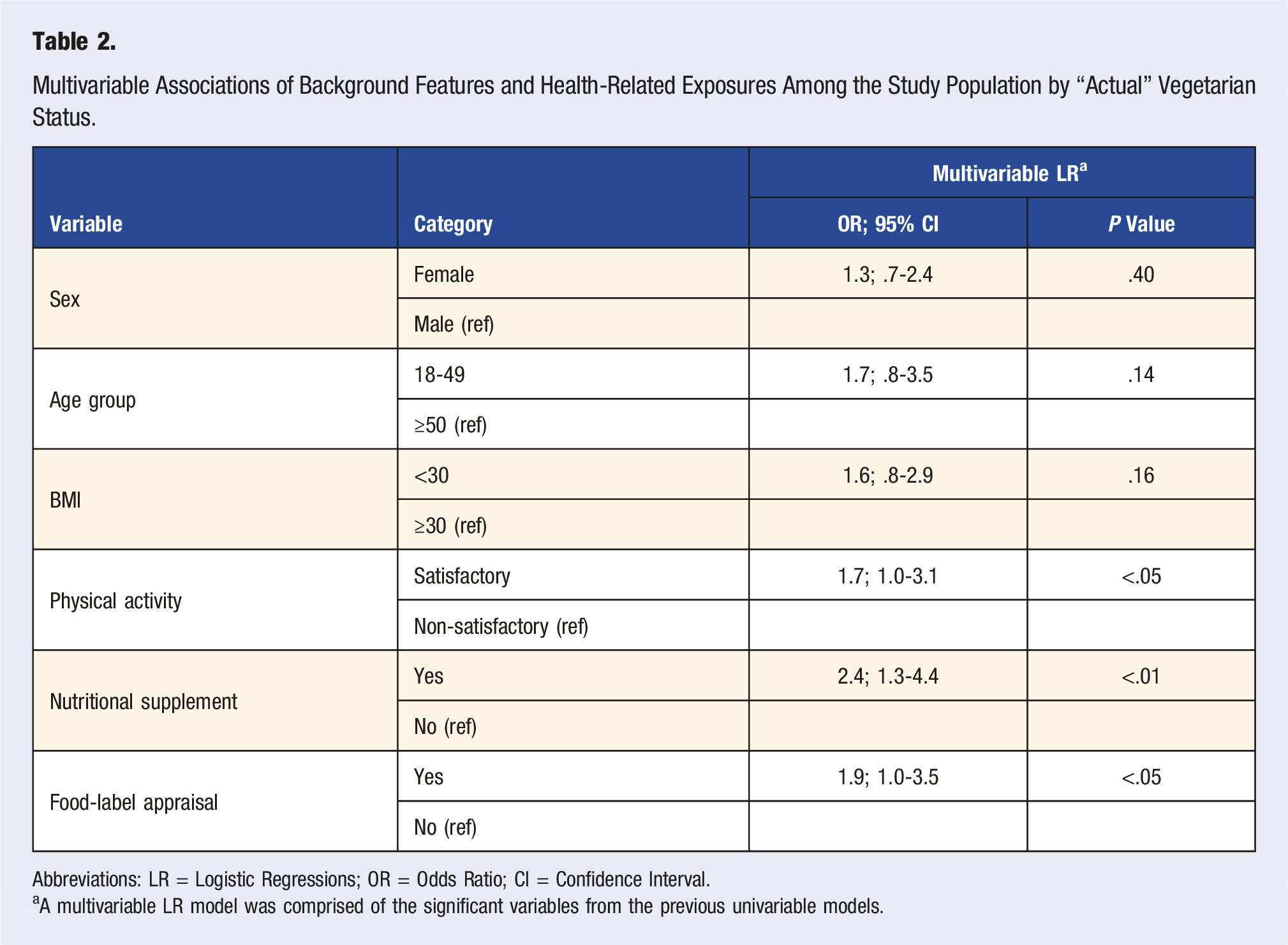
Abbreviations: LR = Logistic Regressions; OR = Odds Ratio; CI = Confidence Interval.
aA multivariable LR model was comprised of the significant variables from the previous univariable models.
