
Abstract
Background:
Little is known about how the knowledge and the knowledge-sharing effectiveness (KSE) of health extension workers (HEWs) affect maternal knowledge of optimal infant and young child feeding (IYCF) and their child’s nutritional status.
Objective:
The objective of this study was to evaluate mothers’ and HEWs’ knowledge of key IYCF practices and to investigate whether mothers’ knowledge and HEWs’ KSE are associated with stunting in young children (aged 12-23 months).
Methods:
This cross-sectional study used face-to-face interviews to assess the IYCF knowledge of HEWs (n = 96) and mothers of 12- to 23-month-old children (n = 122) in Mecha district, West Gojam, Ethiopia. The association between HEWs’ KSE and children’s length-for-age z scores (LAZ) was investigated.
Results:
Stunting (50%), underweight (34%), and wasting (10%) were highly prevalent. Less than half (45%) of the mothers had access to nutrition education through the health extension program, but those who had, had better knowledge of IYCF practices and thus lower rates of stunting (P < .001). However, key IYCF practices were not well understood by the HEWs and this affected their KSE. The gap in KSE was negatively associated with LAZ (r = −.475, P < .001) and remained significant even after adjusting for maternal height, socioeconomic status, and maternal education (r = −.423, P = .002).
Conclusion:
Health extension workers’ KSE is associated with child stunting. Future training of HEWs would benefit from emphasis on not only the content of the IYCF messages but also the process of delivery while increasing their counseling skills.
Keywords
Introduction
In developing countries, growth faltering (stunting) is a serious public health concern that remains unacceptably high. 1 Stunting prevalence reaches its peak during the complementary feeding period (6-23 months) mainly because of the difficulty to provide the high energy and nutrient inputs needed to sustain the child’s rapid growth during this period. 2 Given the long-lasting negative consequences of early childhood stunting, nutrition interventions targeting the first thousand days of life starting from conception are critical. 3
Inappropriate infant and young child feeding (IYCF) practices are among the major causes of stunting 4 and are determined by the availability of and accessibility to nutrient-dense foods, the mother’s knowledge, and prevailing cultural beliefs. 5,6 Previous studies have reported that nutrition education can improve mothers’ nutrition-related knowledge, 7 increase dietary diversity, 8 nutrient intake, 9 and hence the nutritional status of infants and young children. 10 Therefore, the provision of appropriately tailored nutrition education on recommended IYCF practices to mothers plays a vital role in the prevention of stunting.
However, the effectiveness of nutrition education programs depends on many factors including the knowledge and knowledge-sharing effectiveness (KSE) of health workers, 11 maternal knowledge acquisition, 12 and the resources available to enable mothers to apply the recommendations. Furthermore, complementary feeding is a complex set of behaviors that include the timing of the introduction of complementary food (CF), dietary diversity, feeding frequency, responsiveness to child cues, and the safe preparation and storage of foods. The understanding of each behavior by frontline health workers may vary and thus affect their KSE. To what extent this affects the knowledge of mothers and ultimately the nutritional status of their child is largely unknown.
In recent years, many countries have worked on developing health systems and infrastructure that provide essential services at decentralized level. Ethiopia’s health extension program (HEP), which was launched in 2003, is exemplary in this regard. The program provides universal access to primary health care including nutrition through more than 38 000 government-salaried female health extension workers (HEWs). The program operates nationwide and 2 HEWs are placed per health post to serve each kebele (smallest administrative unit ∼5000 habitants).
In Ethiopia, from 2005 to 2011 alone, child mortality dropped from 123 to 77 per 1000 live births, and stunting was reduced from 58% to 44%, 13 and these achievements would have been unlikely without the HEP. 14 Nevertheless, stunting rates are still very high and in some regions such as Amhara, they have not gone down as much as expected. This could partly be due to poor access to nutrition education, since nutrition is just 1 of the 16 modules that the HEWs should deliver and thus may not always be prioritized. It could also be due to the ineffective nutrition education in terms of the knowledge and KSE of the HEWs. However, limited studies are available in this regard partly because indicators for measuring IYCF were not in place until 2008 15 and also because much of the focus was on the accessibility to the program and little on what makes it effective. This is unfortunate, given that such information could improve the effectiveness of the programs that operate at scale and thereby contribute to the reduction in stunting.
In the present cross-sectional study, data were generated on mothers’ access to nutrition education, mothers’ and HEWs’ knowledge of key IYCF practices, and child anthropometry from Mecha district, West Gojam, Ethiopia, to evaluate mothers’ and HEWs’ knowledge of key IYCF practices and to investigate whether mothers’ knowledge and HEWs’ KSE are associated with stunting in young children (aged 12-23 months).
