
Abstract
Background:
The coexistence of underweight and overweight (double burden) remains a major problem in many developing countries. Little is known about the factors associated with the double burden of malnutrition in Palestinian children.
Objective:
To assess factors associated with undernutrition and overnutrition in 1500 schoolchildren aged 5 to 16 years, in the West Bank.
Methods:
We surveyed a sample of 22 schools run by the United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) and the Palestinian government. Binary logistic regression was used to examine the factors associated with malnutrition. The hunger index, a composite score from 8 questions, was used to measure food insecurity.
Results:
In the 1484 children enrolled in UNRWA and government schools in the West Bank, the prevalence of stunting was 7% and underweight 3%. Around 12% of students were overweight and 6% obese. The hunger index was negatively associated with height for age. Factors associated with being underweight were male sex, mother being unemployed, and households not having enough food to eat for at least 2 days in the previous month. Factors associated with obesity were older age and time spent watching television. When overweight and obesity were combined in the analysis, they were inversely associated with increasing number of days spent playing sports.
Conclusion:
Our results show that the important nutritional risks for school-age children in the West Bank would seem to be the simultaneous occurrence of undernutrition and obesity. The study highlights the need to balance obesity management and prevention with interventions to tackle undernutrition.
Introduction
Optimal growth and development of children is a basic human right and a clear objective of health-care systems. 1 Globally, between 20% and 75% of child deaths are attributable to underweight and stunting, with the majority of deaths associated with malnutrition occurring in children who are marginally malnourished. 2 On the other hand, overweight and obesity represent serious health challenges worldwide and their prevalence is increasing at an alarming rate. The worldwide prevalence of obesity has nearly doubled between 1980 and 2008. In 2008, 10% of men and 14% of women in the world were obese, compared with 5% of men and 8% of women in 1980. 3 It is estimated that by the year 2015 noncommunicable diseases associated with obesity will surpass malnutrition as the leading causes of death in low-income communities. 4 Long periods watching television or using the Internet, physical inactivity, food advertisements, high intake of fast foods, and an increase in food intake outside the home are among the factors associated with obesity among children and adolescents. 5 Overweight and obese children are likely to be obese in adulthood and more likely to acquire noncommunicable diseases such as diabetes and cardiovascular risk factors at a younger age. 6
Despite this background, there is a dearth of systematic data on the nutritional status of Palestinian school-age children to guide plan for health and nutrition interventions in Palestinian communities. To our knowledge, previous studies only looked at adolescents 7 or preschoolers. 8 –12 There are no studies to examine malnutrition among 5- to 6-year-old children when they first enter school. 6 –8 The previous study assessed double burden among adolescents 13 to 15 selected from limited geographical areas, involving 2 governorates in the middle and south of West Bank out of the 12 West governorates. 6 The overall objective of this study is to assess the double burden of undernutrition and obesity among schoolchildren and the associated factors.
Methods
Description of Target Population and Sampling Design
The projected number of Palestinians living in State of Palestine at the end of 2015 is 4.75 million: around 2.90 million reside in the West Bank and 1.85 million in the Gaza Strip. Refugees make up 42.8% of the Palestinian population in Palestine: 27.1% of them in the West Bank and 67.3% in Gaza Strip. 13 In 2013, children constituted about 47% of the total population in Palestine: 45% in the West Bank and 51% in the Gaza Strip. 14
In September 2000, restrictions were imposed on the movement of Palestinian goods and people across borders and within the Palestinian territory. In 2013, 33% of Palestinian households were food insecure. 15 In the West Bank, the rates of stunting in children under 5 rose from 7% in 1996 to 11% in 2010. 16 Recently, the increasing rates of obesity, diabetes, and cardiovascular diseases have been observed among Palestinian adults. 17
In 2009, a cross-sectional school-based survey was conducted among a sample of West Bank students randomly selected from United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) and government schools, the 2 main providers of free education in Palestine and serving more than 85% of students. 18,19 The UNRWA provides free schooling for all refugee children. 18,19 For the school sample, the West Bank was arbitrarily divided into 3 geographic areas, north, middle, and south, each accounting for approximately one-third of the total population of schoolchildren. Within each area, government and UNRWA schools with at least 50 students, both girls and boys, in 3 selected grades were selected for study.