Reasons for Vegetarian Lifestyle
Nearly half (49.1%) of the study sample reported positive stances concerning the health profits of plant-based diets. In fact, as illustrated in Figure 2, though these rates were higher for “actual” vegetarians as compared with non-vegetarians (62.7% vs 48.5%, respectively) these associations were not significant (P > .05). Level of agreeability toward perceived health benefits of plant-based diets according to vegetarian status. Note. These items were rated on a categorical scale whereby the level of agreement with the health benefits consequent to vegetarianism correspond to “yes”, “no”, or “do not know” responses.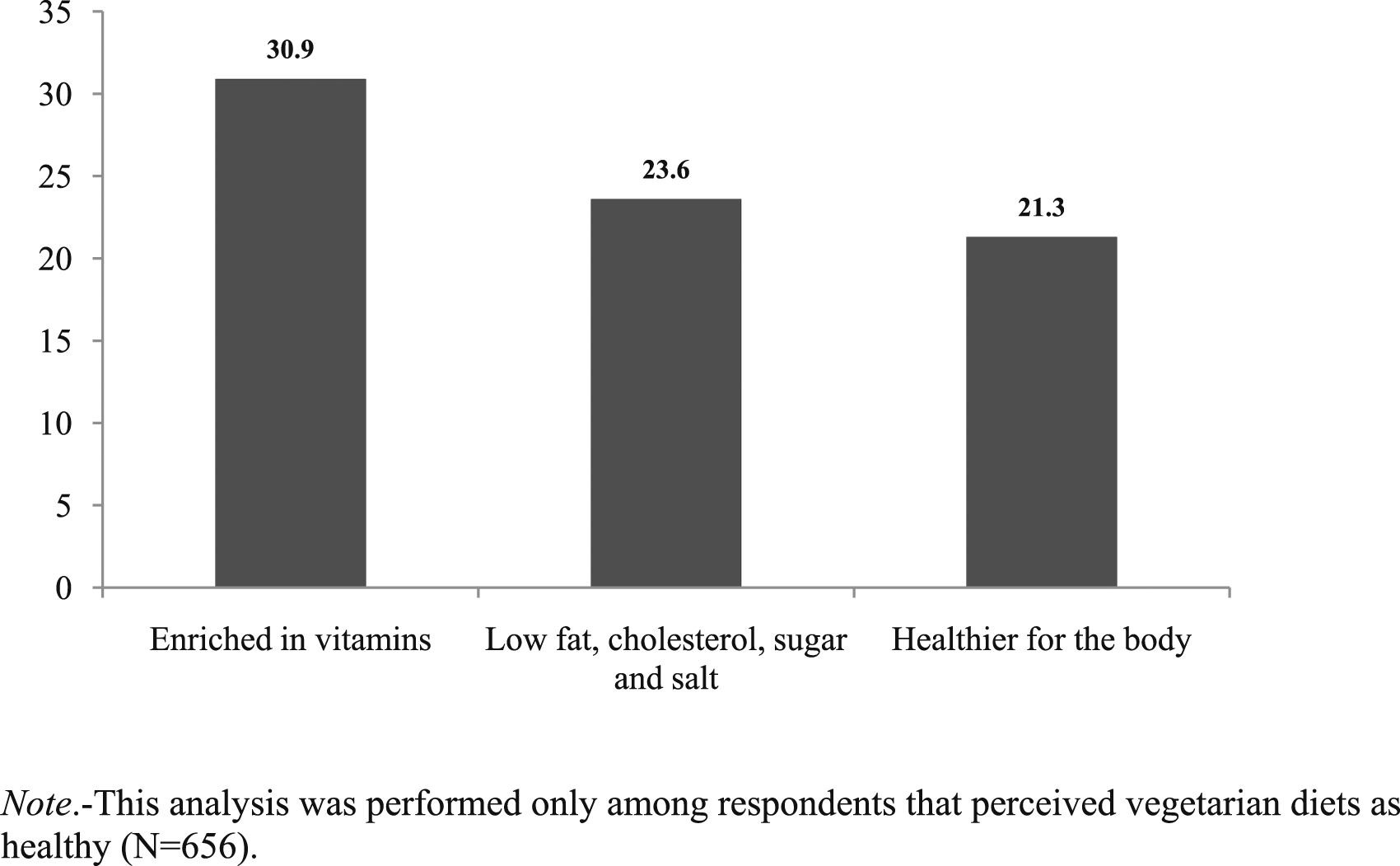
Figure 3, demonstrates that independent of “actual” vegetarian status of those that perceived vegetarianism as a healthier choice (N = 656) reported that the primary health benefits attributed to vegetarianism corresponds (in descending order) to such health benefits as: diets rich in vitamins and minerals (30%); low in fat, cholesterol, sugar and salt (24%); and overall healthier for the body (21%). The leading reported advantages of plant-based diets among the study population. Note. -These items were rated on a categorical scale whereby the level of agreement with the health benefits consequent to vegetarianism correspond to “yes”, “no”, or “do not know” responses.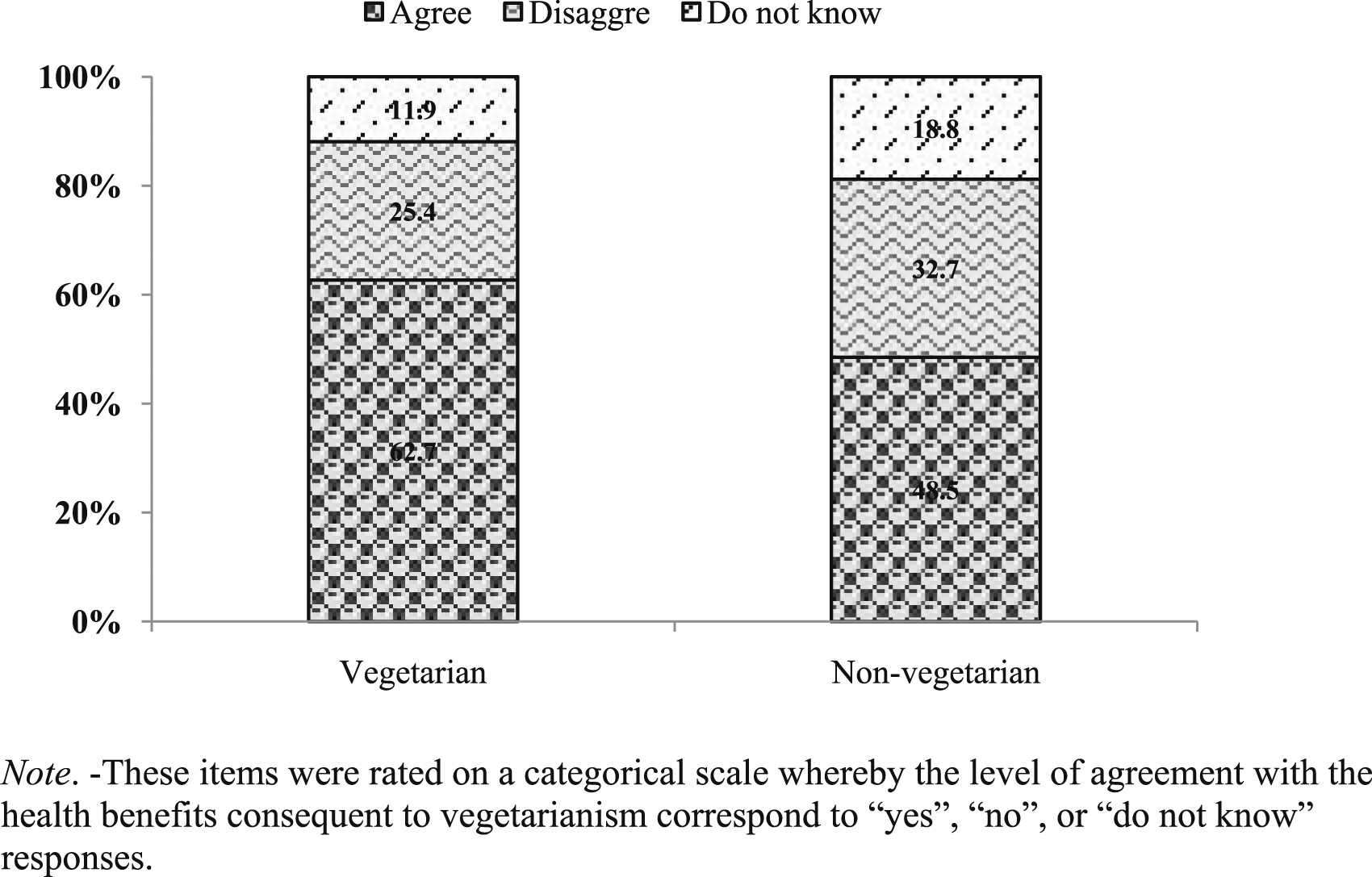
Discussion
Main Findings
This study provides data on the rates of “self-defined” and “actual” vegetarians among a representative sample of Israel’s general population and further supports the notion that vegetarians have healthier lifestyle practices as compared with their non-vegetarian counterparts. 28 Besides which, the prevalence of “self-defined” and “actual” vegetarians in Israel reached 5.3% and 4.4%, respectively, which would be positioned toward the center of the continuum of rates reported in other nations (ranging between 1 and 10%); for example, 2.4 to ∼10% in the United States,21,29 4.3% in Germany, 2 1.6% to 6.2% in Canada,3,21 and 2.8% in New Zealand. 20
