
Abstract
Background:
Maternal mental health problems are associated with poor child growth and suboptimal child feeding practices, yet little qualitative research has been conducted to understand mothers’ perceptions about how maternal mental ill health and child nutrition are related.
Objective:
The objective of the study was to understand maternal perceptions on sources of psychological distress, and how distress impacts functioning, especially related to childcare and feeding practices among mothers of young children in South Kivu, DR Congo.
Methods:
Mothers of young children who were participating in a larger study were eligible. Using purposive sampling, participants were selected if they had high or low levels of psychological distress, based on their mean item score on measures of symptoms of depression, anxiety, and post-traumatic stress. Twenty in-depth interviews and 2 focus group discussions were conducted, with a total of 35 mothers. Key informant interviews were conducted with 5 local health workers. Audio recordings were transcribed and coded, and the analysis was guided by Grounded Theory methodology.
Results:
Major themes to emerge were that women’s husbands were a significant source of distress, with husbands’ infidelity, abandonment, and lack of financial support mentioned by participants. Psychological distress resulted in appetite and weight loss, and poor nutritional status made it difficult to breastfeed. Participants perceived psychological distress caused milk insufficiency and difficulty breastfeeding.
Conclusion:
Mothers experiencing psychological distress may need greater support for maternal nutrition and breastfeeding, and engaging fathers through responsible parenting interventions may reduce psychological distress and have a positive impact on child health.
Introduction
Growing evidence suggests a link between maternal mental ill health and child undernutrition in low-income country settings, 1 –6 with 1 meta-analysis reporting a 40% increased risk of stunting for children of mothers with depression symptoms. Symptoms of common mental disorders (ie, depression, anxiety, and medically unexplained physical symptoms) include fatigue, restlessness, apathy, changes in sleep, difficulty concentrating, and somatic symptoms such as headaches, dizziness or weakness, and racing heart. 7 Relations between depression and functional impairment have been documented in a number of studies. 8 –10 One pathway to explain the association between maternal mental health problems and child undernutrition is that depression symptoms and related functional impairment may negatively impact childcare and feeding practices.
Several studies in low-resource settings have indicated a link between maternal mental health problems and reduced caregiving behavior. For example, studies from Pakistan, Ghana, and Côte d’Ivoire showed higher incidence of diarrheal disease 11 and febrile illness 12 among children of mothers with depression symptoms compared to those without symptoms. Another study in Pakistan found that children of mothers with depression symptoms were less likely to have up-to-date immunizations. 13 Moreover, psychosocial factors including maternal mental health status have been recognized as important for breastfeeding in both high- and low-income countries. 14 –18 Studies in Pakistan and Brazil found that mothers with depression symptoms stopped exclusive breastfeeding earlier than mothers without symptoms, 15,18 and studies in Nigeria and Brazil found that mothers were more likely to stop breastfeeding entirely if they had depression symptoms. 4,19 Research in the United States and United Kingdom has found that maternal depression symptoms were associated with nonresponsive feeding behavior, 20,21 which may negatively influence infant dietary intake. 22,23 Responsive feeding refers to a reciprocal relationship between mother and infant, in which a mother responds appropriately to the infant’s cues of hunger and satiety, and nonresponsive feeding (controlling, indulgent, or uninvolved) can disrupt the infant’s cues. 24 Furthermore, mothers with depression symptoms may be more withdrawn, apathetic, and less emotionally sensitive, affecting mother–child interactions and attachment. 17,25 An association between maternal depression symptoms and reduced interest in child-rearing has been documented in several studies. 26,27
Despite the significant body of quantitative research reporting associations between maternal mental health problems, poor childcare and feeding practices, and child undernutrition, to our knowledge, there have been no qualitative studies conducted to understand mothers’ own perceptions of how their psychological state may affect their ability to care for children. In sub-Saharan Africa, exploratory qualitative studies to understand women’s experiences of perinatal mental distress have been conducted in Malawi, Ethiopia, Zambia, Tanzania, and DR Congo, 28 –32 but these did not focus on the impacts of distress on caregiving. Other qualitative research has focused on barriers to optimal child feeding practices, without specifically evaluating psychosocial factors. 33 –37 The objective of this study was to understand mothers’ perceptions of sources of psychological distress and how maternal psychological distress affects functioning, specifically in childcare and feeding, and identify other factors which they perceive to impact their psychological state and child feeding practices. Understanding mothers’ perceptions and other factors involved is important for the design of culturally sensitive maternal and child health, including mental health, interventions.
Methods
Participants
Study participants were sampled from a larger study evaluating Jenga Jamaa II, a United States Agency for International Development (USAID) Food for Peace multiyear assistance program implemented by the nongovernmental organizations Adventist Development and Relief Association (ADRA) and World Vision in South Kivu, DR Congo. In the parent study, 1820 households were enrolled in 4 intervention groups: Women’s Empowerment Groups (WEGs), the Prevention of Malnutrition in Children under 2 Approach (PM2A), Farmer Field Schools (FFS), and a Farmer to Farmer (F2F), as well as a control group. Parent study surveys, measuring key indicators of household food security, child diet, and child nutritional status, were administered twice yearly from August 2012 to March 2016.
