
Abstract
The course of disease and the predictive value of depression and anxiety in patients with migraine were prospectively examined. We recruited 393 migraineurs through articles in newspapers and performed a follow-up examination 30 months later. At baseline and follow-up, patients underwent a semi-structured interview, filled out the Headache Impact Test (HIT-6), Self-rating Depression Scale (SDS) and Self-rating Anxiety Scale (SAS) and they kept a headache diary for 30 days. One hundred and fifty-one patients (38.6%) were seen at follow-up. The baseline data of patients with and without follow-up were comparable. At follow-up the number of headache days per month had decreased from 9.6 ± 5.8 to 8.1 ± 6.3 (P < 0.001) and the proportion of patients with chronic headache (15.4%) and medication overuse (13%) had remained stable. SDS and SAS scores were associated with a high migraine frequency and high initial SDS scores predicted high migraine frequency at follow-up. This longitudinal study in unselected patients with migraine not excluding subjects with chronic headache, medication overuse, depression or anxiety does not point towards migraine as a progressive disease in the vast majority of patients and confirms the importance of psychiatric comorbidity.
Introduction
Migraine is one of the most frequent neurobiological disorders, with an average prevalence of 12% in the USA and 14% in Europe (1, 2). It imposes a tremendous impact on the individual patient by interfering with the patient's social and work life, lowering quality of life (3). The situation is worsened because migraine patients are at increased risk of psychiatric comorbidities such as depression or anxiety disorders (4), which add up to disease-related disability (5). Because of the great number of patients and the individual burden caused by migraine, clear characterization of the natural course of this disease is desirable.
Concerns about migraine being a progressive disorder originate from brain imaging and clinical studies. Subclinical posterior circulation stroke and diffuse white matter lesion load were found to increase with frequency of migraine attacks in one study (6). In another study the degree of impairment of iron homeostasis in the periaqueductal grey matter increased with disease duration in patients with migraine and chronic daily headache (7). As far as we know from clinical research, prognosis of migraine seems rather favourable. In a population-based study with two interviews 10 years apart, only 37% of patients with the initial diagnosis of migraine retained this diagnosis after 10 years, with most subjects evolving to a less disabling headache type (8). Another study described 36% of initial migraine patients being attack-free in a 12-year follow-up (9). Patient populations of speciality clinics do not seem to differ essentially from the general population: remission rates (defined as no attack within the last 1 or 2 years) were found to be between 35 and 42% (10, 11). Hence, there is a group of patients in whom migraine progresses, evolving from episodic to chronic headache with > 14 migraine days per month (9, 12). Several studies have attempted to identify risk factors for migraine progression to target early intervention for those at high risk. Among non-modifiable risk factors are young onset age, female gender and low socioeconomic status (9, 10, 13). Modifiable risk factors include attack frequency, obesity, medication overuse, caffeine overuse, stressful life events and snoring (14).
A shortcoming of all studies undertaken so far to examine the natural course of migraine is retrospective analysis of headache characteristics by semistructured interview. We therefore performed a longitudinal study using a semistructured interview as well as a diagnostic headache diary at baseline and follow-up to examine the course of migraine, evaluating headache characteristics, classifying each single headache attack recorded in the diary, and assessing use of medication and impact of psychiatric comorbidity.
Patients and methods
In 2002, we recruited patients with migraine through articles in the two most popular newspapers in Eastern Austria and performed a comprehensive diary study analysing a wide spectrum of factors related to headache in migraineurs (15). In this study, we present a 30-month follow-up examination. The study was approved by the local ethics committee and all patients gave written informed consent.
Inclusion and exclusion criteria have been published previously (15). In summary, patients aged ≥ 18 years were included, with at least one migraine attack per month according to the criteria of the International Headache Society (IHS). We included co-existing tension-type headache (TTH), but excluded patients with medication overuse headache, any other primary or secondary headache and severe other diseases. The inclusion and exclusion criteria were based on the first edition of the IHS criteria [International Classification of Headache Disorders (ICHD)-I] (16). We refrained from changing these predefined criteria after the second edition (ICHD-II) had been published, but used ICHD-II and ICHD-IIR (17, 18) for all other diagnoses throughout the study.