The lists of students attending the UNRWA and government schools were stratified by region, sex, and school year (grade). We used one-sample proportion tests to calculate the sample size required to report prevalence data (ie, percentage of first graders with stunting), with 80% of power for a preset type 1 error of 5% for the main variables to be investigated. Our analysis returned a required sample size of 500 for each of the 3 age-groups included in the study: first grade (mean age 6.71 years, standard deviation [SD = 0.45]), sixth grade (11.82 years [0.57]), and ninth grade (14.83 years [0.61]).
The intention was to select 6 government schools and 6 UNRWA schools covering the north, middle, and south regions of the West Bank and to randomly select 42 students from each grade and class to form 504 (42 × 12) students from each grade (252 boys and 252 girls). We randomly recruited students from 16 UNRWA schools instead of 6, because we selected 2 camps from each region; and as in some UNRWA schools, the elementary school is separated from preparatory, so we selected 4 schools instead of 2. Therefore, we ended up with a source population of 22 schools (6 government and 16 UNRWA schools out of 1555 UNRWA and government schools).
In the initial design, the intention was to randomly select 42 students from each grade in government schools. However, some government schools did not actually have this number of students (the lists were not accurate), and we selected 681 students from government schools instead of 756 students. We randomly selected 819 students from UNRWA schools to make the required total of 1500. The response rate was 99% and the final number of students was 1484. Siblings were excluded; 1 student per household was selected to avoid clustering.
Field workers visited participating schools and took 2 measurements of the standing height and weight (lightly dressed but removing shoes) of each study index. If the difference between the 2 measurements was more than 10%, they took a third measurement. Mothers were invited to attend to their children’s schools and were asked to provide information on sociodemographic characteristics and to complete the student survey on behalf of their children in first grade. Sixth and ninth graders were asked to fill in a student survey that collected information on physical activity and the number of hours spent watching TV among other variables. Columbia University’s Institutional Review Board, New York, and Al-Quds University, Jerusalem, Palestine, approved the study protocol in December 2008. Written informed consent and assent were obtained from sixth- and ninth-grade students and their parents.
Variables
Stunting, underweight, overweight, and obesity
Stunting is defined as height-for-age standardized scores below 2 (HAZ < −2). The World Health Organization (WHO) ANTHROPlus program was used in the analysis of the anthropometric data to compute the standardized sores. 20 World Health Organization ANTHROPlus is based on the WHO 2007 reference population where data were pooled from 6 countries unlike the earlier reference data that were based on the US data. 20 The body mass index (BMI) was defined according to age- and gender-specific cutoff values reported as per the 2000 growth charts of the Centers for Disease Control and Prevention (CDC), Atlanta, Georgia, and height and weight measures as per WHO standards. 21 The US 2000 CDC growth charts were used to examine BMI as it was found to be appropriate for use in the developing countries. 22 Underweight was defined as BMI <5th percentile, overweight as BMI >85th percentile, and obesity as BMI >95th percentile. 23
Child and household measures
The main child explanatory variables were age, gender, birth order and birth weight, days per week student engaged in sports, and time spent watching television or videos per day. Maternal factors included education and employment; household factors such as family size and average monthly income, the household having insufficient money for living expenses in the month prior to the survey, the family not having enough food to eat for at least 2 days in the previous month, and the occurrence of hunger as measured by hunger index.
Child age: The age of the child in months completed was calculated from the date of birth taken from school records.
Days per week student engaged in sports: This was measured as the number of days the student exercised for at least 60 minutes in the previous week as reported by student.
Maternal education: This was measured as years of schooling and coded into 6 categories: never been to school, completed up to sixth grade, completed seventh grade to high school, intermediate college, university, master’s/PhD degrees.
Hunger questionnaire: Hunger was measured using the hunger scale of the Community Childhood Hunger Identification Project.
24
The scale consists of 8 items. Food insecurity is indicated by 5 or more positive responses. The hunger index was calculated by adding the following 8 binary items (yes = 1, no = 0) on household food deprivation in the month prior to the survey: Does your household ever run out of money to buy food? Do you ever rely on a limited number of foods to feed your children because you are running out of money to buy food for a meal? Do you ever cut the size of meals or skip a meal because there is not enough food in the house? Do you ever eat less than you should because there is not enough money for food? Do your children ever eat less than you feel they should because there is not enough money for food? Do your children ever say they are hungry because there is not enough food in the house? Do you ever cut the size of your children’s meals or do they ever skip meals because there is not enough money to buy food? Do any of your children ever go to bed hungry because there is not enough money to buy food?
