
Abstract
Background:
Suboptimal breastfeeding results in 800 000 child deaths annually. There are multiple causes of suboptimal breastfeeding, including marketing of breast-milk substitutes.
Objectives:
To describe sales and marketing of breast-milk substitutes and their influence on World Health Organization-recommended breastfeeding behaviors, focusing on low- and middle-income countries.
Methods:
Literature review.
Results:
Global sales of breast-milk substitutes reached US$40 billion in 2013. Growth in sales exceeds 10% annually in many low- and middle-income countries, while it is close to stagnant in high-income countries. Breast-milk substitutes are marketed directly to consumers via mass media and print advertisements and indirectly via incentives, free supplies, and promotions to and through health workers and facilities, retailers, and policy makers. Internet marketing via company web sites and social media is on the rise. Marketing influences social norms by making formula use seem to be extensive, modern, and comparable to or better than breast milk. Clear evidence of a negative impact is found when breast-milk substitutes are provided for free in maternity facilities and when they are promoted by health workers and in the media. Influences through other channels are plausible, but rigorous studies are lacking. It was not possible with the data available to quantify the impact of marketing relative to other factors on suboptimal breastfeeding behaviors. Marketing remains widespread even in countries that have adopted the International Code of Marketing of Breast-milk Substitutes to restrict such activities.
Conclusion:
Adoption of stricter regulatory frameworks coupled with independent, quantitative monitoring and compliance enforcement are needed to counter the impacts of formula marketing globally.
Keywords
Introduction
Breast-milk is the global standard for optimal infant nutrition and health, and breastfeeding promotion is a key newborn and child survival intervention. Optimal breastfeeding practices consist of initiation of breastfeeding within the first hour of birth, feeding the child only breast milk for the first 6 months (exclusive breastfeeding), and continuing to breastfeed for up to 24 months or beyond. 1 Suboptimal breastfeeding results in over 800 000 under-5 child deaths annually or 11.6% of the total, 2 including 250 000 child deaths due to pneumonia and diarrhea. 3 Studies from Nepal, 4 Ghana, 5 and India 6 suggest that early initiation of breastfeeding reduces neonatal mortality by 44% among infants surviving at least 48 hours, and it is especially beneficial for preventing sepsis-related deaths. 7 The benefits of breastfeeding are not limited to settings where water is unsafe and newborns die from infections. In the United States, for example, suboptimal breastfeeding results in an increased risk of diseases such as necrotizing enterocolitis, otitis media, gastroenteritis, and lower respiratory tract infections. 8
The International Code of Marketing of Breast-milk Substitutes (BMS) was adopted by the World Health Assembly in 1981 in response to a rise in child mortality due to promotion of BMS. 9 The International Code includes 14 articles and subsequent resolutions, which lay out responsibilities of governments, health care systems and workers, and BMS manufacturers with respect to providing objective and consistent information on infant and young child feeding, quality of manufactured BMS, and responsible labeling and marketing of these products. Adoption of the Code is voluntary. As of 2014, 39 countries had fully implemented the Code in national legislation and 47 implemented some Code provisions only. Only 45 countries have functioning monitoring and enforcement systems in place according to the World Health Organization (WHO). 10
Multiple factors influence infant feeding decisions. In addition to BMS marketing, these include hospital or delivery center policies and practices that separate mother and baby; inadequate counseling and support and maternal lack of confidence; family or community pressures to introduce other foods or liquids, due to beliefs about thirst, health requirements, or cultural traditions; infant attributes; and lack of maternity protection and work which separates mothers and young infants. 11 It is difficult to parse out the contribution of each of these factors because they coexist and vary by setting, infant age, and specific breastfeeding behavior. This article aims to describe marketing of BMS and assess the extent to which this marketing influences WHO-recommended breastfeeding practices, with a focus on low- and middle-income countries (LMIC).
Materials and Methods
Our review was guided by the conceptual framework shown in Figure 1, based on the theory of planned behavior. 12 The WHO defines a BMS as any food or beverage being marketed or otherwise represented as a partial or total replacement for breast-milk, whether or not suitable for that purpose. 9 Our working definition includes standard infant formula (IF) for children less than 6 months, follow-on formula (FF) for 6 to 11 months old, and growing-up/toddler milks (TM) for children 12 months and older. We define marketing as product promotion and advertising to policy makers, to consumers, and to and through health systems and providers. In this review, we did not consider the impact of marketing of complementary foods for children less than 24 months of age.
