
Abstract
Background
Residential deprivation is a long-established risk factor for poor health outcomes including migraine, depression and anxiety that are significant public health problems in Sweden and globally. Yet the relationship between residential deprivation and patterns of comorbidity among these three conditions is less understood. We aimed to estimate the magnitude and determinants of comorbid depression or anxiety among migraine patients in Sweden including the relationship between residential deprivation and comorbidity prevalence.
Methods
A nationwide register-based cross-sectional study was conducted of persons aged ten years or older in Sweden in 2015–2023. Comorbid depression or anxiety was defined as any depression or anxiety diagnosis or treatment during the migraine-exposed period (from three months before until three months after the first and last recorded migraine exposure in the study period). Small-area deprivation was based on an Index for Multiple Deprivation in Sweden (IMDIS) applied to 5984 small geographic areas. Prevalence ratios (PR) estimated the association between comorbidity and small-area deprivation adjusted for other covariates (age, sex, area of residence, birthplace) using Poisson regression models with robust error variance. We compared sick leave utilization (over fourteen days) for any reason in the migraine-affected years among migraine patients with or without comorbidity.
Results
There were 372,926 migraine patients in the study, and 35.7% (n = 133,219) had comorbid depression or anxiety. There was higher comorbidity prevalence among migraine patients in the most versus the least deprived areas (PR: 1.18, 95% CI: 1.17–1.20). Although the data have limitations, we found that one-third (31.9%) of migraine patients took sick leave (over fourteen days) for any reason during the migraine-exposed years, which rose to 50.9% among migraine patients with comorbid depression or anxiety.
Conclusions
More than one-third of migraine patients had comorbid depression or anxiety with higher prevalence of comorbidity in the most deprived areas. Common comorbid depression or anxiety among migraine patients underscores the need to consider all three conditions in clinical encounters especially for residents of more deprived residential areas.
Introduction
Migraine, depression, and anxiety are considered highly disabling disorders that continue to be significant public health problems in Sweden and globally.1,2 Each of these conditions not only impacts the person's health and well-being but may also result in income or productivity losses, sick leave and disruptions to social relationships.3–5 Women and people with lower socio-economic status are disproportionately affected by migraine, depression and anxiety.6,7
Migraine, depression and anxiety also have a common comorbid presentation, which further worsens the affected person's health, well-being, and quality of life.3–5 From a clinical perspective, comorbid presentation increases disease severity, worsens treatment outcomes, and further reduces the patient's overall quality of life and functioning. 8 The three conditions also share biological pathways and have known bidirectional relationships.8,9
Previous research on patterns and determinants of comorbid headache and psychiatric disorders have focused on individual-level risk factors such as age, sex and socio-economic status.9–14 Yet the relationship between residential deprivation and comorbidity patterns among the three conditions is less understood, despite the well-established role of residential deprivation in contributing to poor health outcomes including for migraine, depression and anxiety.15–20 Residential deprivation contributes to ill health through its links to stress, crime and violence, access to quality services, social cohesion, among other environmental factors. 15 It is therefore plausible that residential deprivation may exacerbate comorbidity across the three conditions although evidence of this outcome is limited.21,22 One study from Scotland found that comorbid depression, anxiety and chronic migraine in the adult population was higher in more deprived areas, 21 but further evidence is limited including from Sweden and for younger age groups who may show different comorbidity patterns than adults.21,22 To help fill this evidence gap, we aimed to examine the association between small-area deprivation and comorbid depression or anxiety among migraine patients aged ten years or older living in Sweden from 2015 to 2023.
Methods
Data sources
We conducted a register-based cross-sectional study based on multiple national and regional administrative registers that used the Swedish identification number unique to each resident to link individual information across data sources including: 1) the Total Population Register with data on population and household characteristics
Study population
All persons registered in Sweden throughout the study period who had a personal identification number and primary address assigned to one of 5984 small geographical areas established by Statistics Sweden (DeSO) were identified (n = 8,728,980). 23 We excluded persons under ten years old on 31 December 2023 (n = 200,782) since migraine, depression and anxiety onset typically occurs in adolescence. 6 We further excluded persons without any migraine exposure (n = 8,148,827) and those under ten years old on the date of the first recorded migraine (n = 6445). The final study population included 372,926 migraine patients and each DeSO included between four and 153 participants (median: 68, IQR: 55-81) (Figure 1).