Materials and Methods
Study Site and Participants
The study was conducted in a food-secure district Mecha in West Gojam, Amhara region, Ethiopia. Although the district benefits from the HEP, the prevalence of stunting (52%) is very high and exceeds the national average (44%). 13 The inhabitants are predominantly subsistence farmers who grow maize (Zea mays L.), millet (Pennisetum glaucum), and pulses as food staples. Vegetables such as kale and potato are also grown. Teff (Eragrostis tef.) is also grown by many as a cash crop.
The participants of the present study were HEWs assigned to the district (n = 100) and mother–child pairs (n = 122) drawn randomly (through generation of random numbers) from the database of local health centers that was completed by a census conducted before the survey. All the HEWs assigned to the district except 4, who were new recruits, were included in the study. The selection criteria for including the mother–child pairs were the mother should have at least 1 child aged 12 to 23 months, has to be a permanent resident of the study area, and the child should be apparently healthy and aged 12 to 23 months.
The projected sample size was determined from power analyses calculated to detect a medium effect size (0.5 standard deviation difference between means [1-tailed], with an α of .05 and power of .80 to allow comparison of 2 groups in 1 or more of the outcomes considered [length-for-age z scores, LAZ; mean knowledge scores; dietary diversity; etc]). The estimated sample size was 102 (51 per group) and was increased to 120 to allow ∼15% nonresponse rate. The study was conducted from October to December 2013.
Sociodemographic and Anthropometric Measures
The sociodemographic characteristics of the mothers were assessed using a pretested questionnaire that included questions on livelihood activities, education level of parents, ownership of livestock, and the size of land owned. The socioeconomic status of the households was estimated by creating an asset index that was constructed by converting the available household resources such as livestock, size of land owned, and available household items (radio, chairs, etc) into their monetary value.
The length/height and weight of the children/mothers were measured in triplicate using standardized techniques, with children and mothers wearing light clothing and no shoes. All anthropometric measurements were made by the same person to avoid interexaminer errors. For the children, z scores for LAZ, weight-for-age z score (WAZ), and weight-for-length z score (WLZ) were calculated using World Health Organization (WHO) multicenter growth reference data 16 using the software ENA 2007. Stunting, underweight, and wasting were defined, respectively, as LAZ, WAZ, or WLZ <−2. Maternal body mass index (BMI) was calculated as weight (kg)/height (m2).
Health Extension Workers’ and Mothers’ Knowledge of Key IYCF Practices
Mothers’ and HEWs’ knowledge of key IYCF practices were evaluated using a questionnaire based on the Pan American Health Organization/ World Health Organization (PAHO/WHO) guiding principles for the complementary feeding of breast-fed children (PAHO/WHO 2003) and the WHO’s IYCF indicators. 17 The questions were divided into 3 sets: breast-feeding, complementary feeding, and hygiene. The questionnaires were pretested and the data were collected in face-to-face interviews with HEWs and mothers. A score of “1” was assigned for correctly answered questions and “0” for incorrectly answered questions. Mothers’ access to IYCF training through the HEP was documented by retrospectively asking whether or not they have received training. For each question, the scores obtained by mothers were compared to access to IYCF training and child stunting.
Health Extension Workers’ KSE
Health extension workers’ knowledge sharing was assumed to be effective if the knowledge of the trained mothers is concordant with that of the average score of the HEWs. The premise being that, under ideal knowledge-sharing practice by the HEWs, mothers should be able to attain the mean knowledge score of the HEWs. Accordingly, KSE and gap in KSE were calculated as follows:


Gap in KSE had a lower limit of 0, and values close to 0 indicated good KSE. The association between gap in KSE and the child’s LAZ was investigated.
Ethical Approval
Ethical approval was obtained from the human ethics committees of the College of Natural Sciences, Addis Ababa University, and the Amhara National Regional State Health Bureau. Verbal informed consent was obtained from the HEWs and mothers of each child after the purpose and methods of the study had been explained in detail and the consent forms read to them in the presence of local health community workers and kebele administrators. All questionnaire and consent forms were translated into Amharic before the survey.
Quality Control
Before the survey, all questionnaire and consent forms were translated into Amharic and were back translated to English by a certified translator to ensure the consistency and quality of the translation. The study employed 3 experienced data collectors who were at least diploma holders in nursing. The data collection was closely monitored by Z.A. who was the in-field supervisor of the survey. In addition, a 2-day intensive training followed by a pretesting of the questionnaires was conducted before the actual survey. Data collectors were not allowed to interview more than 5 caregivers per day. The completeness and accuracy of the data collected were checked on a daily basis. The questionnaires were double entered. All anthropometric measures were conducted by the same person.
