
Abstract
Background:
The nutrition status of primary schoolchildren in Africa has received relatively little attention in comparison to that of younger children. We surveyed primary school students in Guinea-Bissau, a nation that is among the poorest in the world.
Objective:
Anthropometry and prevalence of anemia and vitamin A deficiency were assessed in schoolchildren participating in International Partnership for Human Development’s school feeding program in 2 regions of Guinea-Bissau.
Methods:
A cross-sectional survey of 32 schools in the regions of Cacheu and Oio was conducted in November 2011. Variables included age, gender, weight, height, hemoglobin, and retinol-binding protein concentrations. Z scores for height for age (HAZ), body mass index for age (BAZ), and weight for age were calculated using World Health Organization reference data.
Results:
Anthropometric assessment of 4784 students revealed stunting (HAZ < −2) in 15.5%, thinness (BAZ < −2) in 13.2%, and anemia in 42.0%. Stunting, thinness, and anemia were significantly more common in males, in students from Oio, and in older students. Vitamin A deficiency, detected in 21.5% of the population, was the only assessment that did not demonstrate significant differences between genders or regions. About 61.1% of all children had 1 or more indicators of undernutrition.
Conclusion:
There are substantial rates of stunting, thinness, underweight, anemia, and vitamin A deficiency in primary schoolchildren in Guinea-Bissau, even among those participating in a school lunch program and particularly among males and older students. The results suggest the need for evaluating feeding programs and other methods to improve nutrition status in primary school students, especially in older students.
Introduction
Malnutrition among school-aged children, although believed to have less impact than malnutrition in younger children, 1 has been reported to be associated with reduced academic advancement, 2 –6 low physical capacity, 7 and reduced catch-up growth or progression of stunting in previously malnourished children. 8,9 In a compilation of studies of school-aged children of 6- to 12-years from 2002 to 2009, Best et al reported that the prevalence of underweight among world regions was 8% to 39%, stunting was 16% to 29%, and thinness was 6% to 35%. 1 Additionally, anemia was found in 24% to 31% and vitamin A deficiency (VAD) in 7% to 32%. 1 These and more recent reports 10 –17 suggest that malnutrition in school-aged children remains a serious problem worthy of additional investigation.
Guinea-Bissau is a West African country that is among the poorest in the world. It had 1.7 million inhabitants in 2010, with 69% living below the poverty line 18 and a United Nations Human Development Index ranking of 176 of 186 nations. 19 Malnutrition is a substantial public health problem in Guinea-Bissau, with moderate or severe stunting in 32% of children under 5 years of age, moderate or severe underweight in 18%, and moderate or severe wasting in 6% in 2010. 20 Vitamin A deficiency in children aged 6 months to 2 years in Guinea-Bissau was recently reported to be 65%, 21 exceeding the average rate of 55% predicted by the World Health Organization (WHO) based on the nonbiochemical proxy measures. 22 Although nationwide surveys of anemia prevalence have not been conducted in Guinea-Bissau, anemia was found in 80% of children under the age of 5 residing in the 3 islands of the Bijagos Archipelago region of Guinea-Bissau. 23
Malnutrition is suspected to be common in primary school-aged children in Guinea-Bissau, and some regions of the country now receive school-based supplemental feeding programs to address this concern. However, the extent of malnutrition in school-aged children in Guinea-Bissau has not been systematically assessed. To our knowledge, there are no published reports or publically available data specifically characterizing the nutrition status of school-aged children in Guinea-Bissau. Baseline anthropometric and biochemical data were therefore collected as part of a micronutrient-fortified ready-to-use supplemental food (RUSF) trial conducted among primary school students in Guinea-Bissau, funded as a pilot project of the US Department of Agriculture (USDA) in 2011 to 2012. The results from the baseline survey are presented below.
Methods
Protocol and Participants
The study was conducted in collaboration between the International Partnership for Human Development (IPHD) and Global Food and Nutrition with training and analysis provided by the coinvestigators from Tufts University. Two large regions in Guinea-Bissau, Cacheu and Oio, were chosen to participate, with Oio known to be the more impoverished region. These regions are among IPHD’s 7 active McGovern-Dole International Food for Education and Child Nutrition program areas. Primary schools within the regions of Oio and Cacheu were randomly selected for participation. All students at participating primary schools were eligible to participate regardless of age or health status. Data were collected by IPHD enumerators and nurses or medical personnel provided by the Government of Guinea-Bissau Ministry of Health. Most baseline data were collected from each school on a single day during the period from November 14, 2011, to December 2, 2011. Baseline data collection preceded initiation of a pilot randomized controlled trial of RUSF, to be reported elsewhere.
As part of the existing IPHD McGovern-Dole International Food for Education programs, students were provided 1 meal per day at school, consisting of USDA-supplied beans, rice, vegetable oil, potato flakes, and some local ingredients, as well as a weekly micronutrient supplement and periodic antiparasitic treatment with mebendazole. The weekly micronutrient supplement contained vitamin A 2500 IU, vitamin D3 300 IU, thiamine 1 mg, riboflavin 0.5 mg, vitamin C 15 mg, niacinamide 500 mg, and iron 200 mg.
Ethical Approval
Written approval to conduct the study was obtained from the Government of Guinea-Bissau Ministries of Health and Education, and the study was reviewed by the Tufts Health Sciences/Tufts Medical Center Institutional Review Board. School participation was voluntary, and school principals or other officials provided written informed consent. Students’ permission to participate was obtained by verbal permission and through written informed consent from students’ parents. Students could opt out of any component of the study at any time and there was no requirement to participate in any study assessment in order to receive the RUSF.
Assessments
Demographic and anthropometric assessments
Demographic data included age, gender, region (Cacheu or Oio), and school. Anthropometric data were measured according to the WHO guidelines. 24 Nonfasting weight was measured to the nearest 0.1 kg by calibrated digital scale with students wearing light clothing and no shoes. Height without shoes was measured by stadiometer to the nearest 0.1 cm. Body mass index (BMI) was calculated as weight (kg)/height (m). 2
Z scores for height for age (HAZ), BMI for age (BAZ), and weight for age (WAZ) were calculated with WHO AnthroPlus software version 1.0.4 (http://www.who.int/growthref/tools/en/) based on WHO Reference 2007 data for ages 5 to 19 years. Students having biologically implausible z scores, defined as HAZ < −6 or >6, BAZ < −5 or >5, and WAZ < −6 or >5, were excluded from anthropometric analyses.