Included patients went through a semistructured interview, assessing biographical data, lifestyle, general medical history, headache characteristics and influence of headache on daily life. Following the interview, they were asked to fill out three validated questionnaires: the Headache Impact Test (HIT-6) (19), Self-rating Depression Scale (SDS) (20) and Self-rating Anxiety Scale (SAS) (21).
HIT-6 allows quantification of the impact of headache on daily life and consists of six questions. Each has five possible answers: never (6 points), rarely (8 points), sometimes (10 points), frequently (11 points) and always (13 points) and therefore offers a total score of minimum 36 to maximum 78. A severe impact on quality of life is presumed with scores of ≥ 60 (19).
SDS is a 20-item self-report measure of the symptoms of depression. Subjects rate each item according to how they felt during the preceding 7 days. Item responses are ranked from 1 to 4. The sum of the 20 items produces a score ranging between 20 and 80, a value of ≥ 40 suggesting clinically relevant depression (20).
SAS measures affective and somatic symptoms of an anxiety disorder. The structure of the SAS is like that of the SDS. It also consists of 20 questions, which refer to the past 7 days. The result of the SAS is obtained by summing up the scores. A cut-off value of ≥ 40 suggests the presence of a clinically relevant anxiety disorder (21).
Finally, patients were provided with a paper and pencil diary for 30 days and asked to return it filled out on a second visit. The diary covered questions regarding the presence, characteristics and treatment of headache and was to be filled in every night.
The questions about headache characteristics followed strictly the ICHD-II criteria of migraine and TTH and covered duration, laterality (unilateral or bilateral), quality (pulsating, pressing or other) and intensity (mild, moderate or severe) as well as the absence and presence of aggravation by routine physical activity, nausea, vomiting, photophobia, phonophobia and aura symptoms. In addition, patients filled in the trade names and units of medication taken for acute headache treatment. At data entry each medication was classified as analgesic/non-steroidal anti-inflammatory drug (NSAID), ergotamine or triptan.
Of the 446 persons recruited, 31 did not show up for the first visit and 415 were screened for the fulfilment of the inclusion and exclusion criteria. Eighteen subjects were excluded because of medication overuse (n = 12), pure TTH (n = 3), cluster headache (n = 1) and refusal to participate in the study (n = 2). Three hundred and ninety-seven patients were included, of whom 393 (99.0%) filled in all questionnaires and 327 (82.4%) returned a diary.
Thirty months later, all 393 patients were contacted again and invited for a follow-up examination. One hundred and fifty-three patients did not respond to three phone calls and a letter sent by mail, 86 patients refused further participation, and the current address and phone number of three patients could not be found. Finally, 151 (38.4%) patients were willing to participate again. They underwent a semistructured interview, filled out all required questionnaires and were provided with a paper and pencil diary for 30 days. A complete diary was returned by 123 patients (81.5%).
One of the authors (C.W.) was responsible for classifying each single headache attack documented in the diaries. The evaluation was blinded in two ways. First, C.W. did not see patients at any visit and was not involved in performing interviews. Second, for headache classification an anonymized
Statistical analysis
Statistical analysis was conducted with
Results
Patients without and with follow-up
At baseline, patients without follow-up (n = 242) differed from those with follow-up (n = 151) in three variables only, i.e. time since onset of migraine (21.4 ± 13.2 vs. 17.7 ± 11.6 years, P = 0.009), use of triptans (32.5 vs. 21.1%, P = 0.002) and consultation with a neurologist because of headache (73.8 vs. 61.7%, P = 0.01). All other variables, i.e. biographical data, other diseases, headache diagnosis, days with headache, headache characteristics, impairment due to headache, prophylactic medication, non-pharmacological treatment, HIT-6, SDS and SAS scores, showed no statistically significant differences. We therefore considered the patients with follow-up as representative of the entire group of patients at baseline.
