
Abstract
Objective
This study aimed to evaluate the prevalence of sarcopenia and malnutrition among patients undergoing elective operations and the associated factors.
Methods
A cross-sectional study design was used to analyze data collected from 111 participants (60 males and 51 females) aged ≥50 years. The European Working Group on Sarcopenia in Older People criteria were used to define sarcopenia; anthropometric measurements, body composition data, and Mini Nutritional Assessment-Short Form questionnaire responses were used to assess the nutritional status of the participants.
Results
The prevalence rates of malnutrition and sarcopenia were 34% and 39%, respectively, in the study population. In addition, we found that malnourished patients were more likely to be female, unemployed, diabetic, and dyslipidemic. The study also showed that patients with sarcopenia were more likely to be older and have diabetes.
Conclusions
Malnutrition, diagnosed using the Mini Nutritional Assessment-Short Form questionnaire, is associated with sarcopenia, female sex, working condition, diabetes, and dyslipidemia. A significant association was reported between sarcopenia, age, and diabetes.
Introduction
Sarcopenia has been recognized as a progressive and generalized skeletal muscle disease that includes the accelerated loss of muscle mass and function. 1 This condition is associated with an increased risk of adverse outcomes involving frailty, functional decline, falls, and mortality. 2 The European Working Group on Sarcopenia in Older People (EWGSOP) has stated that sarcopenia can be diagnosed if the patient has low lean muscle mass along with either low physical performance or reduced muscle strength. 3 The global estimates of sarcopenia prevalence in older patients vary from 3% to 30% according to the operational definition implemented and the study settings. 4
Malnutrition is recognized as a condition characterized by deficiency in energy and nutrient supply with negative effects and measurable consequences. 5 Nutritional status plays an important role in health and recovery from illness or injury. Several studies have shown significant correlations between the severity of nutritional deficiencies and a higher risk of related morbid events among the hospitalized older patients and revealed an approximately 30%–50% incidence of malnutrition among hospitalized population. 6
Malnutrition and sarcopenia are present in parallel and often manifest clinically as a combination of disease burden, inflammation, decreased nutrient intake, decreased body weight, altered immune and endocrine functions, and reduced response to oxidative stress as well as decreased muscle mass, strength, and/or physical function. 7 Disease-related malnutrition and sarcopenia are associated with increases in all-cause mortality, morbidity, length of hospital stay, and functional impairments that lead to a loss of independence and higher healthcare costs. Different mortality rates are reported in malnourished patients and well-nourished patients after hospitalization, and higher mortality is the most common complication in sarcopenia patients. 8 Older age is associated with the risk of comorbidities and physically debilitating conditions that are suggestive of negative clinical outcomes. These conditions such as sarcopenia and malnutrition are partially reversible. 9
Several studies have assessed the effect of malnutrition sarcopenia on the clinical outcome of restricted types of surgeries.5,10,11 Other studies have investigated the effect of either sarcopenia, malnutrition, or both on the clinical outcomes of certain medical conditions. 12 A review by Meyer and Valentini8 showed that several studies have emphasized on the increased length of hospitalization in patients with disease-related malnutrition and sarcopenia. Moreover, the review explained that the higher hospitalization duration was related to increased complications and demographic conditions that lead to high hospital and healthcare costs. Moreover, it demonstrated a higher readmission rate among patients with sarcopenia. Furthermore, it linked the increase in postoperative complications, duration of hospitalization, and health costs with advanced stages of sarcopenia.
A study by Sehouli et al. 5 evaluated the effects of sarcopenia and malnutrition on severe postoperative complications and overall survival in patients with gynecologic cancer. They revealed that the prevalence of sarcopenia was 32%; 18% of the patients developed severe postoperative complications, and 4% died. A meta-analysis by Simonsen et al. 13 showed that the preoperative incidence of sarcopenia was associated with a significantly higher risk of major complications and total complications, with risk ratios of 1.4 and 1.35, respectively. In a recent study, Ikeda et al. 14 revealed that sarcopenia and malnutrition were independent prognostic factors, with significant hazard ratios of 1.79 and 1.78, respectively. Patients with sarcopenia and malnutrition were categorized as the high-risk group and those without these conditions were categorized into the low-risk group. The survival rate was significantly lower in the high-risk group.
