
Abstract
Objective
To evaluate the achievement of the International Headache Society (IHS) higher standards for migraine prevention in patients treated with calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) in real-world practice.
Methods
We retrospectively analyzed 307 migraine patients treated with CGRP mAbs at a single center. Monthly migraine days (MMDs) were assessed at baseline and during follow-up (1–24 months). According to IHS recommendations, migraine control was categorized as optimal (<4 migraine days/month), modest (4–6 days/month), or insufficient (>6 days/month). Patients were further classified by the timing of achieving optimal control.
Results
The percentage of patients achieving a ≥ 50% reduction in MMDs increased from 36.2% at month 1 to 71.0% at month 24; optimal control increased from 15.0% to 38.8%. Among patients with a ≥ 50% response, 38.7–55.7% achieved optimal control during follow-up. Migraine freedom remained relatively uncommon (1.6–10.1%). Patients who achieved optimal control early (≤3 months) had a lower baseline migraine burden, whereas nonachievers had a higher baseline disease burden and more prior preventive treatment failures.
Conclusions
CGRP mAbs were associated with substantial reductions in migraine frequency; however, achieving optimal control and migraine freedom remains challenging in real-world practice, particularly in patients with a higher baseline burden.
This is a visual representation of the abstract.
Keywords
Introduction
The efficacy of preventive migraine therapy is typically evaluated by changes in the number of monthly migraine days (MMDs) or monthly headache days, responder rates (≥50%, ≥75%, and 100% reduction), and headache-related disability assessed using the Migraine Disability Assessment (MIDAS) and Headache Impact Test-6. However, the degree of disturbance when a patient achieves a 50% response rate may differ between episodic migraine (EM) and chronic migraine (CM). In patients with CM, headaches may occur on more than 10 days per month even after a 50% response is achieved. The International Headache Society (IHS) recently proposed higher standards for migraine prevention to address this issue. 1
Calcitonin gene-related peptide (CGRP)-targeting preventive migraine therapies, including CGRP monoclonal antibodies (mAbs) and gepants, have emerged as important treatment options for migraine prevention. 2 The application of CGRP-targeting therapies may help achieve higher standards for migraine prevention. We analyzed the achievement of higher standards for migraine prevention and predictors of optimal control using real-world CGRP mAb data.
Methods
This study was conducted at a tertiary-care university hospital with a specialized headache outpatient clinic, and the data were derived from a previously reported real-world observational cohort of migraine patients. 3 The cohort included 307 patients with migraine who received CGRP mAbs for at least 3 months, with a follow-up of up to 24 months. Patients with EM and CM, defined according to the ICHD-3 criteria, were included and analyzed together. This study was approved by the Institutional Review Board of Dokkyo Medical University Hospital. All patients were informed about the observational nature of this study during outpatient visits and were given the opportunity to opt out. This study was reported in accordance with the STROBE guidelines for observational studies.
Clinical information, including headache characteristics, disease duration, aura, preventive medication use, and comorbidities, was obtained from the medical records. Headache-related disability was assessed by determining the MIDAS score at baseline. Based on these data, the percentage reduction in the number of MMDs from baseline was calculated. A ≥ 50% responder was defined as a patient with a ≥ 50% reduction in the number of MMDs from baseline at each time point.
According to the higher standards recommended by the IHS, patients were categorized into optimal control (fewer than 4 days with migraine or moderate-to-severe headache per month), modest control (4–6 days), and insufficient control (7 or more days). 1 Migraine freedom (0 migraine days) was analyzed separately. The percentage of patients who achieved optimal control was compared with the response rate at each time point. Migraine freedom (no migraine days) was also evaluated.
Next, patients were classified according to the timing of achieving optimal control: nonachievers, early achievers (≤3 months), late achievers (4–5 months), and very late achievers (≥6 months), based on previously reported classifications of response timing.3,4 Baseline characteristics were compared among these groups.
Statistical analysis
Continuous variables were assessed for normality using the Shapiro–Wilk test. Differences between groups were evaluated using the chi-square test or Fisher's exact test for categorical variables and analysis of variance or the Kruskal‒Wallis test with post hoc Bonferroni comparisons for continuous variables, as appropriate. Analyses at each time point were based on patients with available follow-up data, without imputation for missing data. A multinomial logistic regression analysis was performed to explore the factors associated with the timing of achieving optimal control, and nonachievers served as the reference group. Variables with a p value <0.2 in the univariate analyses (Table 1) were included in the model, and age was included as a covariate. Variables related to comorbidities (overall comorbidities and psychiatric disorders) were not entered simultaneously, and only the number of comorbidities was included in the final model to avoid multicollinearity. A p value < 0.05 for two-sided tests was considered to indicate statistical significance. Statistical analyses were conducted using IBM SPSS Statistics version 30 (IBM Corp., Tokyo, Japan).