Study participants who were mothers of children under 5 years of age were eligible for participation in in-depth interviews (IDIs) and focus group discussions (FGDs) for the present study. The participants’ children enrolled in the study (n = 35) ranged in age from 34 to 59 months, and none were currently breastfed. However, participants may have had younger children who were not enrolled in the parent study. A purposive sampling strategy was employed, with eligible participants stratified by territory (Uvira and Fizi) and livelihoods zone (plains, lakeside, mountains). A list was compiled of participants who scored in the upper (scores above 2.55) or lower (scores below 1.83) quartiles of the distribution of mean item mental health scores, with higher scores representing a greater level of distress and lower scores representing less distress. This was important for understanding whether the experiences reported by high-distress participants were unique, or if they affected all participants regardless of mental health status. In addition, key informant interviews were conducted with local health workers, from either government-run health clinics in the study area or health/nutrition field agents employed by ADRA.
Instruments
Depression and anxiety symptoms were assessed using the Hopkins Symptom Checklist-25 (HSCL-25) and post-traumatic stress disorder (PTSD) symptoms were assessed using the Harvard Trauma Questionnaire (HTQ). 38,39 All measures asked participants to rate frequency of symptoms in the past month on a 4-point Likert scale with the following response options: “not at all,” “a little,” “a moderate amount,” and “a lot.” Translated measures were available from a prior unrelated study conducted in South Kivu. 40 We also included 14 items measuring locally relevant symptoms such as stigma and fear of being talked about, which were identified through qualitative research in the context of the prior study. 40 Mean item scores were calculated, with a range of 1 to 4. Mental health data were collected in September 2015, concurrently with a wave of data collection in the parent study.
Procedures
Qualitative data collection for the present study occurred over 4 weeks in March 2016, coinciding with the last wave of data collection for the parent study. Interview and focus group discussion guides were developed with input from the local study team as well as mental health experts. For IDIs and FGDs, 2 vignettes were developed based on findings from prior field experiences in the study setting on issues related to women’s mental health and child feeding practices. They were finalized with input from the study team. The first vignette described a woman who had been abandoned by her husband and subsequently experienced symptoms of depression including apathy and fatigue. She lost motivation to continue her agriculture activities which were her main source of income, and her children eventually became undernourished. In the second vignette, another woman was described who was cultivating her crops with her friends when one of her friends was attacked by armed men. In the following weeks, she had recurring nightmares and flashbacks and was too fearful to return to the field. She believed that her milk had dried up from the stress and stopped breastfeeding her children. She went to the health center for advice but was unable to concentrate on what the nurse told her.
The vignettes were read aloud to facilitate discussion. Participants were asked about reactions to these stories and to describe women in their community who had similar problems. Participants were asked how these kinds of problems would affect functioning, in particular the care and feeding of their children. The FGD guide did not ask about participants’ personal experiences in order to protect their confidentiality but asked them to describe how these problems affected women in their community. In-depth interview and FGD guides were translated from English to Swahili by local research assistants. The study team reviewed all guides prior to data collection to identify issues with translation and comprehension, and the guides were adjusted accordingly.
The guides for the key-informant interviews (KIIs) covered similar themes but did not include the vignettes. Key informants were asked about the problems and stressors facing women in their community, and how women’s functioning would be impacted when experiencing psychological distress. The key-informant guide was developed in English and translated to French by local research assistants.
Interviews and focus groups were conducted in a private area, out of hearing range of other study staff, family, and community members. Three female ADRA field agents from Health/Nutrition and Gender sectors were trained in qualitative research methods and interview techniques. For each IDI and FGD, 1 served as a notetaker and the remaining 2 facilitated the discussion. Notes were reviewed with the first author immediately after each IDI and FGD in order to identify new themes to follow up in subsequent interviews and address any issues or concerns. In-depth interviews and FGDs were held in Swahili. Key-informant interviews were conducted by the first author in French, with the exception of 1 interview that required French-Swahili translation assistance from an ADRA field agent. All interviews and focus groups were audio-recorded with digital recording devices.
On average 1 to 2 interviews were conducted per day during the survey period. Efforts were made to achieve an even distribution of participants from each intervention group and the control group. Twenty IDIs were conducted, 13 with mothers who had high levels of distress and 7 with mothers who had low levels of distress. One FGD was conducted in each territory, with 7 participants in Uvira and 8 participants in Fizi. Participants were selected for FGD participation from villages close in geographic proximity. Participants were selected for IDIs from villages that were not sampled for focus groups. The KIIs were conducted with 3 staff members of rural government-run health clinics and 2 ADRA Health and Nutrition field agents.
Ethics
The study protocol was approved by the institutional review board of the Johns Hopkins Bloomberg School of Health. Oral informed consent in Swahili was obtained for participation in the parent study, and additional informed consent was obtained for all components of the substudy, including participation in the maternal mental health assessment, as well as for interviews and FGDs. Consent scripts were adapted to describe the specific risks and benefits of participation in each activity.
Analysis
Audio recordings of interviews and focus groups were first transcribed in Swahili by Congolese research assistants with prior experience conducting qualitative research. The Swahili transcripts were then translated to French by the same research assistants. The analysis was conducted in French by the first author using methods adapted from Grounded Theory, in which codes were grouped into concepts and categories from which theories about the research were then developed. 41,42 An initial codebook was developed based on review of IDI/FGD notes. Transcripts were reviewed and coded, and the codebook was adapted throughout the process. Codes were then grouped into categories based on themes emerging from the data. Figure 1 displays an analytical tree of code categories and response codes for each. Code categories were relationships with husbands, other stressors, effects of stressors and psychological distress, childcare and feeding practices, and positive outcomes related to child health and family relationships. Coding was facilitated by the qualitative research software ATLAS.ti, version 1.0.50. 43 The most salient themes from the response codes for each category and quotes were identified that offered a rich description of participants’ perspectives. Finally, IDI transcripts were stratified according to level of psychological distress (high or low), and codes were reviewed again to evaluate differences between the responses of high- and low-distress participants.