Statistical Analyses
All continuous variables were checked for normality using the Shapiro-Wilk test. Descriptive statistics of continuous and categorical values were presented as mean ± standard deviation and in frequency counts or percentages, respectively. Differences in the proportion of HEWs and mothers who answered questions correctly were tested using χ2 and independent sample t test (1-tailed) for categorical and continuous variables, respectively. Bivariate correlation was run to investigate the association between LAZ and KSE. Partial correlation between LAZ and KSE, adjusting for maternal height, maternal education, and socioeconomic status, was also run. Parity and maternal age were not found associated with LAZ and thus were not adjusted for in the partial correlation. Differences were considered statistically significant for P values < .05. Statistical analyses were performed using SPSS statistical software package version 20.
Results
Sociodemographic Characteristics and Anthropometric Status
The sociodemographic characteristics of the mothers and the anthropometric measures of the mother–child pairs are presented in Table 1. The households’ profile is typical of a rural population whose main occupation is agriculture (93.4%). The mean age of the mothers was 26 years and the majority (63.1%) could not read and write. The average number of children per household was 3.8. Among the children, 50% were stunted, 34% were underweight, and 10% were wasted.
Sociodemographic Characteristics and Nutritional Status: Pairs (n = 122) of Mothers and Young Children Aged 12 to 23 Months in Mecha District, West Gojam, Northern Ethiopia, October to December 2013.
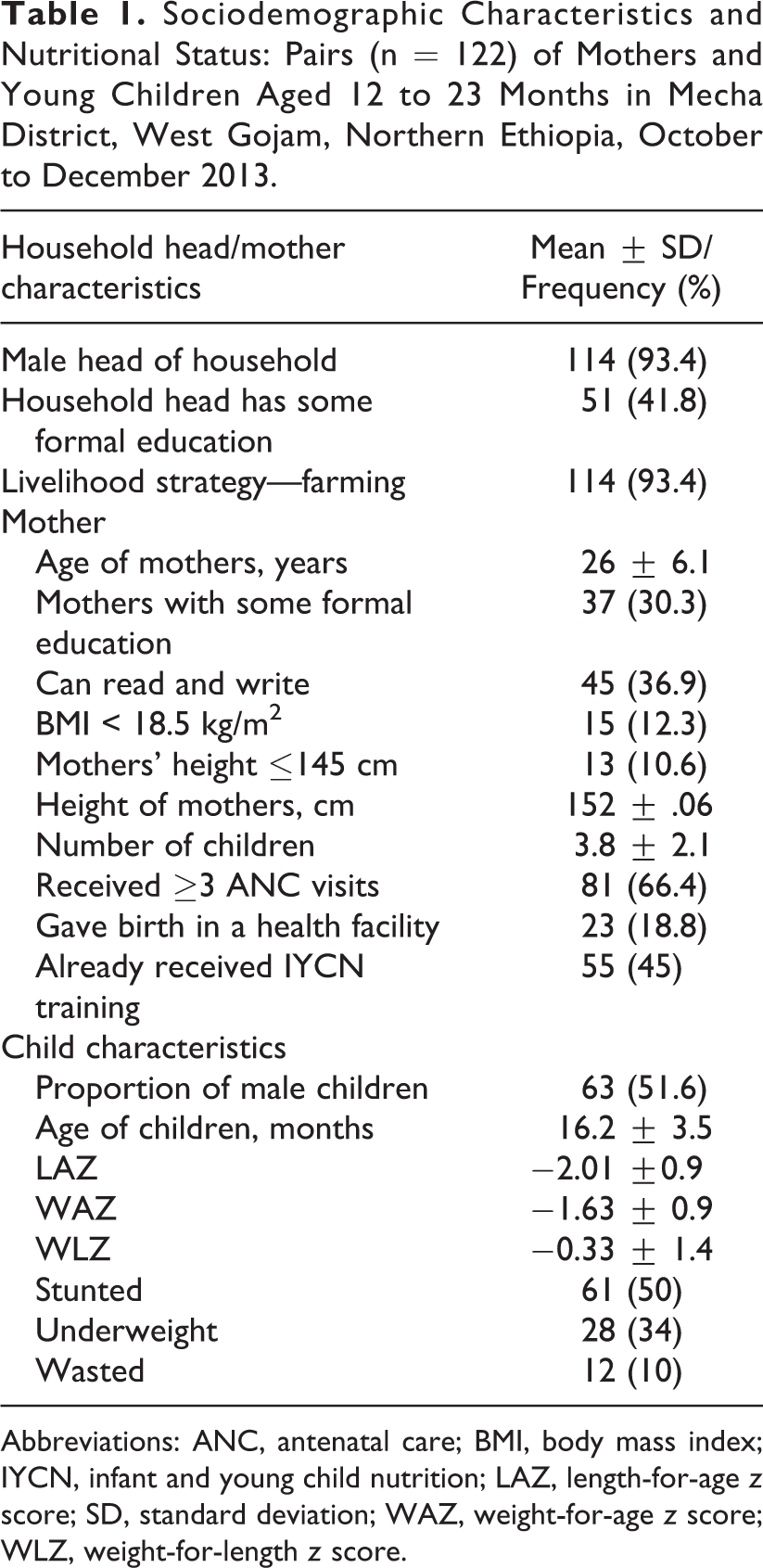
Abbreviations: ANC, antenatal care; BMI, body mass index; IYCN, infant and young child nutrition; LAZ, length-for-age z score; SD, standard deviation; WAZ, weight-for-age z score; WLZ, weight-for-length z score.