Clinical features of migraine patients related to optimal control achievers.
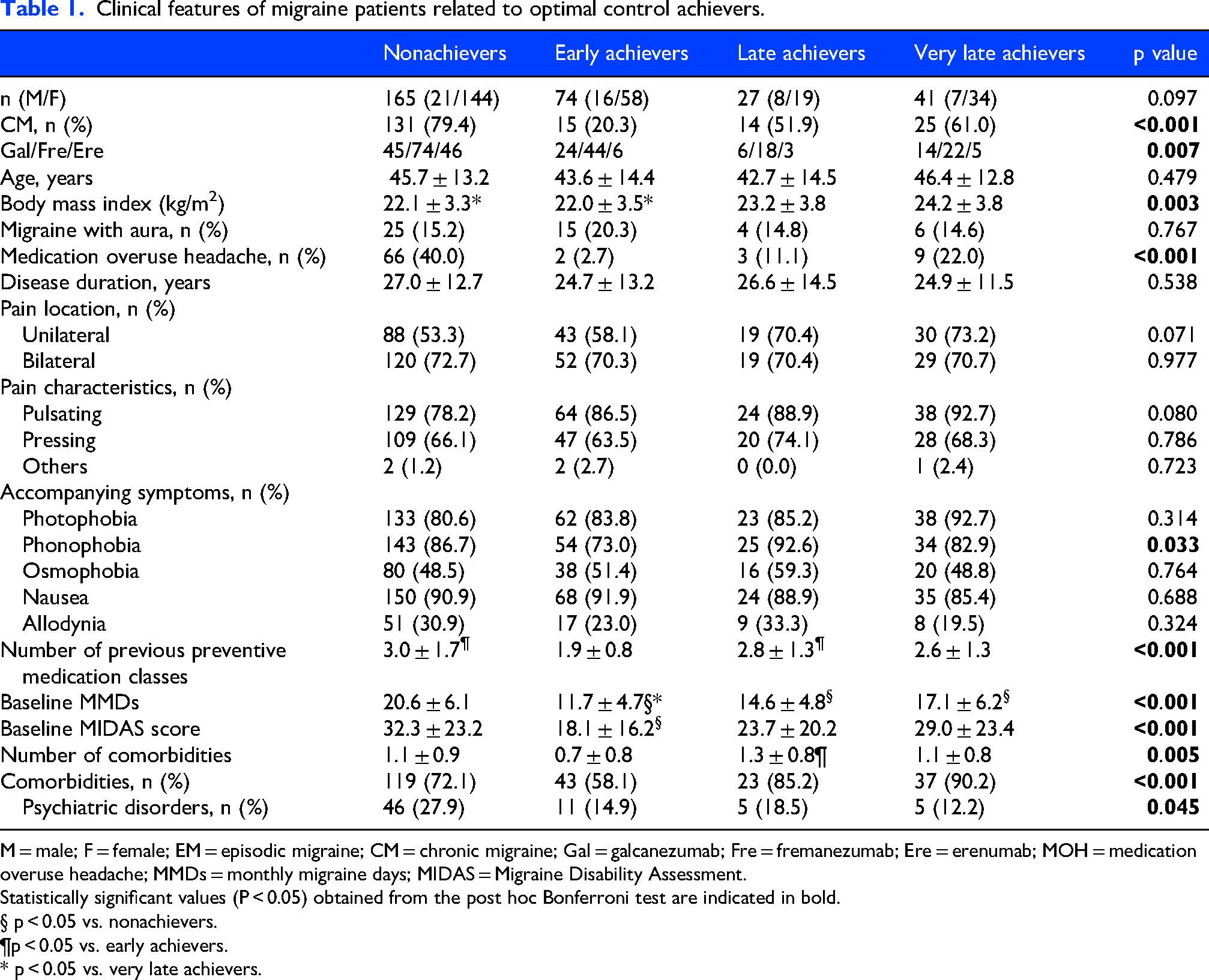
M = male; F = female; EM = episodic migraine; CM = chronic migraine; Gal = galcanezumab; Fre = fremanezumab; Ere = erenumab; MOH = medication overuse headache; MMDs = monthly migraine days; MIDAS = Migraine Disability Assessment.
Statistically significant values (P < 0.05) obtained from the post hoc Bonferroni test are indicated in bold.