Statistical Analysis
SAS software was used for analysis. Means and percentages were used to describe the characteristics of the study sample. The student t test and 1-way analysis of variance were used to examine group differences in playing sports and hours watching TV. Multivariate linear regression was used to examine factors associated with height for age. Binary logistic regression was used to examine factors associated with underweight, overweight and obesity combined, and obesity.
Results
The response rate was 99% (1484/1500). The average size of the household was 7.8 individuals and average monthly income was US$508. Almost 88% of the mothers in the study were housewives with about 80% of them having up to or below high school education. On average, the students played sports for at least 60 minutes for 2 days a week and watched television or video for about 3 hours per day (Table 1). In the higher grades, the amount of sports per week decreased and hours watching TV during weekdays and on Fridays increased (data not shown). Girls spent more time than boys watching TV, mean (SD): 3.1 (1.9) vs 2.8 (2.1), respectively; P = .009.
Characteristics of the Study Sample, West Bank, Palestine.a
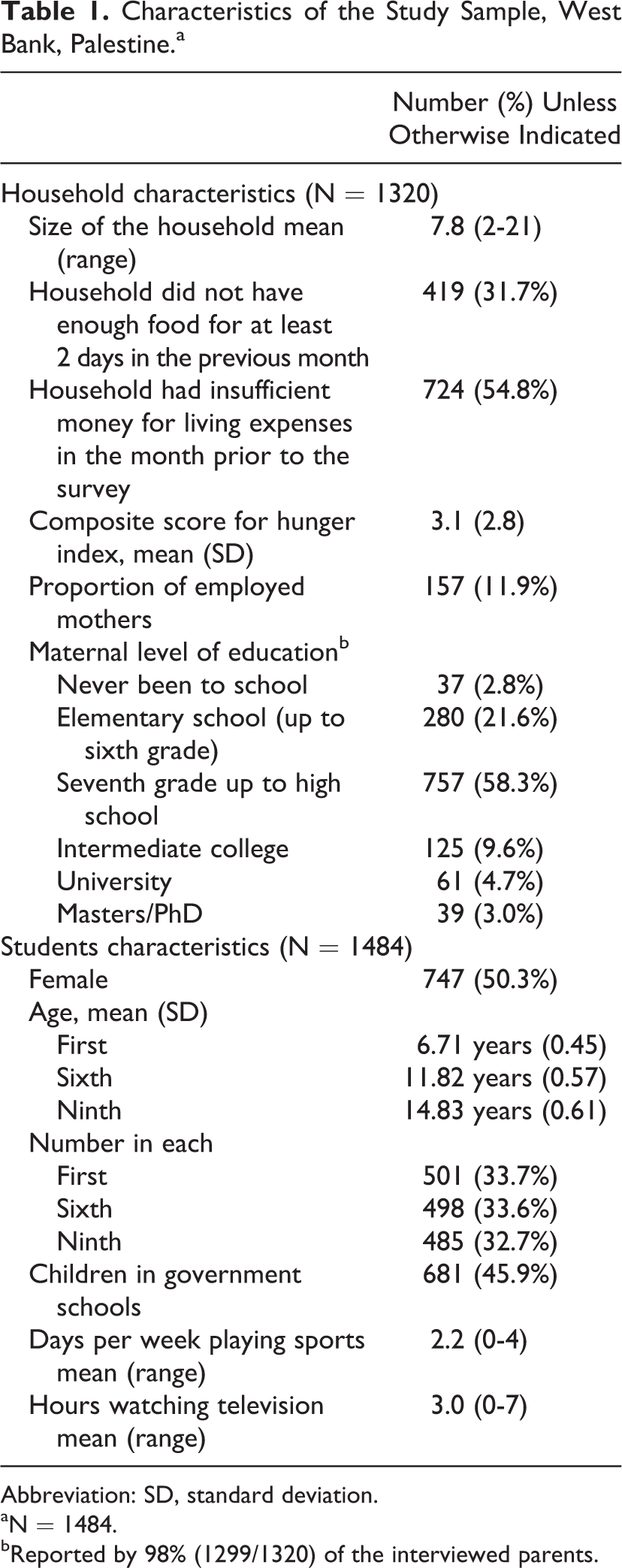
Abbreviation: SD, standard deviation.
aN = 1484.
bReported by 98% (1299/1320) of the interviewed parents.