Biochemical assessments
Hemoglobin (Hb) and retinol-binding protein (RBP) were measured in whole blood from capillary sampling obtained by fingerprick adhering to the WHO guidelines. 25 Hemoglobin was measured on-site by the use of Hemocue Hb201 Hemoglobinometer (Ängelholm, Sweden). Anemia was defined by WHO age- and gender-specific criteria and classified as nonanemia or mild, moderate, or severe anemia. 26
Retinol-binding protein was measured as a proxy for retinol by the dried blood spot method. Three drops of capillary blood were placed on a protein saver card (Whatman 903 Protein Saver Snap-Apart Card; GE Healthcare Bio-Sciences, Pittsburgh, Pennsylvania). Blood spots were dried out of direct sunlight, then packaged individually with desiccant, transported to the United States, and stored at −20°C until analyzed. Retinol-binding protein was analyzed by sandwich enzyme-linked immunosorbent assay (Craft Technologies, Inc, Wilson, North Carolina). Vitamin A deficiency was defined as RBP < 0.7 μmol/L, based on the definition of VAD presuming an equimolar relationship between RBP and retinol. 22,27
Statistics
Sample size goals for the study were based on the RUSF intervention study’s primary outcomes of changes in RBP and Hb. The enrollment goal was 5500 primary school students attending schools in the 2 regions.
Data were analyzed for both regions and genders combined and stratified by region, gender, and age. The effect of age was assessed using age as a continuous variable or by participants grouped by 3 age categories consistent with the WHO AnthroPlus categories: 5 to 9 years (61-119 months), 10 to 14 years (120-179 months), and 15 to 19 years (180-228 months).
Normally distributed variables are described as mean ± standard deviation (SD) or mean with 95% confidence intervals (95% CIs). Variables that were not normally distributed were log transformed for analysis and are presented as medians (25th percentile, 75th percentile). Categorical variables were expressed as percentage of the population. Unpaired t tests or analysis of variance were used to test between-group comparisons of continuous variables. Predictors of continuous variables were derived from multiple linear regression models, and multiple logistic regression models were used for predictors of binary variables. Comparisons between frequencies of categorical variables were made by χ2 test. Predictors of categorical variables were derived by logistic regression. SAS version 9.3 (SAS Institute Inc, Cary, North Carolina) was used to perform analyses.
Results
Demographic Characteristics of Students
No school declined participation in the study. A total of 5539 students were enrolled in the study from 20 schools in Cacheu and 12 schools in Oio. Of the 5539 students, demographic and anthropometric data were available for 4838 students, reflecting that some students declined participation in assessments and/or were absent on the day of data collection. Sixty percent were from Cacheu. The age range was 4.0 to 23.8 years, with 6 students younger than 5 years and 20 students older than 19 years. The mean age of students in first grade was 8.2 years (Cacheu 8.1 years vs Oio 9.1 years), and the mean age of sixth graders was 13.8 years (Cacheu 13.6 years vs Oio 15.2 years). The age ranges within each grade were greatest for the earlier grades, as illustrated in Figure 1. Males constituted 55% of the study population (53% in Cacheu and 57% in Oio). When grouped by AnthroPlus age categories, the percentage of males in the study population significantly increased with age (Figure 2A, P < .001). As age increased, the proportion of students from Cacheu decreased, with students from Cacheu comprising 70% of the 5- to 9-year category, 56% of the 10- to 14-year category, and only 30% of the 15- to 19-year category (Figure 2B, P < .001).
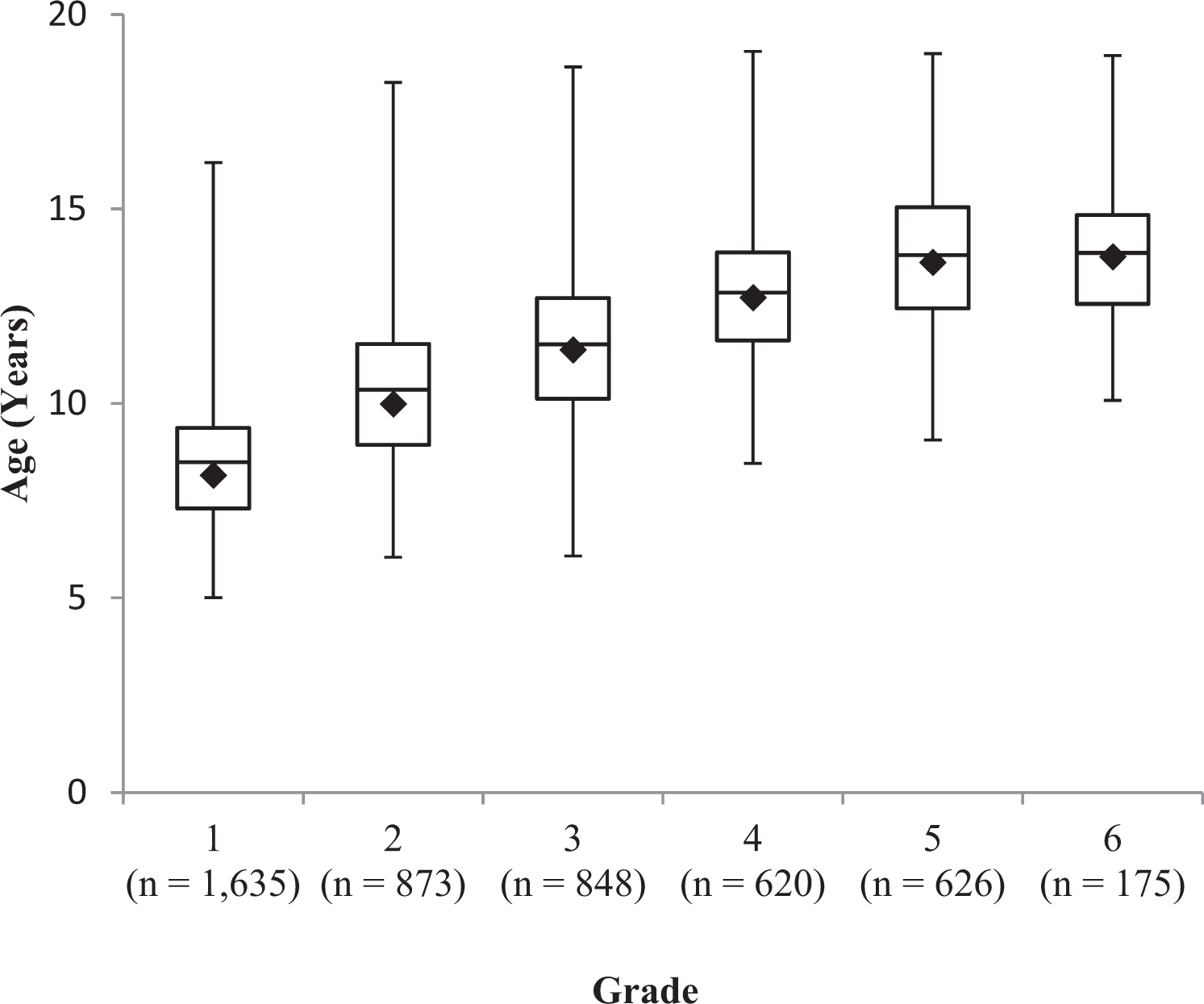
Mean age (diamond), median (bar), and ranges (error bars) of students per grade.