§ p < 0.05 vs. nonachievers.
¶p < 0.05 vs. early achievers.
* p < 0.05 vs. very late achievers.
Results
The baseline characteristics of the patients are shown in Supplementary Table 1. In the total cohort and in the EM and CM groups, MMDs decreased from baseline to 1, 3, 6, 12, 18, and 24 months after CGRP mAb treatment (Supplementary Figure 1). Across the total cohort, the percentage of patients who achieved a ≥ 50% reduction in MMDs increased from 36.2% at month 1 to 71.0% at month 24, whereas the percentage of patients who achieved optimal migraine control increased from 15.0% to 38.8%, which was consistently lower than the ≥50% response rate (Supplementary Figure 2). Throughout follow-up, compared with the CM group, the EM group had higher rates of both ≥50% responses and optimal control.
Among patients with a ≥ 50% response at each time point, the migraine control status varied substantially. In the total cohort, the proportion of patients classified as achieving optimal control among those with a ≥ 50% response increased over time, from 38.7% at month 1 to 55.7% at month 18 and remained relatively high at 53.1% at month 24. Conversely, a considerable proportion of patients with a ≥ 50% response continued to be classified as having modest or insufficient control throughout follow-up (Figure 1A). Among the EM patients, the majority of those with a ≥ 50% response achieved optimal control at all time points, reaching 81.5% at month 18, with no patients classified as having insufficient control after month 12 (Figure 1B). In contrast, among CM patients, optimal control remained less frequent, accounting for 15.6% at month 1 and 42.9% at month 24, while a substantial proportion of patients with a ≥ 50% response continued to meet the criteria for insufficient control at all time points (Figure 1C). The distributions of optimal, modest, and insufficient migraine control among the patients with a ≥ 50% response rate across the three CGRP mAb groups are shown in Supplementary Figure 3.
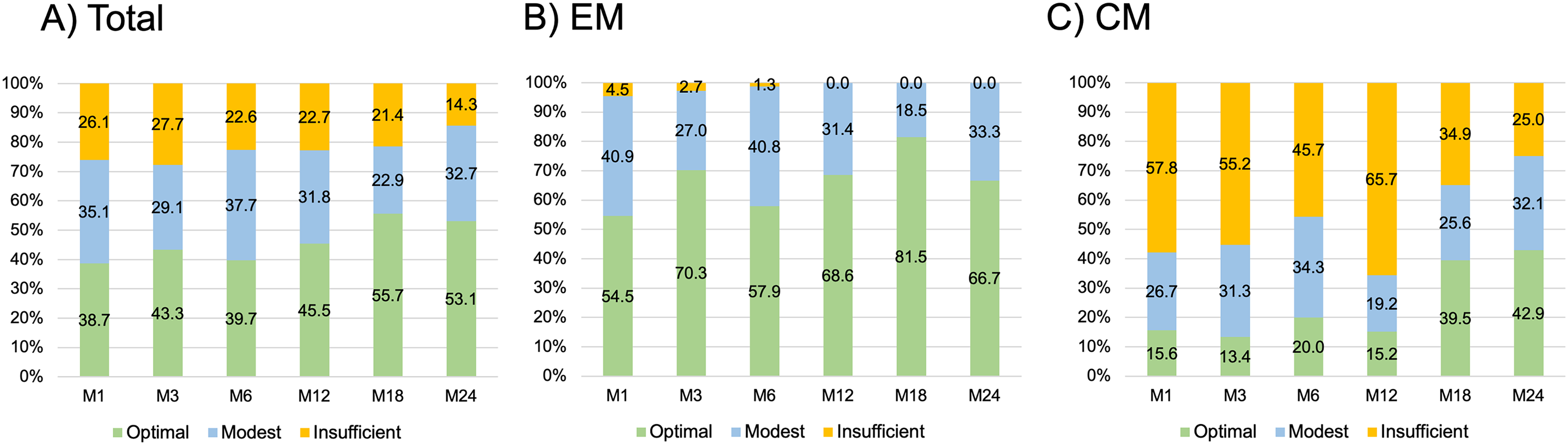
Proportion of patients who achieved optimal, modest, or insufficient migraine control among those with a ≥ 50% response rate at each time point
The percentage of patients who achieved migraine freedom (no migraine days) increased over time but remained relatively low, increasing from 11.6% to 28.0% among optimal achievers and from 1.6% to 10.1% in the overall cohort during the 24-month follow-up (Figure 2).

