
Abstract
Background:
Assessing whether and how the expenditure of emergency cash transfer programs (CTPs) relates to child nutritional status is a necessary step for informed program design and targeting.
Objective:
We hypothesized that greater child food expenditures would have a protective effect against the risk of acute malnutrition in the context of a food crisis in Niger.
Methods:
We investigated the relationship between food and medical expenditures and acute malnutrition in children aged 6 to 36 months through an observational cohort study of 420 households enrolled in an emergency CTP in Niger. A Cox proportional hazards model was used to estimate the risk of acute malnutrition while adjusting for relevant child and household characteristics.
Results:
Seventy-four (18% of the cohort) children developed acute malnutrition. The risk was 1.79 times higher among ill children than healthy children (hazard ratio [HR]: 1.79; 95% confidence interval [CI]: 1.10-2.92; P < .05), nearly 3 times higher among children in the poorest households than those in wealthier households (HR: 2.98; 95% CI: 1.86-4.78; P < .001), and 2.85 times lower with each unit increase in baseline weight-for-height Z score (HR: 0.35; 95% CI: 0.23-0.53; P < .001). Food expenditures were not associated with risk (HR: 0.97; 95% CI: 0.87-1.07; P > .05).
Conclusion:
Our findings highlight the importance of the health-related determinants of child undernutrition and suggest that a potential role of emergency CTPs may be to enable and promote health service access where services exist. They also indicate a need for more sustained poverty reduction and undernutrition prevention activities in concert with well-timed and strategic use of emergency interventions.
Introduction
Despite a renewed global focus on improving child health and nutrition, acute malnutrition affects at least 52 million children annually. 1 It impairs immune function, reduces appetite, increases metabolic rate and nutrient needs, and heightens vulnerability to infection and disease. 2 Children with moderate or severe acute malnutrition have 2- to 9-fold greater odds of dying from pneumonia, diarrhea, or malaria than children without acute malnutrition; ultimately, wasting is responsible for 875 000 child deaths each year. 1,3
The immediate, underlying, and basic causes of acute malnutrition in children are presented in the United Nations Children’s Emergency Fund (UNICEF) framework for child undernutrition. 3 Restricted dietary intake, due to either food access or poor appetite during illness and/or illness alone can result in rapid weight loss in young children. Thus, children in food-insecure households, those with limited or no access to clean water and sanitation, and those whose care and feeding is suboptimal encounter acute malnutrition risk factors. More distally, poverty and the absence of a functional medical infrastructure are widely accepted as basic causes. 4
Nutrition-specific and nutrition-sensitive interventions address the immediate and underlying causes of acute malnutrition, respectively. 5 Cash transfer programs (CTPs), in which cash is distributed to vulnerable households, are an example of the latter. The CTP theory suggests that CTP income increases household purchasing power, which, when paired with conditional terms requiring engagement with public health and social services, results in effective poverty alleviation and positive impacts on child health and nutrition outcomes. 6,7
The relationship between emergency CTPs, expenditures on child food and health, and influences on acute malnutrition has been investigated to varying degrees in a small number of recent studies. Fenn et al documented increases in household- and child-level food, medical, and miscellaneous expenditures, as well as improvements in dietary diversity and food security, in their pre–post study of emergency CTP beneficiaries in Maradi, Niger. 8 Also in Maradi, Langendorf et al compared the effects of different combinations of cash and supplementary food to at-risk children aged 6 to 23 months and found that the combination of the 2 intervention types reduced the incidence of moderate acute malnutrition by half relative to the provision of food or cash alone. 9 In qualitative follow-up interviews, cash beneficiaries reported spending approximately 20% of the transfers on nutritious foods for the child, regardless of whether or not they also received supplementary food.
In contrast, Hoddinott et al investigated 2 different intervention modalities, conditional cash-for-work transfers and in-kind food baskets, to assess the effect of each on household food security, diet, and coping strategies in the Zinder region of Niger. 10 They found that households receiving cash spent a large portion (38%) of monthly transfers on bulk grain purchases and were 30% more likely than in-kind households to do so in the lean season. Bulk grain purchases were considered a strategy to take advantage of seasonally low food prices. No measures of child diet or acute malnutrition were reported, so the influence of food expenditures on child outcomes was unknown. However, relative to in-kind recipients, cash households showed little improvement in any measured indicators of household-level diet quality or food security. In summary, although the use of cash programs in emergency settings is widespread, quality evidence concerning their relationship with child nutrition outcomes is limited and often conflicting.
Despite the absence of rigorous study, the assumption that increased expenditures on child food are protective against the risk of acute malnutrition underlies the majority of work done to evaluate emergency CTPs. 11 We sought to examine this relationship by identifying risk factors for acute malnutrition among a cohort of emergency CTP beneficiaries in Maradi, Niger (the same study population described by Fenn et al previously). We hypothesized that greater expenditures on child food would be associated with lower risk of acute malnutrition. We were also able to estimate the risk associated with other known child and household characteristics as described earlier. We did not estimate CTP impact, nor do we comment on the presence or absence of risk factors among beneficiaries relative to nonbeneficiaries.
Methods
Setting
Niger’s population of 16 million is largely reliant on rain-fed agriculture and experiences extreme food insecurity on an annual basis. Most rural households in the study region of Maradi are supported through a combination of subsistence farming, unskilled manual labor, livestock husbandry, and the selling of commodity items such as firewood, charcoal, or small goods. The prevalence of stunting and wasting among children under 5 years of age in Maradi are 54% and 19%, respectively; this is higher than the national rates (44% and 18%). 12 At 166 deaths per 1000 live births, child mortality in Maradi is lower than the national rate of 198 deaths per 1000 live births. 12 Acute malnutrition is most prevalent during an annual period of food insecurity, the rainy “lean season,” between June and October.