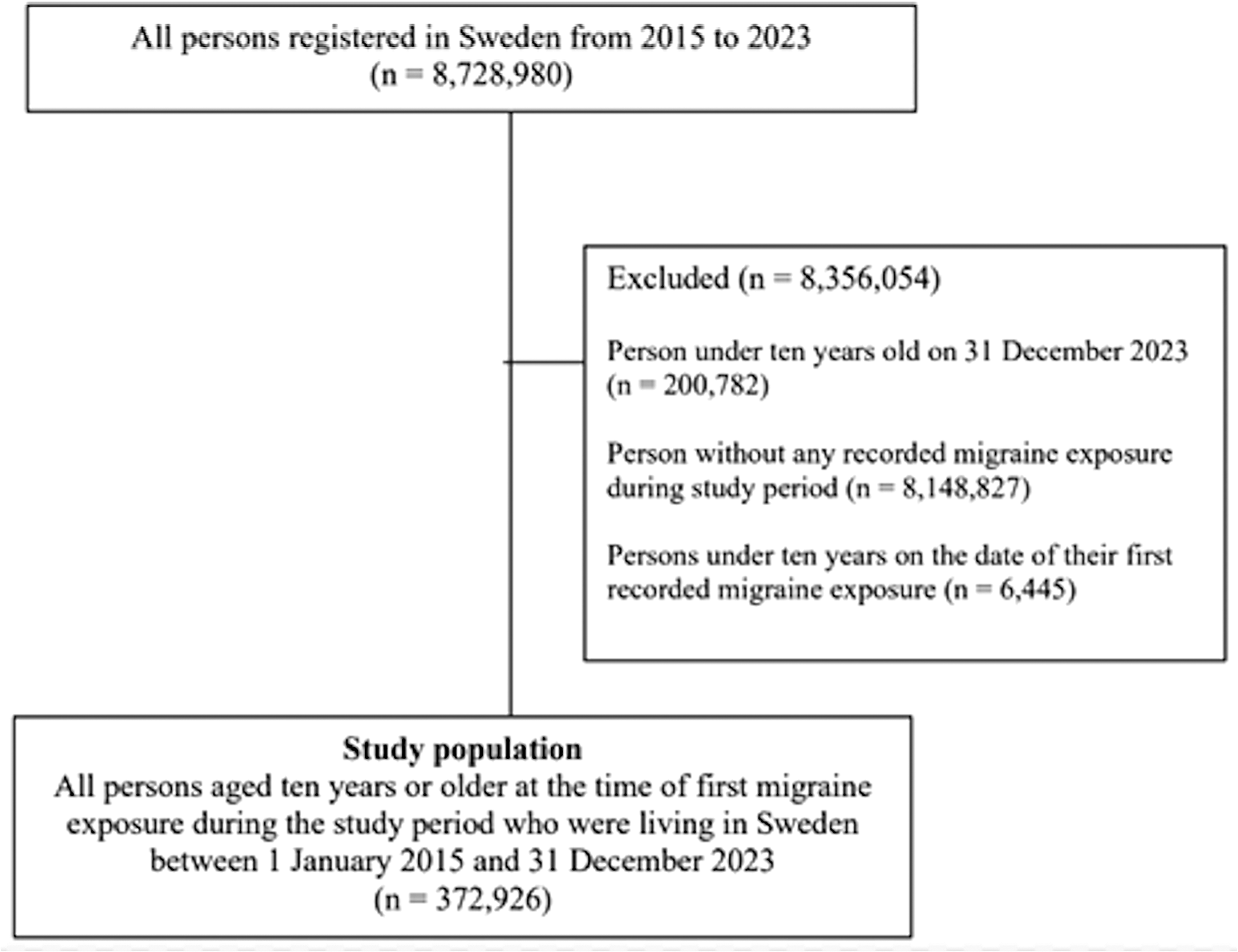
Flow diagram of inclusion criteria for the study population.
Migraine-exposed period
For each migraine patient, we defined a migraine-exposed period that started three months prior to the first recorded migraine date and ended three months after the last recorded migraine date during the study period. This was done such that each migraine-exposed person had a minimum exposure period of six months if there was only one date recorded for a migraine diagnosis or dispensed drug in the study period. The use of a migraine-exposed period to define comorbidity in our study that is based on data from healthcare and prescription registers is consistent with a disorder characterized by recurrent attacks in episodic or chronic form that frequently occur in the period between a medical visit or prescription fulfillment. 14
Migraine exposure was defined as having a diagnosis in primary, specialist outpatient or inpatient care during the study period, or having been dispensed migraine drugs identified in the National Prescribed Drug Register. Online Supplementary Table S1 lists the diagnosis and prescription codes for migraine measurement based on the Swedish adaptation of the International Statistical Classification of Diseases and Related Health Problems, 10th version (ICD-10-SE) and the Anatomical Therapeutic Chemical (ATC) classification system, respectively. Migraine diagnoses were derived from any inpatient admission or specialist outpatient visit during the study period, and any primary care visit in 17 of 21 regions from 2015 to 2017 when data were available. If the diagnosis date was missing (day and month), we imputed the date using the earliest prescription date in the same visit year with the assumption that the prescription date was the same as the primary care visit date. If there was no prescription in that year, the midpoint date in that same year was used to impute the diagnosis date.