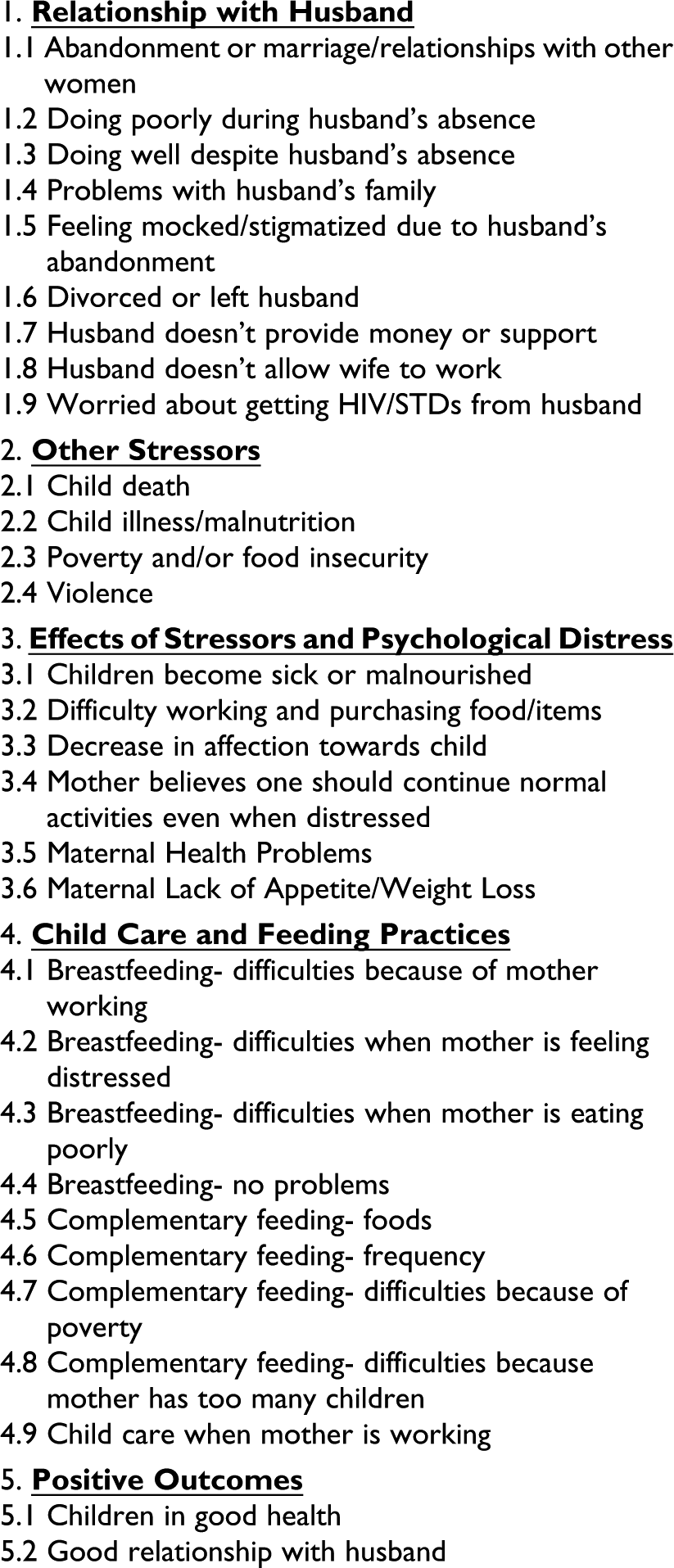
Analytical tree of code categories and codes.
Results
Background and demographic characteristics of IDI and focus group participants are displayed in Table 1. There were 20 mothers of children 5 years of age and under who participated in IDIs and 15 mothers who participated in FGDs. Ten interviews were conducted in villages throughout Uvira territory (Katogota, Nyakabere, Bwegera, Nyamutiri, Lubarika, Ndolera, Kibungu, Langala, and Lemera), and 10 were conducted in villages throughout Fizi territory (Ilakala, Kabumbe, Kaboke, Tchonwe, Lulinda, Bitobolo, Kalundja, Sebele Buzimba, Sebele Kianda, and Mwandiga). Five were participants in the Jenga Jamaa II WEG intervention, 4 were in the PM2A, 4 were in FFS, 3 were in F2F, and 4 were in the Control group. Uvira focus group participants (n = 7) were from Itara, Rugobagoba, Majengo, and Kirindangumi villages and all 4 Jenga Jamaa II interventions were represented (WEG, PM2A, FFS, F2F). The Fizi focus group had 8 participants representing the villages of Katanga, Mukinja, and Katalukulu and the WEG, Control, and PM2A groups.
Background Characteristics of 35 Mothers Participating in In-Depth Interviews and Focus Group Discussions.
