
Abstract
Keywords
Introduction
Acute malnutrition, which includes severe acute malnutrition (SAM) and moderate acute malnutrition (MAM), is a significant public health issue that disproportionately affects children in low- and lower-middle-income countries (Black et al., 2013; World Health Organization, 2013). Approximately 45.4 million children under the age of five globally are affected by SAM and MAM, over 80% of whom reside in low- and lower-middle-income countries (World Health Organization, 2021). MAM is defined by a weight-for-height z-score between −2 and −3 or a mid-upper-arm circumference between 115 and 125 mm (World Health Organization, 2013). SAM is classified as a weight for height z-score below −3, or mid-upper-arm circumference < 115 mm, or the presence of bilateral oedema (World Health Organization, 2013, 1999). Children with SAM are specifically at an increased risk of serious illnesses and death (Bhutta et al., 2017). However, through early identification and treatment, SAM and MAM can be managed safely before the onset of life-threatening complications (World Health Organization, 2013). In 2016, the United Nations declared that 2016–2025 would be the Decade of Action on Nutrition, which set a concrete timeline to address all forms of malnutrition for all people (World Health Organization, 2021a). In alignment with Sustainable Development Goals 2 (zero hunger) and 3 (good health and well-being), the Decade of Action on Nutrition called for policy action across six key areas, including the provision of social protection and nutrition-related education for all, and the provision of universal coverage of essential nutrition interventions (United Nations, 2015; World Health Organization, 2021a). These long-term goals to decrease worldwide acute malnutrition demonstrate global commitment, responsibility, and engagement in reducing nutritional challenges.
The Community Management of Acute Malnutrition (CMAM) approach has been outlined as the standard of care for treating acute malnutrition in children globally (Collins et al., 2006b; World Health Organization, 2013; World Health Organization et al., 2007). The CMAM approach was developed to address the challenges associated with previous inpatient methods of treating acute child malnutrition, especially in settings with few health facilities or limited health facility admission capacity (Wilford et al., 2012). The CMAM approach aims to provide direct treatment for acutely malnourished children, while initiating community mobilization efforts (Collins et al., 2006a, 2006b; World Health Organization et al., 2007). A key component of a CMAM approach is the mobilization of community volunteers, including community health workers (CHWs), to identify, refer, and treat children with acute malnutrition at the household and community level, rather than in the healthcare setting (World Health Organization, 2013). While CMAM programs make use of ready-to-use therapeutic foods (RUTFs) and ready-to-use supplementary foods (RUSFs) there are instances where alternatives to RUTFs and RUSFs are used to treat MAM and SAM in children. Through identifying early cases of malnutrition, providing treatment (i.e. RUTFs and RUSFs) to acutely malnourished children, and incorporating community mobilization and engagement, the CMAM approach aims to increase program accessibility, maximize coverage, and strengthen intervention compliance among program participants in community settings (Collins et al., 2006a).
We define complex community-based interventions for acute child malnutrition as interventions that incorporate active surveillance and screening, treatment, and nutrition education or counselling in community settings (i.e. outside of health care facilities). This review examined the domains and mechanisms that influence the implementation of complex community-based interventions for acute child malnutrition in low- and lower-middle-income countries. Although the establishment of referral pathways with local health facilities is critical in addressing complicated cases of acute child malnutrition, this review focuses specifically on facilitators and barriers to implementing the community-based components of complex community-based interventions for acute child malnutrition. While previous systematic reviews have evaluated the broad role of CMAM programs in addressing acute child malnutrition, limited research has analysed the ways through which program components and mechanisms interact with broader contextual factors to influence intervention implementation in community settings. To address this gap, the aim of this review was to examine the facilitators and barriers to complex community-based nutritional interventions for addressing acute malnutrition in low- and lower-middle-income countries. Our objectives were (1) to identify and describe complex community-based interventions that address acute child malnutrition through active surveillance and screening, treatment, and education in low- and lower-middle-income countries; and (2) to investigate the domains (e.g. sociocultural and geographical) and mechanisms (e.g. multi-stakeholder collaboration) that shape facilitators and barriers in implementing complex community-based interventions to address acute child malnutrition.
Methods
This review followed the methodology outlined by Arksey and O’Malley, in addition to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Scoping Reviews (PRISMA-ScR) to identify relevant published literature using a systematic search process (Arksey and O’Malley, 2005; Tricco et al., 2018).
Search strategy
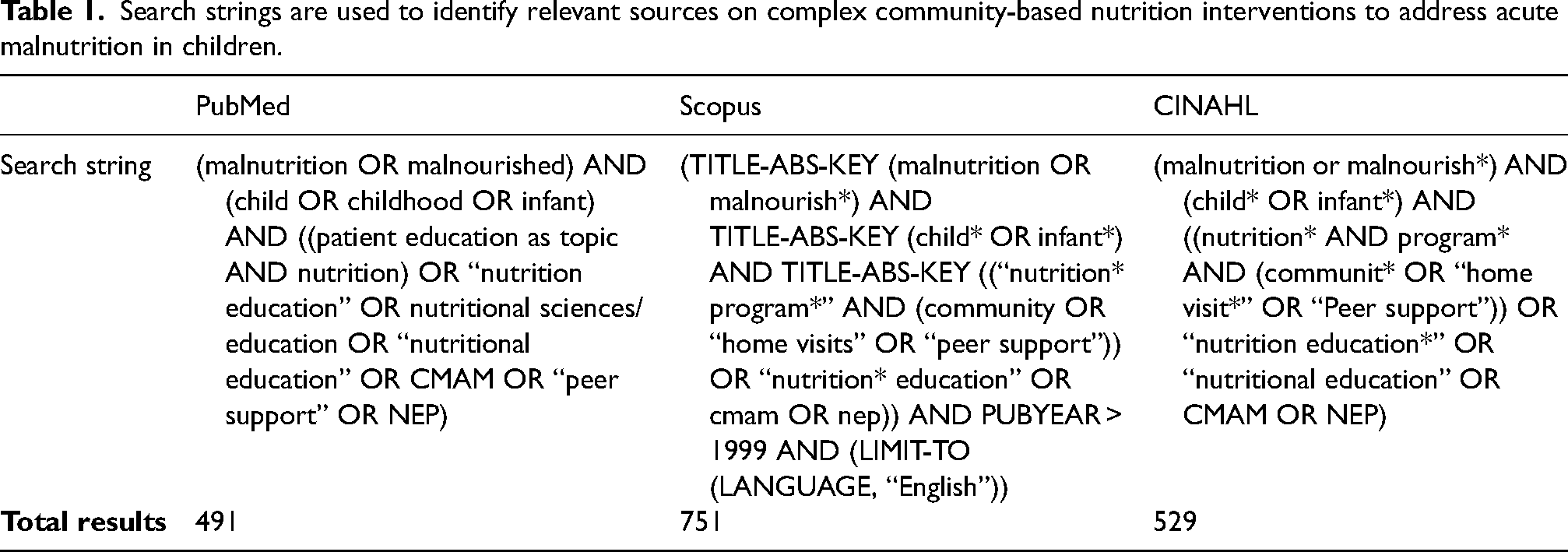
Three databases (PubMed, Scopus, and CINAHL) were searched to identify peer-reviewed articles (Table 1), and search strings were adapted for each database. Database searches were conducted on 3 January 2024. Retrieved articles were imported to Covidence (review management software) for automatic de-duplication and screening.