Based on the hunger questionnaire, more than 50% of households ran out of money to buy food in the month prior to the survey. They relied on a limited number of foods to feed their children because there was insufficient money to buy food for a meal or cut the size of meals or skipped meals because there was not enough food in the house (Table 2). About 44% of the mothers reported eating less than they should because there was not enough money for food. Based on the reports by mothers, 23% of the children complained of hunger because of insufficient food in the house and 17% went to bed hungry.
Responses to Hunger Questionnaire, West Bank, Palestine.a
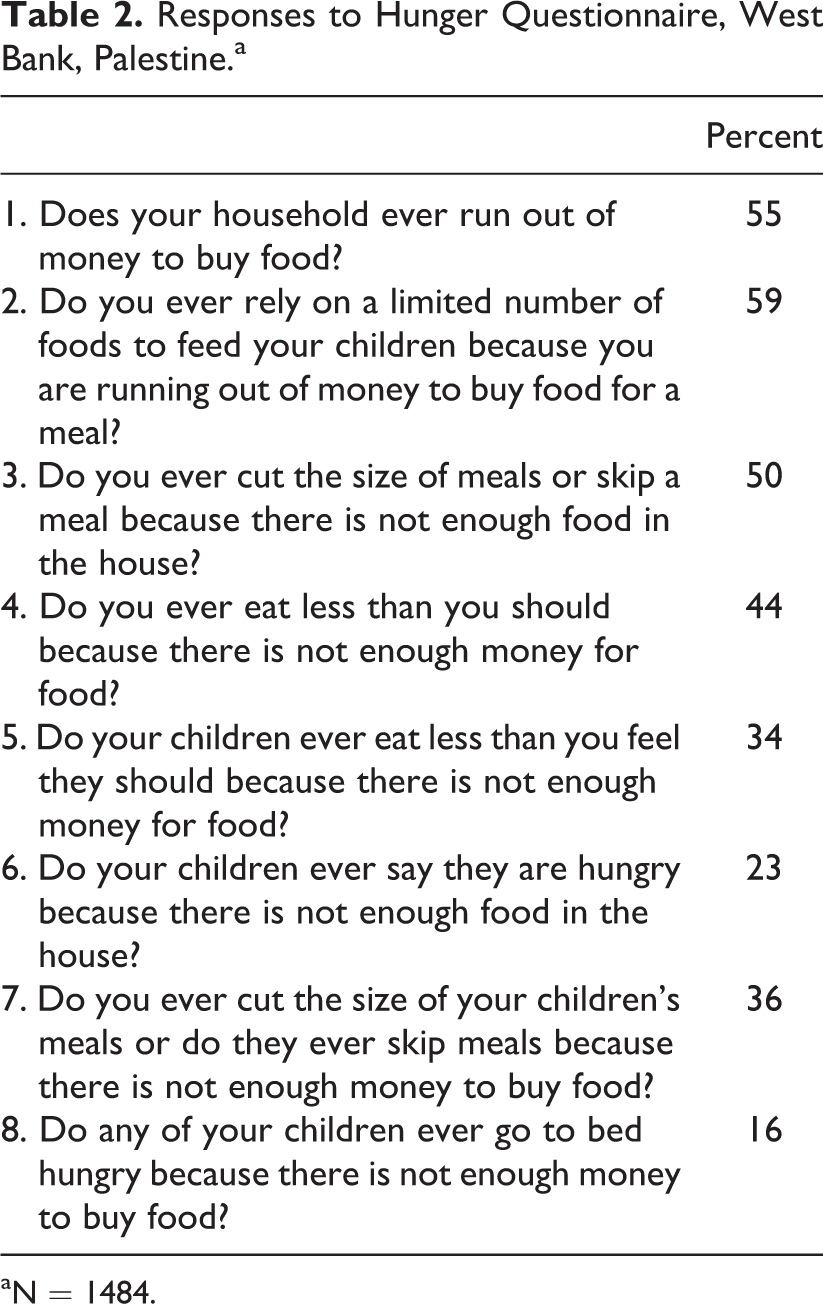
aN = 1484.
Undernutrition and Obesity
The prevalence of stunting was 7% (97/1484) and of underweight 3% (49/1484). Across districts, stunting was between 4% and 11%, and underweight was between 2.5% and 4.2%.