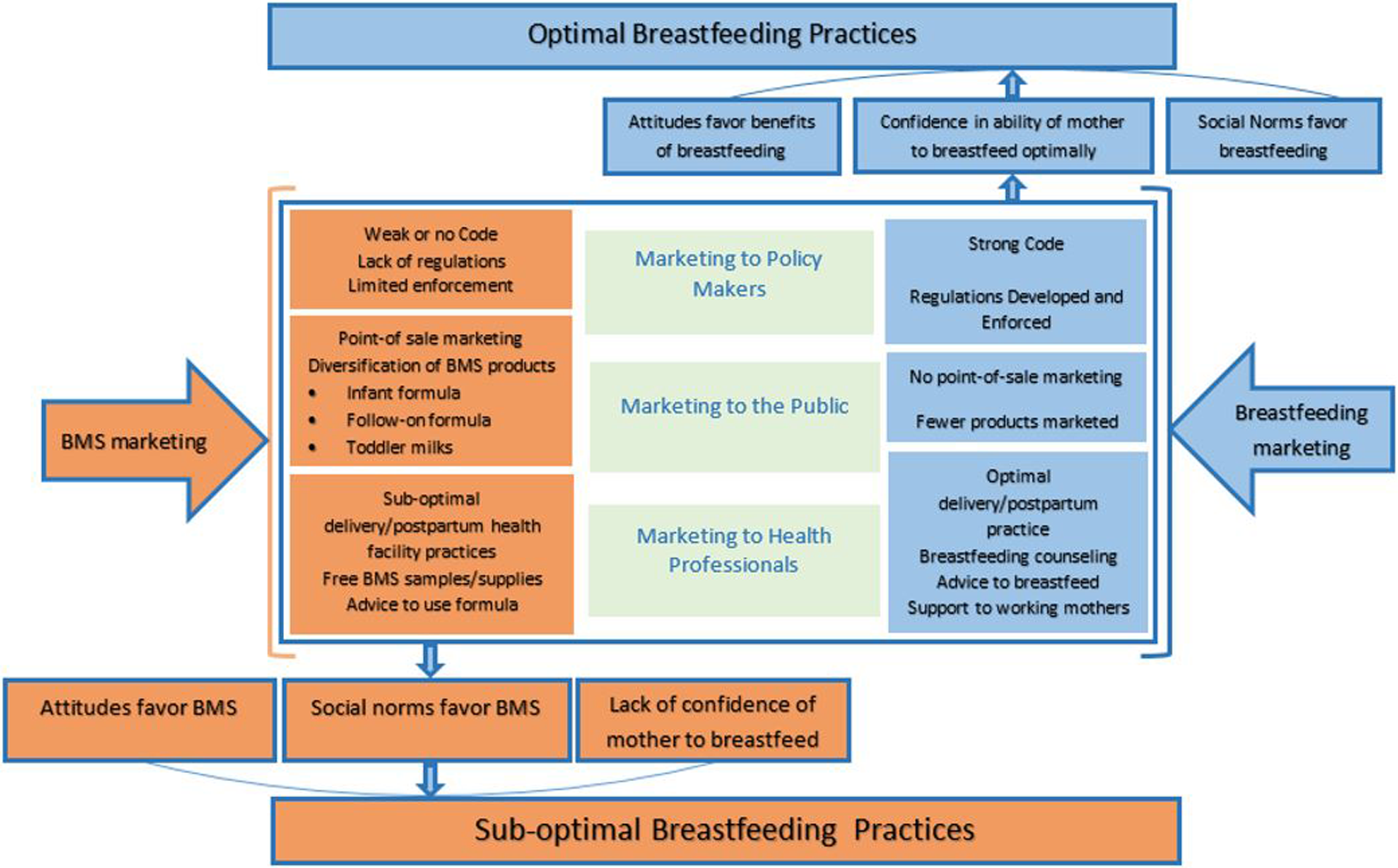
Conceptual framework for the effect of BMS marketing on breastfeeding practices.
Data on BMS sales in US$ equivalents, market trends, and industry patterns were obtained from Euromonitor International (EI), whose reports are available via subscription. The EI collects information from multiple sources, including official statistics, trade associations, company research, store checks, and interviews. For our analyses, we consulted global as well as country reports. Data were triangulated, where possible, with company reports, additional market research and media studies, and information from BMS marketing studies in several countries. Finally, we reviewed the published literature to ascertain the relationship between BMS marketing and breastfeeding initiation, exclusivity, and duration.