Search strings are used to identify relevant sources on complex community-based nutrition interventions to address acute malnutrition in children.
Determining eligibility
Inclusion and exclusion criteria were developed to capture relevant literature discussing complex community-based interventions that address acute malnutrition in children (Table 2). To be included, articles needed to be published in English since the year 2000 (in alignment with the United Nations Millennium Development Goals) and refer to interventions addressing acute malnutrition in children between the ages of 6 months and 5 years (inclusive). Based on the CMAM approach for addressing acute child malnutrition, articles also needed to contain the following three implementation components within community settings to be included in this review: (1) active surveillance and screening of SAM/MAM (i.e. home visits of CHWs to assess anthropometric measures of children to monitor growth and screen for SAM/MAM); (2) treatment of SAM/MAM (i.e. RUTFs and RUSFs); and (3) an educational intervention component for parents/caregivers of children with SAM/MAM (i.e. community workshops and cooking demonstrations). Geographic location was restricted to low- and lower-middle-income countries due to the disproportionate burden of acute child malnutrition in these settings (Otiti and Allen, 2021; World Bank, 2021).
Eligibility criteria used to determine the inclusion or exclusion of sources on complex community-based nutrition interventions to address acute malnutrition in children.
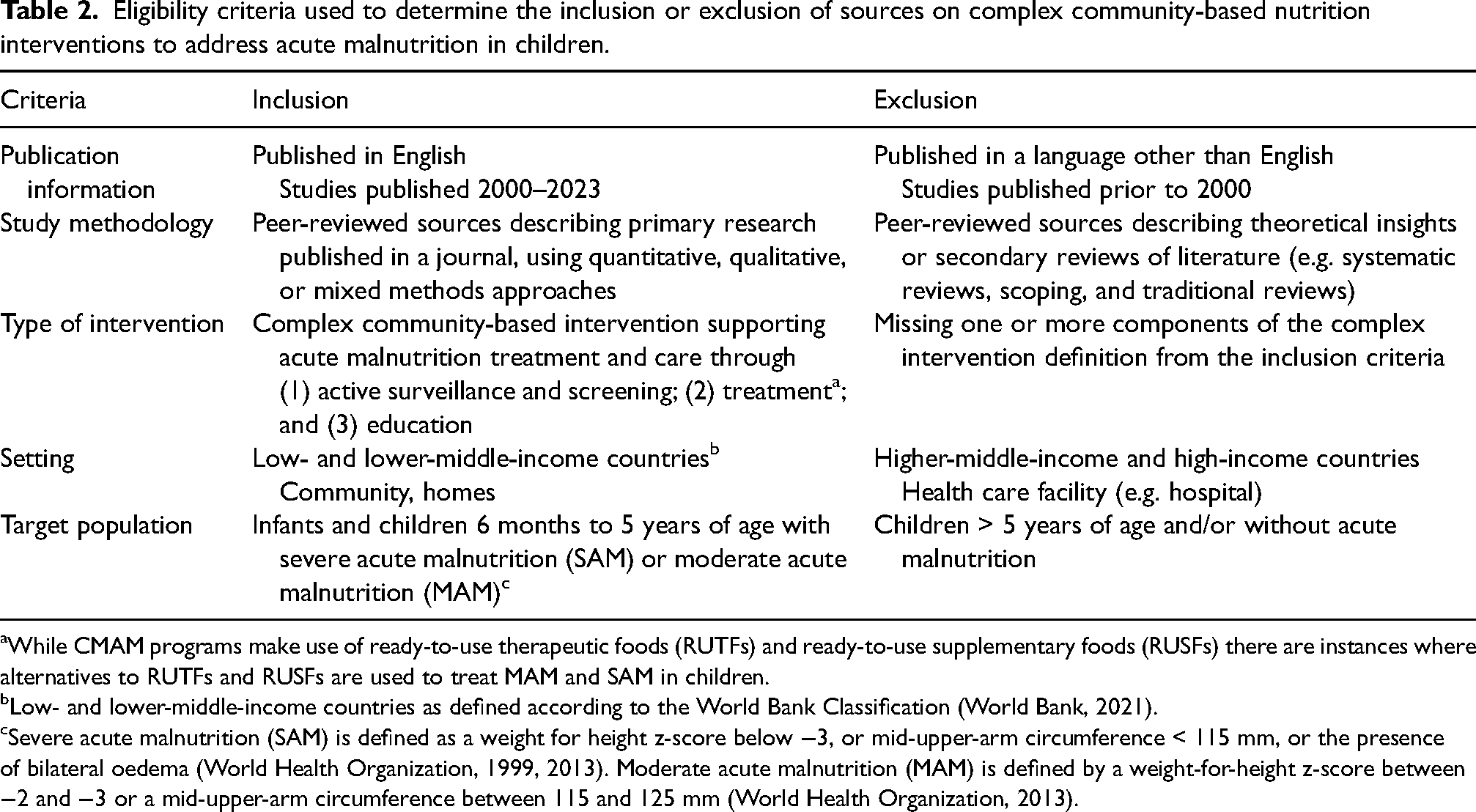
While CMAM programs make use of ready-to-use therapeutic foods (RUTFs) and ready-to-use supplementary foods (RUSFs) there are instances where alternatives to RUTFs and RUSFs are used to treat MAM and SAM in children.
Low- and lower-middle-income countries as defined according to the World Bank Classification (World Bank, 2021).
Severe acute malnutrition (SAM) is defined as a weight for height z-score below −3, or mid-upper-arm circumference < 115 mm, or the presence of bilateral oedema (World Health Organization, 1999, 2013). Moderate acute malnutrition (MAM) is defined by a weight-for-height z-score between −2 and −3 or a mid-upper-arm circumference between 115 and 125 mm (World Health Organization, 2013).
Screening and selection process
Two reviewers (BB and MB) independently screened the titles and abstracts of each article in Covidence using the eligibility criteria. Articles meeting the eligibility criteria proceeded to full-text screening conducted by each reviewer. Reviewers met throughout the screening process to clarify uncertainties and resolve conflicts through iterative discussion and consensus. A third reviewer (WD) was consulted to resolve any cases where there was a lack of consensus between the two reviewers. For both rounds of screening, interrater reliability was determined by calculating Cohen's kappa coefficient (McHugh, 2012). Finally, one reviewer (BB) hand-searched the reference list of each included article to identify any additional articles that met the inclusion criteria. Informed by the approach used by Bustos et al., this final stage of screening included the identification and inclusion of complementary articles from the same project (e.g. study protocols) (Bustos et al., 2021). By including these complementary articles, we aimed to gain a more comprehensive understanding of the design and implementation of the included articles.
Data extraction and analysis
Data were extracted on article characteristics, intervention design, and facilitators and barriers to intervention implementation. The development of the data extraction tool was informed by WHO guidelines, the CMAM model, and the UNICEF conceptual framework on child malnutrition, with attention to how various domains and mechanisms shaped intervention implementation (UNICEF, 2020). This tool was piloted with a subset of included articles, refined, and then used to extract data from all included articles (Appendix A in the Supplemental Material).