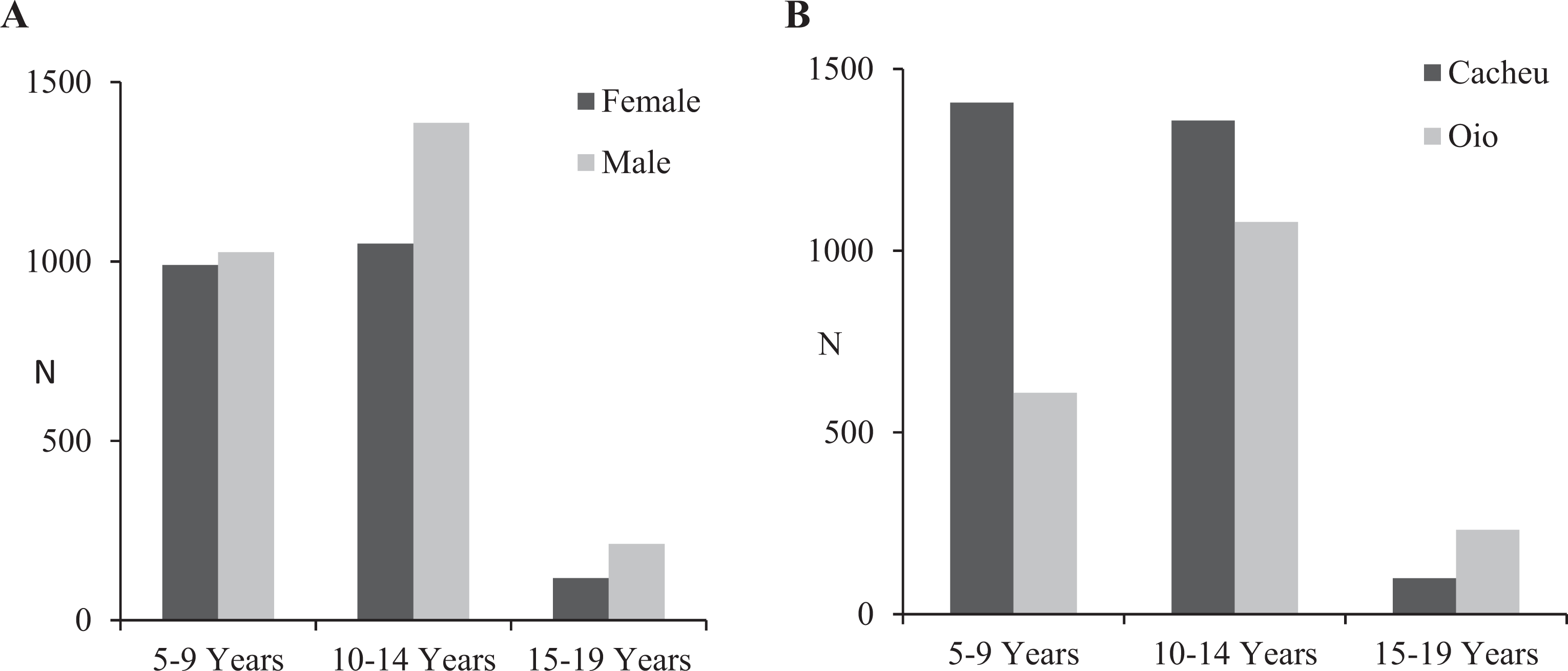
A, Numbers (N) of females and males grouped by AnthroPlus age category. The percentage of males was greater with increasing age (P < .001). B, Numbers of study participants from study regions grouped by AnthroPlus age category. The percentage of participants from Cacheu decreased with increasing age (P < .001).
Anthropometric Assessments
Analyses excluded the 6 students under age 5, 20 students over 19 years, and those with biologically implausible z scores (N = 34), leaving 4784 participants aged 5 to 19 years (48-228 months; Table 1).
Summary of Demographic and Anthropometric Data.a
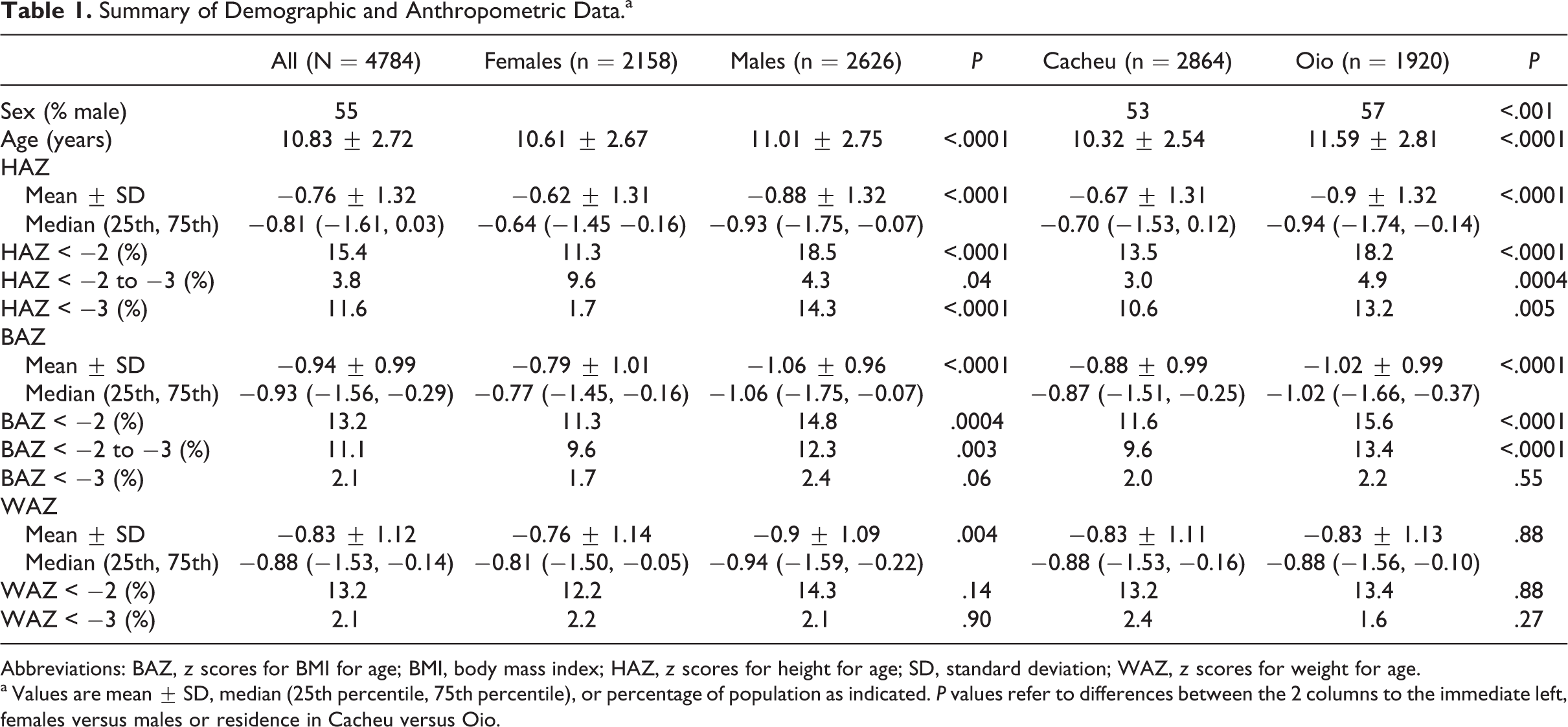
Abbreviations: BAZ, z scores for BMI for age; BMI, body mass index; HAZ, z scores for height for age; SD, standard deviation; WAZ, z scores for weight for age.
a Values are mean ± SD, median (25th percentile, 75th percentile), or percentage of population as indicated. P values refer to differences between the 2 columns to the immediate left, females versus males or residence in Cacheu versus Oio.