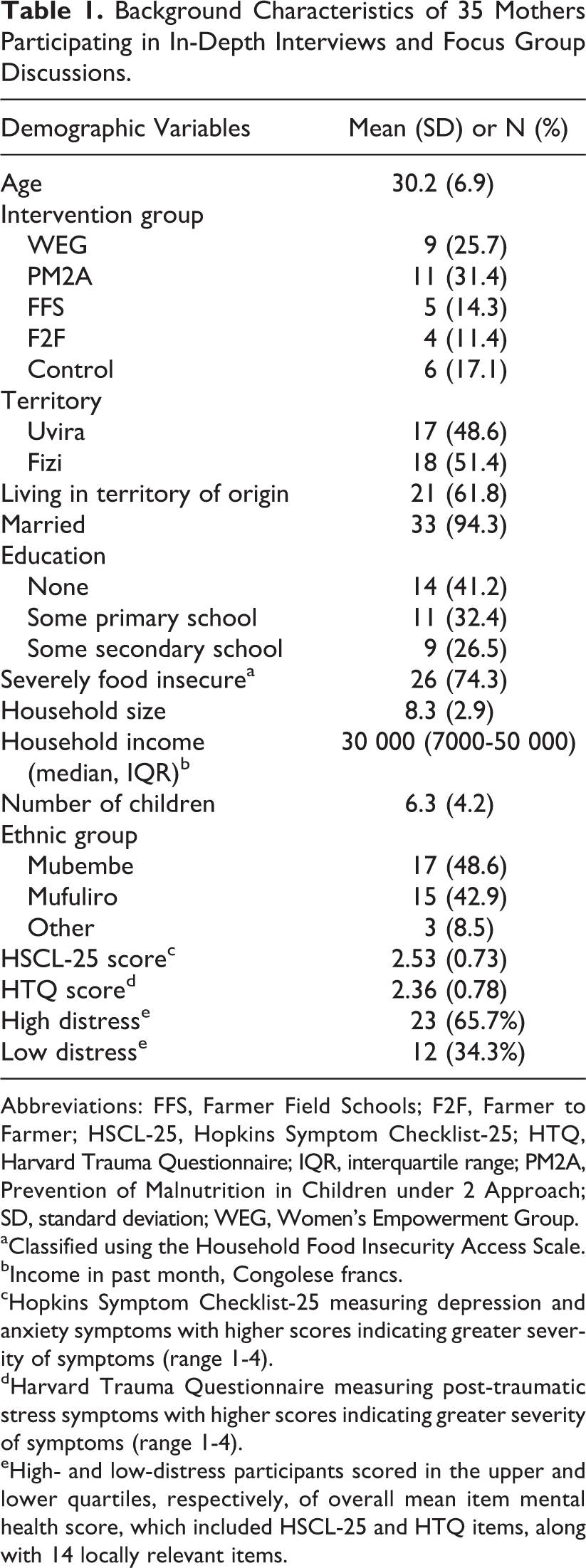
Abbreviations: FFS, Farmer Field Schools; F2F, Farmer to Farmer; HSCL-25, Hopkins Symptom Checklist-25; HTQ, Harvard Trauma Questionnaire; IQR, interquartile range; PM2A, Prevention of Malnutrition in Children under 2 Approach; SD, standard deviation; WEG, Women’s Empowerment Group.
aClassified using the Household Food Insecurity Access Scale.
bIncome in past month, Congolese francs.
cHopkins Symptom Checklist-25 measuring depression and anxiety symptoms with higher scores indicating greater severity of symptoms (range 1-4).
dHarvard Trauma Questionnaire measuring post-traumatic stress symptoms with higher scores indicating greater severity of symptoms (range 1-4).
eHigh- and low-distress participants scored in the upper and lower quartiles, respectively, of overall mean item mental health score, which included HSCL-25 and HTQ items, along with 14 locally relevant items.
The mean age of mothers participating was 30 years (SD, 6.9), 41% had no education, 32% had at least some primary school, and 27% had some secondary school education. The majority (62%) of participants were currently living in their territory of origin. Participants had on average 6.3 children, and 94% were married. About half (49%) of participants were from the Mubembe ethnic group, 43% from the Mufuliro group, and 9% from other ethnic groups. The average household size was 8.3 people, the median household income in the past month was 30 000 Congolese francs (approximately USD$31), and 74% of participants were severely food insecure according to the Household Food Insecurity Access Scale. 44
Participants’ average mean item score on the HSCL-25 (depression and anxiety symptoms) was 2.53, and the average mean item HTQ score (PTSD symptoms) was 2.36. Hopkins Symptom Checklist-25 and HTQ scores were highly correlated (r[34] = 0.90, P < .001). Participant’s average mean score for all items, including the 14 locally relevant symptoms in addition to the HSCL-25 and HTQ items, was 2.39. Seven IDI participants were classified as having low psychological distress based on the results of the mental health questionnaire (scores between 1.09 and 1.80) and 13 were classified as having high psychological distress (scores between 2.56 and 3.61). The Uvira focus group had 5 participants classified as having high psychological distress (scores between 2.56 and 3.35) and 3 participants with low distress (scores between 1.43 and 1.78). The Fizi focus group had 5 participants with high psychological distress (scores between 2.61 and 3.28) and 3 participants with low distress (scores between 1.67 and 1.78).
Two KIIs were conducted in health clinics in Uvira territory (1 general physician in Lubarika and a nurse in Kibungu) and 3 were conducted in Fizi territory (1 clinical officer in Mukinja and 2 ADRA health/nutrition field agents in Baraka).
Relationships with Husbands as a Source of Psychological Distress
Participants perceived that husbands’ behavior, including lack of financial support, infidelity, and abandonment, was a significant source of psychological distress. Their immediate reaction after hearing the vignettes was most often that they knew of someone like the woman described in the first vignette or they had the same issues with their own husbands. Participants reported that their husbands frequently took other wives or mistresses, and they lived in fear of their husbands completely abandoning them for other women. One participant described how she was affected by her husband’s behavior: I have a spouse who is the champion of marrying many women in this community…When he married other women, immediately I felt defeated and didn’t even have the strength to go cultivate. When I see my children, immediately I felt bad. (High-distress IDI participant, Lubarika)
Their husbands’ prolonged absences for work or other reasons, coupled with financial dependency on husbands, made it difficult for participants to care for their families. One participant described her reaction to her husband’s prolonged absence: I was worried because it was only me in charge of the children…worries and tears…My heart was troubled, I was tired, worn out because he had just left. I wanted to also leave and abandon everything, the children, but was convinced to stay. (High-distress IDI participant, Bitobolo).