Comparison of baseline and follow-up
Biographic data and general medical history
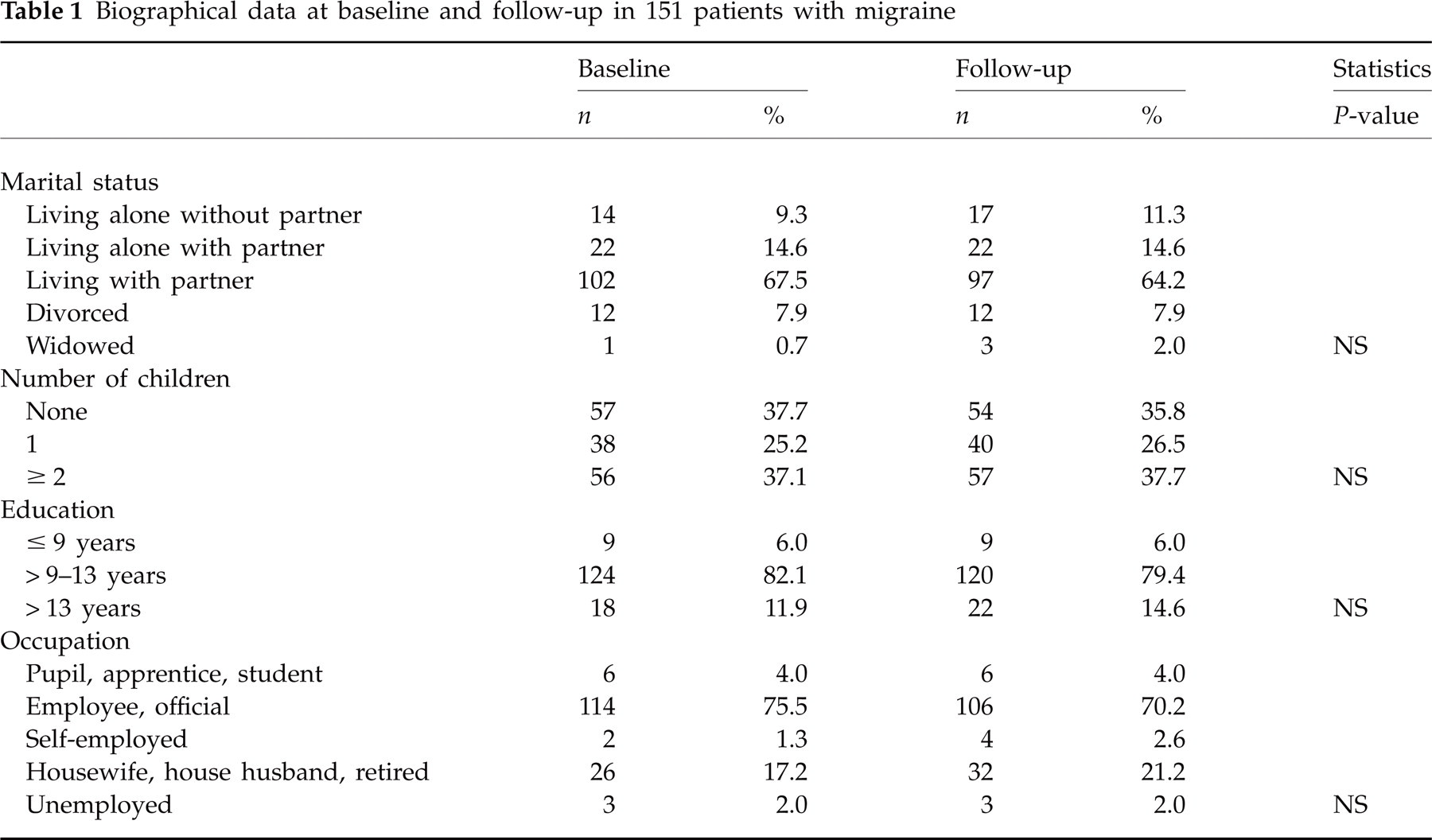
Of 151 patients seen at baseline and follow-up, 130 (86.1%) were female. The mean age was 42.1 ± 12.0 years at baseline and 44.6 ± 12.0 years at follow-up. Further biographical characteristics and details of the general medical history are given in Tables 1 and 2. There were no statistically significant differences other than daily non-headache medication, which was taken more often at follow-up.