Data analysis was informed by the underlying theories of the CMAM model and the UNICEF conceptual framework of child malnutrition (Collins et al., 2006a; UNICEF, 2020; World Health Organization et al., 2007). The UNICEF conceptual framework underscores how child malnutrition is affected by many intersecting factors ranging from macro-level (e.g. good governance; social and cultural norms; adequate health and social services) to micro-level (e.g. availability of nutrient-rich food; feeding and dietary practices) processes and elements. Key considerations in implementing community-based interventions for acute child malnutrition include treatment timeliness and accessibility, sociocultural awareness and sensitivity, and community engagement and trust building (Collins et al., 2006a).
An iterative deductive and inductive approach was used to identify overarching themes, which were organized into domains and mechanisms. For the deductive analysis, the CMAM model and the UNICEF conceptual framework described above initially guided our assessment of how interactions among domains and mechanisms influenced the implementation of complex community-based interventions to address acute malnutrition in children. Then, we examined content related to intervention implementation across included projects to inductively assess whether existing themes required revision or refinement. Overarching themes were then organized iteratively into three main domains and eight mechanisms to describe how different domains and mechanisms influence the implementation of complex community-based nutrition interventions.
Results
The search resulted in a total of 1771 articles. After the removal of duplicate articles, the titles and abstracts of 1229 articles were screened. The Cohen's kappa coefficient at this stage of screening was 0.62, indicating ‘substantial’ agreement between reviewers. Of the 139 articles reviewed for full-text eligibility, 116 articles were excluded due to various reasons, including missing program criteria or including a participant population outside of the scope of the review. The Cohen's kappa coefficient at this stage of screening was 0.67, again indicating ‘substantial’ agreement between reviewers. The reference lists of included articles (n = 23) were hand-searched and a further 15 articles were identified for inclusion in the review. In total, 38 articles representing 26 different projects were included in the review (Figure 1).
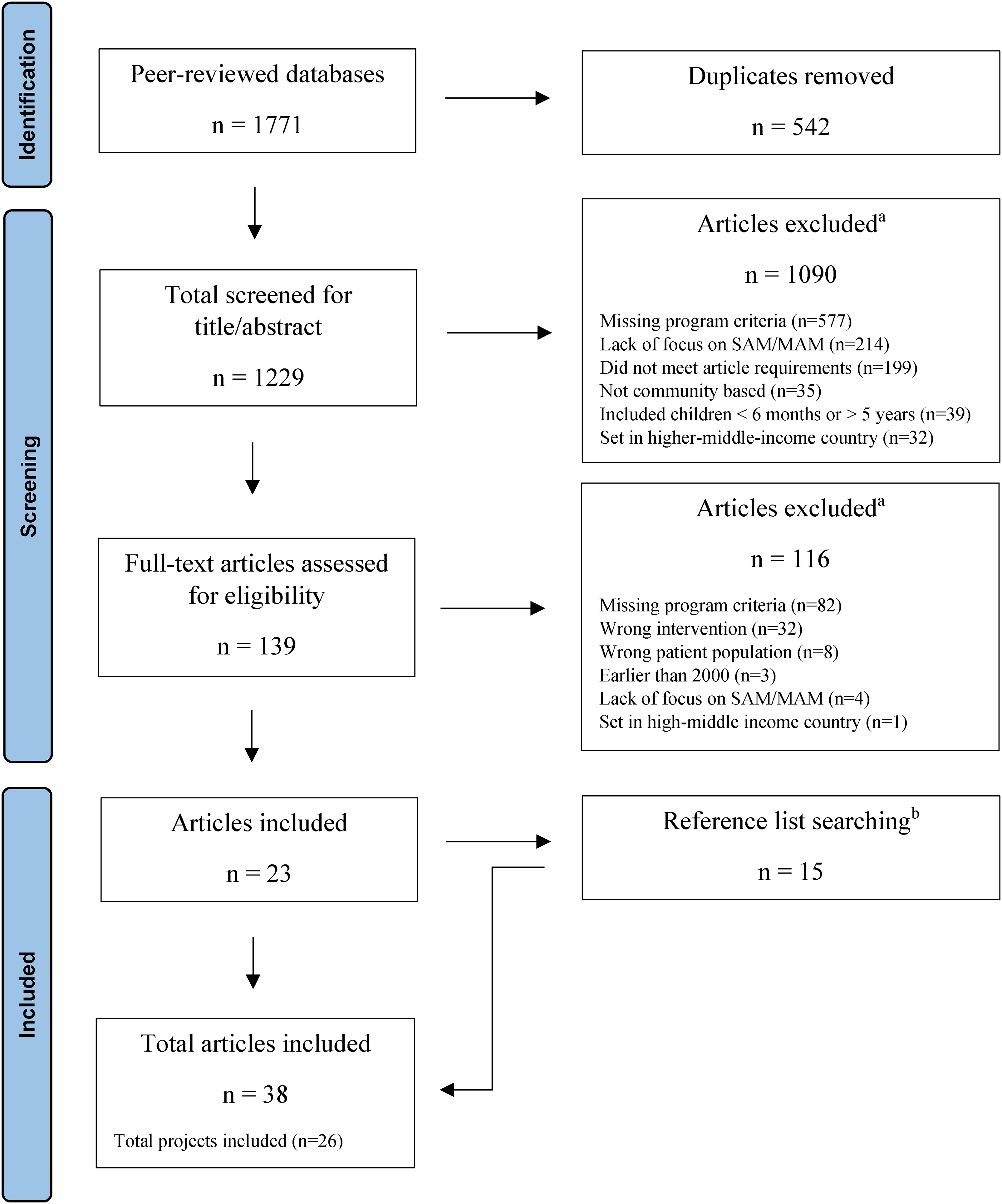
Flowchart indicating stages of screening and number of references included at each stage of the screening process. (a) Articles may have been excluded for multiple reasons. (b) Reference lists of the 23 included articles were hand-searched by one reviewer to identify any additional articles that met the inclusion criteria. This final stage of screening included the identification and inclusion of complementary articles from the same project. This was done to gain a more comprehensive understanding of the design and implementation of included articles. The total number of articles included in this study is n = 38, which includes a total of n = 26 different projects.
Of the 26 projects identified, all projects were situated in either Asia (46%; n = 12) or Africa (54%; n = 14). Further, slightly more projects were situated in lower-middle-income countries (58%; n = 15) than low-income countries (42%; n = 11) (Table 3).
Characteristics of complex community-based nutrition interventions described across projects (n = 26).