In Palestine, a study by Badrasawi et al. (2020) 15 showed that the sarcopenia prevalence was approximately 27% in patients aged ≥60 years. To the best of our knowledge, no studies have explored the effect of malnutrition and sarcopenia on the clinical outcome of the operations. Therefore, this study was conducted to assess the prevalence of sarcopenia and malnutrition among patients aged >50 years who underwent elective surgery and the possible associated factors.
Patients and methods
Study design
This cross-sectional study was conducted at two governmental and three private hospitals in the south of the west bank. The study recruited patients aged ≥50 years who were admitted for elective surgery from December 2022 to April 2022. A list of daily elective surgeries was obtained from the Ministry of Health. Upon admission, one day before the operation, data related to the patients’ demographic characteristics, medical and surgical histories, and sarcopenia and malnutrition status were collected. Ethical approval was taken from the deanship of scientific research of Palestine Polytechnic University (Ref. no: KA/41/2022); permissions were obtained from the Palestinian Ministry of Health and private hospitals. Furthermore, the study was conducted following the Equator guidelines - STROBE criteria. 16
Study population
The study population comprised patients aged >50 years who were admitted for general elective surgeries in Hebron hospitals. A convenient sampling method was used to recruit participants who were assessed upon admission before undergoing an operation. Patients who were admitted for daycare surgery, those with lower limb edema, those who were undergoing chemotherapy, and those diagnosed with neurodegenerative diseases were excluded from the study. The sample size was calculated using Open EPI software, considering an alpha level of 0.05, power of 80%, and sarcopenia prevalence of 20%, as evidenced from a previous study. 17 The expected difference was 5%, and the minimum required sample size was 106. Considering the possibility of dropouts, the required sample size was increased to 120.
Data collection
Patients who agreed to join the study were asked to fill out a structured questionnaire by interview. The questionnaire contains five sections. The first section was about sociodemographic characteristics, and the second section was about medical history. The third section was about the nutritional status assessment of the participants. The fourth section was about sarcopenia assessment using sarcopenia assessment tools. Later on, the clinical outcomes of each patient’s operation were documented.
Assessment tools
Sarcopenia assessment tools
An analysis of strength, performance, and muscle mass was performed as per the European consensus definition of the EWGSOP. Grip strength in both hands (name of device) was examined, the timed “Up and Go” test was performed, and skeletal muscle index was calculated; the values of the stronger hand were used. To obtain the skeletal muscle index, the amount of skeletal muscle mass (SMM) was calculated using the formula by Janssen et al., which included a parameter from bioelectrical impedance analysis. Ultimately, skeletal muscle index was calculated as SMM/body mass × 100, where the patients’ muscle mass was converted to percentage muscle mass and adjusted for nonskeletal muscle tissues, as originally introduced by Janssen et al.5,18
Nutritional status assessment
Nutritional status assessment was performed using anthropometric measurement, body composition, and malnutrition status using the Mini Nutritional Assessment-Short Form (MNA-SF) questionnaire (Arabic version).
Anthropometric measurements
The anthropometric parameters of weight and height were measured; all equipment was adjusted before the measurements were taken to ensure accuracy. Body mass index was calculated as (body in kilogram divided by height squared in meters (kg/m2)).
Body composition
Body composition was measured using full body sensor OMRON HBF-514C. The fat mass, fat percentage, fat-free mass, soft lean mass, SMM, and basal metabolic rate were extracted from the output provided by the sensor.
Malnutrition measurement
MNA-SF (Arabic version)19–22 was used for malnutrition screening. The following cutoff points were used to identify the malnutrition risk: (a) normal: 12–14; (b) at risk of malnutrition: 8–11; and (c) malnourished: 0–7.23–26
Ethical considerations
The study was approved and monitored by the research ethics committee of the Palestine Polytechnic University (Reference number: KA/41/2022). Each participant was informed of the study purpose, assessment procedures, and potential risks after which they provided signed written consent for study participation. Moreover, the data sheet guaranteed de-identification of patient details to ensure privacy and confidentiality. Permission and approval to conduct the study were obtained from the Palestinian Ministry of Health. The study was conducted as per the guidelines in the Declaration of Helsinki. 27
Statistical analysis
The Statistical Package for the Social Sciences TM, version 21 was used to analyze the collected data; 5% alpha level and 80% power were considered for all statistical tests. Independent samples t-test and analysis of variance test were used to determine the significance of differences where data were normally distributed. Mann–Whitney U and Kruskal–Wallis tests were used to determine the significance of differences for data that were not normally distributed. The association of sarcopenia or malnutrition with categorical variables was carried out using the chi-square test.