Proportion of patients who achieved migraine freedom over time among optimal achievers and the overall cohort
The clinical features of patients stratified according to optimal control achievement are shown in Table 1. During the 24-month follow-up period, 53.7% of the patients were nonachievers, and 46.3% achieved optimal control (early 24.1%, late 8.8%, and very late 13.4%). Nonachievers had the highest baseline migraine burden, including higher rates of CM and medication overuse headache (MOH), more prior preventive treatments, and higher baseline MMDs and MIDAS scores, whereas early achievers had the lowest baseline burden. Late achievers had an intermediate baseline burden, whereas very late achievers had fewer psychiatric comorbidities. According to the results of the multinomial logistic regression analysis in which nonachievers were used as the reference group, lower baseline MMDs were associated with earlier achievement of optimal control. Early achievement was also associated with fewer prior preventive treatments, the absence of phonophobia, and the use of galcanezumab, whereas a higher body mass index was associated with delayed achievement. For very late achievers, only a higher body mass index was associated with achievement (Supplementary Table 2).
Discussion
In our study, the proportion of patients who achieved optimal migraine control ranged from 15.0% to 38.8% during the follow-up period. These findings are broadly consistent with recent real-world evidence applying the IHS disease control framework in patients treated with eptinezumab, where approximately 15–20% achieved optimal control after 24 weeks. 5 Unlike prior studies, we specifically examined the relationship between conventional ≥50% response rates and higher-order treatment targets such as optimal control.
In our cohort, although the proportion of patients who achieved a ≥ 50% reduction in MMDs increased substantially over time, the proportion who achieved optimal control remained lower. Even among the patients who achieved a ≥ 50% response rate, a considerable proportion of patients continued to experience modest or insufficient control. These findings suggest that the conventional ≥50% responder definition may not fully capture the remaining disease burden, particularly in patients with a higher baseline migraine frequency.1,6
Migraine freedom, which is defined as the absence of migraine days, represents the highest standard of treatment success and reflects a clinical state in which patients are nearly free from migraine-related disability. However, the proportion of patients achieving migraine freedom remained relatively low in our cohort, reaching 28.0% among those achieving optimal control and 10.1% in the overall cohort at 24 months. These findings indicate that although CGRP-targeting therapies substantially reduce the frequency of migraine, complete remission remains difficult to achieve in routine clinical practice, which is consistent with randomized clinical trials in which only a minority of patients achieve complete migraine freedom. 7 One possible explanation for the difficulty in achieving complete remission may be the influence of mechanisms such as central sensitization, 8 as well as the substantial clinical and biological heterogeneity of migraine, 9 which may contribute to variability in treatment response.
Patients who achieved optimal control early had a lower baseline migraine burden, including fewer MMDs, lower MIDAS scores, and lower rates of CM and MOH. In contrast, nonachievers had the highest disease burden and more prior preventive treatment failures, consistent with previous reports that linked a higher baseline migraine frequency 10 and MOH 11 to a poorer treatment response. Very late achievers differed from nonachievers despite a delayed improvement, with more comorbidities but fewer psychiatric disorders, suggesting that a delayed improvement may occur even in patients with complex clinical profiles. Some recent real-world studies have suggested that migraine with aura may be negatively associated with the response to anti-CGRP mAbs 12 ; however, the findings remain inconsistent, and other studies have reported that the aura status is not associated with the treatment response.3,13
Previous studies of patients with CM have suggested that achieving ≤4 monthly headache days is associated with reduced acute medication use and improved patient-reported outcomes. 14 Therefore, optimal migraine control, which is defined as fewer than four migraine days per month, may represent a clinically meaningful treatment target. In addition, migraine-related quality of life has been shown to worsen with increasing headache frequency, highlighting the clinical importance of achieving a low headache frequency as a treatment goal. 15
Our findings suggest that achieving higher standards for migraine prevention may require optimized clinical strategies, including earlier initiation of effective preventive therapies and improved patient education regarding treatment goals and adherence. Recent studies suggest that earlier use of CGRP-targeting therapies may improve outcomes and reduce the migraine burden.10,16,17The greater improvement in achieving higher standards for migraine prevention among anti-CGRP-naïve patients, compared with non-naïve patients, following initiation of eptinezumab in a recent study 5 may reflect differences in baseline disease burden and prior treatment exposure, potentially indicating variations in disease stage at the time of CGRP-targeting therapy initiation. However, the complete remission or “cure” of migraine remains difficult to achieve, likely reflecting the complex and heterogeneous pathophysiology of the disorder.