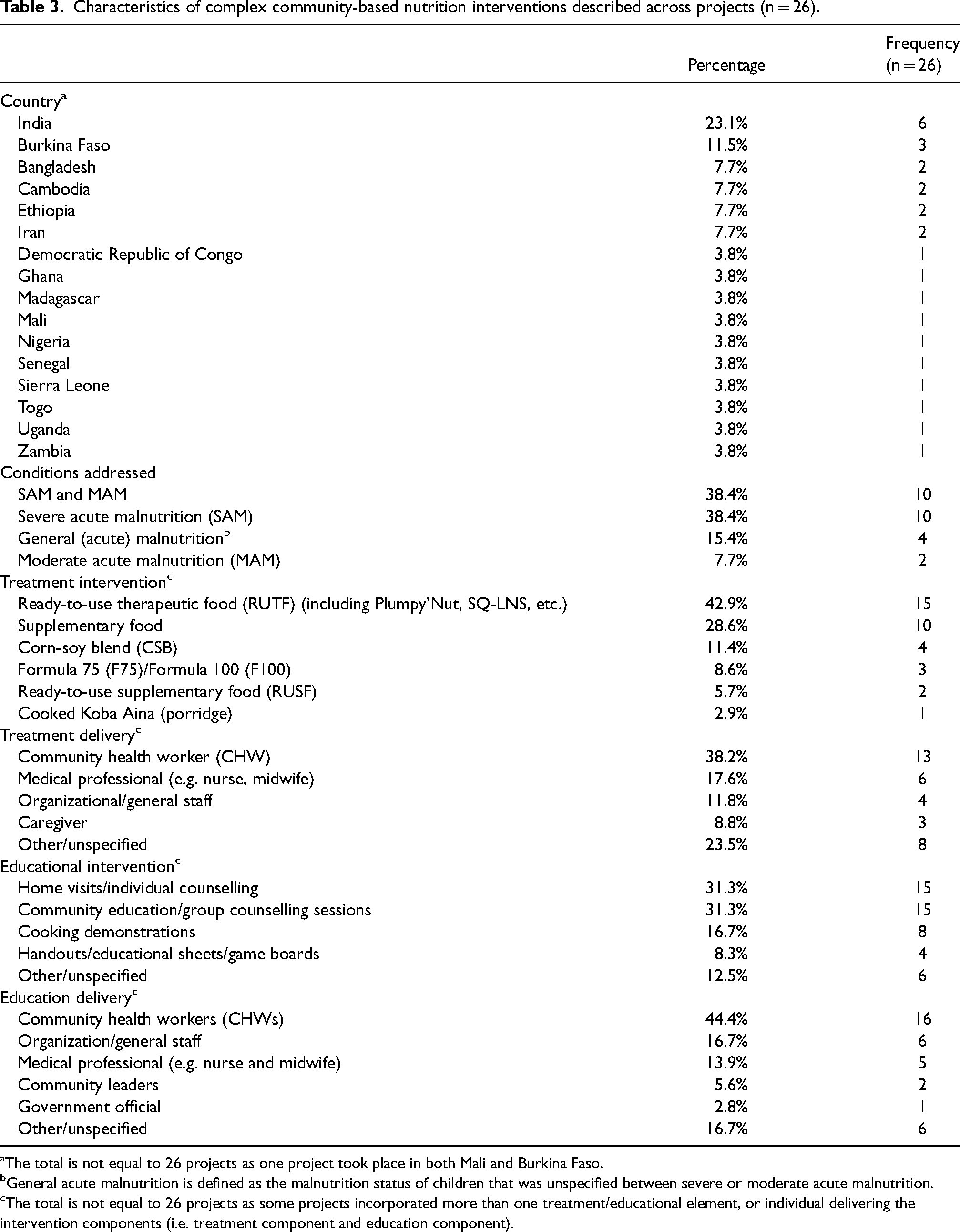
The total is not equal to 26 projects as one project took place in both Mali and Burkina Faso.
General acute malnutrition is defined as the malnutrition status of children that was unspecified between severe or moderate acute malnutrition.
The total is not equal to 26 projects as some projects incorporated more than one treatment/educational element, or individual delivering the intervention components (i.e. treatment component and education component).
The review is organized according to three main domains: the household and interpersonal domain; the sociocultural and geographical domain; and the operational and administrative domain. Examples were drawn from the identified projects to examine and understand how these domains interacted with identified mechanisms to influence the facilitators and barriers that shaped the implementation of complex community-based interventions to address acute child malnutrition (Figure 2).
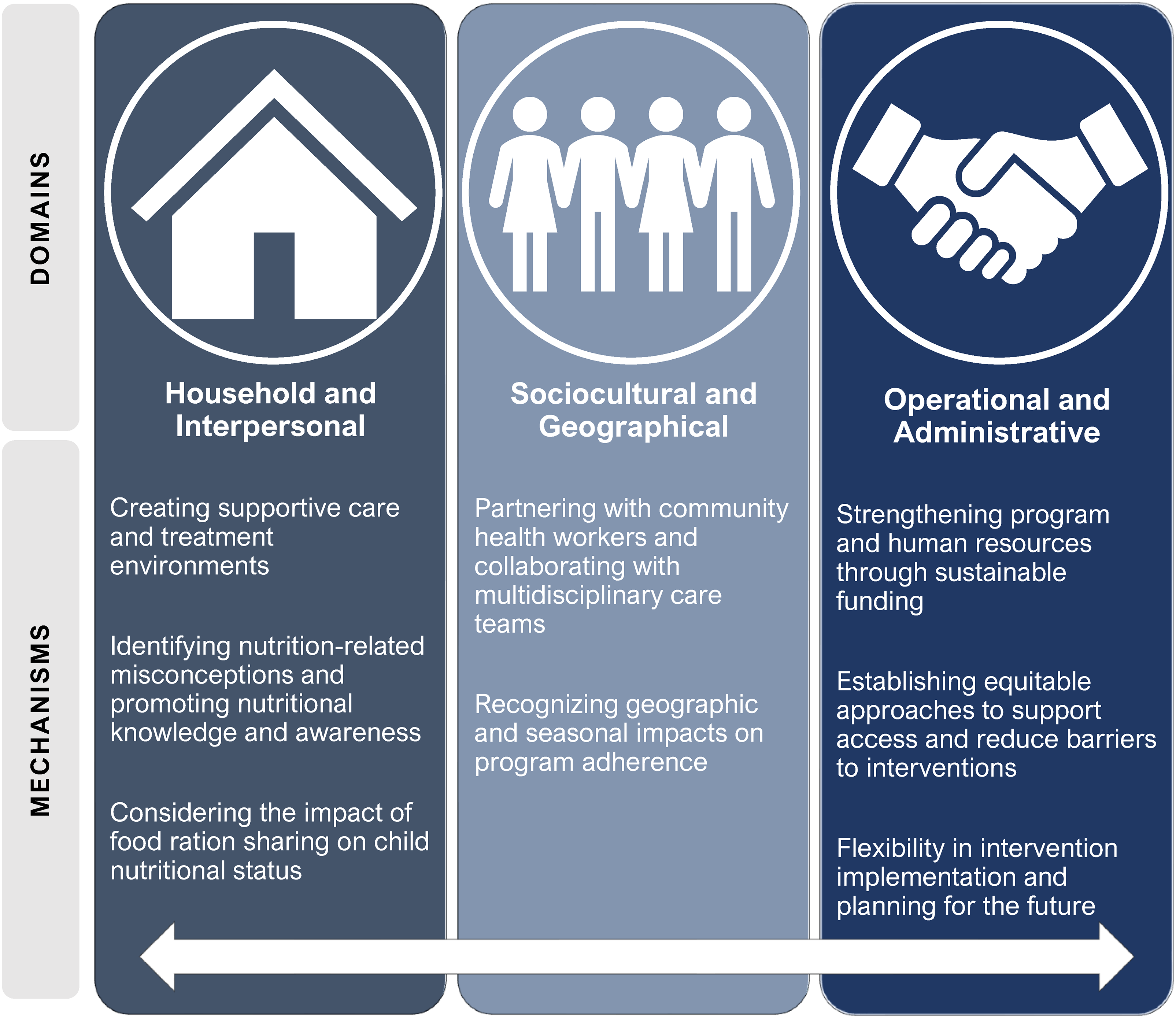
Summary of main domains and mechanisms used to guide the analysis of complex community-based interventions for acute child malnutrition.