For the entire population, mean HAZ was −0.76 and was more negative in males versus females (−0.88 vs −0.62, P < .001) and in students from Oio versus those from Cacheu (−0.90 vs −0.67, P < .001). However, in a multiple regression model including age and gender as covariates, the difference in HAZ between regions was no longer significant (Table 2, P = .07). In the entire population, stunting (HAZ < −2) was present in 15.4%, with moderate stunting (HAZ ≥ −3 to < −2) in 11.6% and severe stunting (HAZ < −3) in 3.8%. Stunting, moderate stunting, and severe stunting were more common in males and in students from Oio (Table 1).
Predictors of HAZ, BAZ, Thinness, and Stunting.a
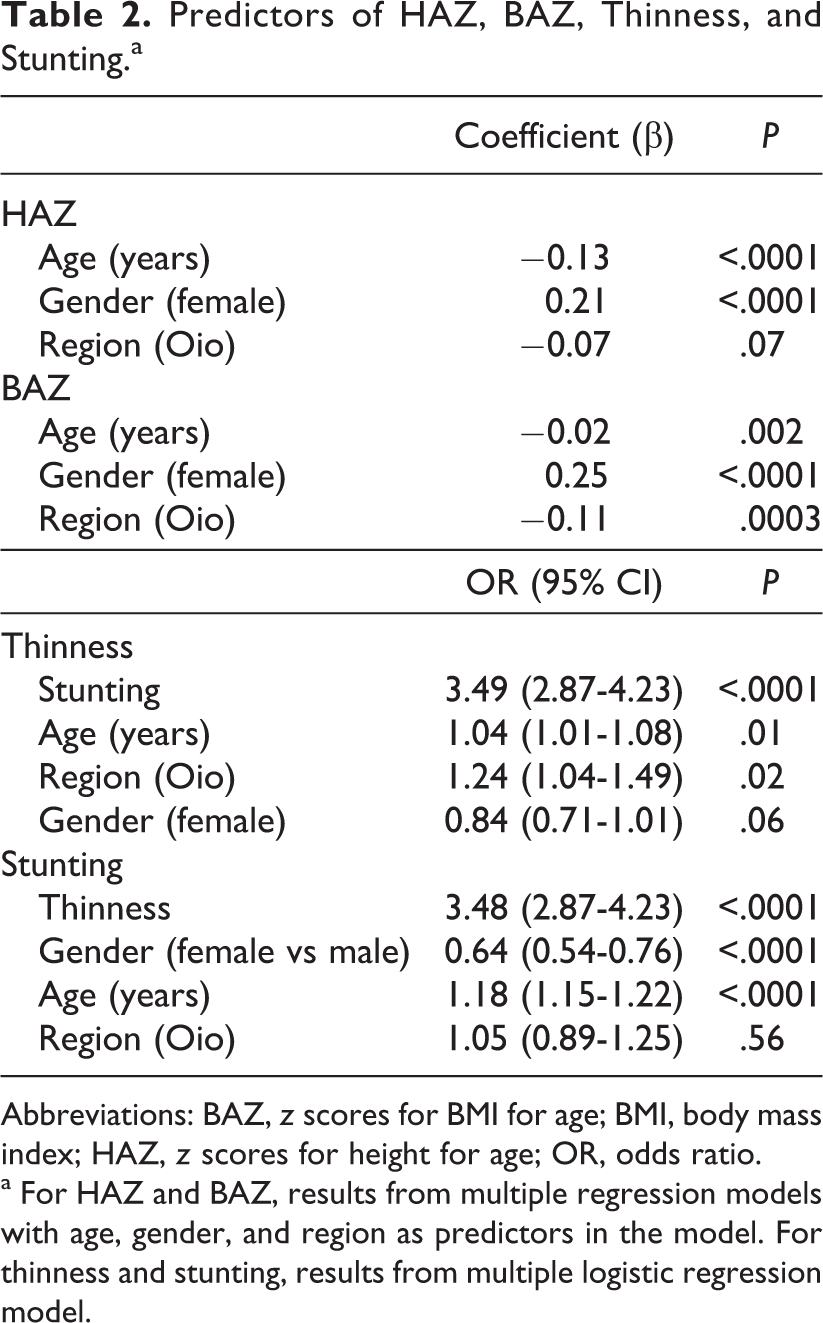
Abbreviations: BAZ, z scores for BMI for age; BMI, body mass index; HAZ, z scores for height for age; OR, odds ratio.
a For HAZ and BAZ, results from multiple regression models with age, gender, and region as predictors in the model. For thinness and stunting, results from multiple logistic regression model.
For the entire population, mean BAZ was −0.94 and was more negative in males versus females (−1.06 vs −0.79, P < .001) and in students from Oio versus those from Cacheu (−1.02 vs −0.88, P < .001). These differences remained significant in the full regression model with age, gender, and region as predictors (Table 2). In the entire population, thinness (BAZ < −2) was present in 13.2%, with moderate thinness (BAZ ≥ −3 to < −2) in 11.1% and severe thinness (BAZ < −3) in 2.1%. Moderate thinness was significantly more common in males and in students from Oio (Table 1).
Z scores for height for age was strongly correlated with BAZ (P < .0001). In a logistic regression model including age, gender, and region, stunting was the strongest predictor for thinness (odds ratio = 3.5, P < .0001; Table 2).
Z scores weight for age was assessed in 2061 students (1011 females and 1050 males) aged 5 to 10 years. Mean WAZ was −0.83, and WAZ was more negative in males versus females (−0.90 vs −0.76, P = .004). Underweight (WAZ < −2) was present in 13.2%, with moderate underweight (WAZ ≥ −3 to < −2) in 11.1% and severe underweight (WAZ < −3) in 2.1%. There was no significant difference between regions in mean WAZ or in percentage of underweight between genders and regions.
Increasing age was associated with more negative mean BAZ and HAZ (P for trends <.001, adjusted for gender and region), and BAZ and HAZ were more negative in older age categories (Figure 3A). Thinness and stunting were more prevalent in age categories 10 to 14 and 15 to 19 years compared to ages 5 to 9 years (Figure 3B).