Results
Breast-milk Substitutes Sales
The sale of BMS in LMICs is extensive and increasing. Milk formula (MF)—the industry term which includes IF + FF + TM—was the fastest growing healthy and functional food/drink category in 2013, with financial performance far ahead of energy drinks and pre- and probiotic yogurts, the next best performers. 13 Globally, MF sales grew from US$2 billion in 1987 14 to about US$40 billion in 2013 and accounted for two-thirds of all baby food sales internationally. 15 Of all the MF sold, about 39% are IF and 25% each are FF and TM. The remaining 11% of products sold are special milks, such as for low birth weight infants. 15 Other studies reported that MF sales were growing at 10% per year in 48 of 55 markets measured. 16
The China market has fueled recent growth, with over US$12 billion in sales in 2012, 17 with sales growth projected to increase annually by 14%. 18 However, other countries have also seen high rates of growth. For example, in 2009, IF sales in Vietnam grew by 18% over the previous year 19 as did sales in Nigeria. 20 India and Indonesia experienced a 13.5% and 8% increase in MF sales, respectively, from 2011 to 2012. 21,22 In Indonesia, TM sales grew by 10.5% and made up more than half of all MF sales, 22 and in China TM sales were nearly half of all MF sales. 18
Global sales of “all baby foods” were US$58 billion in 2013. 23 Milk formula comprised 69% of this total with the remainder including sales of other foods for infants and young children. 23 Four companies—Nestlé, Danone, Mead Johnson, and Abbott—account for more than 50% of all baby food sales worldwide. While the baby food market has been stagnant in high-income countries (HIC), growth in the Asia Pacific and Middle East and Africa regions were 18% and 14%, respectively (see Figure 2).
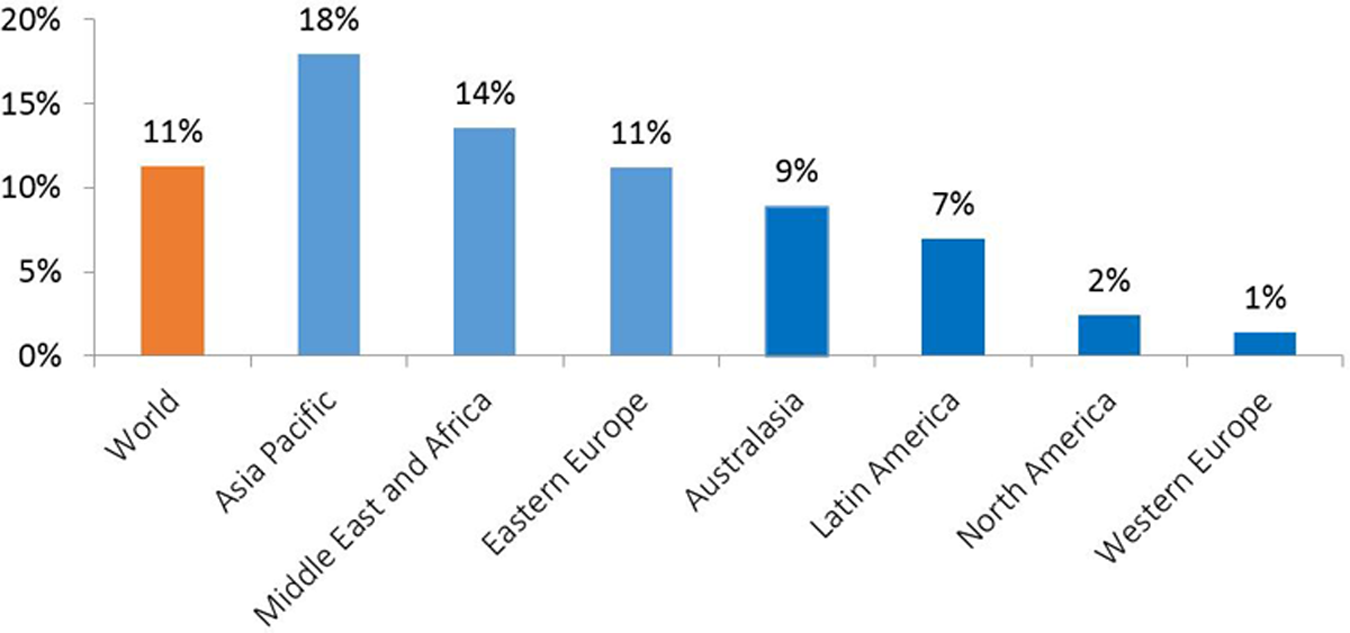
Percentage of growth in annual baby food sales in 2013 compared to 2012 globally and by region. 15
Breast-milk Substitutes Marketing Spending
We were unable to find comprehensive or verifiable data on how much money companies spend to market BMS products, but reports suggest that budgets are rising and significantly exceed what governments spend on promoting breastfeeding. 24 One study estimated that BMS manufacturers spend US$4 to 6 billion per year on marketing or 10% to 15% of gross sales. 25 The amount spent on MF marketing in the United Kingdom in 2006 to 2007 (US$12.8 million) was more than 10 times that spent by the government to promote breastfeeding (US$1.2 million) according to another study. 26 In Cambodia, where BMS marketing is restricted, US$609 914 was spent on television advertisements for MF products from September 2013 to September 2014, according to an independently conducted media monitoring study. 27
In Vietnam, with 6 times the population of Cambodia, BMS companies occupy 2 of the top 10 positions in advertising spend across all sectors, and in 2013 companies spent roughly US$34 million on BMS media advertising compared to US$15 million in 2008. 28 This surge is one reason that Alive & Thrive (an infant feeding promotion initiative in Vietnam) created the “Talking Babies” mass media campaign and worked jointly with local health authorities and United Nations Children's Fund to advocate for stricter regulations on BMS marketing. However, mass media spending by BMS companies was 61-fold greater than mass media spending to promote breastfeeding (averaging US$550 000 per year from 2011 to 2014). 29