Intervention
In May 2012, Save the Children (hereafter “SC”) implemented a 6-month unconditional, emergency CTP in the Maradi region of Niger in response to the Government of Niger’s declaration of an impending food crisis. Program objectives were to improve household food security, prevent the sale of household assets, and reduce the incidence of child wasting. Eligible households were those classified as either “poor” or “poorest” according to the Household Economy Approach (HEA). 13 The HEA defines wealth groups according to locally defined thresholds of land and livestock ownership and household size. In the study context, the “poorest” households had approximately 7 household members and owned <1 hectare of land, no cattle, and no more than 2 goats and 4 hens. “Poor” households, in contrast, had approximately 8 household members and owned approximately 1.5 hectares of land, no cattle, and no more than 3 goats and 8 hens. 14
A total of 2736 households in 21 villages were enrolled in the program; each household received 1 transfer per month from April to September 2012 for a total of 6 transfers. Save the Children staff dispensed the transfers to female heads of households at public distribution sites. The transfer amount for each household started at 20 000 West African Francs (CFA) for each of the first 2 months of the program and 30 000 CFA for each of the subsequent 4 months, for a total value of 160 000 CFA (US$ 296 using July 2012 exchange rates. The total was equivalent to approximately 34% of the gross national income (GNI) per capita, based on purchasing power parity (PPP) in Niger in 2012 (420, 270 CFA, or US$ 870). 15 No stipulations or restrictions were given regarding how the CTP funds could be spent.
Educational sessions did not accompany the intervention. All participants had access to the same medical and nutritional services that existed prior to the study, which would have included supplementary and therapeutic feeding programs for qualifying individuals. Such programs are integrated into routine Ministry of Health services.
Study Design and Eligibility
The Emergency Nutrition Network (ENN), a UK-based research and knowledge management humanitarian organization, collaborated with SC to design and implement a 6-month longitudinal cohort study of children in SC CTP beneficiary households. Four hundred fifty-three households were randomly selected from the SC list of CTP beneficiaries, and 1 child per household was selected as the target child for the study. Children were eligible for the study if they were aged 6 to 36 months and did not have acute malnutrition, defined as a weight-for-height Z-score (WHZ) <−2 using the World Health Organization (WHO) standards for child growth, 16 a mid-upper arm circumference (MUAC) <125 mm, or edema, in April 2012. Eligibility did not discount participation in other health or livelihood programs. In households with more than 1 eligible child, all eligible children’s names were written on folded pieces of paper and one was randomly selected as the target child.
Data Collection
Data on child diet, health and anthropometric status, and household expenditures were collected at the homes of study participants for 6 consecutive months, from April (baseline) to September (endline) 2012. Data on household composition, education, income, and assets were collected only at baseline and endline. One-time qualitative interviews with 34 female beneficiaries, 17 with an acutely malnourished child and 17 with a nonacutely malnourished child, were conducted and recorded to collect data on program delivery and uptake.
Any target child diagnosed with acute malnutrition (a “case”) at any survey round was referred to treatment services. Their household remained a beneficiary of the CTP, but no further data were collected from the target child or the household until the endline survey.
All data were collected in the Hausa language in the week prior to the cash transfer distributions by 10 teams of 3 enumerators each (1 team leader and 2 individuals to measure and record data). Enumerators were identified based on the previous experience conducting surveys with SC in Niger, selected through interviews and references, and trained during a 1-week course followed by 3 days of field piloting.
Model Variables and Measurement
Child anthropometric measurements were made using standard techniques, applying Standardized Monitoring and Assessment of Relief and Transitions (SMART) guidelines. 17 The Emergency Nutrition Assessment (ENA) software was used to test both inter- and intrameasurer reliability during training and refresher training. 18 Weight was recorded to a precision of 0.1 kg using an electronic baby/toddler scale (Tanita BD-590, Middlesex, UK). Length of <87 cm was measured to a precision of 1 mm using a baby mat (SECA S210, United Kingdom); height of children ≥87 cm was measured using a plastic stadiometer (Leicester, Child Growth Foundation, United Kingdom). A tape was used to measure MUAC on the left arm to a precision of 0.1 cm. The presence of bilateral pitting edema was recorded. Moyo (note 1) weight-for-height charts were used to assess and interpret a child’s weight-for-height according to the 2006 WHO growth standards. 16 Age was determined by asking to see a birth certificate or by asking the mother directly, or, if not known, it was estimated using a local events calendar. Exact dates of birth were known for 281 (62%) children in the study.
Child dietary diversity was assessed by summing the total number of WHO food groups (grains/tubers, fruits and vegetables rich in vitamin A, legumes/nuts, animal flesh foods, eggs, dairy, and other fruits/vegetables) consumed on the day preceding each survey. 19 Child meal frequency was the number of snacks or meals fed to the child on the previous day. Breast-feeding status was assessed by asking whether the child had received breast milk in the preceding day (0, no breast milk fed; 1, breast milk was fed). Current consumption of supplementary or therapeutic foods by the target child was also documented and used to assess participation in the nutritional rehabilitation programs (0, no supplement; 1, received supplement).
Child illness was defined as the occurrence of any of the following 5 symptoms or diseases within the previous 2 weeks as observed by the mother: diarrhea, cough, fever, malaria, or measles (0, healthy; 1, recently ill). Maternal mental health was assessed using the self-reporting questionnaire, which scores mental health from 0 to 19, where 0 is no symptoms and 19 is all elicited symptoms of poor mental health. 20
Expenditures on food, medical, or other expenses were recalled by participants for the previous 1 week and are expressed in units of 100 CFA (approximately 19 cents using July 2012 exchange rates). Estimates were for expenditures related to the target child only. “Other” expenses included the cost of materials such as clothing, cloth, soap, or any nonfood, nonmedical expense incurred for the target child.