Results
The sociodemographic characteristics of the patients showed that 54.1% of the patients were males. The median participant age was 60 years (52–67 years). In total, 89.2% of the patients were married, and 38.7% of the patients had received high school education. The mean number of years spent in receiving education was 6.33 ± 4.39 years. In total, 43.2% of the patients were unemployed, 91.9% lived with their families, 48.6% lived in cities, and 40.5% had a monthly income of 1500–3000 Israeli Shekel (ILS). The participants’ characteristics are presented in Supplementary File 1. (Supplementary File 1: Table 1: Sociodemographic characteristics, Table 2: Medical history, Table 3: Clinical features of the current surgery).
Figure 1 demonstrates the prevalence of sarcopenia and malnutrition using MNA-SF and their association among the study patients. In total, 37.8% of the patients were categorized into the group at risk of malnutrition. Furthermore, 38.7% of the patients had sarcopenia. Sarcopenia was significantly associated with malnutrition and malnutrition risk according to MNA-SF in our study sample.
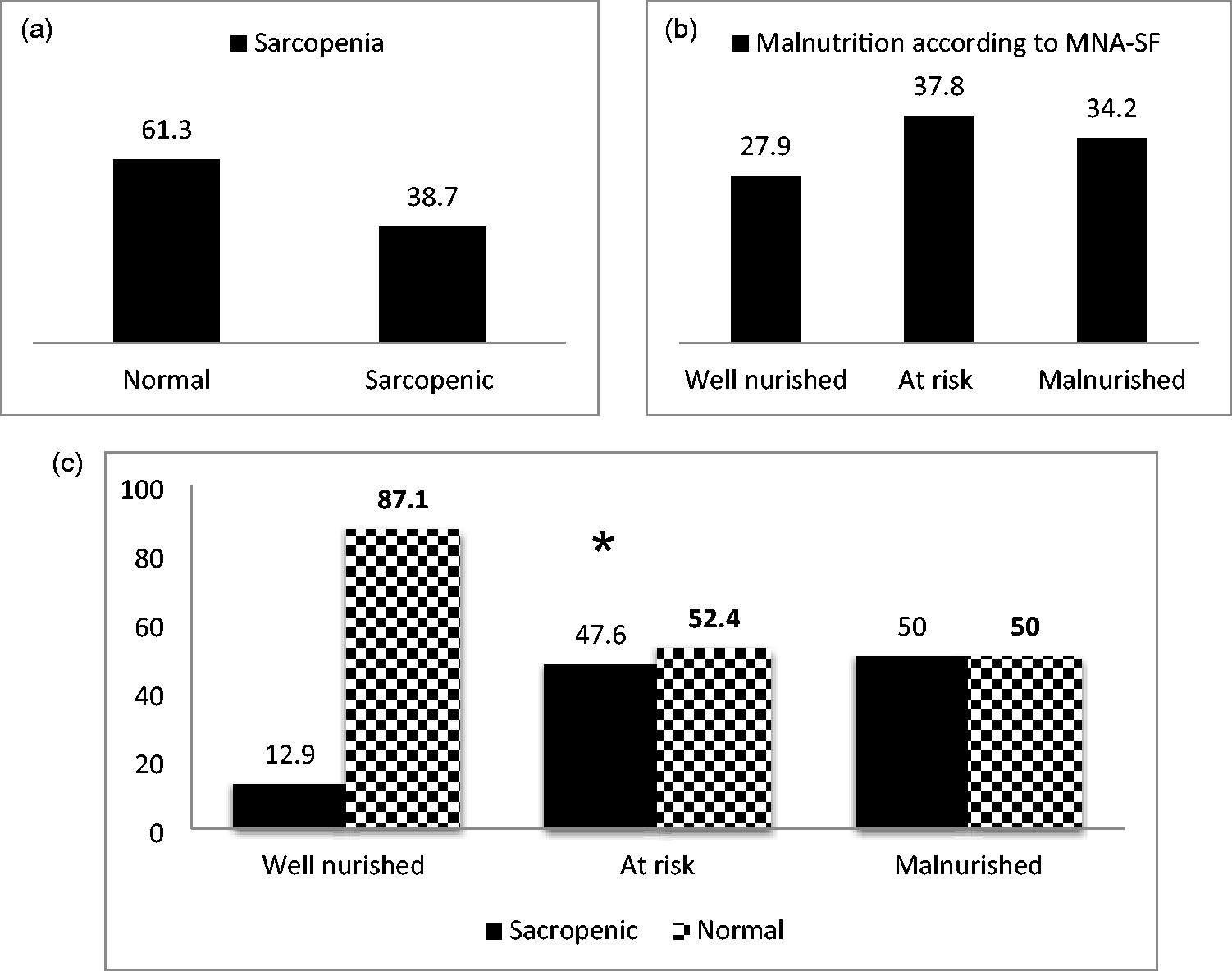
Prevalence of sarcopenia and malnutrition among study patients according to MNA-SF. *significant, p < 0.05 using chi-square test. MNA-SF: Mini Nutritional Assessment-Short Form questionnaire
With respect to the association between malnutrition according to MNA-SF and sociodemographic variables, female sex was significantly associated with malnutrition according to MNA-SF (p < 0.05). Being unemployed was also associated with malnutrition according to MNA-SF (p < 0.004) (Supplementary File 1: Table 4). In terms of medical history, malnutrition was associated with diabetes, (p < 0.05) and dyslipidemia (p < 0.05), as revealed by the chi-square test. The results are presented in (Supplementary File 1: Table 5). The association between sarcopenia and sociodemographic factors revealed significant association with older age only, p < 0.05. (Supplementary File 1: Table 6). In terms of medical history sarcopenia was associated with diabetes mellitus. (Supplementary File 1: Table 7).
Table 1 shows the association between malnutrition risk and surgery-related data among the study participants.
Association between surgery-related data and malnutrition according to MNA-SF.

ICU: intensive care unit.
The results revealed that age is significantly associated with sarcopenia (p < 0.05), and among comorbidities, only diabetes showed a significant association with sarcopenia (p < 0.05).
Table 2 demonstrates the association between sarcopenic status and the clinical outcomes of operations. The detailed results are presented in Supplementary File 1.
Association between surgery-related data and sarcopenia.
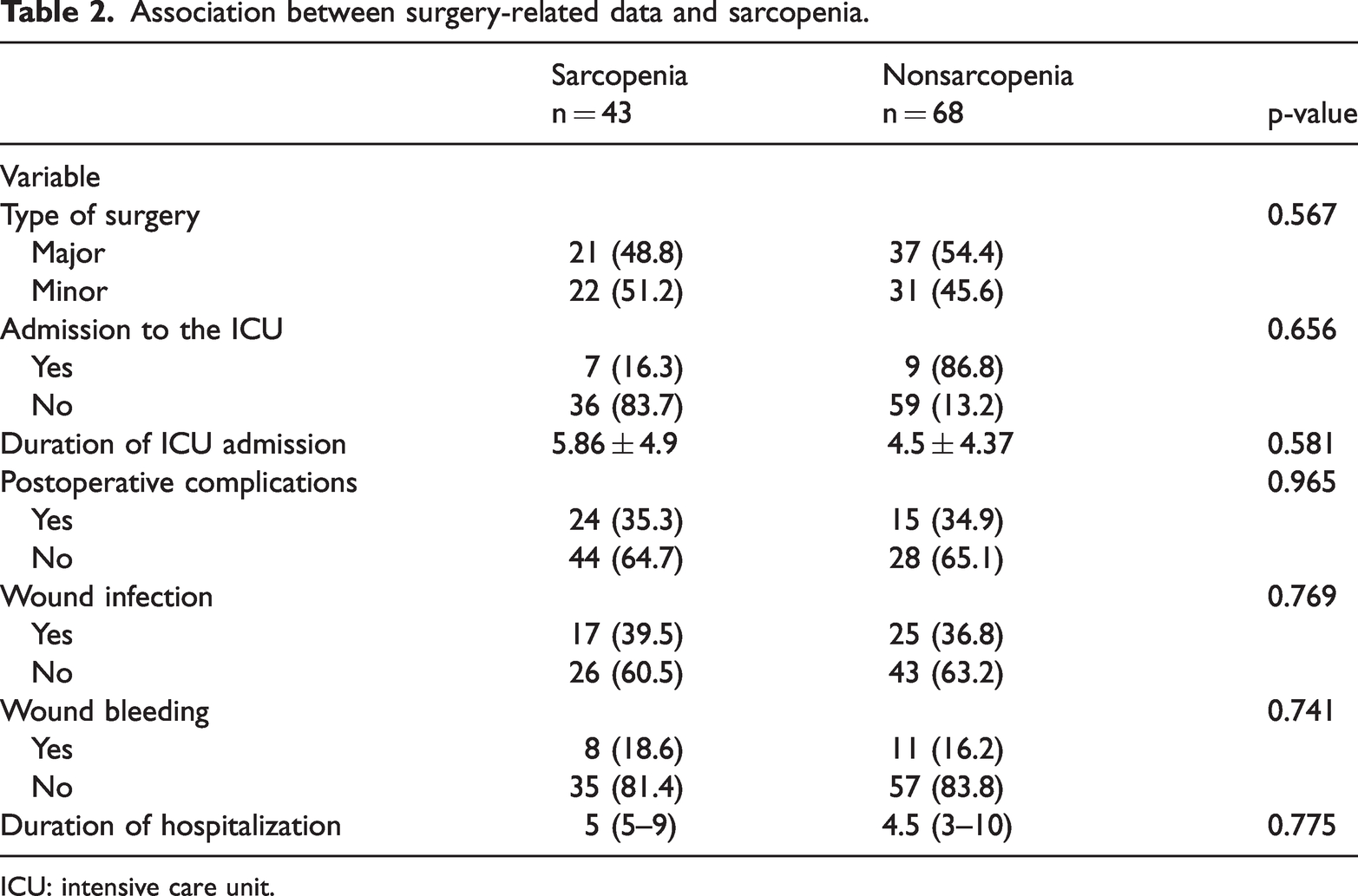
ICU: intensive care unit.
Discussion