Household and interpersonal domain
Creating supportive care and treatment environments
Relationships fostered within the community-based interventions were frequently highlighted as important mechanisms to facilitate caregiver empowerment and subsequent success in the interventions. Strong connections and relationships created between caregivers participating in programs often contributed to support outside of the program (More et al., 2018). For instance, women in Madagascar felt connected to their peers within the program after participating in group activities, and felt confident to share their knowledge and educate other mothers in their community (Magnin et al., 2018). Mothers in Sierra Leone also participated in a peer-counselling group focused on child nutrition, which was positively associated with child recovery (Maust et al., 2015).
Positive relationships between program implementers and participants also facilitated effective intervention implementation and positive treatment outcomes. For example, in Madagascar, women felt welcomed by and equal to health workers, which increased confidence (Magnin et al., 2018). Similarly, mothers in Mumbai, India, were regularly encouraged by health workers, and subsequently gained confidence to act on child health issues (More et al., 2018). In Iran, caregivers were offered both group-based nutritional education sessions as well as monthly face-to-face counselling sessions to learn about their children's requirements (Shenavar et al., 2022). Overall, trust in CHWs and other leaders, including religious leaders, nutrition experts, and practitioners in the community, was frequently highlighted as a key component to facilitating effective intervention implementation (Chanani et al., 2019; Gartner et al., 2006; More et al., 2018). While some health educators in Jharkhand, India, found it challenging to quickly establish a trusting and reciprocal relationship with caregivers during their initial home visits (Chaand et al., 2019), the support and positive involvement demonstrated by CHWs and other community members toward caregivers participating in these interventions acted as key facilitators for empowerment among caregivers and improved the nutritional outcomes of children.
Identifying nutrition-related misconceptions and promoting nutritional knowledge and awareness
When implementing each stage of complex community-based nutrition interventions, community engagement was essential to ensure programs were appropriate and relevant for intended participants. Community engagement and trust were especially important in projects where cultural norms or limited education contributed to misconceptions surrounding food and child nutrition. For example, many caregivers in Bihar, India, indicated that they did not consider the peanut oil-based treatment (i.e. RUSF) offered to their children as effective and, consequently, would often think about stopping treatment (Burtscher and Burza, 2015). Additionally, caregivers in this project wanted to see immediate results when their child started any treatment, so some caregivers were discouraged when their child did not rapidly gain weight. Prior to intervention educational sessions in Bangladesh, some caregivers believed that expensive fruits, including grapes and apples, were healthy for their children, whereas other foods, such as oil and eggs, were regarded as indigestible for young children (Roy et al., 2005). Further, many caregivers held passive beliefs surrounding the causes of child malnutrition and disease. However, through community engagement to promote awareness of treatment options by local health services, a change in health-seeking behaviour was observed among participating caregivers (Burtscher and Burza, 2015; Roy et al., 2005).
Across multiple projects, semi-regular (i.e. weekly or monthly) community workshops and cooking demonstrations were used as methods to teach nutrition education. For example, in Burkina Faso, weekly nutritional counselling sessions included cooking demonstrations to teach participants how to make enriched porridge with local ingredients (Somassè et al., 2016). Similarly, caregivers in Gujarat, India, were shown how to prepare recipes using locally available ingredients, and were also provided information on feeding practices and hygiene (Umallawala et al., 2022). In Cambodia, caregivers participated in two nutrition education sessions each month, with a focus on child feeding practices and food preparation. Furthermore, caregivers in Nigeria were provided with culturally appropriate education tools for both clinic and home use, which led to improvements in recognizing clinical danger signs and symptoms related to their child's nutritional status (Hitchings et al., 2022). In order to reduce nutritional misconceptions and promote nutritional knowledge and awareness in both Mumbai, India, and Madagascar, frontline health workers frequently inquired about children's well-being, repeatedly provided educational information to mothers using simple language, and took time to encourage the entire family throughout their completion of the program (Magnin et al., 2018). This advice was perceived as practical, concrete, and realistic, which helped caregivers understand the program content and facilitated their continued attendance and intervention adherence (Magnin et al., 2018). In contrast, inconsistent counselling and knowledge transfer appeared to negatively impact program implementation. For instance, caregivers in Uganda expressed that they did not receive sufficient nutritional counselling, which contributed to uncertainty about how to best care for their children (Gagnon-Dufresne et al., 2022). However, in Cambodia and Mumbai, India, home visits were integrated into nutrition interventions to promote the consumption of food supplements and encourage caring practices (Chanani et al., 2019; Menasria et al., 2018). Recognizing an opportunity to expand health education and financial literacy, additional information beyond nutritional requirements was implemented into a nutrition education program in Madagascar, including information on hygiene, handwashing, and budgeting (Magnin et al., 2018). These components added to the comprehensiveness of the program and offered additional information to facilitate positive outcomes for participants that addressed the broader social determinants of health. Across projects, culturally appropriate education of caregivers delivered by trusted community members or intervention implementers facilitated confidence in the intervention among caregivers.
Considering the impact of food ration sharing on child nutritional status
In alignment with the UNICEF conceptual framework, successful intervention implementation and adherence to nutrition interventions were directly influenced by immediate and micro-level determinants. For instance, many of the families involved in complex community-based nutrition interventions experienced poverty, which meant that food-based treatments intended for acutely malnourished children (i.e. RUSF and RUTF) were often shared with other family members (Collins et al., 2006a; Ghodsi et al., 2018; Moramarco et al., 2018). In Ghana, these sharing practices impacted intervention outcomes as sharing RUTFs with siblings was directly linked to poor recovery and nutritional outcomes among children being treated for acute malnutrition (Akparibo et al., 2017). Similarly, researchers in Cambodia found it difficult to ascertain the degree to which food-based treatment contributed to an individual child's nutritional rehabilitation, as food rations were frequently shared with other family members (Harris and Jack, 2011). With this challenge in mind, programs in Ethiopia and Zambia successfully provided larger quantities of food to participating households. Thus, in areas where food availability was often inadequate, acutely malnourished children still received the required treatment to facilitate recovery, even if the rations were shared with family members (Collins et al., 2006a; Moramarco et al., 2016). Evidently, attention to intrahousehold dynamics including the distribution and consumption of food was important for intervention design and implementation.
Sociocultural and geographical domain
Partnering with community health workers and collaborating with multidisciplinary care teams
Collaboration with multiple partners prior to and during program implementation was a key mechanism that facilitated successful intervention implementation in community settings. Of note, CHWs were consistently recognized as key partners and implementers of complex community-based nutrition interventions. In Bangladesh, CHWs received routine supervision and refresher trainings, which included a bimonthly two-day intensive session on technical aspects of the program and provided a way for CHWs to ask questions and receive feedback throughout the intervention implementation process (Puett et al., 2013). Further, CHW supervisors were sometimes strategically placed as surveyors to oversee implementation processes in this program in Bangladesh. As these supervisors held pre-existing relationships with CHWs, this collaboration between CHWs and their supervisors was intended to enhance the comfort of CHWs throughout the implementation phase, in contrast to being monitored by unfamiliar third parties (Puett et al., 2013). Conversely, most of the CHWs in an intervention in Iran reported that they had not been supervised by health inspectors and had not received any feedback on their performance (Ghodsi et al., 2017). In this case, CHWs felt that regular visits with their supervisors could facilitate collaboration and enable them to speak about their daily challenges, which could lead to practical solutions to improve intervention outcomes (Ghodsi et al., 2017). Thus, supportive collaboration with supervisors who held pre-existing relationships with CHWs appeared to facilitate successful intervention implementation.