All household-level variables were assessed at baseline and treated as time invariant. Household size was the number of family members living in the household. Education referred to the presence of any individual in the household with formal (primary or secondary) education (0, no formal education; 1, formal education). Participants estimated the time to the nearest health facility in minutes. Discrete categories of time to health facilities did not appear in the data, so the variable was left continuous and log-transformed for modeling. Protected water sources were covered wells or pumps, whereas unprotected sources were open wells or bodies of water (0, protected; 1, unprotected). Household food insecurity was assessed using a shortened validated version of the Household Food Insecurity Access Scale. 21 The scale was dichotomized for analysis (0, no indicators of household food insecurity; 1, at least 1 indicator of food insecurity). We categorized household wealth using the HEA system as described earlier (0, “poor”; 1, “poorest”).
Ethical Approval of Studies and Informed Consent
Study participants gave verbal and written informed consent at each month of data collection and were free to leave the study at any point. Study procedures were in accordance with SC’s routine program monitoring and evaluation protocols. Any target child found to have acute malnutrition was referred to treatment and removed from the study; the household remained a beneficiary of the CTP. This study was approved by the Niger Ministry of Health.
Statistical Methods
Data were double entered into EpiInfo version 7 22 by 2 data entry clerks on the day after data collection and analyzed using the STATA statistical software package version 12. 23 Anthropometric indicators of the attained growth standards were calculated using the WHO macro for STATA. 24 A quality check of the anthropometric data using the ENA plausibility software declared the data to be of “good” quality. 18
We used a continuous time Cox proportional hazards model to estimate the risk of acute malnutrition based on fixed and time-variant variables, using month as the underlying time variable. Cox proportional hazards models estimate the effect of covariates on the likelihood of an event (becoming acutely malnourished in this case) relative to a common underlying risk function; it is the appropriate modeling approach for right-censored data with time-dependent covariates. 25
Model Construction
Our binary outcome variable was the diagnosis of acute malnutrition. We began model construction by selecting explanatory variables with theoretical significance to child undernutrition as identified by the UNICEF framework. 26 The full model included 17 explanatory variables representing the immediate, underlying, and basic causes of undernutrition. We then used a backward elimination approach to reduce the full model to a parsimonious one, removing variables that did not reach marginal statistical significance (P < .10). We planned a priori to include an interaction term between medical expenditures and child health status to examine whether the effect of child health status on acute malnutrition risk varied with the level of medical investment.
The results of the hazard analysis are expressed in terms of hazard ratios (HRs). For categorical predictors, HRs represent the relative risk of becoming acutely malnourished in the category of interest compared with children in the reference category. For continuous predictors, the HR is the relative risk of acute malnutrition associated with a 1-unit increase in the predictor. The exact marginal method was used to account for ties due to discrete time units.
We provide baseline descriptive statistics for all independent variables. We also report significance tests comparing mean differences for normally distributed variables (t tests), equality of medians for nonnormally distributed variables (Wilcoxon rank-sum tests), and frequencies for categorical variables (Pearson χ2 tests) at baseline between those children who eventually developed acute malnutrition and those who did not. Survival curves are provided for select outcomes using the Cox hazard model estimates. Values in the text are HRs with 95% confidence intervals (CIs), means (standard deviation), or frequency and percentage, as appropriate. Significance was assessed at the P < .05 level.
Exclusions
Data for 33 children were excluded after an analysis of changes in height between surveys suggested that in some households, children other than the target child may have been measured and/or height measurement errors exceeded plausible limits. We identified these 33 individuals as those whose height reduced between 2 consecutive surveys and/or those whose height increased at a pace >2.5 cm between 2 consecutive surveys while making allowances for measurement error (±2 cm). This limit to linear growth has been used elsewhere. 27 There is no evidence that excluded children were more or less likely to develop acute malnutrition than those retained (Pearson χ2 = 0.0067, P = .94).
Role of the Funding Source
The United States Agency for International Development (USAID) was not involved in the study design, data collection, analysis, writing, or the decision to seek publication.
Results
Participant Outcomes
Participation in the CTP was 100%; all 453 enrolled households received 6 cash transfers. Among households that retained for data analysis (n = 420), adherence to the survey and anthropometric measurement was 99% (n = 414),; 3 households declined participation in the survey in select months, and 3 were unable to be contacted in 1 or more months. Data for these households were included in analysis when available. Data for 2 households were right censored due to death of the target child. Post hoc power analysis indicates that the study sample size (n = 420) provided >80% power to detect each of the effects estimated by our Cox Proportional Hazard model (α = .05, 2 sided).
Figure 1 depicts a flow diagram of study participants. Seventy-four (18%) children became acutely malnourished (cases) over the course of the study; 58 (14%) of these were moderately malnourished and 16 (4%) severely malnourished. Thirty-four of the cases were indicated by WHZ alone, 4 by MUAC alone, 31 by both MUAC and WHZ, and 5 by edema. Moderately and severely malnourished children did not differ significantly by any of the baseline variables measured (results not shown).