Health Extension Workers’ and Mothers’ Knowledge of Optimal IYCF Practices
Although 66.4% of the mothers received antenatal care ≥ 3 times, less than 20% delivered their babies in a health facility. Only 45% of the mothers declared they had received IYCF training and about 12% had a BMI of <18.5 (Table 1). Not surprisingly, a higher proportion of HEWs than mothers answered questions concerning optimal breast-feeding, complementary feeding, and hygiene correctly (P < .001; Table 2). Almost all HEWs (>95%) and 67% of the mothers answered questions related to optimal breast-feeding correctly, but fewer (50% of the HEWs and ∼40% of the mothers) knew the optimal duration of continued breast-feeding.
Proportion of HEWs and Mothers (Trained vs Untrained) Who Answered Questions on Optimal Infant and Young Child Feeding Correctly, and Child Feeding Practices in Mecha District, West Gojam, Northern Ethiopia, October to December 2013.
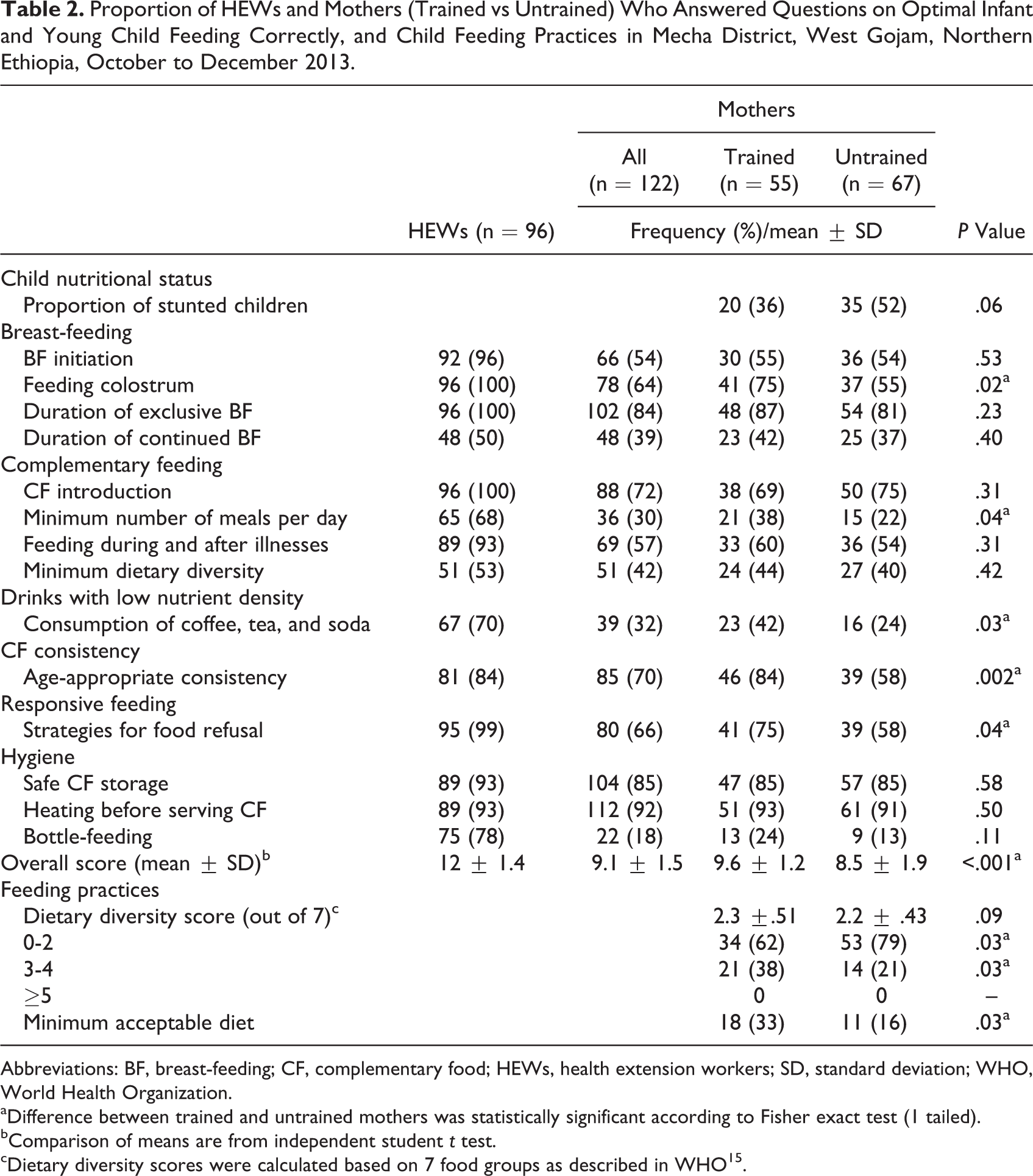
Abbreviations: BF, breast-feeding; CF, complementary food; HEWs, health extension workers; SD, standard deviation; WHO, World Health Organization.
aDifference between trained and untrained mothers was statistically significant according to Fisher exact test (1 tailed).
bComparison of means are from independent student t test.
cDietary diversity scores were calculated based on 7 food groups as described in WHO15.
Questions related to complementary feeding including questions on the optimal timing for introduction of CF, feeding strategies when a child refuses food, and feeding during and after illnesses were correctly answered by most HEWs, whereas those were correctly answered only by ∼70% of the mothers.
Concerning questions on optimal IYCF practices during the complementary feeding period (6-23 months), only 50% of the HEWs correctly answered questions on the optimal duration of continued breast-feeding, the minimum number of meals per day (68%), minimum dietary diversity (53%), and beverages not recommended for IYC such as sugary drinks and tea (70%). An even smaller number of mothers answered these questions correctly. On the other hand, the majority of the HEWs (88%) and mothers (65%) correctly answered most of the questions related to hygiene (Table 2).