Collaboration among CHWs, other health care workers, and caregivers was also important in effective intervention delivery. For instance, while CHWs were able to lead the intervention in Burkina Faso, collaboration between CHWs and nurses was necessary for the calculation of anthropometric measures that were required for discharge (Somassè et al., 2013). In Mumbai, India, health workers collaborated with community members outside of standard intervention components, with some respondents mentioning that frontline health workers helped them with referrals to healthcare services, including accompanying mothers and their children to hospitals if needed (More et al., 2018). In response, community members felt grateful for the health care workers and were motivated to participate in program activities, which improved intervention and health outcomes (More et al., 2018). However, CHWs in Jharkhand, India, generally found it challenging to encourage caregivers to adhere to the treatment plan and stated that the CMAM program seemed to be competing with other government-led initiatives without ensuring adequate participation from frontline health workers (Chaand et al., 2019). Across projects, when CHWs were involved in the delivery of complex community-based interventions, appropriate training and supervision of CHWs, in addition to collaboration between CHWs and other individuals or organizations (e.g. local health facilities, frontline healthcare workers, and non-governmental organizations), were highlighted as key facilitators to ensure effective intervention implementation.
Recognizing geographical and seasonal impacts on program adherence
Geographical distance and seasonal employment also acted as barriers to intervention accessibility and made it difficult both for caregivers to participate in program components with their children and for implementers to monitor and support participants (Akparibo et al., 2017; Burtscher and Burza, 2015; Burza et al., 2015; Chaand et al., 2019; Hitchings et al., 2022). For instance, program implementers found active surveillance and screening challenging in Jharkhand, India, because of the remote location of many villages, which frequently led to the automatic exclusion of participants living in these settings. Across several projects, some caregivers were unable to afford transportation costs, which influenced their decision to attend or complete treatment sessions (Burtscher and Burza, 2015; Gagnon-Dufresne et al., 2022; Harris and Jack, 2011). To address the geographical and financial challenges associated with program adherence, caregivers in the Democratic Republic of Congo were given an unrestricted cash transfer each month, and were encouraged to use it however they needed (Grellety et al., 2017). An intervention in Mumbai, India, strategically targeted a community in which houses were located close to each other, which enabled frontline health workers to make frequent home visits to specific households while also conducting ongoing active surveillance of children across the community (More et al., 2018).
Another barrier to intervention adherence was that caregivers in some settings were unable to routinely attend nutritional education sessions due to work-related absences (Nikièma et al., 2014). For instance, an analysis of seasonal trends in Bihar, India, indicated an increase in participants defaulting from nutritional programs during months when there was a high demand for agricultural work (Burza et al., 2015). Acknowledging this challenge, community-based treatment centres in Bihar, India, were generally open on the same day each week to provide consistency and reliability for caregivers (Burza et al., 2015). This consistency allowed caregivers to anticipate when treatment would be offered and optimize their time to better engage in the educational components of the program. Overall, recognizing seasonal challenges and accounting for geographical barriers when designing interventions facilitated successful recruitment, participation, and adherence.
Operational and administrative domain
Strengthening program and human resources through sustainable funding
Establishing sustainable funding approaches to facilitate program and human resource distribution across program activities increased adherence to program components and positively influenced program sustainability. In Burkina Faso, efforts to increase community participation in a CMAM program and reduce drop-out rates were facilitated through the development of a community fund supported by program stakeholders (Somassè et al., 2013). For an intervention in Mumbai, India, program costs were subsidized by a network of municipal health facilities, and costs were further minimized by using locally produced RUTF (Goudet et al., 2018; More et al., 2018). Similarly, food baskets and food vouchers in an intervention in Bangladesh were funded and provided by an NGO and distributed to households through health centres, which reduced barriers to accessing these resources (Ghodsi et al., 2017, 2018).
While sustainable funding and incentives were important for reducing barriers to intervention access for caregivers and children enrolled in various programs, incentives and compensation were also often necessary for encouraging and maintaining the involvement of implementers throughout the program duration. For instance, due to a high workload for staff and human resource shortages during an intervention in Iran, it was indicated that both financial and nonfinancial incentives may encourage and motivate health workers involved in intervention implementation (Ghodsi et al., 2017). In Burkina Faso, community volunteers initially agreed to work without financial compensation, but the volume of work led them to expect compensation (Somassè et al., 2013). Both of these experiences contributed to a decrease in health workers’ motivation and weakened ongoing monitoring of malnourished children (Ghodsi et al., 2017; Somassè et al., 2013). Recognizing the complexity of these interventions, compensation for implementers was an important facilitator of effective program implementation and maintenance.
Establishing equitable approaches to support access and reduce barriers to interventions
The various approaches used to identify potential participants and deliver effective interventions influenced equity considerations within the implementation, evaluation, and outcomes of complex community-based nutrition interventions across settings. To reduce barriers to participation, it was important for interventions to account for the specific needs of participants and to design incentives that addressed these community needs in various contexts. In Iran, researchers believed that increasing knowledge was critical for program success, and food baskets were only provided if mothers attended education sessions along with routine health monitoring of children (Ghodsi et al., 2017). Similarly, in Senegal, children were provided weekly or monthly food supplementation only if their mothers attended nutrition and health education sessions (Gartner et al., 2006). While mothers were provided with incentives to support adherence to program components in these settings, these approaches may unintentionally increase barriers to participation among some caregivers and children when the distribution of incentives is conditional on attendance to educational sessions.
While the provision of education services and resources encouraged caregivers to participate in both treatment and education program components, financial barriers still impacted participants during intervention delivery. For example, while it was important that caregivers were provided with nutrition education, knowledge about feeding practices did not compensate for the impacts of poverty, which limited the ability of some caregivers to purchase high-quality food and adopt nutritional advice (Gagnon-Dufresne et al., 2022; Grellety et al., 2017; Magnin et al., 2018). With this challenge in mind, interventions in Burkina Faso and Zambia incorporated cooking lessons that used local ingredients that were culturally acceptable and frequently consumed by the population, which made it easier for caregivers to follow cooking advice provided in nutritional education sessions (Moramarco et al., 2018; Nikièma et al., 2014; Somassè et al., 2013). In Madagascar, caregivers reported that their ability to implement nutritional advice in their household was possible due to complementary financial support provided through the intervention (Magnin et al., 2018).
Inequitable access to nutrition treatment and education due to transportation costs was a frequent barrier for community members living far from settings where interventions were implemented. In Bangladesh, caregivers living near the treatment and education site were more likely to be recruited for the intervention because there were no funds available to reimburse transportation costs associated with caregivers living further away from program sites (Puett et al., 2013). However, in India, transportation and treatment were fully covered for children who were hospitalized but then returned to their home community to restart the community-based intervention (Bhandari et al., 2016). This approach ensured that health emergencies did not impact the ability of these children and their caregivers to participate in the intervention. Overall, addressing barriers to treatment and education access, in addition to centring equity considerations in intervention design, facilitated successful intervention implementation.