Several studies have explored the association between diabetes, sarcopenia, and malnutrition according to MNA-SF. Muscle loss in sarcopenia differs between healthy individuals and people with diabetes. Muscle catabolism is enhanced in individuals with diabetes as a result of insulin resistance and attenuated insulin signaling. The association of sarcopenia, diabetes, and malnutrition is a result of metabolic, hormonal, and inflammatory mechanisms that consequently lead to muscle degradation. Malnutrition leads to decreased protein synthesis, increased inflammatory cytokines levels (interleukin-6, tumor necrosis factor), and mitochondrial dysfunction, ending with muscular atrophy. 1 Diabetes, especially type 2 diabetes, that occurs as a result of insulin resistance, leads to muscle glucose absorption, resulting in catabolism and muscle degradation. 28 The hyperglycemic state results in oxidative stress and glycation end products, which worsen muscle function. 29
Diabetes, especially type 2 diabetes is related to a 1.55-fold higher risk of sarcopenia in older adults than in the general population. Therefore, sarcopenia in people with diabetes needs more attention than in those without diabetes. 30 Sarcopenia could be the link between malnutrition and diabetes; a study showed that women with a poor nutritional status were more likely to have sarcopenia with an odds ratio of OR 4.97, while those with type 2 diabetes showed a higher probability of sarcopenia with an odds ratio of 5.52 than nondiabetic women. 31
The prevalence of malnutrition according to MNA-SF in this study is considered significantly higher than that in the previous study, which was performed among 302 patients using the same screening tool, MNA-SF, showing prevalence rates of 18% in participants at risk of developing malnutrition and 8% in those who were malnourished. 32 However, the prevalence was lower than that in other studies. For instance, Dubhashi and Kayal in their study on 47 patients demonstrated that 10.6% of the cases were at no risk of malnutrition and 89.4% were at risk of malnutrition and malnourished. Kagansky et al. in their study on 414 patients, found that 17.6% of the participants were well-nourished, 33.2% were at risk of malnutrition, and 49.4% were malnourished. 33 According to Soini et al., based on their study of 178 patients, 49% was well-nourished, 48% were at risk of malnutrition, and 3% were malnourished. 34 Pepersack et al. highlighted the high prevalence of poor nutritional status among geriatric hospitalized patients because they found 82% were at risk and 31% were severely malnourished. 35 Lopez et al. in their study on 89 patients, 36 demonstrated that 7.9% were malnourished, 61.8% were at risk of malnutrition, and 30.3% were well-nourished. Cansado et al. in a study on 531 using MNA, reported that 26.6% of patients were malnourished. 37 This high prevalence could be attributed to the fact that poor nutritional status is linked with numerous factors in older individuals, such as decreased cognitive and functional status, medications, presence of chronic diseases, isolation, poverty, and poor dentition. 38 This should raise concern as the medical staff are usually insufficiently aware of the significance of nutritional assessment in older patients. 33