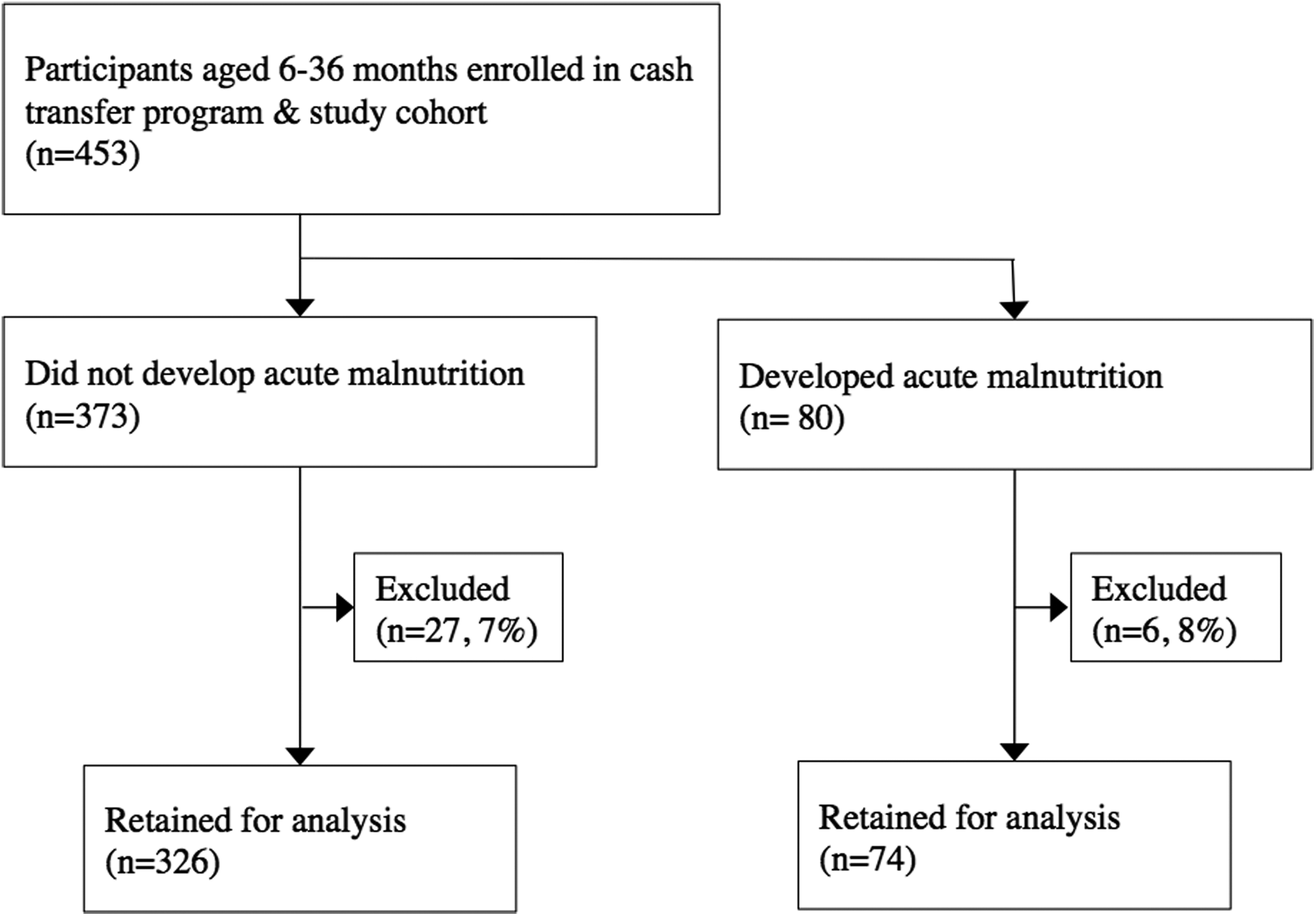
Flow diagram of study participants in Save the Children’s emergency cash transfer program in Maradi, Niger. Of the households in this study (n = 420), approximately 18% (n = 74) included a child who developed acute malnutrition. Data for households where a child was acutely malnourished were included in the analysis until the point of censorship. Children who exceeded plausible linear growth (>2.5 cm) and measurement error tolerances (±2 cm) between any 2 consecutive months were excluded from the analysis. In households with incomplete data due to refusal (n = 3) or loss to follow-up (n = 3), data were included in the analysis when available. Data from households in which a target child died (n = 2) were included until the month of the child’s death.
Comparison of Baseline Indicators Between Cases and Noncases
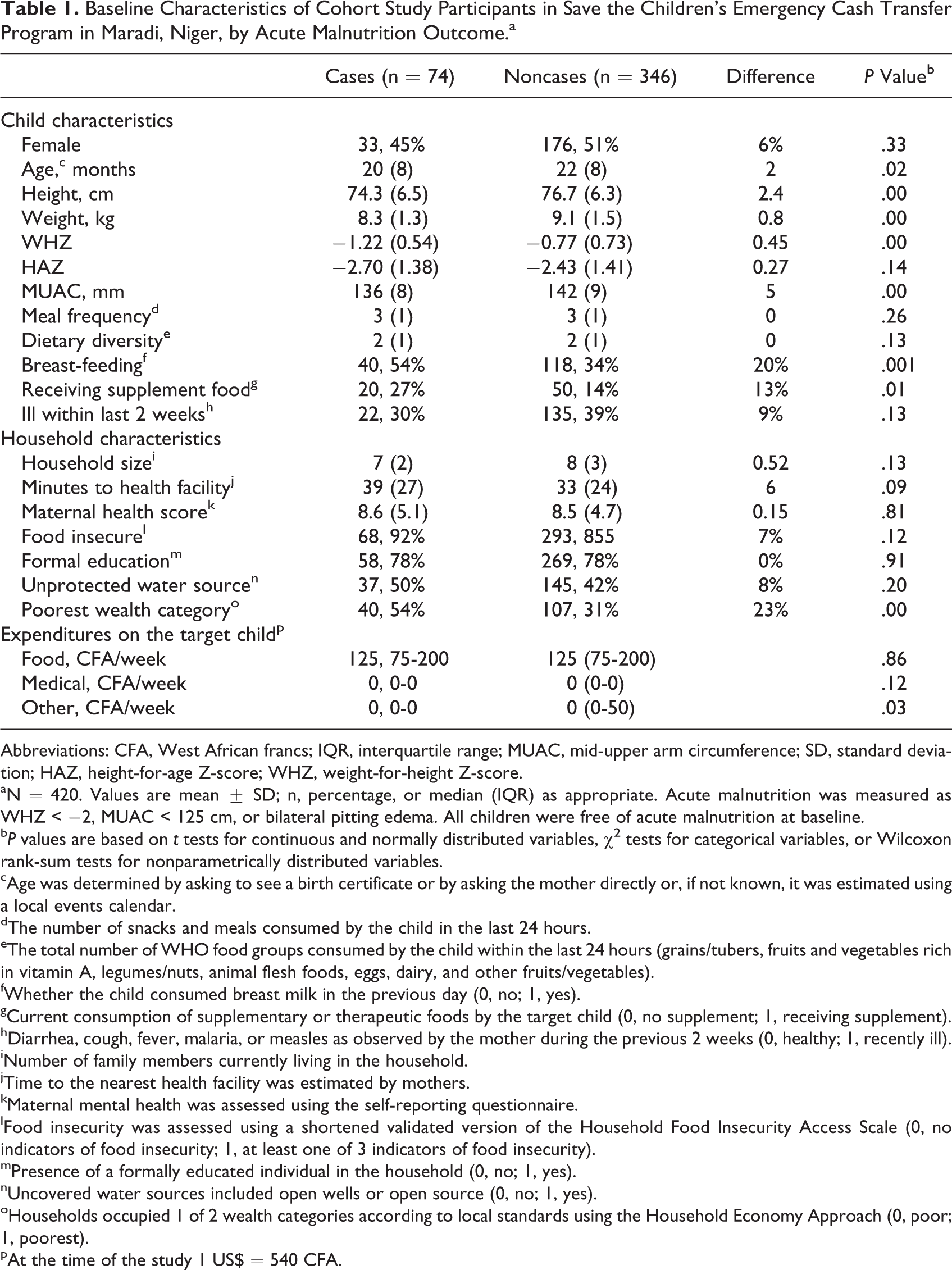
The baseline characteristics of participants are presented by acute malnutrition outcome in Table 1. The mean baseline age, WHZ, and MUAC of cases were lower by a magnitude of 2 months, 0.45 Z, and 5 mm, respectively (P < .05). Case households reported slightly but significantly less general spending (nonmedical and nonfood) on the target child (P < .05), and a larger proportion of case households were in the lowest wealth category (23% difference; P < .001). There were no significant differences between case and noncase households in terms of dietary diversity, meal frequency, recent childhood illness, household size, food insecurity, reported weekly spending on food or medical costs, education level, mothers’ health, time to nearest health facility, or the use of protected water sources at baseline. There were 950 reports of child illness, with between 33% (n = 138) and 53% (n = 222) of participants reporting an ill child in a given month.
Baseline Characteristics of Cohort Study Participants in Save the Children’s Emergency Cash Transfer Program in Maradi, Niger, by Acute Malnutrition Outcome.a
Abbreviations: CFA, West African francs; IQR, interquartile range; MUAC, mid-upper arm circumference; SD, standard deviation; HAZ, height-for-age Z-score; WHZ, weight-for-height Z-score.
aN = 420. Values are mean ± SD; n, percentage, or median (IQR) as appropriate. Acute malnutrition was measured as WHZ < −2, MUAC < 125 cm, or bilateral pitting edema. All children were free of acute malnutrition at baseline.