Comorbid depression or anxiety measurement
Comorbid depression or anxiety was defined as having at least one depression or anxiety diagnosis or prescribed antidepressant during the migraine-exposed period. Depression or anxiety was defined as a diagnosis in primary, specialist outpatient or inpatient care, or a dispensed drug for depression or anxiety if no diagnosis was recorded during the study period. Online Supplementary Table S2 lists the ICD-10-SE and ATC codes that measured the outcome in these registers. We considered depression or anxiety jointly for the outcome since medications could not be easily separated for the two conditions. Depression or anxiety diagnoses were derived from any inpatient admission or specialist outpatient visit in the study period, and any primary care visit in 17 of 21 regions from 2015 to 2017 when data were available. If the diagnosis date was missing (day and month), we imputed the date using the earliest prescription date in the same visit year with the assumption that the prescription date was the same as the primary care visit date. If there was no prescription in that year, the midpoint date of the visit year was used to impute the diagnosis date.
Small-area deprivation
The level of deprivation for each of the 5984 DeSO areas in our study was estimated using an Index for Multiple Deprivation in Sweden (IMDIS), which has been described elsewhere. 24 IMDIS is a composite deprivation index that includes 15 indicators to measure four domains: 1) income and capital; 2) education; 3) employment; 4) housing. The IMDIS value for each DeSO area was ranked from least to most deprived and categorized into quartiles using the 25th, 50th, and 75th percentiles (very low, low, high, and very high deprivation levels). Each study participant was assigned the deprivation level for the DeSO where they lived based on their address in the Total Population Register in the year of their first migraine exposure. We assumed the deprivation level of each DeSO in the year 2015 remained unchanged throughout the study period. Recent research from Stockholm indicated that nearly 80% of neighborhoods had stable housing and socio-economic characteristics between 1990 and 2015. 25
Other covariates
Region and area of residence (urban, peri-urban, rural) as defined by Statistics Sweden was derived from the person's DeSO code for the address where they lived in the year of their first migraine exposure. 18 Other regression covariates included sex (male or female), birthplace (Sweden, Nordic outside Sweden, European Union (EU28) outside Nordic, Europe outside EU28, or another birthplace), and age at first migraine exposure (10 to 19 years; 20 to 29 years; 30 to 39 years; 40 to 49 years; 50 to 59 years; 60 years or more).
Statistical analyses
We calculated the median migraine-exposed period (in days) and frequency of comorbid depression or anxiety among persons with migraine in our study population. To examine comorbid determinants, we initially evaluated the extent of variation in the outcome across small geographic areas using a random-intercept model with a DeSO identifier as the random intercept. A small proportion of variance in the outcome was attributed to differences between DeSO areas (intra-class correlation (ICC) = 0.006) suggesting that a standard regression model was suitable to estimate coefficients with 95% confidence intervals (CI). We used Poisson regression models with robust error variance to estimate prevalence ratios (PR) for the association between comorbidity, small-area deprivation level and other covariates (age, sex, area of residence, birthplace). Since the outcome is common, we used prevalence ratios to better approximate relative risk. 26 We initially estimated crude PRs for the association between comorbidity and each covariate and subsequently adjusted for all covariates simultaneously in the final model. Wald tests were used to determine if there was an interaction between small-area deprivation and each covariate on the comorbid outcome. The level of statistical significance was set to 0.05. We analyzed data using Stata 18.1 (Stata Corp., College Station, TX).
Sensitivity analyses
Two sensitivity analyses were conducted for this study. In the first analysis, the definition of comorbid depression or anxiety was restricted to diagnoses only, e.g., prescribed drug was not included in the definition, since some antidepressants may be used to treat other conditions including chronic pain. In the second analysis, migraine, depression and anxiety were measured without primary healthcare data since these data were not available throughout the study period or for all regions.
Sick leave utilization
We conducted a descriptive analysis of certified sick leave use (over fourteen days) among migraine patients with or without comorbid depression or anxiety, including by region and personal characteristics. Sick leave use was defined as any payment received from the Swedish Social Insurance Agency for certified sick leave taken from employment that lasted more than fourteen days and was taken in the year(s) of the person's migraine-exposed period. The medical diagnosis motivating the sick leave was not recorded in our dataset nor were the exact sick leave dates beyond the year(s) the sick leave was taken by the person.