Biographical data at baseline and follow-up in 151 patients with migraine
General medical history at baseline and follow-up in 151 patients with migraine
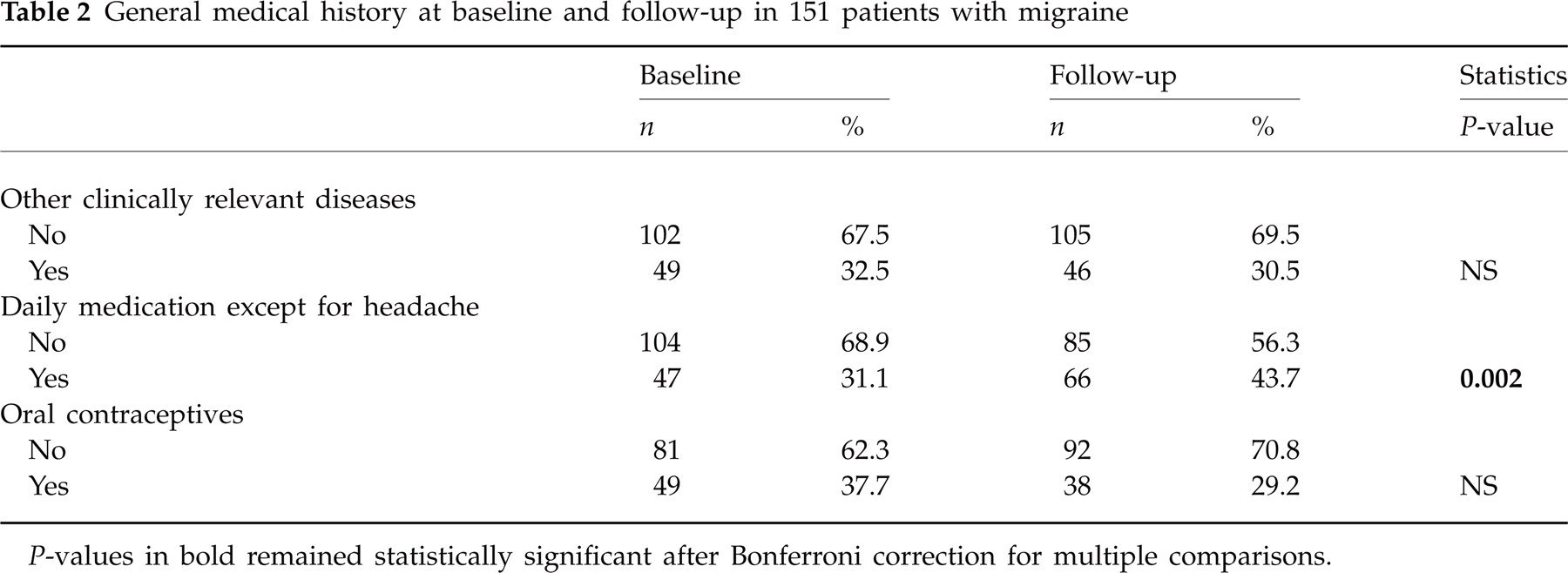
P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
Headache characteristics
For evaluating headache characteristics we used primarily the prospective data from headache diaries. A total of 117 (77.5%) patients returned a completed diary both at baseline and at follow-up.
Between baseline and follow-up, the average number of days with headache per month dropped significantly from 9.6 ± 5.8 to 8.1 ± 6.3 days (P < 0.001) according to the diaries and from 9.9 ± 6.2 to 8.2 ± 5.9 days (P < 0.001) according to the interviews. The number of headache days decreased by > 25% in almost one-half of patients, increased by > 25% in 16% and showed a decrease or increase of ≤ 25% in the others. Similar figures were given by the patients retrospectively in the semistructured interview (improvement 43%, deterioration 16%, no change 41%).