Furthermore, donor funding for breastfeeding promotion appears to have declined over time, although precise figures are also difficult to obtain because there is no dedicated code for breastfeeding promotion in official development assistance resource tracking systems. Historically, USAID has been a major supporter of breastfeeding programs. One analysis of their spending showed that funding for breastfeeding promotion globally increased from US$8.3 million in 1989 to US$16.6 million in 1999 and declined to US$13.3 million in 2003 and US$2.3 million in 2005. 30
Impact of Government Policies on BMS Sales and Marketing
We could find no studies that directly evaluated the impact of government policies, including national adoption of the Code, on BMS sales and marketing practices, though company reports suggest that this is a source of concern for sales. 31 When we consulted Code experts about this issue, we were referred to an EI report contrasting BMS sales in India and China (see Figure 3), which we contrasted to information on Code implementation and breastfeeding practices over time.
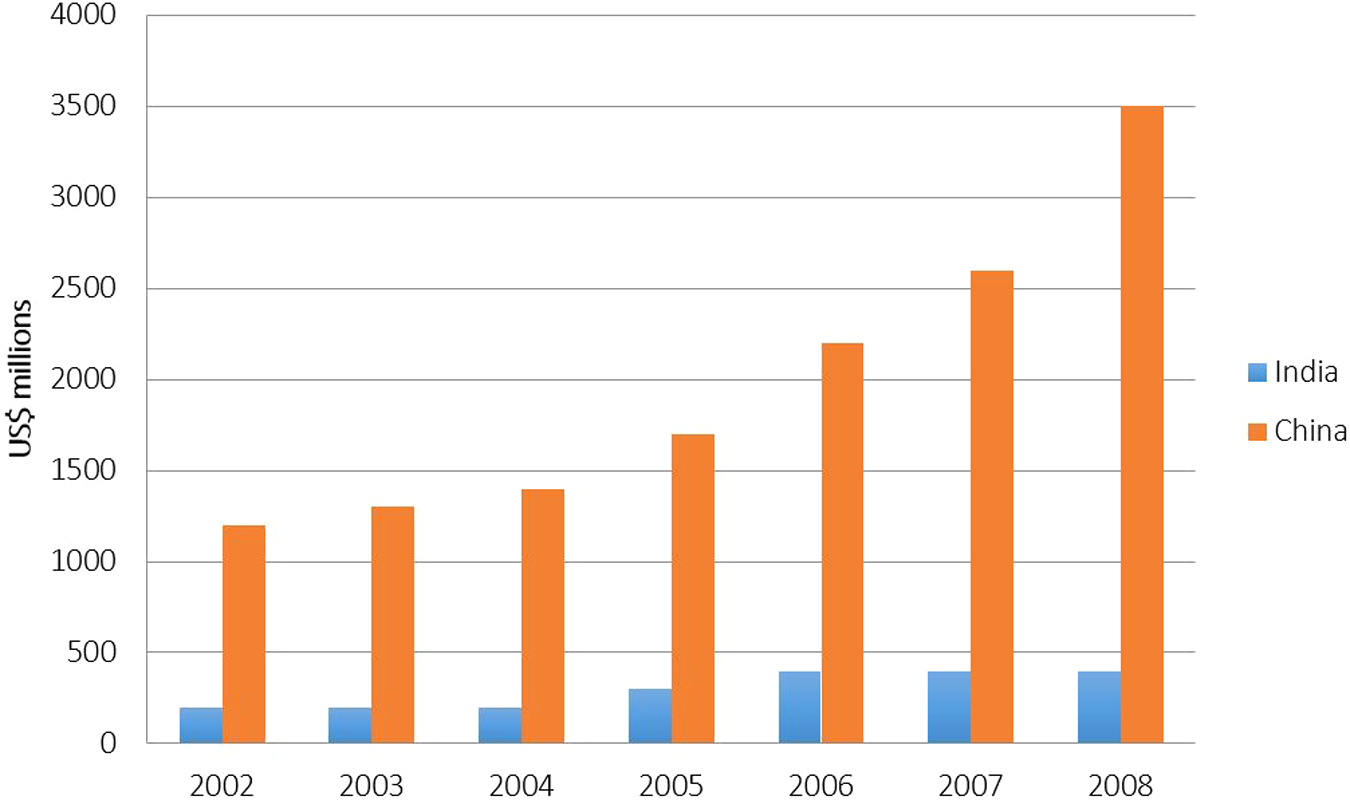
Retail value of formula in India and China: 2002-2008. 32
There are many differences between these 2 large countries that could explain divergent BMS sales. China is more urban (51%) than India (31%) with a higher proportion of women working outside the home (68% vs 29%). 33 China has a much higher gross domestic product per capita (US$6070 in 2012) and a more rapid GDP growth (9.3% from 1990-2011) compared to India (US$1516 and 4.9%, respectively). 34 Nevertheless, India has nearly twice as many births as China, making these differences in sales striking. 35 The Indian Code restricts the marketing of MF and infant foods up to age 2, while the Chinese Code applies only to infants <6 months of age. The WHO reports that India has a functioning Code implementation and monitoring mechanism and China does not, although this assessment is unverified. 10 Breastfeeding patterns are significantly different in the 2 countries: exclusive breastfeeding was 46% and 88% of infants were still breastfed at 1 year in India, 36 whereas the corresponding figures for China were 28% and 37%, respectively. 37 We could not ascertain breastfeeding trends because national data are collected infrequently.
Evidence of the Impact of BMS Sales and Marketing on Breastfeeding Practices
Multiple factors influence breastfeeding decisions (Figure 1). Each of these conditions is amenable to influence, positive or negative, by BMS marketing. Here we review evidence on the impact on breastfeeding initiation, exclusivity or duration of marketing to and through health systems and providers, directly to consumers, and through policy makers.
Impact of BMS Marketing to and through Health Systems and Providers
Breast-milk substitute manufacturers and sometimes also importers, distributors, and retailers promote their products directly to and through health systems and providers by offering stipends to attend sponsored meetings, free gifts (with company logos), and providing free formula in maternity discharge packs. Company representatives have also, in the past and recently, offered financial incentives to health workers for promoting their products in countries as diverse as Ukraine, 38 India, 39 China, 40 Indonesia, 41 the Philippines, 42 Togo and Burkina Faso, 43 and other parts of Central and West Africa. 44 In some instances, health workers have provided companies with contact information on new births for the purpose of product promotion, in violation of privacy agreements, as reported recently in China. 45 The impact of these incentives on breastfeeding behaviors has not been systematically assessed due to their “behind the scenes” nature. More visible examples of BMS promotion within health systems, such as informational brochures and posters with company brands displayed in health facilities, are also commonplace and may be interpreted as tacit endorsements for companies and products.