Results
Among the 372,926 patients diagnosed or treated for migraine in our analysis, a total of 133,219 (35.7%) had comorbid depression or anxiety according to the study definition. The median migraine-exposed period was 482 days (IQR: 182–2132 days). Comorbidity was higher among migraine patients living in the most versus the least deprived areas (37.6% vs 32.8%), women versus men (39.5% vs 24.5%), age group 40–49 years versus 20–29 years (43.1% vs 17.0%), and for those born within Europe (outside the European Union) compared to native-born Swedes (38.1% vs 35.9%) (Table 1).
Characteristics of migraine patients with or without comorbid depression or anxiety.

Associations with comorbid depression or anxiety
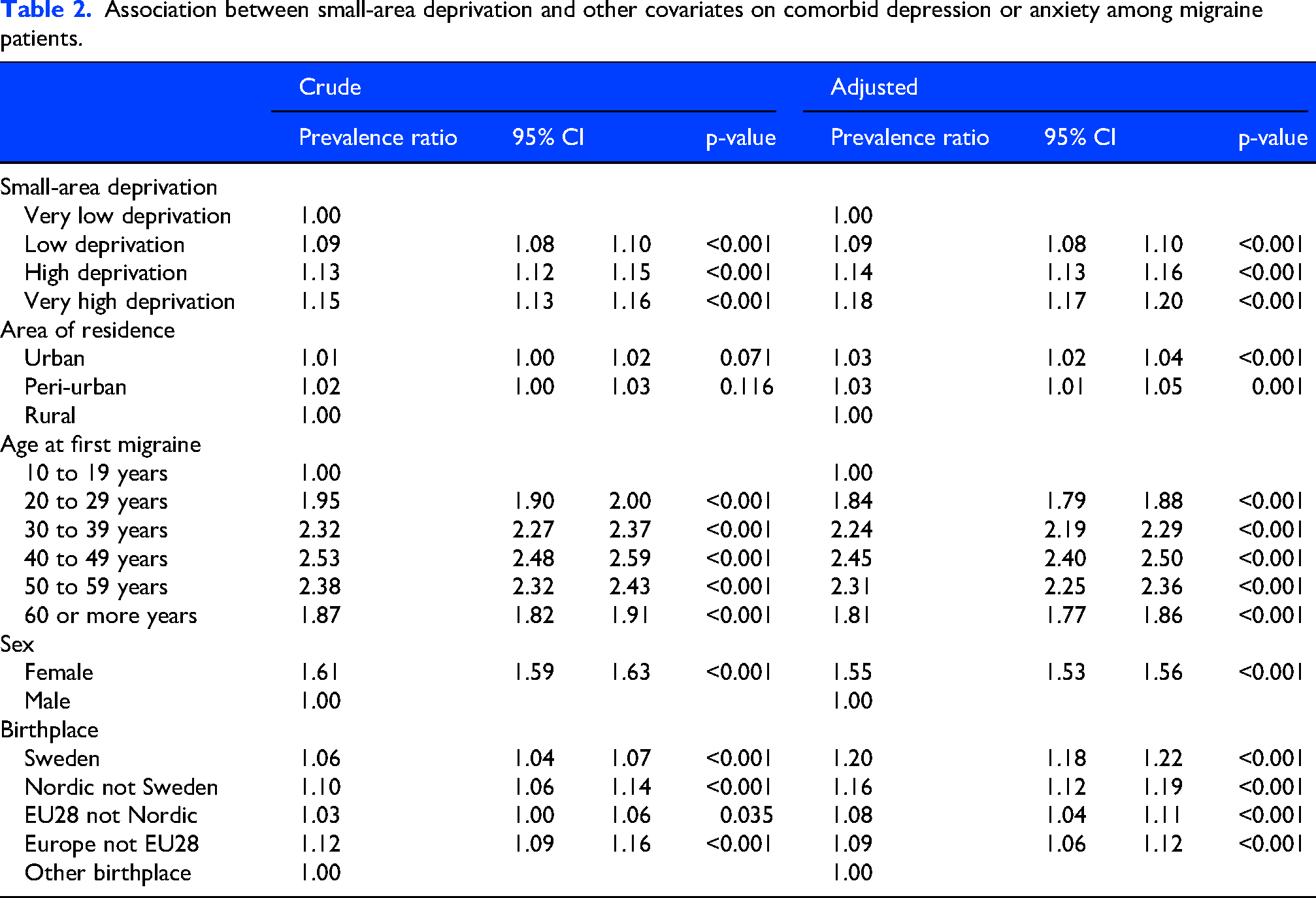
All covariates were significantly associated with comorbid depression or anxiety among migraine patients after adjustment (Table 2). For small-area deprivation, compared to migraine patients in the least deprived areas, there was higher prevalence of comorbid depression or anxiety among migraine patients in very high (PR: 1.18, 95% CI: 1.17–1.20), high (PR: 1.14, 95% CI: 1.13–1.16) and low (PR: 1.09, 95% CI: 1.08–1.10) deprivation areas. Similarly, urban (PR: 1.03, 95% CI: 1.02–1.04) and peri-urban (PR: 1.03, 95% CI: 1.01–1.05) residents with migraine had increased comorbid prevalence than their rural counterparts. Women with migraine had 55% higher prevalence of comorbid depression or anxiety than men (PR: 1.55, 95% CI: 1.53–1.56). Compared to migraine patients born outside Europe, there was higher comorbidity prevalence for all other groups including native-born Swedes (PR: 1.20, 95% CI: 1.18–1.22). Migraine patients in each older age group had higher prevalence of comorbid depression or anxiety than patients under 20 years.