b P values are based on t tests for continuous and normally distributed variables, χ2 tests for categorical variables, or Wilcoxon rank-sum tests for nonparametrically distributed variables.
cAge was determined by asking to see a birth certificate or by asking the mother directly or, if not known, it was estimated using a local events calendar.
dThe number of snacks and meals consumed by the child in the last 24 hours.
eThe total number of WHO food groups consumed by the child within the last 24 hours (grains/tubers, fruits and vegetables rich in vitamin A, legumes/nuts, animal flesh foods, eggs, dairy, and other fruits/vegetables).
fWhether the child consumed breast milk in the previous day (0, no; 1, yes).
gCurrent consumption of supplementary or therapeutic foods by the target child (0, no supplement; 1, receiving supplement).
hDiarrhea, cough, fever, malaria, or measles as observed by the mother during the previous 2 weeks (0, healthy; 1, recently ill).
iNumber of family members currently living in the household.
jTime to the nearest health facility was estimated by mothers.
kMaternal mental health was assessed using the self-reporting questionnaire.
lFood insecurity was assessed using a shortened validated version of the Household Food Insecurity Access Scale (0, no indicators of food insecurity; 1, at least one of 3 indicators of food insecurity).
mPresence of a formally educated individual in the household (0, no; 1, yes).
nUncovered water sources included open wells or open source (0, no; 1, yes).
oHouseholds occupied 1 of 2 wealth categories according to local standards using the Household Economy Approach (0, poor; 1, poorest).
pAt the time of the study 1 US$ = 540 CFA.
Acute Malnutrition Risk Factors
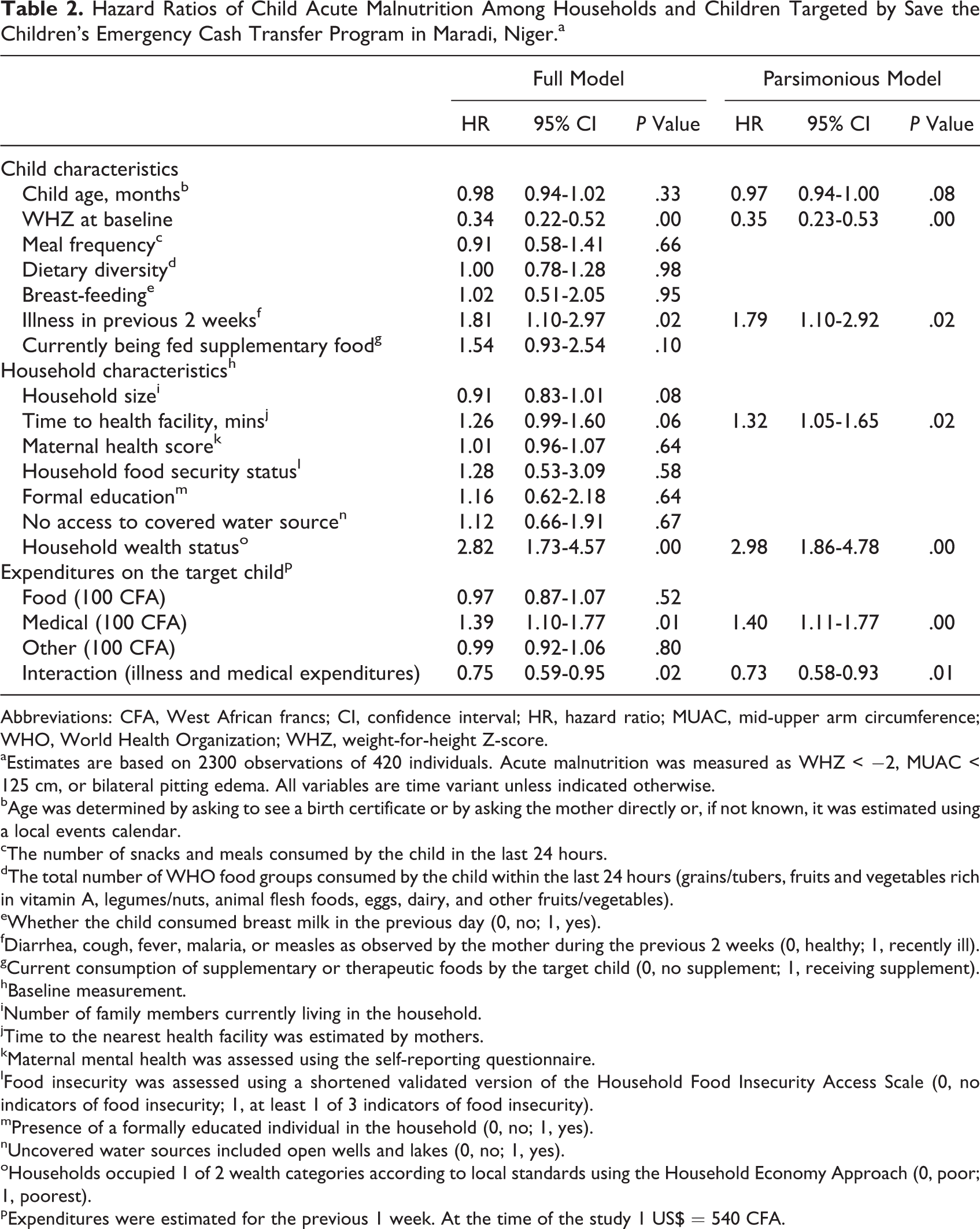
Hazard ratios from our full and parsimonious Cox proportional hazards models are presented in Table 2; estimates from the parsimonious model are referenced in the text unless otherwise noted. Weekly child food expenditures were not associated with the risk of acute malnutrition (HR: 0.97; 95% CI: 0.87-1.07; P > .05; full model; Figure 2, panel A). Children who had at least 1 of the 5 elicited symptoms of illness within the previous 2 weeks were 1.79 times more likely to become acutely malnourished than healthy children (HR: 1.79; 95% CI: 1.10-2.92; P < .05). Among ill children, medical expenditures were not associated with the risk of acute malnutrition (HR: 1.03; 95% CI: 0.98-1.08; P = .25). Weekly medical expenditures spent on healthy children were significantly associated with becoming acutely malnourished (HR: 1.40; 95% CI: 1.11-1.77; P < .01; Figure 2, panel B).