Knowledge of Trained and Untrained Mothers
The average score of the trained mothers was significantly higher than that of the untrained mothers (Table 2; P < .001). However, training had more effect on the ability of mothers to correctly answer questions related to complementary feeding than those on breast-feeding or hygiene. Regarding questions on optimal breast-feeding, only the question on “feeding colostrum” was answered correctly by more trained than untrained mothers (P = .02). Questions on complementary feeding such as “minimum number of meals per day” (P = .04) and “age-appropriate consistency of CFs” (P = .002) were correctly answered by a significantly higher number of trained than untrained mothers (Table 2). In contrast, the proportion of mothers who correctly answered hygiene-related questions was similar irrespective of the mothers’ access to training.
Child Feeding Practices and Nutritional Characteristics in Relation to Mothers’ Training and Knowledge of Optimal IYCF
A significantly higher proportion of children of trained mothers met the minimum (≥3) dietary diversity requirements (P = .03). Although the dietary diversity of the children was low (0-2), a significantly higher proportion of children of untrained mothers had low dietary diversity (P ≤ .03). Untrained mothers had a higher proportion of stunted children (52%) than trained mothers (36%; P = .06).
Overall, mothers with a not stunted child had a significantly higher mean score than those with a stunted child (P < .001; Table 3). A significantly higher proportion of mothers with a not stunted child than mothers with stunted child correctly answered questions related to optimal duration of exclusive breast feeding (P = .03), minimum number of meals per day (P = .02), strategies when food is refused (P = .007), feeding during and after illnesses (P = .04), minimum dietary diversity (P = 009), age-appropriate consistency of CFs (P = .03), and proper storage of CFs (P = .02).
Proportion of Mothers (%) With Stunted and Not Stunted Children Who Correctly Answered Questions on Optimal Infant and Young Child Feeding and Their Feeding Practices in Mecha District, West Gojam, Northern Ethiopia, October to December 2013.