Advice by Health Professionals to Mothers
Health professionals around the world provide mothers with advice on infant feeding and are viewed as credible sources of information. 46 -48 For this reason, studies showing that trusted health professionals are the source of advice that undermines breastfeeding are a cause for concern. Such advice may be provided due to lack of knowledge, personal beliefs, or because of company influences such as promotional materials or incentives. Doctors’ motivations are rarely known, but their promotion of formula is frequently documented. For example, in Pakistan, a country with significant malnutrition-related mortality, 40% of mothers of infants less than 6 months of age received advice from doctors to use formula. 49 In Kathmandu, Nepal, infant formula was recommended by health providers to 36% of recently delivered mothers. 50 Formula use was 4 times more likely to be reported among mothers receiving doctor's feeding advice in the Philippines, after adjusting for education and economic indicators. 51
Free BMS, Discharge Gift Packs, and Other Promotional Materials
Breastfeeding initiation within the first hour of birth is considered a gateway behavior, strongly predictive of successful lactation establishment and of subsequent breastfeeding exclusivity. 52 Should prelacteal feeds such as IF be introduced at birth, the likelihood the mother will revert to exclusive breastfeeding is usually low. 53 Perception of insufficient milk by mothers is one of the most common reasons for early IF use. 54,55 Early use of IF interferes with suckling-induced breast-milk production, potentially turning this perception into a reality. 56 Among women with the intent to breastfeed, use of IF during maternity stays is predictive of shortened duration of exclusive breastfeeding and any breastfeeding in a range of studies. 57,58
Provision of free IF in hospital discharge packs containing promotional materials and baby products is one of the most common BMS marketing practices in the United States. Its prevalence elsewhere is unknown. A national study found that 81% of US mothers reported receiving IF-containing discharge packs in the hospital, 59 and a survey of over 3200 maternity hospitals reported that 91% distributed IF in company-sponsored discharge packs. 60 A 2000 Cochrane review of 9 randomized studies on the impact of IF-containing discharge packs reported a negative effect on exclusive breastfeeding. 61 In contrast, mothers not receiving discharge bags with formula or coupons were 58% more likely to breastfeed exclusively for 6 months compared to those who received discharge bags containing formula or coupons for it. 62
Marketing of BMS Directly to Consumers
Data on the influence of direct to consumer marketing on breastfeeding practices are limited to a handful of studies that link recall of BMS advertisements to prevalence of specific feeding decisions. A 2011 study in the Philippines found that 59% of mothers of young children recalled an IF advertisement, primarily via television, and that formula use was twice as common among those who recalled the advertisements compared to those who did not see them. Use of IF was also associated with a 6-fold higher likelihood of breastfeeding cessation before 12 months of age, though other factors including reverse causality may be responsible in part for this difference. 51 In Vietnam, researchers found that 80% of mothers reported seeing advertisements for IF on television in the past 30 days, while only 39% mentioned seeing any breastfeeding information, but feeding practices by television viewership was not reported. 