When husbands were present, they often did not provide adequate support. In some cases, husbands worked alongside their wives to cultivate the fields but then took all of the harvest to sell themselves (rather than consume) and did not put the income toward the family. When children fell ill, fathers often refused to pay their medical expenses. Many participants reported that their husbands did not contribute to pay their children’s school fees. Additionally, many participants said that their husbands would take what little money they earned to spend on alcohol and often described their husbands as “drunks.” The lack of support from their husbands left participants struggling to meet basic needs and was also a source of stress.
Secondary sources of stress related to their husbands included fear of getting a sexually transmitted disease, particularly HIV/AIDS, due to husbands’ infidelity. Several women reported that they or other women in their community were mocked or stigmatized due to their husbands’ abandonment. In some cases, women living on their own were accused of adultery or prostitution. One participant said: “Certain neighbors mocked me and some said to return to [my parents’ house] because my husband left, instead of staying by myself” (High-distress IDI participant, Nyamutiri).
Psychological Distress in the Context of Poverty and Food Insecurity
Other problems participants frequently discussed were poverty and food insecurity. Most participants were engaged in agriculture but the harvest was poor: In brief, life is very bad here in Bwegera…As soon as you don’t have an income-generating activity, there’s great suffering in the household to feed the children, for education, and health care. (High-distress IDI participant) Psychological traumas come from the fact that someone who cultivates their field well and is able to eat, feed the children, and now it doesn’t produce anymore. You have today the problem of ‘mosaique’ [African cassava mosaic virus] that effectively lowered production, from which came cases of malnutrition among children in the household and this provoked psychological traumas because families can’t withstand the conditions in their life following the deteriorating soil quality. (KII participant, Health Worker, Lubarika)
Few women reported violence as a source of stress in their lives. In some areas, sexual violence committed by armed groups had been a problem up until a few years ago, but participants said that recent cases were rare. One participant said she had fled armed men and stopped going to the fields as a result. In 1 focus group, participants discussed a particular group of cattle herders that threatened them in the fields, and they were afraid to return to this area to cultivate. None of the participants mentioned experiencing domestic violence specifically, although 1 ADRA health worker mentioned it: There is also the problem of violence in the family, domestic violence, violence in various domains. When women cultivate their field, men don’t participate, but once the crops are sold the men take the money in their hands which is economic violence. If women refuse, they’re threatened by domestic violence. (KII participant, ADRA Field Agent, Baraka)
Psychological Distress and Psychosomatic Problems
Most participants reported somatic symptoms in relation to their stressful experiences. Weight loss and lack of appetite were frequently reported, as well as general pain and feeling “sick in the heart.” In some cases, “sickness/hurting of the heart” meant hypertension when participants were pushed for further clarification. When 1 participant’s child died, she said she felt pain in her body and fell ill. When asked what kind of sickness, she said it was sickness of the heart and she did not have an appetite. One participant said: I became seriously thin in a way that people mocked me…really a lot of suffering, pain in the heart, I spent almost a year in my house without going out until my friend intervened and got me back to doing my activities. (Uvira FGD participant)
It was very common for participants to report weight loss in times of stress: “I don’t feel good because my weight has gone down due to the problems that gnaw at me. I weighed 40 kilograms or more before, now I barely weigh 37 kilograms” (High-distress IDI participant, Tchonwe). One participant said she lost weight because of “thinking a lot” about her situation. Another participant said, “Before the problems between me and my spouse I was 60 kilograms but now I weigh 40 kilograms. In fact, I lost weight because of the issues with my husband and I had a lot of problems” (Low-distress participant, Ndolera).
Many participants associated stressful life events, psychosomatic problems, and weight loss with deteriorating physical health: When I was in crisis…I had lost so much weight. My sister-in-law said you refuse to eat sombé [cassava leaves] here, you are going to suffer. I was almost gone…(Uvira FGD participant)
Links Between Distress and Functioning
To gain an understanding of how mental distress might affect women’s functioning, participants were asked what activities they thought would be difficult for someone like the women described in the vignettes. When asked what tasks would be difficult for women experiencing distress, almost universally participants responded with cultivating their fields, doing household tasks, looking for firewood, preparing food, or paying for clothes and education for their children. Some specified that these tasks would be difficult because they “feel bad” or lack strength. Interviews with health workers supported these findings: “That happens here, when a woman is stressed do you think that she can still go to the field to cultivate?” (KII participant, ADRA Field Agent, Baraka). Another health worker said, “In this case feeding also becomes a problem, it’s the mother that looks for food…she will rarely go to the field because she’s frustrated and this will negatively affect the feeding of the children” (KII participant, ADRA Health Worker, Baraka).