Association between small-area deprivation and other covariates on comorbid depression or anxiety among migraine patients.
Stratification by small-area deprivation
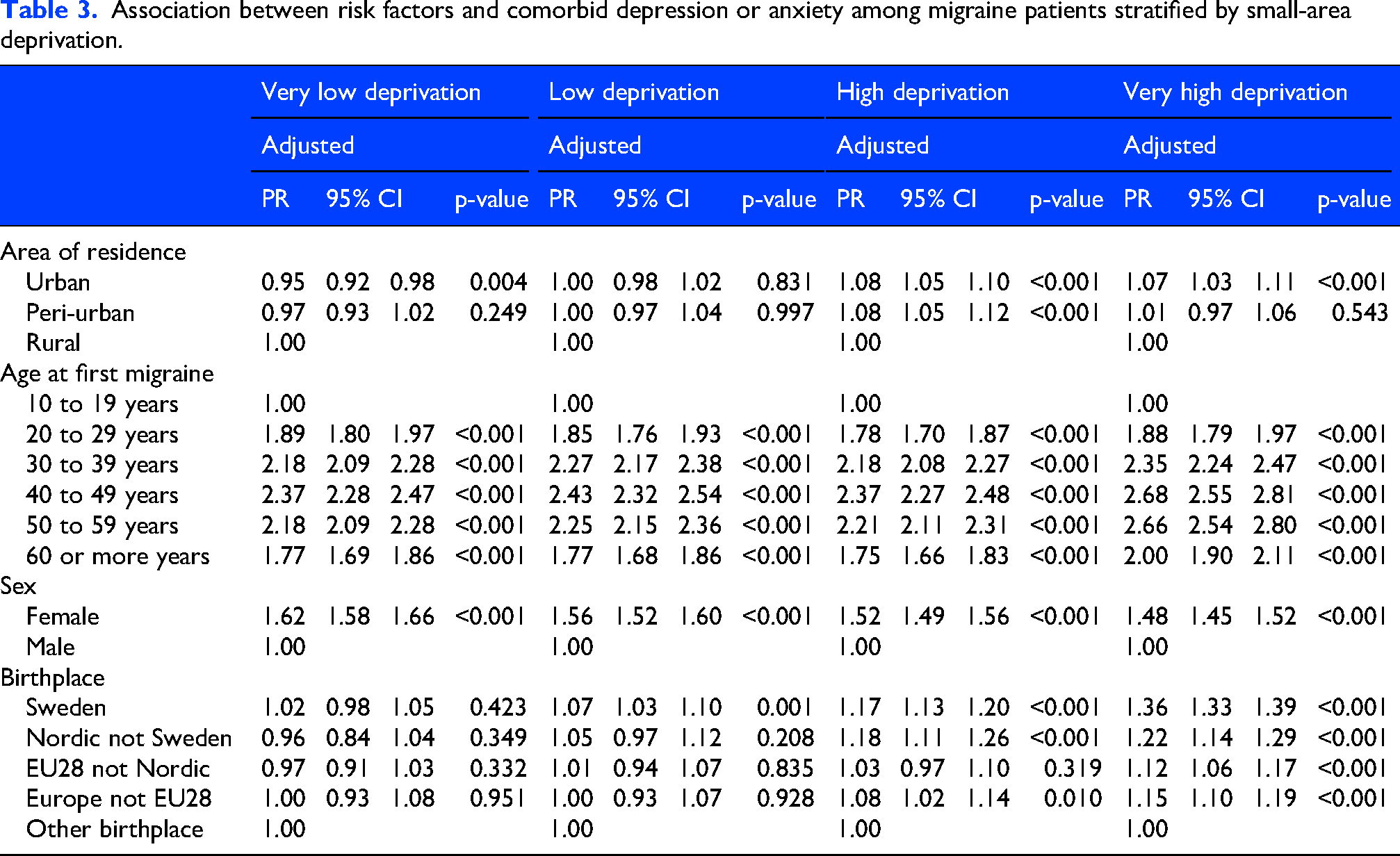
We found significant interaction terms for small-area deprivation level with age (p < 0.001), sex (p < 0.001), birthplace (p < 0.001) and area of residence (p < 0.001) on the comorbidity outcome. Specifically, the prevalence ratio of comorbid depression or anxiety among migraine patients associated with urban versus rural residence in the most deprived areas was 1.07 (95% CI: 1.03–1.11) while there was an opposite association in the least deprived areas (PR: 0.95, 95% CI: 0.92–0.98) (Table 3). There was also higher comorbidity prevalence for women versus men in the least deprived areas (PR: 1.62, 95% CI: 1.58–1.66) compared to the most deprived areas (PR: 1.48, 95% CI: 1.45–1.52). Similarly, in the most deprived areas, the prevalence of comorbid depression or anxiety among migraine patients associated with being a native-born Swede versus born outside Europe was 1.36 (95% CI: 1.33–1.39) while there was a non-significant association in least deprived areas (PR: 1.02, 95% CI: 0.98–1.05).
Association between risk factors and comorbid depression or anxiety among migraine patients stratified by small-area deprivation.
Sensitivity analysis
In the sensitivity analysis excluding primary healthcare data, 121,599 (32.6%) of migraine patients had comorbid depression or anxiety. There was no significant difference in adjusted coefficients compared to the main analysis (Online Supplementary Table S3). In the sensitivity analysis excluding prescribed drugs without a concurrent diagnosis, 57,839 (15.5%) of migraine patients had comorbid depression or anxiety. Compared to the main analysis, we found stronger relative associations between the comorbid outcome and small-area deprivation level, area of residence, and sex, while there was a weaker relative association between comorbidity and age at first migraine exposure (Online Supplementary Table S4).
Sick leave utilization