63 Researchers in Laos PDR report that Thai television advertisements are influencing mothers’ attitudes toward formula feeding, and this influence is associated with a 75% reduction in exclusive breastfeeding. 64 Legislation to restrict BMS marketing if unenforced does little to abate BMS advertisement. As reported previously, BMS television ads air in Cambodia even though this is prohibited by local legislation. In one study, 85% of Phnom Penh mothers interviewed at discharge after delivery reported having read, heard, or seen a commercial promotion for BMS. 65
Breast-milk substitutes are also promoted to new mothers via other means, such as home visits or through the mail. In a study in China, 40% of mothers reported receiving free BMS samples after delivery, with the majority (61%) coming from BMS company representatives. 66 A US study found that 55% of mothers received free formula in the mail from manufacturers, a practice not prohibited in the United States. 67
Companies are increasingly using the Internet and social media, including Facebook pages, Twitter, You-Tube videos, and mobile applications to promote and sell their products, including online ordering and coupons for free or reduced price BMS. 68 The influence of these outlets on breastfeeding behavior and BMS use has not been measured but is likely to increase as Internet access, e-commerce, and mining of web-based consumer data grows, and because it is largely unregulated.
How do Advertisements Influence Behavior?
Advertisements influence social norms—or the shared understanding about expectations of behavior within a social group—by illustrating that the behavior is common and accepted in the population 69,70 This logic applies both to BMS use and to exclusive breastfeeding. 71 A content analysis of advertisements in 87 issues of a popular parenting magazine in the United States, published between 1971 and 1999, revealed that when bottle-feeding and solid food advertisements increased, breastfeeding rates reported the following year generally tended to decline. 72
Marketing also aims to influence attitudes about the safety and benefits of IF, portraying it to be as good as or better than breast milk, or presenting it as a lifestyle choice rather than a decision with economic and/or health consequences. In Vietnam, for example, formula advertisements appealed to family's concerns to have smart and tall children. 73 Data from the United States suggest that mothers increasingly agree with the statement that “infant formula is as good as breast milk,” paralleling changes in formula advertising content during the time period being studied (1999-2005). 74 In the United Kingdom, an analysis of 13 Websites with parental chat rooms noted that the single most mentioned brand was Aptamil (Danone), and the single most repeated idea across the sites was that it was closest to breast milk, a statement that originated with the company's marketing. 75
The proliferation of BMS products on the market may also influence social norms and attitudes about breastfeeding, albeit indirectly. A study in Cambodia reported over 100 different MF on the market. 76 This diversity of brands and products occupies significant shelf space in local shops. Studies suggest that increased shelf space is positively associated with sales. 32 Sales of new MF products targeting children ≥12 months have driven market growth in many settings and are projected to rise in the future. 15 This trend has the potential to influence norms and attitudes toward continued breastfeeding, although this relationship has not been systematically studied.