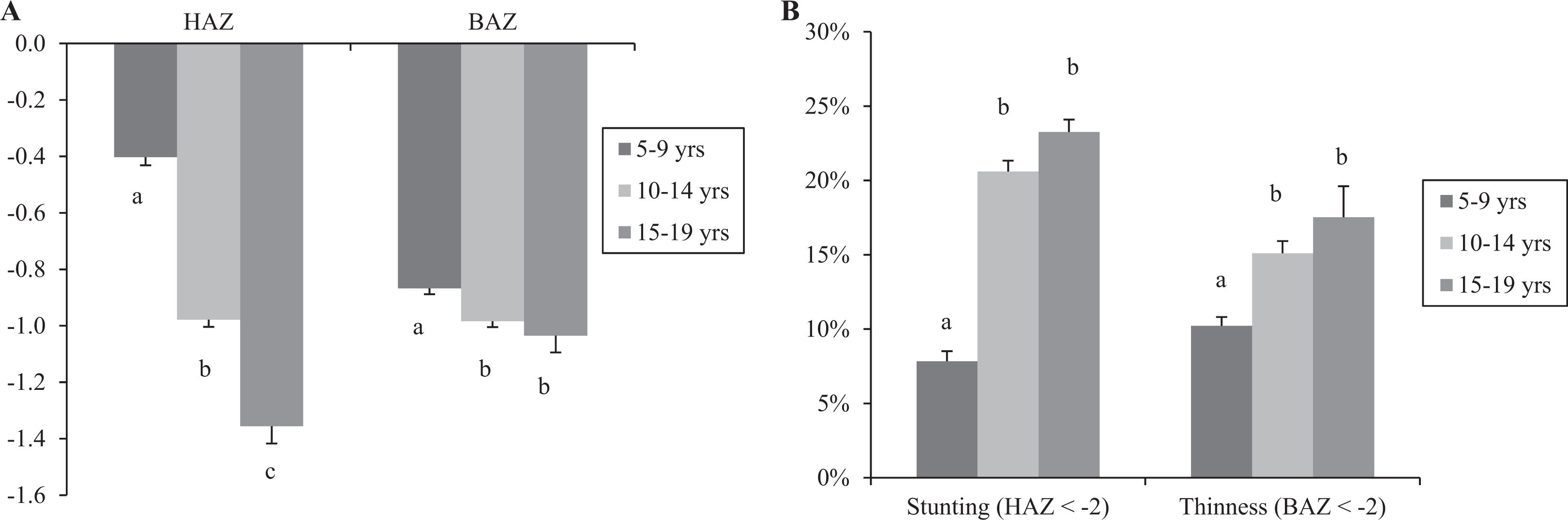
A, Mean HAZ and BAZ (±SE) by age categories. Different letters denote significant differences between age categories within HAZ and BAZ (P < .001). B, Percentage of the entire population with stunting (HAZ < −2) and thinness (BAZ < −2) per age categories. Different letters denote significant differences between age categories for stunting and thinness (P < .001). BAZ indicates z scores for BMI for age; BMI, body mass index; HAZ, z scores for height for age; SE, standard error.
Biochemical Assessments
Hemoglobin
Data for Hb were available for 4538 students aged 5 to 19 years and are presented in Table 3. For the entire population, mean Hb was 11.9 mg/dL and did not significantly differ between genders or regions. Combined anemia (total of mild, moderate, and severe) was present in 42%, with mild anemia in 18.8% and moderate anemia in 22.2%. Combined anemia and mild anemia were more common in males versus females and in students from Oio versus Cacheu. Severe anemia was uncommon (0.5% overall) but was significantly greater in students from Oio versus students from Cacheu (1.0% vs 0.1%, P < .001). Rates of moderate and severe anemia decreased with age and were above 40% for children aged 5 and 6, dropping below 20% in children over 11 years old (Figure 4).
Biochemical Assessments.a
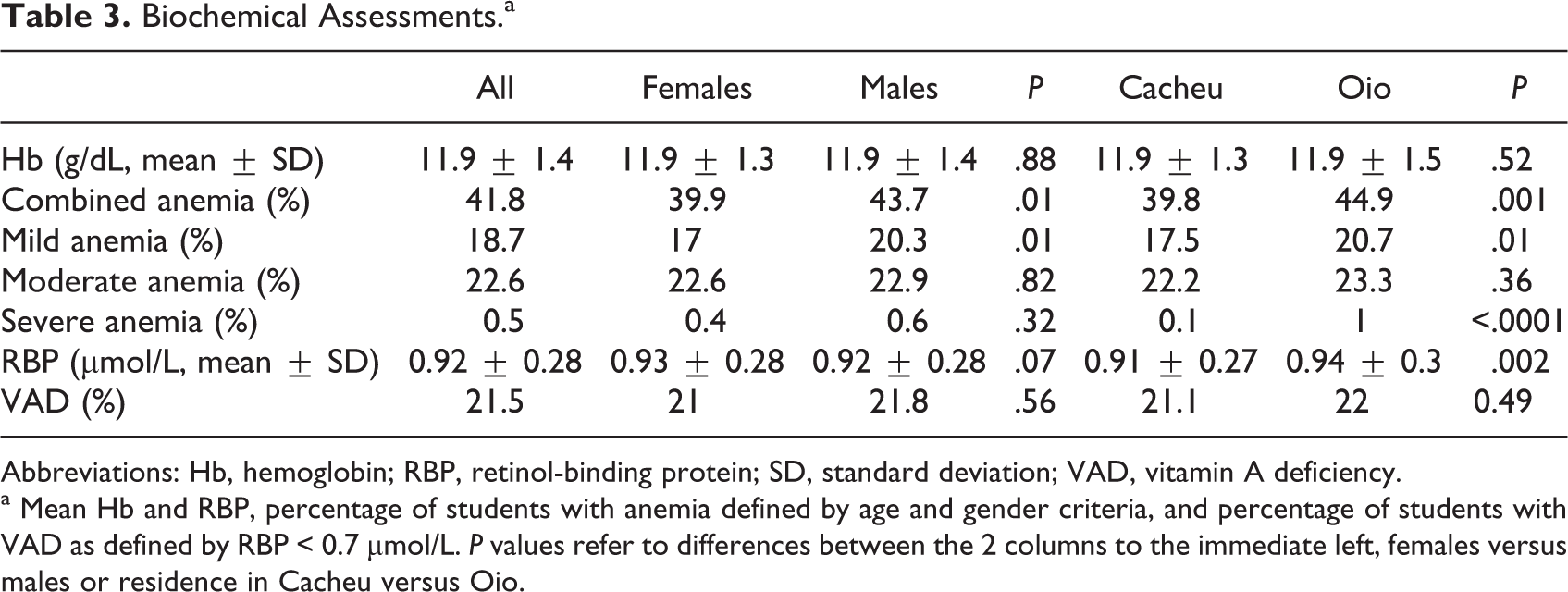
Abbreviations: Hb, hemoglobin; RBP, retinol-binding protein; SD, standard deviation; VAD, vitamin A deficiency.
a Mean Hb and RBP, percentage of students with anemia defined by age and gender criteria, and percentage of students with VAD as defined by RBP < 0.7 μmol/L. P values refer to differences between the 2 columns to the immediate left, females versus males or residence in Cacheu versus Oio.