Overweight was found in 180 (12%) of 1484 students, and 86 (6%) of 1484 students were obese (Table 3). Across districts, overweight ranged from 11% to 16%, and obesity was between 3.4% and 11%. There were no differences between children in UNRWA and government schools in stunting (52 [7%] of 772 vs 45 [7%] of 674; difference 1.0, 95% confidence interval [CI] 0.7-1.4), underweight (25 [3%] of 771 vs 24 [4%] of 673; 0.9, 95% CI 0.5-1.6), and overweight (99 [13%] vs 81 [12%]; 1.1, 95% CI 0.8-1.4). Obesity was more prevalent in UNRWA schools than in government schools (56 [7%] vs 30 [4%]; 1.6, 95% CI 1.1-2.5).
Prevalence of Undernutrition and Overweight/Obesity Among a Sample of Palestinian Children by Gender and Grade in West Bank, Palestine.a
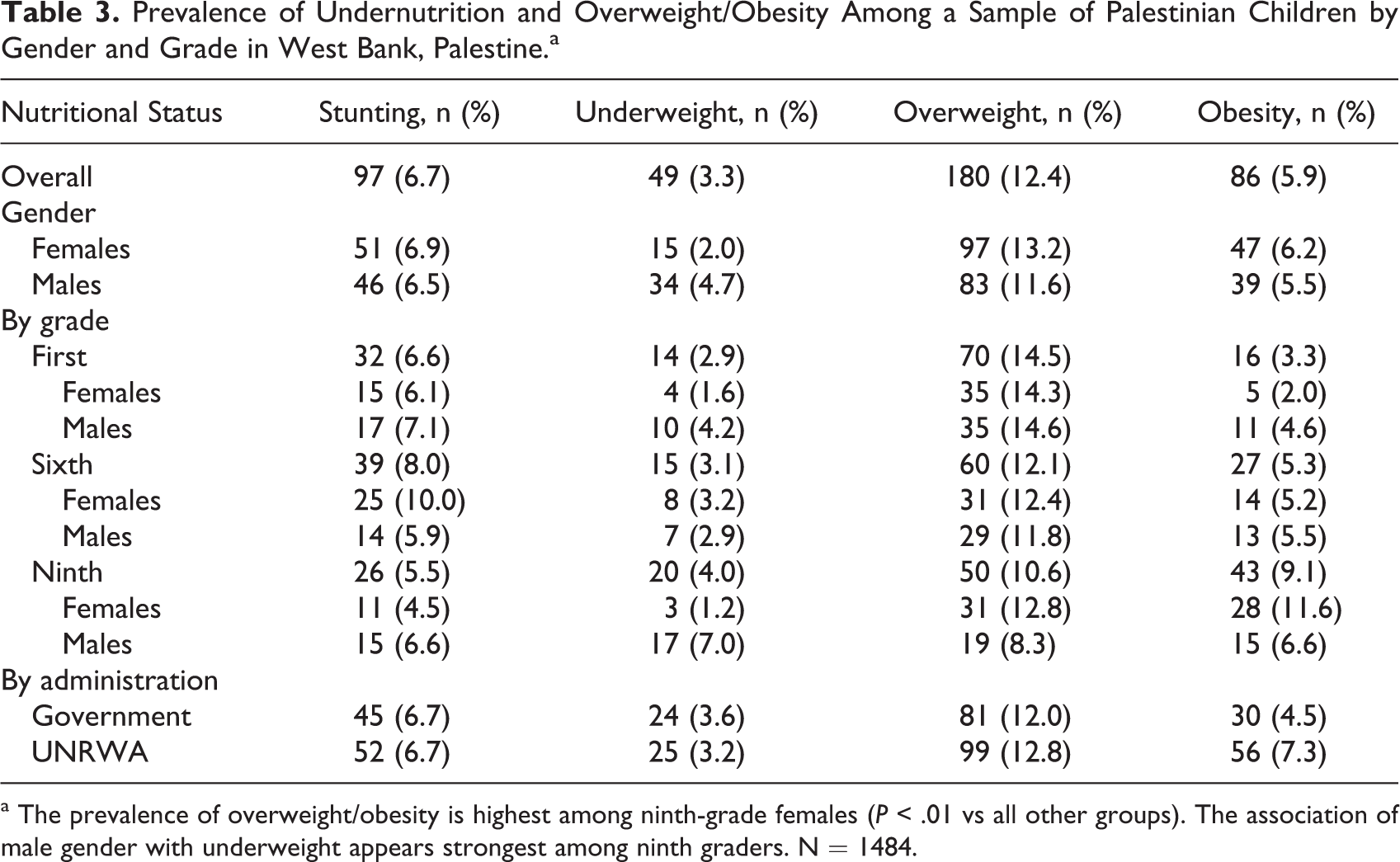
a The prevalence of overweight/obesity is highest among ninth-grade females (P < .01 vs all other groups). The association of male gender with underweight appears strongest among ninth graders. N = 1484.