Finally, the way that BMS products are labeled may also influence norms and attitudes, particularly when labels contain words like “gold standard” or show healthy smiling babies, implying positive health and developmental benefits. 77 Labeling studies reveal that most companies use similar packaging on all of their formula products, 78 making it difficult for consumers to differentiate among them. 77 -79 This practice may be used to skirt local legislation, which varies across countries, as suggested in a recent Australian study. 80 In the United Kingdom, 16% of mothers in a national survey reported that they first used follow-on formula before 6 months of age, 32% of mothers reported they did not know the difference between the various BMS products, and health workers were unable to differentiate them as well. 78
Impact of Marketing on Maternal Self-Confidence
Marketing may also affect breastfeeding behaviors by diminishing maternal confidence and by influencing behavioral control, which is the perceived ease or difficulty of a behavior. For example, BMS advertisements suggesting that added ingredients improve baby intelligence may leave some mothers with the impression that their breast milk is inferior. 81 The literature contains an abundance of studies on the reasons why mothers abandon exclusive breastfeeding, 82,83 and these have been incorporated into BMS marketing. The BMS advertisements frequently appeal to parental concerns that a baby is hungry, has a digestive problem that formula can solve, or can help a baby sleep through the night. Such claims are not evidence based and can undermine breastfeeding confidence. 84 A baby's cry is often misinterpreted by families as an indication of hunger (and need for supplements), yet hunger is just one of many reasons for an infant crying response. Digestive problems such as colic are no lower with IF than with breast milk, 85 contrary to some advertisements. Mothers of formula-fed infants do not sleep more than breastfeeding mothers, 86 though advertisements suggesting that babies will sleep at night can encourage women to use them. In fact, some manufacturers promoted “Goodnight Milks” stating they would help settle babies at bedtime, a claim that was disputed by the United Kingdom Scientific Advisory Committee on Nutrition due to concerns that it could undermine breastfeeding and replace or displace night-time breastfeeding. 87
Marketing to Policy Makers
Evidence of BMS manufacturers,’ importers,’ distributors,’ and retailers’ efforts to influence local infant feeding policy has been reported in several LMIC. 49,88 One of the best-documented case studies of industry efforts to influence local policy processes comes from the Philippines. In 2003, a national survey revealed that nearly half of all Filipino families with infants and young children, and one-third of families living on less than US$2 per day purchased IF and that formula use was associated with US$400 million in out of pocket health care costs compared to US$57 million by nonformula buying families or about an additional US$0.30 in medical care for every US$1 spent on formula. 89 These data underpinned government efforts to introduce national Code legislation. However, in response to intense lobbying by industry and the US Chamber of Commerce, in 2004 the Philippine Supreme Court issued a restraining order preventing introduction of the bill and marketing continued unabated. 90 The restraining order was lifted in 2007, but the legislation's regulations were weakened substantially. During this period, timely initiation of breastfeeding declined from 54% to 39% but median duration of any breastfeeding remained unchanged (14.1-14.3 months), well below WHO recommendations. 91
Impact of National Policies and Programs on Breastfeeding
Finally, we briefly consider the evidence that policies and programs to support breastfeeding are beneficial for achieving breastfeeding outcomes. There is a significant evidence base demonstrating that breastfeeding promotion, including antenatal counseling, individual and group counseling, and breastfeeding support at delivery and postnatal visits can significantly increase early initiation and breastfeeding exclusivity 92,93 Implementation of the 10 Steps to Successful Breastfeeding through the Baby Friendly Hospital Initiative, including postdischarge community level support, has been credited with upward breastfeeding trends in income-diverse settings. 94 -97 Brazil stands out as a country that has significantly improved its national breastfeeding statistics following introduction of supportive policies and programs at a time when economic factors likely to favor BMS use were on the rise though breastfeeding practices remain far from optimal. 98 These and other data suggest a degree of elasticity in breastfeeding behavior when nations adopt supportive policies and programs. 99
Discussion
This review has reported on various aspects of BMS marketing and evidence of their impact on breastfeeding behaviors. The paucity of published data required us to use nontraditional sources of information in order to document some of the pathways through which marketing affects behavior and the potential consequences of these practices.
From this review, we conclude that BMS marketing impacts breastfeeding behaviors via multiple channels, including marketing to and through health facilities and providers, consumers, and policy makers. Such marketing influences health system practices and community norms around the social acceptability and desirability of MF use. It undermines breastfeeding confidence among women, and it affects implementation of local policies and regulations. Clear evidence is found for negative impacts on breastfeeding initiation and exclusivity when BMS are provided for free in maternity facilities and when BMS are promoted by health workers. Television and other direct to consumer marketing influence breastfeeding norms and practices, though the frequency and extent of this influence require more rigorous study. The impact on continued breastfeeding of marketing and sales of TM products should be assessed in the future. Pro-breastfeeding policies and programs may help to mitigate but are not likely completely reverse the impact of BMS marketing.
Advice by health professionals to introduce IF, whether stemming directly from company interactions or due to lack of knowledge or personal beliefs, is a vital concern. We believe this should be addressed on 2 fronts: strengthening national regulatory frameworks prohibiting BMS promotion and provision of incentives by company representatives, coupled with efforts to ensure that health providers are well equipped with the knowledge and skills to promote, protect, and support breastfeeding. These actions are, in essence, the core elements of the Code. We therefore conclude that implementation and enforcement of the Code by countries and companies would contribute significantly to improving breastfeeding practices in HIC and LMIC countries alike.