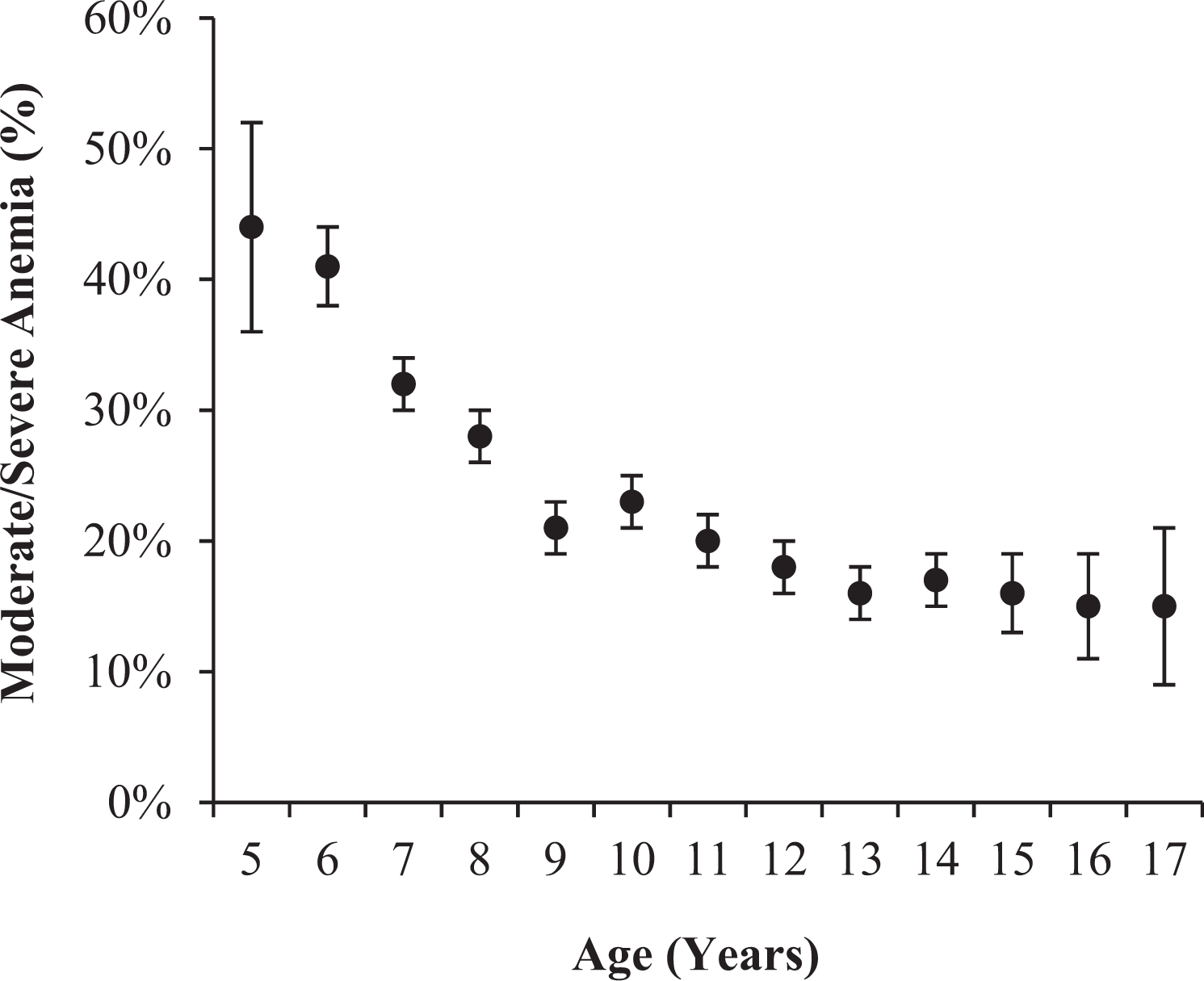
Percentage and standard error of students with moderate or severe anemia by age.
There were no differences in anemia rates among females and males within age categories 5 to 9 years and 10 to 14 years. However, for ages 15 to 19 years, males had substantially greater rates of mild anemia than did females (49.5% vs 15.0%); this pattern was evident in Cacheu (48.1% vs 9.5%) and Oio (50.0% vs 18.5%). Positive predictors of Hb included age and increasing BAZ, HAZ, and RBP, while residence in Oio was associated with lower Hb levels (Table 4). Using a logistic regression model, factors associated with moderate or severe anemia included residence in Oio, younger age, and lower HAZ and RBP.
Predictors of Biochemical Parameters.a
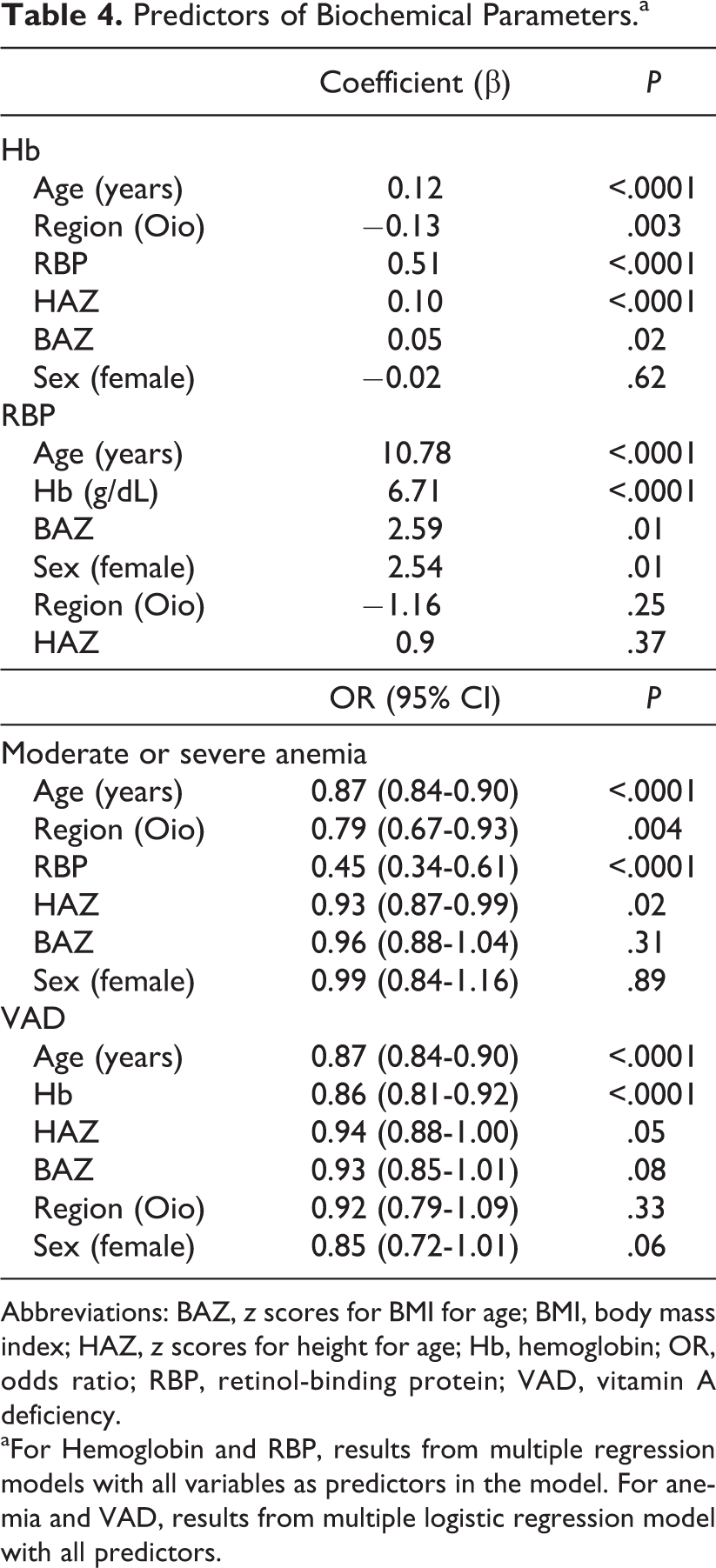
Abbreviations: BAZ, z scores for BMI for age; BMI, body mass index; HAZ, z scores for height for age; Hb, hemoglobin; OR, odds ratio; RBP, retinol-binding protein; VAD, vitamin A deficiency.