According to the present study, malnourished patients are likely to be elder females. This is in accordance with other studies including the Kostecka and Bojanowskain 39 study, and the Ghosh et al. study 40 and other studies.41,42
In addition, this study demonstrates a significant association between unemployment and malnutrition as well as between working conditions and malnutrition. This is in accordance with the study by Keshavarzi et al., who revealed that malnourished or at-risk patients were more likely to be unemployed. Furthermore, an Egyptian study confirmed that unemployment is an absolute risk factor for malnutrition among older patients. 43 Unemployment had a significant impact on the malnutrition status in the older population. Those who were unemployed were 3.23 times more likely to be malnourished. This can be attributed to the fact that the employed older individuals possibly could have good financial status, which leads to good access to nutritional foods. Moreover, they are known to depend economically less on the caregivers for the fulfillment of dietary and other basic needs required for good health. 44 Furthermore, studies showed that unemployed older adults were more malnourished than employed ones; thus, being employed and having social support provide economic stability and mental contentment in the older population. 44
Furthermore, this study showed a significant association between the nutritional status and the presence of diabetes, as the majority of malnourished patients were more likely to be diabetics. Although our study confirmed the association, other studies using MNA-SF could not confirm it 45 because they used different screening tools. 46 However, the present study findings are consistent with those of a study done by Bourdel-Marchasson and Alan Sinclair. Older patients with diabetes, specifically type 2 diabetes, were at high risk of developing both undernutrition and malnutrition. One of the reasons that could explain this is what concluded in the Finestone et al. study as they explored the reasons for this higher risk. Dysphagia was more common in patients with type 2 diabetes, and dysphagia increases the risk of malnutrition. 47 The association between diabetes and poor nutrition can be explained by the fact that diabetes is a chronic and catabolic disease; furthermore, most patients had poorly controlled diabetes, diabetic complications, medications side effects, decrease in functional and cognitive status, loss of taste and smell, poor dentition, isolation, poverty, endocrine and gastrointestinal disorders, loss of appetite due to both disease state and psychosocial factors, sarcopenia, and accelerated muscle mass and strength loss. 48