Hazard Ratios of Child Acute Malnutrition Among Households and Children Targeted by Save the Children’s Emergency Cash Transfer Program in Maradi, Niger.a
Abbreviations: CFA, West African francs; CI, confidence interval; HR, hazard ratio; MUAC, mid-upper arm circumference; WHO, World Health Organization; WHZ, weight-for-height Z-score.
aEstimates are based on 2300 observations of 420 individuals. Acute malnutrition was measured as WHZ < −2, MUAC < 125 cm, or bilateral pitting edema. All variables are time variant unless indicated otherwise.
bAge was determined by asking to see a birth certificate or by asking the mother directly or, if not known, it was estimated using a local events calendar.
cThe number of snacks and meals consumed by the child in the last 24 hours.
dThe total number of WHO food groups consumed by the child within the last 24 hours (grains/tubers, fruits and vegetables rich in vitamin A, legumes/nuts, animal flesh foods, eggs, dairy, and other fruits/vegetables).
eWhether the child consumed breast milk in the previous day (0, no; 1, yes).
fDiarrhea, cough, fever, malaria, or measles as observed by the mother during the previous 2 weeks (0, healthy; 1, recently ill).
gCurrent consumption of supplementary or therapeutic foods by the target child (0, no supplement; 1, receiving supplement).
hBaseline measurement.
iNumber of family members currently living in the household.
jTime to the nearest health facility was estimated by mothers.
kMaternal mental health was assessed using the self-reporting questionnaire.
lFood insecurity was assessed using a shortened validated version of the Household Food Insecurity Access Scale (0, no indicators of food insecurity; 1, at least 1 of 3 indicators of food insecurity).
mPresence of a formally educated individual in the household (0, no; 1, yes).
nUncovered water sources included open wells and lakes (0, no; 1, yes).
oHouseholds occupied 1 of 2 wealth categories according to local standards using the Household Economy Approach (0, poor; 1, poorest).
pExpenditures were estimated for the previous 1 week. At the time of the study 1 US$ = 540 CFA.