Links Between Distress and Child Feeding Practices
Participants also saw a link between mental distress and child feeding practices particularly breastfeeding. “When you have problems, you don’t breastfeed like you should, you sit there with your hand on your forehead and a lot of worries and pain in the heart” (Uvira FGD participant). They often perceived that stress caused milk insufficiency: “I have to tell you that I had insufficient milk with my second-to-youngest child because of the troubles gnawing at me. Anyway, the last child had difficulties because there’s no milk due to the troubles” (Fizi FGD participant). When 1 woman was asked how she felt breastfeeding her 6-month-old infant after her husband had left, she said, “As I was so troubled I didn’t have enough milk to give to the child” (High-distress IDI participant, Bitobolo). When asked how she feels breastfeeding when her heart feels bad, 1 participant said “I lose my head, especially when I breastfeed a lot” and mentioned that she did not have any milk (High-distress IDI participant, Sebele Kianda). Another participant said, “I have troubles…When I had my baby I had difficulty finding food and when I breastfeed I feel pain in my heart” (High-distress IDI participant, Kabumbe).
Participants frequently made an association between poor maternal nutritional status and difficulties breastfeeding. During a stressful time, 1 participant said, “I felt pain in my breast while breastfeeding due to the lack of food…I felt bad and I didn’t have sufficient milk” (High-distress IDI participant, Kabumbe). Another participant said she currently had sufficient milk, but sometimes her milk is insufficient due to “lack of food and many troubles.” One participant who had several children who died said that she became seriously thin afterward and was advised to stop breastfeeding. Regardless of mental health status, participants felt that they could breastfeed well when they were eating well themselves, and when they were eating poorly they felt pain when breastfeeding or had perceived milk insufficiency.
In terms of complementary feeding practices, participants mainly attributed feeding difficulties to poverty. Yet to the extent that mothers perceived psychological distress as linked with problems breastfeeding, it would also result in early introduction of complementary foods. Often they could only afford staple foods and it was more difficult to incorporate animal source foods in children’s diets: Children are suffering at all times because they eat very poorly, the situation is very bad. When you find 1000 francs you go directly to buy flour instead of buying fish or meat so that the children have food…The day passes, they become malnourished because the children eat very poorly. (Low-distress IDI participant, Nyakabere)
Some participants attributed psychological distress to a deterioration in children’s health and nutritional status. One participant said that for mothers like the ones described in the vignettes, their children would lack strength and fall ill. Another mentioned that the children’s health would deteriorate because the mother would stop preparing food for the children. One of the health workers said that if a mother was experiencing psychological distress during weaning, she may not be able to find adequate complementary foods, having a negative effect on the health of the children. Therefore, “the mother’s stress can affect the life of the infant or young child” (KII, ADRA Field Agent, Baraka).
Another theme that emerged was the lessening of affection toward children when the mother felt distressed. One participant described this phenomenon: And the love toward the child diminishes when one is in a time of difficulty as you think of the difficulty caused by their father. You have a load and the child increases the load, the love decreases. It is said in the rules or principles of feeding, the child should look at you and you should reciprocate with a smile. (Uvira FGD participant)
Experiences of Low-Distress Participants
Although similar themes emerged between high- and low-distress IDI participants, interviews conducted among low-distress participants tended to be shorter in duration and less rich in content. Participants in the low-distress group were more likely to discuss abandonment by their husband as an issue affecting other women in their community rather than affecting them personally. In some cases, they discussed social support as a moderating factor that reduced the negative impact of their husbands’ behavior. One low-distress participant said her husband did not work or contribute financially, but then her mother-in-law helped with providing food. Another participant mentioned that support and advice from other women in the community helped her overcome conflict with her unfaithful husband, and “for the moment there’s a change in the household” (Low-distress IDI participant, Lulinda). Several low-distress participants reported good relationships with their husbands, including 1 that said her husband stayed with her hospitalized child and helped her in the fields: I don’t have any problem with my husband because we live well together with my mother-in-law…He doesn’t do anything in the house without consulting me. Troubles can come at any moment but when you live together you have to have a dialogue. (Low-distress IDI participant, Kaboke)
Almost twice as many participants in the high-distress group mentioned that breastfeeding would be difficult when feeling distressed. Low-distress participants sometimes mentioned problems with breastfeeding due to their poor nutritional status or lack of access to food: “Because I don’t eat well, when the child breastfeeds I feel pain in my breast. The child doesn’t eat and I have a reduction in milk” (Low-distress IDI participant, Nyakabere). Another participant said she didn’t have breast milk because she did not have enough access to food, and gave hot water to her child when she felt her milk was insufficient. She said that she did not feel differently about breastfeeding during times when she has a lot of problems. One participant reported that she only had insufficient breast milk when she was sick, but would continue to breastfeed the child because “it is their right” (Low-distress IDI participant, Kaboke). Similarly, another participant said she breastfed “like normal” even when experiencing problems (Low-distress IDI participant, Kalundja).
Several low-distress participants did not identify with the vignettes, and felt that women who experience these kinds of problems should continue with their normal activities: I can’t stay at the house [like the woman in the vignette] because I don’t have food. It’s better to go to the field instead of staying at the house, that doesn’t have any importance. I’m obliged to do agricultural work so that I can find food for my children. (Low-distress IDI participant, Nyakabere)
All participants faced similar challenges and stressors, but some may have been more acute for the high-distress participants, and high-distress participants tended to relate more to the topics discussed. Low-distress participants may have had greater social support, either through friends or extended family, which served as protective factors. Low-distress participants did not perceive that problems or worries affected their ability to breastfeed or function normally.