Factors associated with undernutrition and overweight/obesity
The hunger index was negatively associated with height for age (P = .018). Factors associated with underweight were being of male sex (odds ratio 2.8, 95% CI 1.5-5.3), mother being unemployed (3.0, 95% CI 1.0-8.4), and households not having enough food to eat for at least 2 days in the previous month (1.8, 95% CI 1.0-3.3). Based on the study findings, physical activity was not associated with obesity. When overweight and obesity were combined in the analysis, they were significantly and inversely associated with an increase in the number of days spent playing sports (0.9, 95% CI 0.8-1.00; Table 4).
Factors Associated With Overweight and Obesitya Among a Sample of Palestinian Schoolchildren in West Bank, Palestine.b
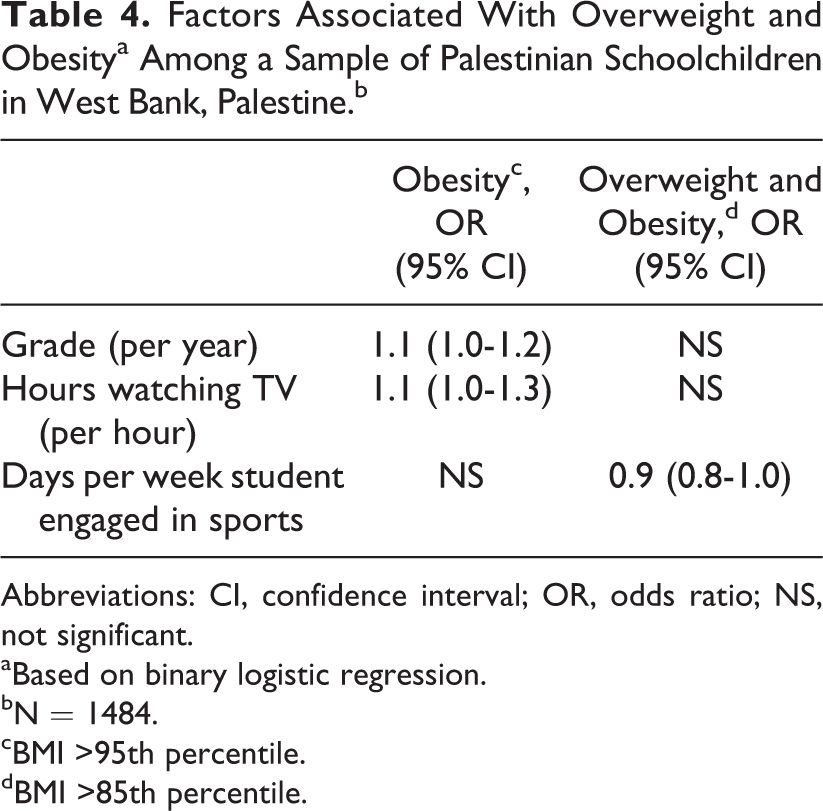
Abbreviations: CI, confidence interval; OR, odds ratio; NS, not significant.
aBased on binary logistic regression.
bN = 1484.
cBMI >95th percentile.
dBMI >85th percentile.
Discussion
Our observations in this study clearly point to the fact that the important nutritional risks for school-age children in the West Bank would seem to be the simultaneous occurrence of undernutrition and obesity. Underweight was mostly prevalent among ninth graders (14-16 years), a phenomenon that may partly be explained by increases in physical growth and accelerated development, which lead to greater total energy and nutrient needs than younger children, especially among males. 23 Food insecurity was associated with undernutrition; hunger with stunting and underweight with households not having enough food for at least 2 days in the previous month. Maternal unemployment increased the likelihood of the child being underweight by 3-fold. Based on a recent national labor force survey, the female labor force participation rate in Palestine is 18.8% compared with 72.1% for males. 25 Contrary to previous studies, 26,27 our data did not demonstrate an association between birth order, birth weight, size of household, or maternal education and malnutrition among schoolchildren.