In total, 39% of the study participants had sarcopenia. This parallels the prevalence in a meta-analysis and systematic review, which was 37%. 49 The sarcopenia prevalence of hospitalized older adults was substantially higher than that of community-dwelling according to Cruz-Jentoft et al. 50 It is likely that the sarcopenia prevalence in inpatients depends considerably on the applied definition and that the prevalence is even higher when measured at hospital discharge because of a rapid decline in strength and mass during hospitalization. 49 The finding also is in agreement with the prevalence of 36.4% reported by Wang et al. 51
Sarcopenia is an age-related syndrome 52 characterized by progressive and generalized loss of SMM and strength; recent findings indicate that sarcopenic patients are more likely to be older. The risk factors for sarcopenia include low body mass index, decreased activity and protein intake, and the presence of chronic diseases. 53 It is also considered a combination of changes in insulin resistance, chronic disease, inflammation, endocrine function, muscle disuse, and nutritional deficiencies. Reduction in growth hormone, insulin-like growth factor-1 (IGF-1), and testosterone levels may lead to the loss of lean body mass and increase in body fat. Additionally, insulin resistance, higher cortisol levels, high levels of inflammatory markers, low vitamin D levels, and immune system changes could contribute to sarcopenia and cause alterations in protein metabolism. All these factors can combine with age to cause sarcopenia; however, sarcopenia tends to be more prevalent in individuals with comorbidities. 53
Sarcopenia has been linked to chronic diseases; therefore, it is not surprising that the present study found an association between diabetes and sarcopenia. This result is in agreement with that reported by Yuenyongchaiwat et al., who confirmed the association between diabetes and sarcopenia, as diabetic patients were two-fold likely to have sarcopenia. 54 This could be attributed to the presence of type 2 diabetes, an increasingly prevalent metabolic disease worldwide, which has been documented to result in a more rapid decline in muscle mass along with strength and functional capacity, contributing to the mechanism of sarcopenia. Diabetes, especially type 2, is believed to be an important predictive factor of sarcopenia, and the presence of sarcopenia with diabetes could lead to an increased risk of mental health issues, frailty, physical disability, and dependency. Moreover, individuals with type 2 diabetes mellitus are more vulnerable to greater loss in muscle mass, strength, and functional capacity with aging than nondiabetic individuals. 55 A meta-analysis illustrated that sarcopenia and diabetes seem to be reciprocally related and could share similar pathogenetic pathways. Diabetes may lead to sarcopenia, and sarcopenia may lead to lower muscle glucose uptake, hyperglycemia/hyperinsulinemia, and insulin resistance, all known precursors of diabetes. Poor physical performance can be associated with an increased risk of diabetes. Moreover, muscle fat infiltration might also cause insulin resistance promoting both the development of sarcopenia and diabetes.