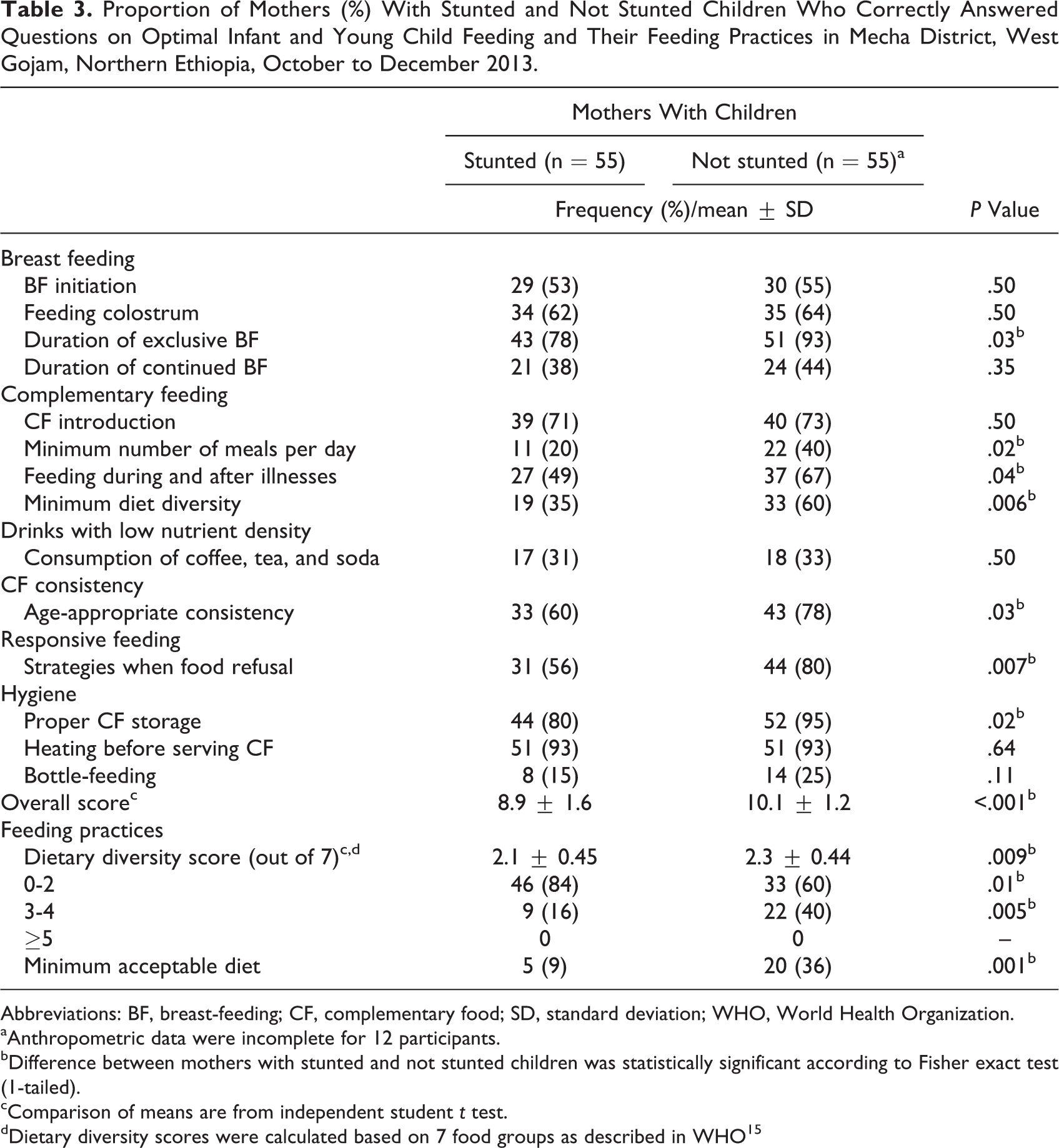
Abbreviations: BF, breast-feeding; CF, complementary food; SD, standard deviation; WHO, World Health Organization.
aAnthropometric data were incomplete for 12 participants.
bDifference between mothers with stunted and not stunted children was statistically significant according to Fisher exact test (1-tailed).
cComparison of means are from independent student t test.
dDietary diversity scores were calculated based on 7 food groups as described in WHO15
Health Workers’ KSE
The gap in KSE was inversely associated with the child’s LAZ (r 2 = −.475, P < .001) and remained significant after adjusting for variables like maternal height, maternal education, and socioeconomic status that were not affected by the HEP training but were significantly associated with LAZ (r 2 = −.423, P = .002; Figure 1).