aFor Hemoglobin and RBP, results from multiple regression models with all variables as predictors in the model. For anemia and VAD, results from multiple logistic regression model with all predictors.
Retinol-binding protein
Dried blood spots were collected from 4433 students aged 5 to 19 years, with 3867 samples adequate for the analysis. Mean RBP was 0.92 ± 0.28 μmol/L and was significantly greater in students from Cacheu versus Oio (0.91 vs. 0.94, P = .002; Table 3). Vitamin A deficiency (RBP < 0.7 μmol/L) was observed in 21.5% of students, with no significant differences by region or gender. Percentage of those with VAD significantly decreased with age (P < .001). When assessed by AnthroPlus age categories, VAD occurred in 27% of those aged 5 to 9 years, 18% of those aged 10 to 14 years, and 8% of those aged 15 to 19 years (P < .001). Using a multiple linear regression model, factors associated with a higher RBP included increasing age, BAZ, Hb, and residence in Cacheu. Predictors of VAD included younger age and lower Hb.
Discussion
In this first report of the nutrition status among primary school students in Guinea-Bissau, we found that students were considerably older than expected, stunting was present in over 15%, thinness or underweight was present in 13%, anemia was present in 42%, and VAD was present in 21%. In addition, 61% of students had 1 or more indicators of moderate or severe nutritional problems (at least 1 z score < −2, anemia or VAD), making this one of the most undernourished countries in the world among those without current crises such as war or famine. These results occurred despite the fact that children were receiving a school lunch, suggesting that additional supplementary feeding programs should be considered for children in the lowest income countries such as Guinea-Bissau.
An average first-grade student was 8.5 years old at the beginning of the school year; ages ranged widely, especially among children in the earlier grades. This pattern is consistent with Guinea-Bissau national data for primary school gross enrollment ratios (ie, number of students enrolled regardless of age/number of students of typical primary school age) of 119% for females and 127% for males. 28 The broad age ranges and the older mean student age are typical in West Africa (as well as Haiti) and may be explained by delayed entry into school, the need for students to work, interruption due to illnesses, and/or disruptive political and economic events.
Indicators of malnutrition were generally worse in students from Oio, with higher rates of stunting and thinness, lower mean HAZ and BAZ, and higher rates of combined, mild, and severe anemia. Oio is generally considered to be more economically challenged than Cacheu, which may account for this observation and may also explain why students from Oio were older. A gender effect was also observed, with males having greater rates of stunting and thinness and lower mean HAZ, BAZ, and WAZ. Several investigations of school-aged children have also reported greater prevalence of stunting among males, 12 –14,29 suggesting that greater rates of undernutrition in teenage males is a generalized problem that requires greater attention.
We observed that the prevalence rates of stunting and thinness increased with age. Malnutrition during the primary school years is often associated with further stunting, reduced school attendance, impaired ability to perform physical work, and lower labor force productivity. Academic achievement is directly related to height for age, 30 possibly indicating that effects of chronic malnutrition on both height and cognitive development also lead to reduced school attendance. The greater rates of stunting among older students may reflect the cumulative effect of malnutrition over time. In a longitudinal survey of 1080 Kenyan schoolchildren aged 4.5 to 13.5 years, older children exhibited more stunting and lower HAZ scores at baseline, while the prevalence of stunting increased over the 2 years of study. 17 Similar patterns of an age-related increase in stunting or decrease in HAZ were found in investigations of school-aged children in other countries including Senegal, Nairobi, Pakistan, and India. 10,14 –16 One study noted that older children were less likely to consume adequate energy, possibly in part due to their greater energy needs. 12 In Guinea-Bissau, we are also aware of social factors that may contribute, for example, that children in higher classes often have to live away from home to complete their schooling and thus do not have their parents to rely on for food security.
Moderate or severe anemia was observed in 22.7%, and these degrees of anemia have implications for impaired cognitive performance 4 and reduced work capacity. 7 Although iron deficiency is the most likely cause of anemia, contributing factors could include other nutritional deficiencies such as that of vitamin A, 31 infections such as malaria and intestinal parasites, 31,32 and (of likely lesser importance) hemoglobinopathies. 33 We observed that lower BAZ, HAZ, and RBP were associated with lower Hb, and lower HAZ and RBP were predictors for moderate or severe anemia. Hemoglobin increased with age and rates of moderate and severe anemia were highest in children under 8 years of age, with levels about 40% in children aged 5 and 6 years of age. The reasons for these trends are not known but may possibly relate to lower dietary quality in small children associated with the food taboos, which are common in this population. The increased prevalence of mild anemia in older males (15-19 years) overlaps with a growth period known to increase iron requirements (14-18 years) and provides a possible explanation. A similar pattern was not observed for females, who also have increased requirements during that period in preparation for reproductive function. Although the weekly multivitamin supplement included 200 mg iron, which represents 91% to 205% (depending on age and gender) of students’ weekly iron requirements based on the US Recommended Dietary Intake for iron, it was provided in a single weekly dose, which is not the optimal method for enhancing iron absorption. Approaches to reducing anemia might therefore include consideration of daily supplements or the addition of micronutrients to the provided lunch meals.