On admission to school at a young age (5-6 years), the prevalence rates of overweight and obesity among children in our study were low, but by ninth grade (14-16 years) these conditions are clearly observed. Among ninth graders (14-16 years), overweight and obesity were more prevalent among girls than among boys; this may partly be explained by the marked decrease in physical activity by girls when entering adolescence, in addition to hormonal changes that make girls more prone to weight gain, and an increase in fat mass. 28 The prevalence of overweight and obesity among study participants matches findings from previous studies in Arab countries in which 18% to 46.9% of male schoolchildren aged 6 to 18 years were reported to be overweight or obese and from 17.6% to 46.9% of female schoolchildren. 5
In the present study, children watched television or videos for about 3 hours per day. The American Academy of Pediatrics recommends that parents limit the time spent by their children in such activities to 2 hours per day. 29 The study found that girls spent more hours watching TV than boys did, and ninth-grade students spent more hours watching TV than first- and sixth-grade students did. In addition, ninth-grade students spent fewer days per week playing sports than those in first and sixth grades. This matches a previous study of obesity among children in the Arab world. 5
Physical inactivity was positively associated with obesity (measured by hours of television watched) and with overweight and obesity combined (measured by days per week in which students engaged in sports). Parallel findings in a US study in Texas among students of grades 4, 8, and 11 showed a combined effect of high levels of television watching and low physical activity on the risk of obesity in children and adolescents. 30 The number of hours playing sports became a significant factor when obesity and overweight were combined and this may be due to the increased power to detect significance. The association between physical activity and obesity may also be in part explained by reverse causation, that is, children do not play sports because they are overweight and obese. However, longitudinal studies of 1-year interventions based on diet and physical activity showed a reduction in BMI among children and adolescents by the end of the intervention. 31,32
Many researchers have described obesity, many more undernutrition, but few have described what we are writing about, the coexistence of these 2 conditions. The Palestinian situation may be a model for the study of both undernutrition and obesity since these conditions occur in the same population at the same time. This is an important topic for further studies on issues of causality that could not be addressed with certainty in this cross-sectional study. Our study identifies modifiable risk factors for both overweight and obesity, and for malnutrition, in children exposed to political unrest and food insecurity, physical inactivity, and maternal unemployment. Although overweight and obesity were found to be more prevalent than stunting and low weight in the present study, undernutrition is still a health priority in view of its negative long-term impact on growth and development. We must continue our work on reducing undernutrition while simultaneously preventing overnutrition through integrated child health programs that incorporate prevention of infection, diet quality, and physical activity. 33
The cross-sectional design of the study precludes an examination of causality. Other limitations are that physical activity and the hours watching TV were self-reported; the lack of observational or quantitative detail limited our ability to conduct more specific and objective analyses. Another limitation is that we only examined children from government and UNRWA schools and excluded those from private schools. Thus, the study targeted children in schools that provide free education and who are more likely to be less privileged and more at risk of malnutrition, about 86% of schoolchildren in the West Bank. Finally, schools were not randomly selected from all government and UNRWA schools. They were selected from different regions of the West Bank and students were randomly selected from each school. Therefore, we believe our sample can be generalized to schoolchildren attending UNRWA and government schools in the West Bank.
The findings of the present study point to both fundamental underlying factors and secondary issues that have a strong bearing on the growth, development, and well-being of young children and adolescents. The findings in the present study provide a basis for the revision of child and family-oriented policies and programs, even in areas of conflict where populations are exposed to food insecurity. Despite the conditions of prevailing stress, it is vital to target food insecurity, support long-term income-generating projects, increase the proportion of women in the labor market, increase local food production, and promote child health, with focus on increasing awareness and encouraging changes to sedentary lifestyles. “Low and middle income countries should target both undernutrition and growing rates of overweight and obesity, even if they are not yet of public health importance. Without stronger nutritional governance, policies alone may not be enough to address the growing threat of nutrition transition.” 34
Footnotes
Acknowledgement
We are grateful for helpful comments from Dr. Wahida Karmally, Columbia University.
Authors’ Note
All authors were responsible for the study design, data gathering, interpretation of the results and writing. S.M., S.H., and R.J.D. contributed to the data analysis. All authors have read and approved the final paper for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from UNRWA, UNICEF, Juzoor for Health and Social Development, and the Institute of Human Nutrition, Columbia University.