Our review highlights the stark difference in resources dedicated to BMS marketing in comparison to that available for breastfeeding policy and programs. Key elements of effective breastfeeding programs include investments to: (1) create an enabling environment (including baby-friendly birthplaces, workplaces and communities, maternity entitlements, and Code enforcement); (2) adequately train front line health workers to promote and support optimal breastfeeding and manage barriers and complications; (3) support mothers so they have the confidence and skills to breastfeed optimally; and (4) sensitize communities and families about optimal breastfeeding and how to support breastfeeding mothers.95,97 Sustainable financing to support these proven interventions is needed, as are commitments made by governments to support breastfeeding.
It was not possible with the type and quality of data available to quantify the contribution of BMS marketing, relative to other influencing factors, to suboptimal breastfeeding behavior. BMS marketing is likely to be a significant factor in settings where: (1) there are high numbers of annual births; (2) BMS companies are competing with each other to market BMS products so that the number of advertisements viewed by families is increased; (3) pro-breastfeeding policies and programs are underresourced and poorly implemented; (4) facility births are high or increasing; (5) high proportions of women work outside the home; and (6) families are likely to have sufficient funds to purchase BMS. China is a clear example of a country with these characteristics and where BMS marketing by numerous international and national companies is extensive. However, as shown decades ago, even in countries with few of these characteristics, BMS marketing can be detrimental. 100 In Pakistan, facility births are low, relatively few women work outside the home, and there is little disposable income for most families, yet BMS companies market their products extensively through the media and health professionals perhaps due to the large number of births and limited breastfeeding support programs. 49
This review has several limitations. No studies examined the impact of BMS marketing relative to other determinants of suboptimal breastfeeding so we cannot say what proportion of the burden of late breastfeeding initiation, nonexclusive breastfeeding, and shortened breastfeeding duration is due to marketing versus other factors although these factors are often inter-related and difficult to disentangle. We were also unable to use standard evidence grading methods for this review because most studies were descriptive, qualitative, or relied on nontraditional sources, such as industry reports. Randomized trials, the gold standard for evidence in public health, were only available to assess the impact of IF-containing discharge packs on early breastfeeding behaviors. Finally, our review focused on the impact of marketing in LMIC. However, evidence for some marketing practices was only available from studies conducted in high-income locations. We included these data because we believe they are informative for policies and programs in both settings.
On the basis of this review, we conclude that countries that have not adopted the International Code of Marketing of BMS should take steps to establish appropriate regulatory frameworks. Countries with national Codes should focus on effective monitoring and enforcement. Companies should agree to adhere to the Code, while refraining from lobbying to restrict its implementation and enforcement. According to Article 4 of the Code, governments have the responsibility to ensure that families and people involved in infant and young child nutrition have access to consistent and accurate information to enable informed choices about infant feeding. 9 Compliance with this element of the Code also must be increased and enforced. These recommendations are consistent with the United Nations Convention on the Rights of the Child, which calls for all segments of society to have access to information and education on child health and nutrition, including the advantages of breastfeeding. Increased investments to promote, protect, and support breastfeeding coupled with more robust implementation and enforcement of national regulations to ensure that BMS marketing practices do not undermine breastfeeding norms and behaviors will reap significant benefits globally.
Footnotes
Key Messages
Breastfeeding conveys health benefits regardless of socioeconomic status. BMS marketing to and through health facilities and providers and direct to consumers influences social norms and attitudes and undermines optimal breastfeeding behavior. Stricter regulatory frameworks with independent monitoring and compliance enforcement are needed to counter the impacts of BMS marketing. Marketing restrictions should address products targeting children below 2 years of age since branding, labeling, and market segmentation tactics make it hard for mothers and health providers to distinguish among the different products being marketed for varying ages. Increased investments to promote, protect, and support breastfeeding will reap significant benefits to society.
Authors' Note
Sandra L. Huffman was employed by the University of California, Davis, when the research for this paper was conducted but she is now retired.
Acknowledgments
We would like to acknowledge the following individuals for their useful comments on earlier drafts of this manuscript: Jane Badham, Shawn Baker, Ken Brown, Nemat Hajeebhoy, Ruth Landy, Chessa Lutter, Purnima Menon, Yvette Mirabal, Alex Reid, Shelly Sundberg, Senoe Torgerson, Neil Watkins, and Elizabeth Zehner. Harvard Business School students Ana Mendy, Elise-Marie Menke, Chelsea Miller, and Alexandra Minnis provided early analysis of BMS market data. Special thanks to Emily Davis and Yvette Mirabal for assistance with the figures and graphs. The views presented are those of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Bill & Melinda Gates Foundation.