Flexibility in intervention implementation and planning for the future
An openness to revise or change intervention components was an important mechanism for intervention design and implementation. For example, in Burkina Faso, screening criteria evolved to include more participants in the intervention (Chaand et al., 2019). In Nigeria, a weekly schedule of clinic visits was recommended whenever possible, but monthly visits were acknowledged as a more feasible alternative to deliver effective treatment when travel was difficult for caregivers (Hitchings et al., 2022).
Evaluations of intervention implementation yielded important information that could be used for future program development. Following the evaluation of a CMAM intervention in Bihar, India, researchers determined that future communication plans needed to include education strategies that acknowledged acute child malnutrition as a disease in communities, along with the use of trusted community members (including priests and healers) to disseminate this information (Burtscher and Burza, 2015; Chanani et al., 2019). In Burkina Faso and Cambodia, researchers acknowledged that future education programs needed to deliver more concrete information about nutrients and the use of local foods in addressing acute child malnutrition (Harris and Jack, 2011; Menasria et al., 2018; Nikièma et al., 2014; Somassè et al., 2016).
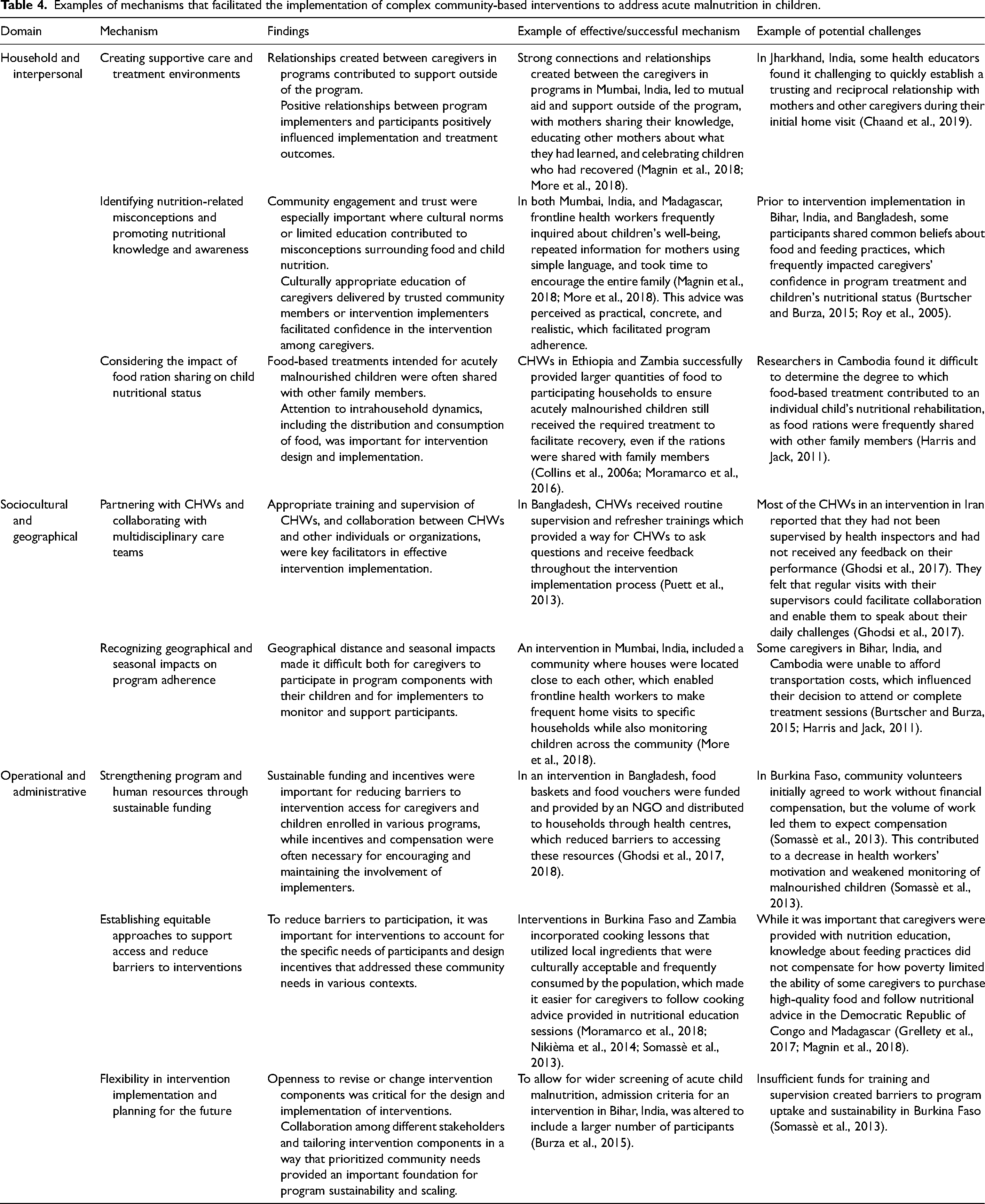
Some projects explicitly considered the sustainability of interventions and the ability to replicate interventions in the future. In Burkina Faso, community volunteers, women, and older adults collectively demonstrated ownership of the intervention, and were ready to take over the intervention following initial implementation (Somassè et al., 2013). However, a key challenge reported from an intervention in Mumbai, India, was the lack of focus on handing over responsibility of program activities to either government partners or to the communities where the intervention was implemented (More et al., 2018). Similarly, Somassè et al. reported that a lack of funds for training and supervision, in addition to management of the program by a team external to the local health system, were the main barriers to broader uptake and sustainability of the program in Burkina Faso (Somassè et al., 2013). Thus, collaboration among different stakeholders and tailoring intervention components in a way that prioritized community needs provided an important foundation for program sustainability and scaling (Table 4).
Examples of mechanisms that facilitated the implementation of complex community-based interventions to address acute malnutrition in children.
Discussion
This review mapped three domains and eight mechanisms that were integral to the successful implementation of complex community-based interventions to address acute child malnutrition. A total of 38 articles, including 26 different projects, were examined in this review. The need to account for context-specific factors to address challenges in program accessibility and adherence was acknowledged across different mechanisms identified in this review. For instance, in the sociocultural and geographical domain, the influence of distance and seasonal work demands was a consistent barrier to intervention adherence, particularly for women with multiple caregiving responsibilities (Akparibo et al., 2017; Burtscher and Burza, 2015; Burza et al., 2015; Chaand et al., 2019). The cost of transportation and the commute time acted as a barrier in several interventions, which influenced the extent to which caregivers could participate in nutritional program components such as education and counselling workshops. As such, these geographical barriers may aggravate other challenges in the household domain, such as limited nutrition-related knowledge and awareness among caregivers. In addition, geographical barriers may also create challenges for CHWs and health workers who need to reach specific populations for surveillance, screening, and treatment. While the CMAM approach emphasizes a community-based approach to addressing acute child malnutrition, there is limited guidance on how to account for and address geographical factors that influence program accessibility, adherence, and implementation. This gap points to the need to identify, define, and account for contextual challenges, including geographical barriers, that program participants may encounter at an operations and administration level when planning and designing complex community-based interventions to address acute malnutrition in children.