While sick leave utilization data in our analysis has important limitations, we found that 31.9% of the 372,926 migraine patients took certified sick leave (over fourteen days) for any reason during the years of their migraine-exposed period. Among the subset of migraine patients with comorbid depression or anxiety, 50.9% took sick leave for any reason in the exposed years (Table 4). Among all migraine patients, a higher proportion took sick leave (over fourteen days) if they lived in the most versus least deprived areas (32.2% versus 29.3%), lived in rural versus urban areas (34.0% vs 31.3%), were female (35.1% vs 22.1%), or were 50–59 years versus 20–29 years (41.0% vs 33.2%). The proportion of migraine patients taking sick leave (over fourteen days) for any reason during the migraine-exposed years varied between 30.0% in Stockholm and 30.4% in Skåne to 34.3% in three regions (Södermanland, Örebro, and Västerbotten).
Sick leave utilization (over fourteen days) for any reason in the affected years among migraine patients with or without comorbid depression or anxiety.

Discussion
Principle findings
In this nationwide register-based cross-sectional study, over one-third of migraine patients aged ten years or older had comorbid depression or anxiety with higher prevalence of comorbidity among patients living in more deprived areas, females, and older age groups. Findings suggest that comorbid depression or anxiety in migraine patients is common in our study population and reinforces the importance of considering all three conditions in clinical encounters, particularly in deprived residential areas where comorbidity occurrence is more frequent.
Comparisons with other studies
Numerous studies have reported increased rates of depression or anxiety among migraine patients although the magnitude of the comorbid occurrence has differed across analyses depending on the study context, population, data sources or measurement methods.9,13,27 Across several population-based surveys, between approximately one-fifth and one-half of migraine patients reported comorbid depression, anxiety or other mental health condition,5,10,12,27,28 including one study from Västerbotten (Sweden) where one-fifth of migraine patients reported any psychiatric disorder. 13 A recent analysis of Japanese insurance claims data showed that 10% of migraine patients had comorbid depression or anxiety, 4 which is a lower estimate that may be partly due to the focus on insured persons who sought care and received a diagnosis. In our study using health and prescription registers, one-third of migraine patients aged ten years or older had comorbid depression or anxiety, which is broadly consistent with prior estimates.