Discussion
We conducted qualitative research with women in South Kivu to understand their perspectives on sources of maternal psychological distress and the links between maternal psychological distress and child nutrition. The most salient theme to emerge was that poor relationships with their husbands were a significant source of distress for participants, with husbands often traveling for prolonged periods, taking other mistresses or wives, or abandoning their wives completely. Husbands were perceived to contribute little to the household financially, and the fact that many husbands had children with multiple women increased the financial strain on households. This finding has been reported in studies in other low-income countries. In Malawi, infidelity, abuse, and abandonment by husbands were stressors for women in the perinatal period, in addition to poverty, lack of support, and child illness. 28 One multicountry study found that lack of social support, poor relationships with partners, and husbands’ infidelity were a source of stress for postpartum mothers. 47 In 1 study in Kinshasa, the capital of DR Congo, new mothers said that partner infidelity and lack of support were problems they had that affected their children, 32 issues which also resonated among participants in this study.
Poverty and food insecurity emerged as other critical factors associated with psychological distress, with most participants struggling to provide food on a day-to-day basis, and worrying about how to pay for children’s school fees and hospital bills when they fell ill. These findings are consistent with quantitative studies that have linked poverty and food insecurity with depression symptoms. Studies in low-income populations in the United States have found that depression symptoms are associated with household food insecurity among adults 48 and pregnant women. 49,50 Studies among mothers in Tanzania and South Africa have found associations between household food insecurity and symptoms of depression and anxiety. 51,52 Food insecurity was also associated with depression symptoms among adults more generally in South Africa, and among adults in Ethiopia, food insecurity and stressful life events were associated with symptoms of depression and PTSD. 53,54 Relative poverty has also been identified as a correlate of depression symptoms among women in low-income country settings, 55 –60 and poverty has been associated with depression symptoms in women in high-income country settings as well. 61,62
Poverty, food insecurity, and psychological distress are highly interconnected, and 1 study conducted among rural, low-income women in the United States found bidirectional relations between food insecurity and depression symptoms. 63 However, there have been few other longitudinal studies and none in developing countries. Food insecurity may cause stress, which is a risk factor for depression and anxiety symptoms. 64 Additionally, certain micronutrient deficiencies are linked with changes in cognition, including mood, 65 which could explain a link between undernourished individuals in food insecure households and symptoms of anxiety and depression. Yet food insecurity may also result from depression symptoms, potentially through reduced functioning. There is also some overlap between measures of psychological distress and measures of food insecurity, as reporting to have worried about having enough food in the past day or night is a question included in the Household Food Insecurity Access Scale, and the presence of excessive worry is an anxiety symptom. 38,44 Thus, food insecurity and psychological distress might be thought about as interrelated problems occurring in the context of poverty and adversity.
Although Eastern DR Congo remains politically unstable with continued episodes of violence, the experience of conflict-related sexual violence did not emerge as a source of psychological distress for participants in the present study. Participants were more likely to discuss the death of children or extreme financial hardship as traumatic events in their lives. This is consistent with recent literature identifying a mediating role of ongoing stressors in the relationship between past traumatic events and mental health problems. 66,67 A recent study in Timor-Leste similarly found a mediating role for ongoing adversities, but also identified direct relations between past conflict-related traumas and maternal depression symptoms. 68 Several prior studies in South Kivu have focused on the mental health of sexual violence survivors or those who have experienced conflict-related trauma 40,69 –71 ; these studies occurred several years prior and in a geographic area that experienced greater insecurity, which could explain why sexual violence and trauma were not frequently reported in the present study.
Participants also did not mention intimate partner violence when discussing their relationships with their husbands. Although participants did not mention it specifically, intimate-partner violence is highly prevalent in DR Congo and may have contributed to poor spousal relationships. 45,72 A cycle of violence model has been proposed in postconflict settings in which men exposed to war-related traumatic events are at increased risk of enacting intimate partner violence and violence against children. 73,74 Among Congolese refugees in Uganda, exposure to conflict-related violence was associated with community and family violence in the past month. 75 Even though participants did not report experiencing conflict-related sexual violence, the cycle of violence model suggests that conflict may have contributed to higher levels of violence in the home.
Despite a context defined by poverty, food insecurity, and potential exposure to traumatic events, many participants exhibited resilience to these factors. Resilience refers to the capacity of some individuals to experience little disruption in functioning and emotional state after experiencing traumatic or adverse events. 76 Resilience may also mitigate severity of depression symptoms among individuals exposed to earlier traumatic events. 77 More resilient participants often described higher levels of social support. Low-distress participants reported good relationships with their husbands, or discussed social support mechanisms which may have mitigated the negative impact of husbands’ behavior and other stressors on their well-being. Social support has long been considered to have a “buffering” effect on stress. 78 In a study of people living with HIV/AIDS in Uganda, social support reduced the effects of food insecurity on depression symptoms, 79 and social support has been found to be a moderator for the effects of stressors on mental health symptoms in a variety of contexts. 80 –82
Participants in the present study often mentioned “thinking too much” (kuwa na mawazo mengi sana in Swahili) as a symptom of distress, which has been found to be a common idiom of distress across cultures. 83 Depression-like symptoms were described as having a “hurting heart,” an idiom which has emerged from research in other settings including Haiti, West Africa, and South Asia. 84 –86 Many associated weight loss with psychological distress, which could be due to loss of appetite, increased food insecurity, or a combination of both. Loss of appetite is a symptom of depression, and agitation (potentiating increased activity and subsequent weight loss) is a symptom of both depression and anxiety. 7 Studies in high-income settings have found significant associations between higher depression symptoms and underweight (Body mass index < 18.5 kg/m2) among adults, 87,88 and in 1 qualitative study in Malawi, women also described losing weight as a symptom of perinatal psychological distress. 28 Among pregnant women in urban Tanzania, not eating well and weight loss were attributed to lack of access to food and not as idioms of distress. 31
Participants perceived that stressful events and psychological distress were linked with difficulties breastfeeding, sometimes directly and sometimes mediated by perceived milk insufficiency due to stress or weight loss/poor maternal nutritional status. It has been previously reported that stressful events can suppress breast milk production, and social/partner support has also been identified as an important factor for breastfeeding. 89 –91 In Zimbabwe, both social support and perceived milk sufficiency were predictors of exclusive breastfeeding. 92 In rural Pakistan, maternal depression was associated with perceived milk insufficiency, and in Kenya, women from food insecure households were more likely to believe their milk to be insufficient. 18,93
Difficulties with complementary feeding were more often associated with mothers’ inability to afford adequate quantity and quality of foods for their children, which was also found in formative research conducted for the parent study. 37 One study in Bangladesh found that mothers perceived poverty as a barrier to feeding their children nutritious foods, 94 and lower household wealth has been identified as a correlate of suboptimal complementary feeding practices in quantitative studies as well. 95,96 Some participants described a decrease in affection toward their children in times of distress. This finding is supported by other literature showing an association between maternal depression, insecure attachment, and lower quality of mother-child bonding. 97,98 Insecure attachment is in turn related to feeding problems and nonorganic failure to thrive in infancy. 99
A number of studies have found an association between maternal mental health problems and child undernutrition, yet this is the first to assess mothers’ perspectives and awareness of how psychological distress affects maternal functioning, childcare and feeding practices, and child nutritional status. The validity of the findings was confirmed by key informant interviews, which supported the relevancy of the themes emerging from IDIs and FGDs. Another strength of the study was the purposive sampling technique, which achieved balance across the intervention groups.