Data also show, that the prevalence of “actual” vegetarians was slightly lower when compared with rates of “self-defined” vegetarians both in our study and also when contrasted with ICBS data which evaluated the prevalence of self-defined vegetarian status alone (6.4%). 25 Similarly, this pattern of results was also identified in Canada; whereby the prevalence of vegetarianism was lower when evaluating “actual” vegetarians as compared with “self-perceived” vegetarians alone (those rates were 1.6% and 6.2%, respectively).3,21
Moreover, accumulating evidence24,30 suggests that some self-identifying vegetarians do not strictly adhere to operational definitions of vegetarian diets (e.g., complete exclusion of certain types of animal products such as meat or fish) and their vegetarian status might therefore, not be valid. Such discrepancies can lead to an over-, or under-estimation of the prevalence of vegetarianism. As a matter of fact, were we to have used self-report criteria, instead of actual food intake to verify vegetarian status nearly half of those considered “actual” vegetarians would have erroneously been studied as non-vegetarians (as they were self-proclaimed non-vegetarians) as would approximately half of the self-defined vegetarians, since they did not maintain plant-based diets.
In this regard, directing attention towards potential reasons for the misalignment between self-perceived vs actual vegetarianism could help form a broader rubric to determine true rates.
These include such factors as: (1) the awareness gap between an individuals’ self-perception of their dietary choices (knowledge) and their actual dietary behavior (engagement); (2) motivations and intentions behind self-identifying as vegetarian (ethical concerns, health motivations, or environmental beliefs); (3) social or cultural expectations which may influence individuals to identify as vegetarian, even if their dietary habits do not align; (4) methodological limitations associated with ascertaining diets (reliance on self-reported data, recall bias). To this end, employing a comprehensive questionnaire that addresses these issues would allow for a more accurate estimation of the prevalence of vegetarian forms of nutrition. 20
Even though socio-demographic indices did not meaningfully distinguish across “actual” vegetarian status—possibly owing to power limitations and thus preclude firm conclusion—trend-level distinctions were however identified. For instance, “actual” vegetarians had a propensity toward being younger, female, Jewish (the majority population group), more educated, and non-married as compared with non-vegetarian references. It could then be that pending replication in future work using larger samples these descriptive features might constitute a preliminary depiction of a “vegetarian profile.”
As well, aligned with prior research8,31 indication of higher levels of engagement with health behaviors was provided by our findings as “actual” vegetarians were significantly more likely to be: non-obese (as evidenced by lower BMIs), more physically active and minded to aspects of sustenance (frequent use of nutrient supplements and food product labeling) than their omnivore non-vegetarian counterparts. So emphasizing, that along with diet other health determinants also seem to be associated with the vegetarian lifestyle and that these might also contribute to enhanced health and well-being.