This study has several limitations. First, this study was conducted at a single tertiary-care hospital, which may limit the generalizability of the findings. Second, the retrospective observational design may have introduced inherent biases. Because of the real-world observational design, the number of patients decreased during long-term follow-up. Additionally, analyses at each time point were based on available follow-up data without imputation for missing data, which may have introduced attrition bias. Baseline differences between patient groups may have influenced the observed outcomes, and residual confounding cannot be excluded. Furthermore, the analyses were primarily descriptive, and causal relationships or independent associations could not be established. Patient-reported outcomes, including the interictal burden and disability measures, were also not evaluated in relation to the treatment response, although baseline MIDAS scores were available. Moreover, the present study did not include gepants, which may also play a role in achieving higher standards for migraine prevention. Further studies are needed to clarify the clinical significance of achieving higher standards for migraine prevention in relation to these patient-reported outcomes.
Conclusions
CGRP mAbs were associated with substantial reductions in migraine frequency; however, achieving higher treatment targets, such as optimal control and migraine freedom, remained challenging in real-world practice, particularly in patients with a higher baseline migraine burden.
Clinical implications
Response rates may overestimate real-world migraine control, particularly in patients with a high baseline migraine burden.
Patients with a lower baseline migraine burden are more likely to achieve optimal control earlier.
Early initiation of effective preventive therapies may improve the likelihood of achieving optimal migraine control.
Optimal control (<4 migraine days/month) may represent a clinically meaningful treatment target in migraine prevention.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261453284 - Supplemental material for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies
Supplemental material, sj-docx-1-cep-10.1177_03331024261453284 for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies by Keisuke Suzuki, Shiho Suzuki, Saro Kobayashi, Mukuto Shioda, Hiroaki Fujita, Yasuo Haruyama, Ryotaro Hida and Koichi Hirata in Cephalalgia
Supplemental Material
sj-png-2-cep-10.1177_03331024261453284 - Supplemental material for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies
Supplemental material, sj-png-2-cep-10.1177_03331024261453284 for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies by Keisuke Suzuki, Shiho Suzuki, Saro Kobayashi, Mukuto Shioda, Hiroaki Fujita, Yasuo Haruyama, Ryotaro Hida and Koichi Hirata in Cephalalgia
Supplemental Material
sj-png-3-cep-10.1177_03331024261453284 - Supplemental material for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies
Supplemental material, sj-png-3-cep-10.1177_03331024261453284 for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies by Keisuke Suzuki, Shiho Suzuki, Saro Kobayashi, Mukuto Shioda, Hiroaki Fujita, Yasuo Haruyama, Ryotaro Hida and Koichi Hirata in Cephalalgia
Supplemental Material
sj-png-4-cep-10.1177_03331024261453284 - Supplemental material for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies
Supplemental material, sj-png-4-cep-10.1177_03331024261453284 for Real-world achievement of higher standards for migraine prevention with CGRP monoclonal antibodies by Keisuke Suzuki, Shiho Suzuki, Saro Kobayashi, Mukuto Shioda, Hiroaki Fujita, Yasuo Haruyama, Ryotaro Hida and Koichi Hirata in Cephalalgia
Footnotes
Acknowledgements
The authors thank Dr Tomohiko Shiina, Ms. Sanae Tani and Ms. Kaori Soma, Department of Neurology, Dokkyo Medical University, for their help with this study.
Ethical considerations
This study was approved by the Institutional Review Board of Dokkyo Medical University Hospital.
Consent to participate
All patients were informed about the observational nature of this study during outpatient visits and were given the opportunity to opt out.
Consent for publication
All authors have read and approved the final manuscript for publication in Cephalalgia
Author contributions
KS: Conceptualization, Data curation, Formal analysis, Writing – original draft.YH: Formal analysis, Investigation, Writing – review & editing. SS, SK, MS, HF, RH, KH: Investigation, Writing – review & editing. All authors contributed to data interpretation and approved the final manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. K Suzuki received lecture fees from Eli Lilly Japan, Daiichi Sankyo, Amgen, and Otsuka Pharmaceutical Co., Ltd, during this study. S Suzuki received lecture fees from Eli Lilly Japan, Daiichi Sankyo, Amgen, and Otsuka Pharmaceutical Co., Ltd, during this study. S Kobayashi, M Shioda, H Fujita, Y Haruyama, and R Hida have nothing to disclose. K Hirata received lecture fees from Eli Lilly Japan, Daiichi Sankyo, Amgen, Pfizer, and Otsuka Pharmaceutical Co., Ltd, during this study.
Data availability statement
The datasets from this study are available from the corresponding author upon reasonable request.
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.