In terms of limitations, intervention group assignment may have biased the responses of some participants. For example, PM2A group members received education and behavior change messaging on child feeding practices, thus they may have been more aware of child feeding problems. The vignettes that were used to facilitate the IDIs and FGDs may have been leading. However, there were differences in high and low distress participants’ responses, and the trauma-focused vignette did not resonate with most participants, which indicates that participants’ responses were not biased due to the vignettes. Another limitation was that the sampling strategy was based on participants’ cumulative mental disorder symptom score, representing HSCL-25 (measuring depression/anxiety symptoms), HTQ (measuring PTSD symptoms), and 14 other locally relevant symptoms, thus the study did not differentiate between those who had depression/anxiety symptoms versus PTSD symptoms. Although HSCL-25 and HTQ scores were highly correlated (r[34] = 0.90, P < .001), it is possible that symptoms of different disorders may have manifested differently in terms of their relations to child feeding behaviors, which this study did not capture. There was a 5-month gap in between when the maternal mental health assessment was conducted and when the IDIs and FGDs were conducted. Therefore, it is possible that classifications of low and high distress based on the mental health assessment were not accurate, if mental health symptoms were alleviated or worsened over the 5-month period in between assessments.
The study occurred in the context of a large-scale intervention designed to increase household income and food security, yet the experiences of the participants indicated that many remained disempowered, in a state of acute economic distress and lacking financial decision-making power in the household. Family-focused interventions that target fathers may be an effective way to address maternal mental health problems and child undernutrition, as the lack of a supportive husband was a factor contributing to both problems. In high-income countries, responsible parenting interventions have increased fathers’ involvement, but these interventions have not been widely evaluated with regard to maternal and child health outcomes. 100,101 In Uganda, a community-based cluster randomized trial of a parenting intervention focusing on childcare and maternal well-being targeted at mothers increased child cognition scores and reduced maternal depression symptoms, but had no impact on child growth. 102 The inclusion of fathers in such an intervention strategy may provide further benefits to both mothers and children.
Additionally, more resources should be devoted to breastfeeding counseling and support for mothers to continue breastfeeding also when distressed. Individual and group counseling and education by peers and trained health workers has been effective in promoting optimal breastfeeding practices, 103,104 and integrating these approaches with more dedicated psychosocial support for mothers has the potential to benefit mothers and children and warrants further evaluation.
In summary, husbands’ infidelity, abandonment, and lack of financial support were reported as a common source of psychological distress, along with poverty and food insecurity. High-distress participants perceived that psychological distress made them lose their appetite or lose weight, and also affected functioning, such as one’s ability to work and care for children. Psychological distress was perceived to be associated with insufficient breast milk, as well as a decrease in affection toward children. Low-distress participants tended to have better relationships with their husbands, greater social support from extended family or friends, and did not perceive there to be a link between psychological distress and breastfeeding or impaired functioning. Further research is needed to evaluate responsible parenting interventions targeted at fathers, which may have psychosocial benefits for mothers and children. The overwhelming psychological distress expressed by many participants indicates that policymakers and programs should increase resources for women’s mental health programs as part of maternal and child health care in impoverished, food insecure settings like DR Congo.
Footnotes
Authors’ Note
This research was presented in part as a poster at the Experimental Biology Conference, Chicago, IL, April 2017.
Acknowledgments
The authors wish to thank the staff of the Adventist Development and Relief Agency (ADRA) for their support of this research. Special thanks to Espoir Musafiri Kishimata and Jean Pierre Nzanzu for coordinating the logistics and to Jeanine Mukoko, Furaha Mawazo, and Linda Nsmire for facilitating the interviews and focus groups.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ADRA provided funding for the parent study through a USAID Office of Food for Peace Cooperative Agreement (AID-FFP-A-11-00006). Jillian Emerson received support from the Harry D. Kruse, Harry J. Prebluda, and Bacon Field Chow Fellowships from the Center for Human Nutrition, and tuition support from the Department of International Health, at the Johns Hopkins Bloomberg School of Public Health.