We observed VAD, as indicated by RBP < 0.7 μmol/L, in 21% of students and as high as 28% for children aged 5 to 9, again indicating a lower quality of diet in the youngest students. While there are no guidelines for the population-level significance of VAD for school-aged and older children, for children under the age of 6 years, VAD of ≥20% is classified as having severe public health significance. Since we were unable to assess the acute phase response, the actual prevalence of VAD could have been lower than 21%. 34,35 In a study of Ugandan children aged 6 to 59 months, correction for c-reactive protein (CRP) > 5 mg/L resulted in an increase in mean RBP from 1.18 to 1.26 μmol/L and a decrease in the prevalence of VAD from 18.4% to 14.9%. 35 A meta-analysis of the effects of the acute phase response on VAD suggested that serum retinol should be adjusted by 25% to account for CRP > 5 mg/L. 36 If an additional 25% is added to all of our RBP values, the prevalence of VAD would be 8%. This adjustment, however, should only be applied to those individuals with evidence of the acute phase response, since application to all participants would likely result in a gross underestimate of VAD. Use of RBP to assess vitamin A status remains a useful approach in populations since the relationship between RBP and serum vitamin A remains relatively constant in spite of the presence of inflammation. 27,34 For example, in 600 Kenyan women, 400 of whom were HIV positive, Baeten et al used equimolar RBP and serum retinol cutoffs to assess the ability of RBP to detect hypovitaminosis A. When unadjusted for the acute phase response and HIV status, the sensitivity of RBP for hypovitaminosis A was 91% and the specificity was 94%. 27 Further, in that study, the combined presence of HIV, elevated acute phase response, and low albumin concentration reduced the correlation between RBP and serum retinol modestly from 0.95 in those with the absence of these factors to 0.87. Although RBP and serum retinol are highly correlated, the equimolar RBP cutoff of <0.7 μmol/L may actually underestimate the prevalence of VAD. Although RBP and retinol theoretically circulate in an equimolar ratio, it has been observed in young children that retinol <0.7 μmol/L corresponds to RBP < 0.83 μmol/L. 34,37 Using this cutoff, our population would have a VAD prevalence of 38.5%, and even with the adjustment of an additional 25% to account for inflammation in all participants, the VAD prevalence would be 17.7%.
As expected, the rate of VAD in our study was lower than that found for younger children. In a national study of children aged 6 to 24 months conducted in 9 regions of Guinea-Bissau, Danneskiold-Samsoe et al measured RBP from dried blood spots in Guinea-Bissau and employed the same cutoff for VAD as in our study. 21 The overall prevalence of VAD was 66%. Importantly the seasonal effects observed in that study suggest that November and December were among the 6 months with greatest VAD. This would suggest that VAD prevalence in primary school students is lower in other months, if factors associated with VAD are similar across the range of childhood. Although numbers from individual regions were small, Danneskiold-Samsoe et al also reported that among the 9 regions studied, VAD was most common in Oio (prevalence 91%, N = 89) and least common in Cacheu (prevalence 43%, N = 53). Further, in a cross-sectional study of pregnant women in Guinea-Bissau, low serum retinol was associated with the late rainy season, 38 which is when data were collected for our study. The main food sources of vitamin A in that study were red palm oil, mango, dried fish, egg, margarine, and carrots, but each of these foods were consumed by no more than 40% of women. 38
The multivitamin supplement provided to students weekly contained 2500 IU of vitamin A, which provides a range equivalent to 40% (males over 14 years) and 89% (children 4-8 years) of the US recommended dietary intake of vitamin A for 1 week. 39 Thus, the marked age-related decrease in VAD we observed was despite the fact that the supplement provided a lower percentage of daily requirements in older children, suggesting lower quality of home food for young children. It should also be noted that the national vitamin A supplementation campaign that included school-aged children had not begun at the time when data for our study were collected but had started for children under 5 years of age.
Our study had several limitations. Collection of data in primary school students may be inherently biased, and it is impossible to generalize our results to age- and gender-matched populations who do not attend schools with a school lunch program. A meta-analysis of school feeding trials in developing countries through 2006 revealed modest benefits on weight and height. 40 The meal provided daily at school and the multivitamin supplement might also be expected to benefit weight, height, and micronutrient status. We also are unable to generalize results to other regions of Guinea-Bissau. Some of the age–gender groups, such as students 14 to 18 years old, were comparatively small, and interpretation of findings should be replicated in larger numbers. We also had no ability to ascertain whether students who were absent for the testing were similar in terms of the measured parameters to students who were present. The child labor rate in Guinea-Bissau is 38%, 28 and child labor has been associated with increased malnutrition in developing countries 41 ; however, we were unable to assess its impact in this study. In Guinea-Bissau, mortality of children under 5 years is 6%, and survival rate through the last primary school grade is 79%, 28 indicating the presence of serious illnesses. Given that serious illness could have influenced anthropometric and biochemical assessments, absence due to illness may have reduced that bias. An additional potential problem is the possible misclassification resulting from differences in the age of puberty onset in Guinea-Bissau versus the US population from whom the WHO growth standards were derived. If the increased height growth and weight growth velocities associated with puberty occur later in Guinea-Bissau adolescents than in the reference population, this could increase the extent to which prepubertal participants being classified as having low height or BMI for age. Unfortunately, our survey did not include pubertal status. Both HAZ and BAZ were more negative with age and were most negative in the oldest age group, which argues against an effect of delayed puberty. However, we cannot rule out other factors that resulted in more negative HAZ and BAZ in older students.
In conclusion, data from this cross-sectional observational study of 2 regions in Guinea-Bissau during the late rainy season revealed substantial rates of malnutrition, despite the fact that the children received a school lunch, with the highest rates in males, students in Oio, and in older children. In addition, anemia was present in 42%, with the risk for anemia being greater among males, students in Oio, and younger children, and VAD was present in 21%. Such high rates of undernutrition compromise physical and cognitive development, leading to a negative cycle of unhealthy adults and stagnant national development. Future approaches to improve the nutrition of children in the poorest countries worldwide, such as Guinea-Bissau, should include interventions earlier, in preschool, increasing the nutrient density of meals provided, and adding a second school meal for those times of the year when malnutrition is most prevalent.
Footnotes
Authors’ Note
ES, NS, and WMP contributed to the design of the study. ES, NS, PF, PB, and SBR participated in the development of standardized data collection protocols and training. NS, IB, AS, and CB participated in the data collection. Data analysis was performed by ES, CB, and KS. Interpretation of results was performed by ES, NS, and SR. ES, NS, MS, and SR helped in the manuscript preparation. All authors have reviewed and approved the form and content of the submitted manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the US Department of Agriculture (USDA) Micronutrient Fortified Food Aid Pilot Project under Agreement No. FFE-657-2012/043-00 with International Partnership for Human Development.