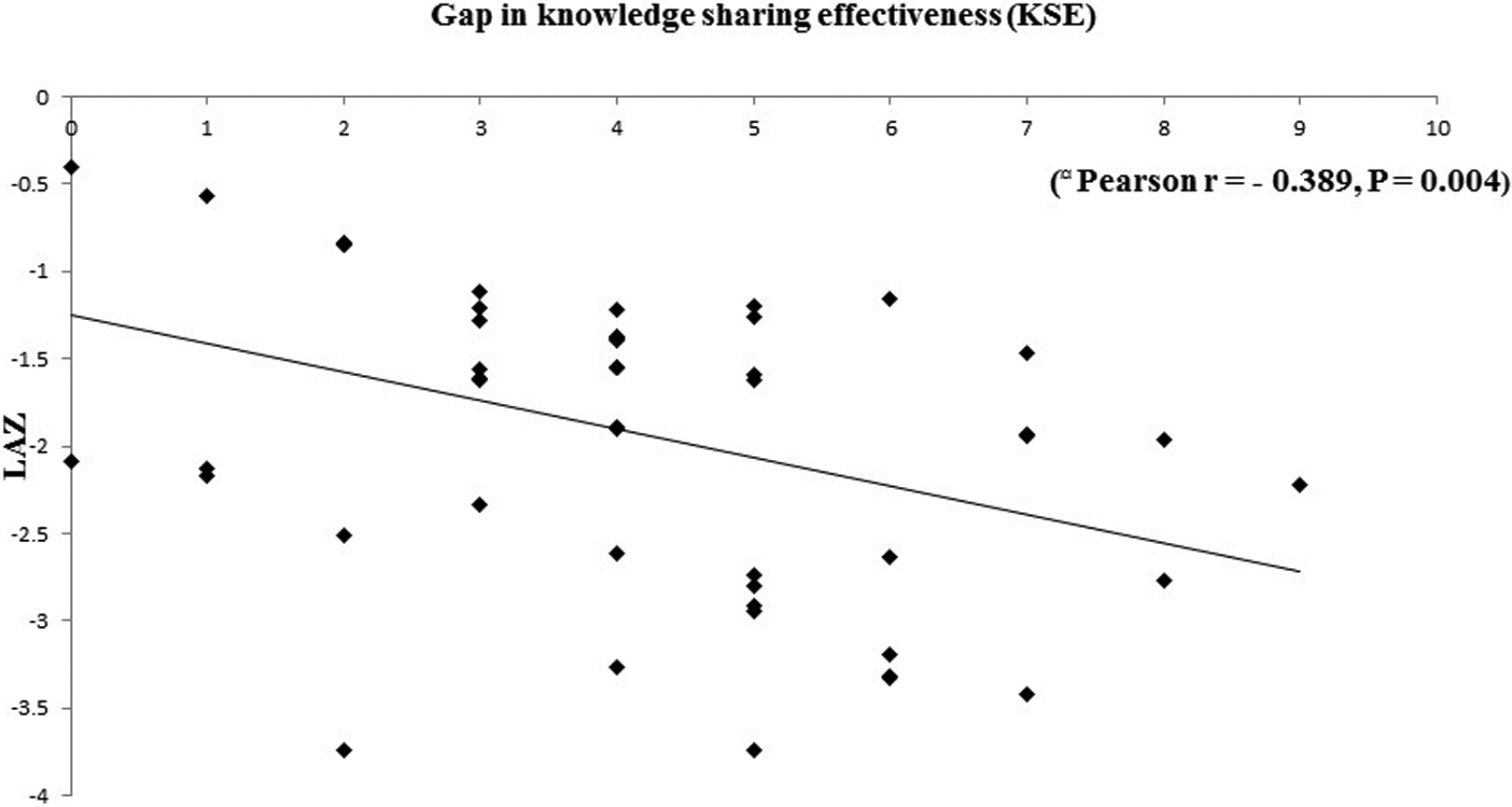
Association between the gaps in the health extension workers’ (HEWs) knowledge-sharing effectiveness (KSE) and the linear growth of children of mothers trained by the health extension program (HEP). Pearson correlation coefficients and P values are those from a bivariate (unadjusted) correlation. Correlations remained significant after adjusting for maternal height, maternal education, and socioeconomic status (r = −.396, P = .005).
Discussion
The present study investigated mothers’ and HEWs’ knowledge of key IYCF practices and its association with child anthropometric outcomes, in Mecha district, West Gojam, Ethiopia. The study showed that a significant proportion of the mothers have not had access to training on IYCF, but those who had, had better IYCF knowledge and practice. The study also revealed that certain key IYCF recommendations such as minimum duration of continued breast-feeding, minimum dietary diversity, and minimum acceptable meal frequency were not well understood by the HEWs. This affected the effectiveness of the knowledge transfer to mothers and was associated with child stunting.