Limitations
This study is one of the few studies that describe malnutrition screening and sarcopenia among surgery patients in Palestine. However, this study had certain limitations. First, the study’s small sample size (n = 111) limited the generalizability of the findings in a larger population. A greater sample size would increase the study’s statistical power and the reliability of the associations discovered. Second, participants were selected from individuals attending elective procedures, which may not represent the broader surgical patient population. Finally, unreported lifestyle factors, which are key contributors to sarcopenia and malnutrition, such as dietary habits, diet intake, physical activity, and exercise, were not investigated in this study and must be explored in future studies.
Conclusions
The findings of this observational study indicate a notable prevalence of sarcopenia and malnutrition according to MNA-SF among patients aged ≥50 years as well as a possible link between these disorders. The study also suggests that sarcopenia is associated with factors such as sex, working conditions, a history of surgical procedures, advanced age, and diabetes. More studies with larger, more varied cohorts are needed to confirm these findings and determine causal relationships.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251342030 - Supplemental material for Sarcopenia is linked to malnutrition among Palestinian patients aged >50 years admitted for elective surgeries, along with associated factors
Supplemental material, sj-pdf-1-imr-10.1177_03000605251342030 for Sarcopenia is linked to malnutrition among Palestinian patients aged >50 years admitted for elective surgeries, along with associated factors by Ali Shakhshir, May Hamdan, Islam Thaher, Nada Dweik, Ruba Abu Iram, Shurooq Osama and Manal Badrasawi in Journal of International Medical Research
Footnotes
Acknowledgments
The authors would like to thank the patients who contributed their time to this project. Moreover, the authors would like to thank Nestle company for permitting the use of MNA-SF, which facilitated malnutrition assessment.
Authors’ contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Ali Shakhshir, May Hamdan, Islam Thaher, Nada Dweik, Ruba Abu Iram, Shurooq Osama, and Manal Badrasawi. The first draft of the manuscript was written by Ali Shakhshir, May Hamdan, Islam Thaher, Nada Dweik, Ruba Abu Iram, Shurooq Osama, and Manal Badrasawi. Additionally, all authors commented on previous versions of the manuscript. All authors have read and approved the final manuscript.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.