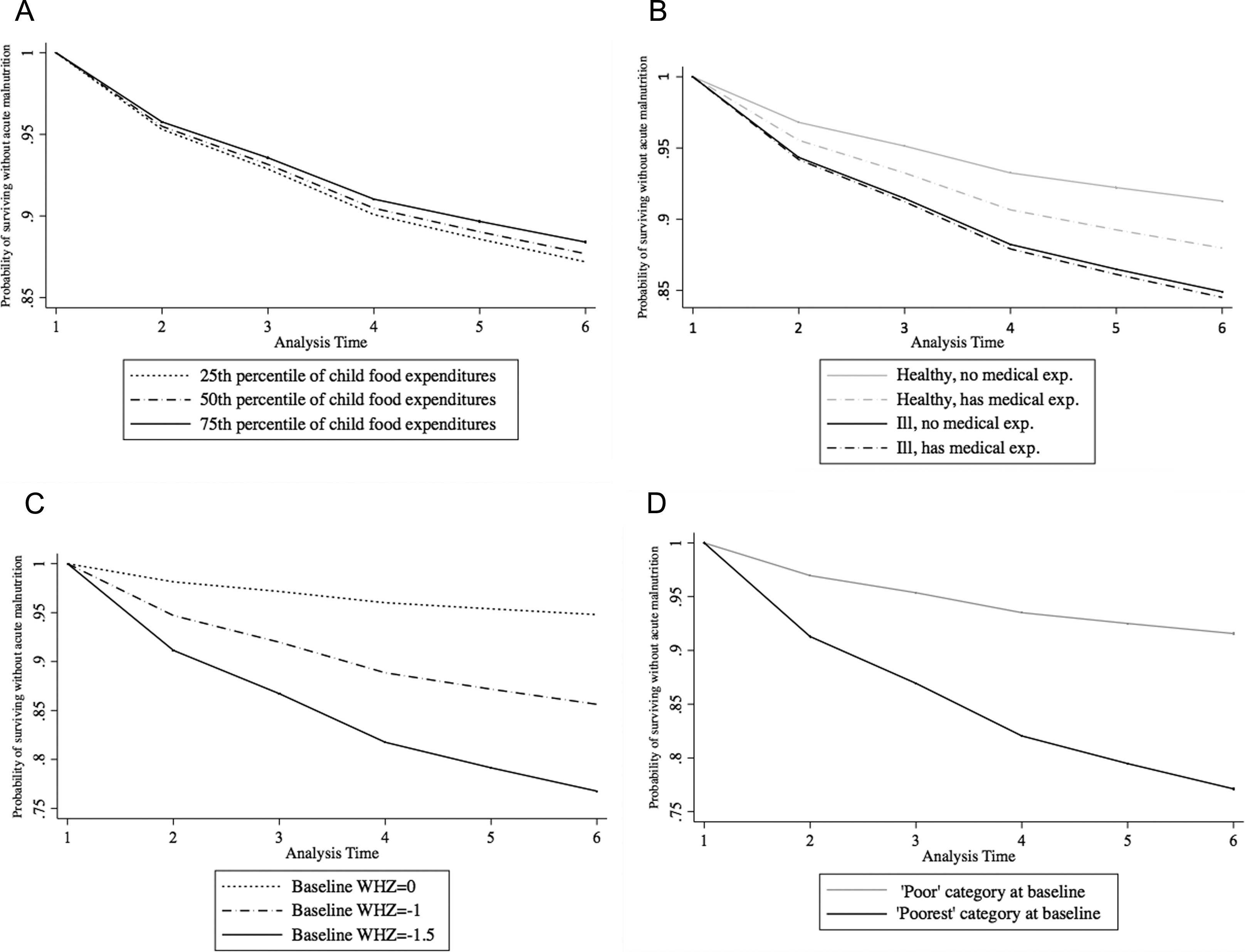
Acute malnutrition-free survival at specified levels of food expenditures, health status, medical expenditures, baseline weight-for-height Z-score (WHZ), and wealth category among participants in a study of Save the Children’s emergency cash transfer program in Maradi, Niger. The probability of surviving free of acute malnutrition among (A) children whose caregivers reported spending at the 25th, 50th, and 75th percentiles of weekly child food expenditures; (B) healthy and ill children, with and without medical expenditures (100 CFA); (C) children with no wasting (WHZ = 0), mild wasting (WHZ = −1) or borderline moderate wasting (WHZ = −1.5) at baseline; and (D) children in households in 1 of 2 different wealth categories, “poor” or “poorest”, at baseline, as estimated by our Cox Proportional Hazards models. Unspecified covariates are evaluated at their mean values.
Children with a higher WHZ at baseline had a lower risk of acute malnutrition compared to those with lower baseline WHZ, with each unit increase in baseline WHZ associated with a 65% reduction in risk (HR: 0.35; 95% CI: 0.23-0.53; P < .001; Figure 2, panel C). Children in households ranked as “poorest” at baseline were significantly more likely than children in households ranked as “poor” to become acutely malnourished (HR: 2.98; 95% CI: 1.86-4.78; P < .001; Figure 2, panel D). Greater distance from health facilities was associated with greater risk (HR: 1.32; 95% CI: 1.05-1.65, P < .05).
Older child age showed a trend toward lower risk (HR for age: 0.97; 95% CI: 0.94-1.00; P = .08). None of the following factors were found to be significantly associated with the risk of acute malnutrition: food or other expenditures, meal frequency, dietary diversity, current breast-feeding, household food security status, household size, maternal mental health, the presence of a formally educated household member, or the use of protected water sources. An interaction between baseline WHZ and child age was not significant (results not shown).
In the qualitative interviews, most respondents reported returning home following transfer distributions and handing their household’s transfer directly to their husband. Further investigation of the data on medical expenditures revealed that the majority of households spent no money on medical costs: Of the 950 reports of child illness, only 300 were accompanied by reports of medical expenditures. An additional 43 reports of child medical expenditures were unaccompanied by reports of recent child illness and are presumed to represent either preventive medical spending on healthy children or unelicited cases of child illness.
Discussion
Among households targeted by this 6-month emergency CTP, food expenditures for children and other diet-related factors were not found to be associated with the risk of acute malnutrition. Rather, low baseline WHZ, baseline household poverty status, and the occurrence of child illness were significantly associated with high risk.