Misconceptions surrounding nutrition among caregivers and food ration sharing among household members were challenges that shaped intervention outcomes across projects and articles. As acute child malnutrition is prevalent among populations experiencing poverty in resource-constrained settings, it is important to consider that caregivers and households may have limited educational opportunities or insufficient resources for their daily needs. These poverty-related factors may create additional barriers to intervention adherence and effectiveness. To support participants and address these challenges, interventions should prioritize education efforts that are culturally appropriate (e.g. use of recipes that include available and accessible ingredients) and focus on ongoing engagement to facilitate improved nutritional knowledge and adherence to interventions. Moreover, frequent instances of food sharing among household members may indicate that these interventions must also address the economic and food security needs of the entire household to ensure the success of nutrition interventions for SAM and MAM (Tadesse et al., 2015). However, in some cases, certain program design elements, such as mandatory attendance or engagement in certain program components, may have unintentionally acted as a barrier to program participation. Thus, when designing complex community-based nutrition interventions, consideration should be given to which elements may create barriers to intervention participation or adherence. To mitigate these barriers, program implementers can weigh the relative value and necessity of these elements along with the potential use of incentives to further mitigate barriers to participation and adherence.
The essential role that CHWs play in the implementation of community-based nutrition interventions was highlighted across different domains and mechanisms identified in this review. Specifically, engaging and collaborating with CHWs and non-formal healthcare workers facilitated successful implementation because participants and community members were often comfortable with these individuals, which enhanced program adherence (Puett et al., 2013). Moreover, CHWs play a particularly important role in community-based approaches as they have the potential to address concerns and challenges that are experienced in specific community settings given their unique positionality as both members of the community and health workers with specialized nutritional knowledge. Thus, CHWs may be better aware of and able to address barriers to program participation and adherence, which ultimately can increase the likelihood that interventions are delivered as intended at the community and household level (Heidkamp et al., 2021; Puett et al., 2013; World Health Organization, 2021b). Further, the critical role of CHWs within the health system should be matched with an equivalent investment in resources to equip and enable these individuals to fully contribute at various stages of community-based interventions to address acute malnutrition in children. Indeed, many projects and articles included in this review noted a need for CHWs to be more thoroughly equipped, compensated, and supported in their involvement and leadership with complex community-based interventions (Briaux et al., 2020; Chaand et al., 2019; Ghodsi et al., 2017; Somassè et al., 2013). Overall, adequate training, management, and compensation need to be provided to CHWs at the operational and administrative levels to ensure that future interventions maintain strong community trust and engagement while ensuring long-term program sustainability.
This review highlights the importance of recognizing community-based nutrition interventions for acute child malnutrition as complex interventions that are comprised of multiple intersecting program components. To address acute malnutrition in children and support sustainable interventions, these interventions must be designed, implemented, and evaluated with sensitivity to context-specific factors. While this review identified multiple domains with underlying program mechanisms, it should be emphasized that these mechanisms and domains interact and overlap to influence program implementation and intervention outcomes directly and indirectly. For instance, the mechanisms identified in the sociocultural and geographical domains and the strategies implemented in the operational and administrative domains have implications for the experiences of program participants and implementers in the household and interpersonal domains. In designing and implementing future interventions, teams could more explicitly incorporate and consider how the various domains and mechanisms identified through this review interact and shape complex community-based nutrition interventions that aim to address acute malnutrition in children.
This review has several limitations. First, projects or articles that did not explicitly include all three components of our definition of a complex community-based nutrition intervention (screening, treatment, education) were excluded from the review. This means that we may have excluded interventions that did not highlight one component of this definition, but that could have enhanced our understanding of how various domains and mechanisms influence child nutrition outcomes. Additionally, studies published in languages other than English were excluded from this review, which may have led to the exclusion of relevant literature. Second, this review specifically focused on acute malnutrition in children (i.e. MAM and SAM) and excluded interventions that addressed other forms of malnutrition, such as stunting, underweight, or micronutrient deficiencies. As such, the generalizability of the findings from this review may be limited for nutrition interventions that address other forms of child malnutrition. Medical components of treatment were also excluded from this review, as the focus of the review was on the implementation of complex community-based nutrition interventions. Identifying the medical factors associated with treatment and examining facilitators and barriers to establishing effective referral linkages for medically complicated cases within a CMAM approach would be a valuable avenue for future research. In addition, future research may benefit from further analysis of the differences in results for programs that addressed only SAM, only MAM, or both SAM and MAM. Third, this review was mainly informed by the CMAM model and the UNICEF Conceptual Framework for Child Malnutrition. While these frameworks are relevant for acute child malnutrition, we were not able to integrate insights from other nutrition-related programs that consider the intersections between childhood illnesses and child feeding practices with acute child malnutrition (Keats et al., 2021; World Health Organization, 2009; Young et al., 2012). Finally, this review excluded grey literature, which may have provided further implementation details. Future research would benefit from a systematic search of grey literature to examine the domains and mechanisms highlighted in this review. In particular, while the involvement of CHWs was broadly highlighted as a critical facilitator influencing project implementation across settings, limited details were provided within projects about how the profile or characteristics of CHWs may shape efforts to address acute malnutrition in children (Heidkamp et al., 2021; López-Ejeda et al., 2019; Ogobara Dougnon et al., 2021). Notwithstanding these limitations, this review provides important insights into facilitators and barriers to implementing complex community-based interventions to address acute malnutrition in children in low- and lower-middle-income countries.
Conclusion
We identified eight mechanisms across the interpersonal, sociocultural, and operational domains that influenced the implementation of complex community-based nutrition interventions to address acute child malnutrition in low- and lower-middle-income countries. Identifying and addressing contextual challenges experienced by program participants and implementers, such as the influence of geographical barriers, can support program accessibility and adherence. Moreover, the process of designing complex community-based nutrition interventions should include a critical evaluation of the relative importance of various program components to reduce participant burden, mitigate barriers to access, and support program participation (Heidkamp et al., 2021). Lastly, strengthening the potential of CHWs to contribute to nutrition interventions through sufficient management, support, and compensation can facilitate strong community trust and engagement and ensure program sustainability. Moving forward, future nutrition interventions should develop, design, and implement community-based approaches that integrate the interpersonal, sociocultural, and operational domains to facilitate effective and sustainable strategies to improve acute malnutrition among children in low- and lower-middle-income countries.
Supplemental Material
sj-docx-1-nah-10.1177_02601060241253327 - Supplemental material for Facilitators and barriers to implementing complex community-based interventions for addressing acute malnutrition in low- and lower-middle income countries: A scoping review
Supplemental material, sj-docx-1-nah-10.1177_02601060241253327 for Facilitators and barriers to implementing complex community-based interventions for addressing acute malnutrition in low- and lower-middle income countries: A scoping review by Bridget Beggs, Monica Bustos, Laura Jane Brubacher, Matthew Little, Lincoln Lau and Warren Dodd in Nutrition and Health
Footnotes
Acknowledgements
The authors are grateful to Ashleigh Domingo and Taylor Harris for project support.
Authors’ contributions
MB and WD led project conceptualization, methodology development, and data collection. BB finalized data collection and conducted the formal analysis. BB, MB, and WD wrote the first version of the manuscript draft. LJB, ML, and LL provided detailed review and input for the manuscript.
Availability of data and materials
The authors confirm that the data supporting the findings of this review are available within the article and/or its supplementary materials.
Consent for publication
All authors consent to the publication of this review in Nutrition and Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this scoping review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.