We further showed that the risk of comorbid depression or anxiety among migraine patients is higher among people living in more deprived areas, as well as for women, urban residents, older persons, and migraine patients born within Europe. Previous research has shown similar population patterns for comorbid depression or anxiety among migraine patients,11,12,29 although our analysis is one of the first to examine this relationship by small-area deprivation.21,22,30 One prior study from Scotland showed that migraine patients in more deprived areas had an increased risk of combined mental and physical conditions, including pain and depression. 22 This finding builds on other studies showing higher multimorbidity rates among residents of areas with greater deprivation.21,30
We also conducted stratified analyses by small-area deprivation level to examine variations in the associations of other factors on comorbid depression or anxiety among migraine patients. In this analysis, there was higher comorbidity prevalence among urban residents and older age groups in the most deprived versus the least deprived areas, while the opposite occurred for women. It could be that urban or older migraine patients in the most deprived areas are at higher risk of comorbid depression or anxiety than their counterparts in the least deprived areas potentially due to structural conditions of deprived areas (e.g., stress levels or worse healthcare accessibility). 15 Indeed, worse accessibility to specialized healthcare for migraine and mental health disorders in rural areas of Sweden is well-documented,1,31 which could lead to further underdiagnosis especially in deprived and remote rural areas. In contrast, for women compared to men, higher comorbidity prevalence remained across deprivation levels but was reduced in the most deprived areas compared to other deprivation levels. The complicated inter-relationship between gender and occupation or socio-economic status on health outcomes has been reported in other research and should be further explored in relation to residential deprivation and comorbidity patterns for migraine, depression and anxiety.32,33 These hypotheses merit further investigation to understand reasons for varying effects of risk factors for comorbid depression or anxiety in migraine patients across deprivation areas in our study.
Finally, we conducted a descriptive analysis of sick leave utilization for migraine patients with or without comorbidity based on available data. In our study nearly one-third of migraine patients took certified sick leave (over fourteen days) for any reason during the years of their migraine-exposed period, and this proportion rose to over half for migraine patients with comorbid depression or anxiety. Importantly, there are data limitations to consider in the interpretation of results. First, the diagnosis motivating the long-term sick leave is unknown and could be unrelated to migraine, depression, or anxiety (e.g., injury) leading to overestimation. At the same time, shorter sick leave periods are not captured in our dataset that are more common for migraine patients who typically experience acute migraine attacks. We therefore may additionally underestimate short-term work and productivity losses in our cohort given this issue. 4 Nevertheless, in this exploratory analysis of certified sick leave utilization (over fourteen days) for any reason in the migraine-exposed years, we described variations in utilization within Sweden by region and personal characteristics based on data available and as potentially additional evidence of associated income or productivity losses.34,35
Methodological limitations
The main strength of this study is the linkage of multiple administrative registers, including primary healthcare data, to enable research on a national level. At the same time, there are several limitations to consider when interpreting results. First, the reliance on healthcare registers to capture people affected by migraine, depression or anxiety will undercount cases at a population level due to healthcare gaps for these patients in Sweden. In addition, a large proportion of cases were ascertained from prescription registers alone. We included only migraine drugs that did not have multiple indications, and the registers did not include over-the-counter drugs used in migraine, such as NSAIDs. In contrast, antidepressants may be prescribed for unrelated conditions, e.g., chronic pain, which could overestimate the rate of comorbidity with depression or anxiety found in our study. We aimed to address this issue in sensitivity analyses using diagnosed cases only. Nevertheless, depression or anxiety identification in the main analysis relied heavily on prescription data (35.7% vs 15.5%) that could misclassify individuals and thus overestimate comorbidity prevalence. It could also result in biased associations if people with migraine taking antidepressants for other conditions are systematically different from those diagnosed with depression or anxiety. Moreover, primary care registers were available for only 17 of 21 regions (89% of the Swedish population) in the years 2015 to 2017 further contributing to this underestimation that could bias associations if conditions are differentially diagnosed at primary versus specialist care for specific regions and population groups (e.g., adolescents versus older adults), or if milder cases commonly diagnosed in primary care visits are less likely to lead to comorbid depression or anxiety. Second, the analysis of sick leave use for migraine patients captured only sick leave taken for at least fourteen days that was certified and reimbursed by national authorities, which underestimates work and productivity losses in migraine patients who commonly require shorter sick leave periods. 14 Moreover, the diagnosis motivating sick leave was not recorded in our dataset, and the work absence may be unrelated to these conditions making it difficult to attribute the loss of workdays or productivity to migraine, depression or anxiety. Third, observational studies are prone to residual confounding that makes causal inferences difficult. Fourth, small-area deprivation has measurement challenges including defining areas or indicators, and composite indices could obscure differences in areas even within the same deprivation level. Fifth, small-area deprivation level for each DeSO was measured in 2015 and the quartile grouping was assumed to remain unchanged throughout the study period. This assumption could result in exposure misclassification given changes in neighborhood characteristics over time. A recent study showed stability in the housing and socio-economic characteristics of over 80% of Stockholm neighborhoods between 1990 and 2015. 25 Although this research does not cover all of Sweden or the most recent period from 2015 onwards, it does suggest that the vast majority of the nearly 6000 small geographic areas in our analysis could likely be classified into the same deprivation quartile over the study period. Finally, estimates were not adjusted for individual-level socio-economic characteristics (e.g., income or education) although the small-area deprivation measure assigns the area-level value to each individual residing in the area. While this could increase risks of ecological fallacy, interpretations of results have focused on associations between comorbid depression or anxiety and small-area deprivation levels.