The Lack of Association Between Dietary Risk Factors and Acute Malnutrition
Our findings draw attention to a prevailing paradigm regarding the role of emergency CTPs, which equates increased income with increased expenditures on food and, ultimately, improved child nutritional status. 11 Similar thinking perpetuates in nutrition research, programming, and policy, which tend to focus on the dietary causes of undernutrition and retain a strong “food-first” bias. 28,29 This paradigm exists, despite extensive evidence from income generation and poverty reduction interventions, which demonstrates that increased income and/or food expenditures are insufficient to influence child growth. As reported previously in a pre–post analysis of the same cohort studied here, median food and medical expenditures for children increased significantly over the duration of the SC intervention, 8 and yet we observed no protective effect of this behavior. Rather, our findings are consistent with early work showing that additional income has little effect on child nutritional status, particularly when households remain below or near the poverty line 30 or subsist in the context of a poor health environment. 31 Even in food-secure or well-off households, children may not have adequate diets due to variation in infant and child-feeding practices, household coping strategies in which poor and wealthy households alike reduce food intake during food shortages, and intrahousehold food and resource allocation. 32
In The Food Policy and Research Institute’s (IFPRI) recent study from Niger, cash transfers were found to be less effective promoters of diet quality where markets were poorly functioning, food prices were unstable, and/or beneficiaries favored bulk grain purchases over diet diversification. 10 High food prices were viewed as a key factor in the Nigerien food crisis of 2012 33 and were ongoing during the CTP studied here. High prices, in concert with the purchasing preferences seen by Hoddinott et al, may have constrained SC program’s potential to influence children’s acute malnutrition risk through diet-related factors.
Understanding Factors Associated With Acute Malnutrition Risk in the Nigerien Context
The food-first bias neglects the causative role of disease and the importance of access to medical care, factors that our analysis showed to be more indicative of acute malnutrition risk than food- and diet-related factors. Illness was frequent in our study population and was associated with a high risk of acute malnutrition; this risk did not vary significantly with medical spending. Two studies by Hampshire et al, both conducted in Niger following a food crisis in 2005, lend valuable insight into caregiver decision-making regarding child health and nutrition in emergency contexts. 32,34 Uptake of child health services was very low: children with commonplace illnesses (diarrhea, fever, or respiratory infection) were seldom taken for treatment, while more serious or chronic conditions were often considered an intrinsic quality of the child rather than a treatable illness. The authors observed that while the intent of humanitarian interventions is to save lives, the behaviors and decisions made by households and caregivers in emergency-prone contexts are often risk adverse and detrimental to child health, favoring instead the preservation of the long-term viability of the household. Constrained decision-making abilities and the need for long-term livelihood preservation resulted in a “failure to invest in growth-faltering children.” 32 It is reasonable to expect that similar circumstances informed beneficiary decision-making in the context of our study and the 2012 food crisis and may further explain the high risk of acute malnutrition associated with illness.
Improving health service access by alleviating financial barriers is a realistic emergency CTP objective with precedence in nonemergency conditional programs, particularly those that promote awareness of how and when to pursue care in contexts where services exist. 6,35 However, for an unconditional CTP in a context such as Niger, where health service infrastructure is weak, 36 where the health environment is suboptimal, and where livelihood preservation strategies may not always favor child health outcomes, mitigating acute malnutrition risk factors is likely to be especially challenging. This was seen in the study by Langendorf et al in Niger, where cash-only beneficiaries experienced a 2-fold greater risk of acute malnutrition than households receiving any combination of cash and supplementary food. 9
The significance of preintervention child anthropometric status and household wealth in our results suggests that the CTP in question may have come too late to help the most vulnerable children in the sample. It is reasonable to infer that an emergency CTP alone cannot offset the major physiological vulnerabilities associated with extreme and chronic poverty. Further research about the optimal timing and appropriate value of emergency CTPs would help inform future program design. 37 Commitment and investment in nutrition-specific and nutrition-sensitive interventions, including agriculture, public health initiatives including water and sanitation, and social protection schemes with capacity for seasonal surges in resources and programming, may be more effective approaches for increasing resilience to shocks and promoting sustained prevention of undernutrition and poverty. 5,38
Limitations
This analysis relied on retrospective expenditure data, which may have been recalled differentially for food and medical expenses. Given the communal nature of food preparation and consumption in Niger, estimating food expenditures for 1 child was likely to introduce bias. Medical expenditures may have been easier to recall, as they were discrete events with more obvious ties to 1 individual. We do not expect that food or medical expenditure recall errors varied systematically, and we posit that the short recall period (1 week) limited the extent of recall errors. 39 Expenditure is difficult to measure accurately, and the lack of significant findings in this study should not diminish their importance in promoting positive child health outcomes.
We also see limitations in our definition of child illness. Our survey tool was restricted to 5 acute conditions and neglected to capture many common or chronic conditions or symptoms (such as vomiting, anemia, helminth infection, micronutrient deficiency, or HIV/AIDS), which would have necessitated medical costs and been associated with higher risk of acute malnutrition but were not elicited by study enumerators. As a result, we suspect that some individuals were misclassified as healthy, leading to conflation of the impact of the influences of medical expenditures and undocumented child illness. In these cases, medical expenditures were tantamount to a second variable capturing unqueried illnesses and their associated risk of acute malnutrition.
Although higher maternal education and knowledge has been associated with improved child nutrition outcomes in previous studies, our data did not contain enough variation to assess this relationship. Finally, although a pre–post analysis of this data reveals that participants showed substantial improvements in anthropometric outcomes, the attributable impact of the CTP cannot be estimated in the absence of a control group. 8
Conclusion
We found several health-related factors—medical expenditures, child illness, low baseline WHZ, and poverty—to be associated with a high risk of the development of acute malnutrition in the context of an unconditional emergency CTP implemented during the 2012 food crisis in Niger. Food- and diet-related factors—food expenditures, meal frequency, dietary diversity, and household food insecurity—were conversely not associated with the risk of acute malnutrition. These findings highlight the importance of the health-related determinants of child undernutrition and suggest that a potential role of emergency CTPs may be to enable and promote health service access where services exist. They also indicate a need for more sustained poverty reduction and undernutrition prevention activities in concert with well-timed and strategic use of emergency interventions. Future study involving the use of a comparison group and conditional terms that promote child health and nutrition would be an appropriate way to determine how and whether the incidence of acute malnutrition is reduced in the presence of emergency CTPs.
Footnotes
Authors’ Note
This article is an original work and has not been submitted for publication elsewhere. The authors state no conflicts of interest. All authors have seen and approved the form and content of the submitted manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.