Further sanctioning these suppositions is that the vast majority of “actual” vegetarians and nearly half of the non-vegetarian participants expressed favorable opinions concerning health benefits associated with vegetarianism. Specifically, among those perceiving vegetarianism as advantageous, the principal reasons for adhering to vegetarian diets were without exceptions all health-related (e.g., diets fortified with vitamins, low in fat and healthier for the body). These findings support the notion that it is becoming more common to consider the associated health gains of a vegetarian lifestyle prior to making the actual choice of adopting a plant-based diet per se. 32
Implications for Research and Practice
The findings presented in this research add to our understanding of the dietary practices and health beliefs associated with plant-based nutrition. Yet, several aspects of our results warrant additional consideration, one of which is sample size. Indeed, we did not have a large enough sample of vegetarians to examine specific subgroups independently. As a matter of fact, were we not to have adopted austere criteria in sample recruitment, excluding fish consumption from the vegetarian group, the prevalence of vegetarians in our study would have reached 9.7% rather than 4.4%.
Certainly, as the aforementioned idea that self-perception of vegetarianism can be ambiguous and lead to incongruity concerning the true rates of vegetarianism, implications for research, public health interventions, and dietary counseling are inevitable.33,34 As an example, it might be revealing to collect data at several stages of follow up to allow for comparisons on the diversity of vegetarian diets and how they might fluctuate over time. If this methodology were to incorporate partial- vs full-time use or complete meat abstinence vs vegetarian-inclined diets, it would offer a more sensitive appraisal of individual dietary practices and lead to better estimates of genuine vegetarian rates. Especially so if accounting for cultural variances within and across nations and intra-personal differences as well.
Likewise, as “actual” vegetarians were more inclined than non-vegetarians to sustain the dietary demands of healthy eating, nutrition that is essentially plant-based might enhance the Israeli food pattern for better prevention and condition management of food related diseases. However, to exploit fully these diets research is needed to examine the efficacy and safety of integrating nutrition into local health care delivery. And as alluded above, it is difficult to extricate the effects of other health behaviors aside from plant-based nutrition that contribute to improved health and since differences in lifestyle behaviors were only partially assessed in this study, forthcoming research is needed to decipher the true differences observed in health conditions by vegetarian status. This could be done using matched samples 19 —whereby “actual” vegetarian and non-vegetarian participants are similar with regards to a wide range of physical, lifestyle and social factors.
Strengths and Limitations
The credibility of our results should also be viewed in relation to the following strengths and limitations. First, we acknowledge that while the data presented has aged, and can therefore, introduce inherent limitations concerning its applicability, it is not antiquated as per its accuracy or relevance. In fact, using the current study can help contextualize vegetarianism in Israel and provide deeper insights into vegetarian trends and unique lifestyle patterns (dietary preferences and health behaviors) and serve as (baseline data) or a reference point for forthcoming research.
Second, as we did not use a standard validated food frequency questionnaire the findings might not be comparable to those of studies that did use such instruments. And while previously collected ICBS data reported similar rates of non-verified vegetarians to those reported here, forthcoming studies on both local-, and national-levels are needed to replicate and validate these results using similar study procedures.
Third, the cross-sectional design of this research did not allow for the investigation of temporal relationships; as a result, it could not be determined if and to what extent the decision to become vegetarian took place before or after certain health-related behaviors. Yet, the purpose of this investigation was to estimate the scale of vegetarianism and identify potential associations between “actual” vegetarian status and healthier living and not for establishing causality.
Fourth, we acknowledge that even if selection bias concerning sample recruitment might have restricted the validity of our findings, because this study was a nationally representative sample inclusive of both Jews and Arabs (the major population groups in Israel), this limit was perhaps minimized. Reliance on authentic food-based criteria vs self-definition may have also served to bypass misallocation of vegetarian participants.
Fifth, the data did not permit consideration of more specified diet groups, such as meat vs fish consumers or vegans separate from vegetarians. Besides, stratifying the sample by sex and age or studying multiple categories separately (e.g., well-defined age groups) rather than in binary groups was not possible because of power issues. Reinforcing the importance of using larger samples to repeat this work among pre-specified sub-populations.
Conclusions
This study provides new data on the prevalence of vegetarianism and health-related correlates using a nationally representative population-based sample. As disparities were found between “self-defined” and “actual” vegetarianism, formulating a consistent portrayal of dietary patterns, is advised. By and large, the findings strengthen the notion that vegetarians practice healthier lifestyles than non-vegetarians; however, additional research is needed to corroborate these findings and broaden our understanding of the inter-dependence between plant-based nutrition, lifestyle choices and positive health outcomes in order to discern the true profit of health-promoting behaviors.
Footnotes
Author Contribution
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.