Conclusions
Our nationwide register-based cross-sectional study showed that approximately one-third of migraine patients aged ten years or older in Sweden had comorbid depression or anxiety, with higher comorbidity prevalence among women, older age groups, and people with migraine living in more deprived areas. Common comorbid depression or anxiety in migraine patients reinforces the importance of considering all three conditions, especially in more deprived areas where comorbidity occurrence is more prevalent.
Article highlights
35.7% of migraine patients in Sweden in 2015–2017 had comorbid depression or anxiety. Prevalence of comorbidity was higher among migraine patients in the most versus least deprived areas (PR: 1.18, 95% CI: 1.17–1.20). Although data have limitations, 31.9% of migraine patients took sick leave (over fourteen days) for any reason during their migraine-exposed years, which rose to 50.9% for migraineurs with comorbid depression or anxiety.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261430855 - Supplemental material for Comorbid depression or anxiety among migraine patients aged ten years or older living in Sweden in 2015 to 2023: A nationwide study
Supplemental material, sj-docx-1-cep-10.1177_03331024261430855 for Comorbid depression or anxiety among migraine patients aged ten years or older living in Sweden in 2015 to 2023: A nationwide study by Emily White Johansson, Ahmed Nabil Shaaban, Mattias Linde, Anna Ohlis, Mathias Mattsson, Sofie Gustafsson, Johan Holm, Christina Dalman and Emilie E. Agardh in Cephalalgia
Footnotes
Acknowledgments
We would like to thank Ulla Sollenberg PhD for contributions in the study design phase.
Ethical considerations
Ethical approvals for this study were received from the Swedish Ethical Review Authority (DNR: 2018/1339-31/5, 2018/2292-32, 2019-02185, 2021-00657 and 2022-03111-02, 2023-07509-02.2018/1339-31/5, 2018/2292-32, 2019-02185, 2021-00657, 2022-03111-02, 2023-07509-02, 2024-02816-02).
Author contributions
Concept and design: E.W.J., A.N.S., E.E.A., S.G. Additional input on design: all authors. Data acquisition, processing, and analysis: E.W.J., A.N.S., , M.M., E.E.A. Data interpretation: all authors. Statistical analysis: E.W.J., A.N.S., M.M., E.E.A. Drafting of the manuscript: E.W.J., A.N.S., E.E.A. Critical revision of the manuscript for important intellectual content: all authors. Accessed and verified the data and had responsibility for the integrity of the data and accuracy of the data analysis: E.W.J., A.N.S., M.M., E.E.A. Read and approved the final manuscript and had final responsibility for the decision to submit for publication: all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Pfizer Sweden.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() . J.H. and S.G. are employees and stock owners at Pfizer. M.L. has received honoraria from Abbvie, Lundbeck, Novartis, Pfizer, TEVA, and holds a patent related to a biofeedback intervention for migraine prophylaxis, Coinventor. No other competing interests have been declared.
. J.H. and S.G. are employees and stock owners at Pfizer. M.L. has received honoraria from Abbvie, Lundbeck, Novartis, Pfizer, TEVA, and holds a patent related to a biofeedback intervention for migraine prophylaxis, Coinventor. No other competing interests have been declared.
Data availability statement
Due to ethical restrictions, the individual level data used in this study are not publicly available. However, the data supporting the findings of this study can be obtained from Statistics Sweden (www.scb.se) and the Swedish National Board of Health and Welfare (![]() ).
).
Supplemental material
Supplemental material for this article is available online.