Stunting remains highly prevalent in most developing countries like Ethiopia and poor IYCF practices are partly the cause. 18,19 Thus, the provision of nutrition education on optimal IYCF practices through the HEP could improve IYCF practices, especially in rural communities like Mecha where the HEWs are often the only source of nutrition information. Trained mothers had higher knowledge scores and better child feeding practices (Dietary diversity score and minimum acceptable diet) than untrained mothers. They also tended to have a lower proportion of stunted children. There is growing evidence that improving the accessibility to and quality of nutrition education through health services can increase both mothers’ knowledge and child’s dietary intake, both of which can reduce the prevalence of child stunting. 9,11 Unfortunately, more than half of the mothers did not have access to IYCF training through the HEP. This highlights the need to increase the accessibility to nutrition education provided through the HEP.
One key to improving the quality of the IYCF training is to increase the HEWs’ knowledge. Across the globe, the quality of health workers’ knowledge of nutrition has been a concern. 20,21 Similarly, the present study showed that not all aspects of the IYCF were equally understood. A significant proportion of the HEWs had difficulty correctly answering questions related to the minimum duration of continued breast-feeding, minimum dietary diversity, and minimum meal frequency. This is unfortunate because these feeding practices are intimately linked to linear growth. For instance, Jones et al 22 showed that dietary diversity and overall diet quality were positively associated with height-for-age z-scores (HAZ) in many countries, including Ethiopia. Although the knowledge of key IYCF practices was higher in trained than in untrained mothers, this depended on the knowledge of the HEWs. Therefore, improving the HEWs’ understanding of such recommended IYCF practices should be a priority in future refreshment training courses.
A considerable knowledge gap between the HEWs and the trained mothers was observed concerning some key IYCF recommendations, even those recommendations about which the HEWs were found to be knowledgeable. The way IYCF messages are conveyed, the education level of mothers, the cultural acceptability/adoptability of the messages, the frequency of the training provided are all factors that can affect the outcome of the targeted behavioral change. 23,24
One remarkable finding is that this gap in KSE was negatively associated with linear growth. Our findings are in line with recent findings in Haiti, showing that the outcomes of behavioral change communications depend on both the knowledge and the knowledge-sharing efficacy of frontline health workers. 11 This suggests that besides working to increase the knowledge of the HEWs, it is equally important to strengthen their knowledge-sharing efficiency through process training. This is especially needed for aspects of IYCF such as optimal timing for breast-feeding initiation, optimal timing for introduction to complementary feeding, feeding during and after illnesses, and avoiding beverages not recommended for IYC, about which a large knowledge gap was observed between HEWs and mothers.
Given that mothers with a stunted child had a significantly lower knowledge score than those whose child was not stunted (P < .001), increasing the effectiveness of the IYCF training provided through the HEP could also be an effective strategy to prevent stunting.
The cross-sectional nature of the present study does not allow causal inferences regarding the association reported in this study. The study focused on HEWs’ and mothers’ knowledge and their association with child stunting, but we recognize that knowledge does not always lead to practice. However, we included a few practice-related questions that, considering the age of the child at the time of the survey, were found to be relevant. We recognize that the IYCF knowledge of trained mothers can be affected by the HEWs’ knowledge; this can be a potential confounding factor in some of our comparisons between trained and untrained mothers. The present results came from a single district in West Gojam and thus cannot be extrapolated to all mothers and HEWs in West Gojam, Ethiopia. Nevertheless, the findings of this study may apply to other similar settings, both in Ethiopia and elsewhere, and contribute to the limited body of literature on implementation and utilization of nutrition education interventions.
Conclusion
The present study highlighted that access to training on IYCF through the HEP was associated with higher mothers’ knowledge score. Unfortunately, IYCF training was not accessible to all mothers and when accessible, its effectiveness depended on the HEWs’ level of knowledge and understanding of key IYCF recommendations. Maternal knowledge of optimal child feeding was positively associated with dietary diversity and linear growth. Improving mothers’ access to IYCF training along with efforts to increase the HEWs’ knowledge and strengthening their KSE may improve feeding practices and prevent stunting.
Footnotes
Authors’ Note
All authors were involved in developing the study design. Z.A. and K.B. looked for funding. Z.A. coordinated and supervised the fieldwork. Z.A. and K.B. analyzed and interpreted the data. Z.A. wrote the first draft of the manuscript. All the authors contributed to manuscript preparation.
Acknowledgments
The authors thank all of the children and families who took part in this survey, and all the dedicated data collectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the German Academic Exchange Service (DAAD), Germany, Addis Ababa University, and Ambo University. The funding was only for the data collection and thus does not cover authorship or publication fees.