Further details of the evolution of headache characteristics are shown in Table 3. Headache frequency decreased statistically significantly. This decrease was seen in patients with episodic headaches, whereas the prevalence of chronic headache remained stable. Five patients evolved from chronic to episodic headache and five from episodic to chronic. In addition, headaches of any duration and those of mild intensity had decreased, whereas moderate or severe headaches and the prevalence of associated symptoms had not changed from baseline to follow-up.
Headache characteristics at baseline and follow-up according to a 30-day headache diary in 117 patients with migraine

P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
Headache diagnoses
The headache diagnoses derived from the semistructured interview changed significantly from baseline to follow-up (Table 4), and this was true for the main diagnosis as well as for possible additional headache diagnoses. Concerning the main diagnosis, the most prominent change was an increase in probable migraine. The number of patients reporting different types of headache had decreased, and this was due to less frequently reported TTH.
Headache diagnoses at baseline and follow-up according to a semistructured interview in 151 patients with migraine

P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
The headache diagnoses obtained from the headache diaries revealed a different pattern (Table 5). The number of patients with at least one attack of migraine with aura and TTH had decreased, whereas overall migraine and probable migraine had remained stable. The difference in migraine without aura did not reach the level of statistical significance after Bonferroni correction for multiple comparisons (Table 5). Regarding the number of days with a specific headache type, we found a decrease in migraine with aura and TTH and no change in the other headache types. In contrast to the interviews, the diaries revealed two or more different types of headache in the vast majority of patients. Similar to the interviews, the diaries showed a statistically significant decrease in multiple diagnoses at follow-up.
Headache diagnoses at baseline and follow-up according to a 30-day headache diary in 117 patients with migraine

P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
For each diagnosis the mean number of days as well as the number of patients are given.
Quality of life, depression and anxiety
Asking patients to rate headache-associated impairment of quality of life and productivity on a four-point Likert scale showed a statistically significant improvement from baseline to follow-up (Fig. 1). The number of patients with a HIT-6 score of ≥ 60 and a SAS score of ≥ 40 had decreased, whereas the number of patients with an SDS score of ≥ 40 was unchanged at follow-up (Fig. 2).

Impairment of quality of life and productivity measured by means of a four-point Likert scale in 151 patients with migraine at baseline and 30 months’ follow-up. P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.

Results of questionnaires on impact of headache (HIT-6), depression (SDS) and anxiety (SAS) at baseline and 30 months’ follow-up in 151 patients with migraine. P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
HIT-6, SDS and SAS scores increased statistically significantly with the frequency of migraine at baseline and at follow-up (details not shown), but they were not related to the frequency of TTH. High initial SDS scores (but not SAS scores) predicted high migraine frequency at follow-up (Pearson correlation coefficient = 0.28, P = 0.003).
Management and therapy of headache
Regarding medical management, it is important to point out that none of the patients was treated at our clinic. Until baseline, 8.6% of patients had not seen a doctor because of headache, 72.9% had presented themselves to a general practitioner and 73.5% to a neurologist. During the follow-up period the consultation rates were 18 and 42.6%, respectively, and 43.7% had not seen a doctor.
Patients who had consulted a doctor during follow-up used triptans more often than those who had not seen a doctor (56.5 vs. 26.7%, P < 0.001). The differences in baseline HIT-6 scores (60.5 ± 5.8 vs. 58.1 ± 5.8, P = 0.01) and use of prophylactic medication (17.6 vs. 4.5%, P = 0.014) did not remain statistically significant after Bonferroni correction. SDS and SAS scores were similar in the two groups.
According to the interviews, headache treatment showed only minor changes from baseline to follow-up (Table 6). The small number of patients using no headache medication at all had increased statistically significantly, and there was a trend towards more frequent use of triptans and prophylactic medication, which failed statistical significance, however.
Headache treatment according to a semistructured interview in 151 patients with migraine
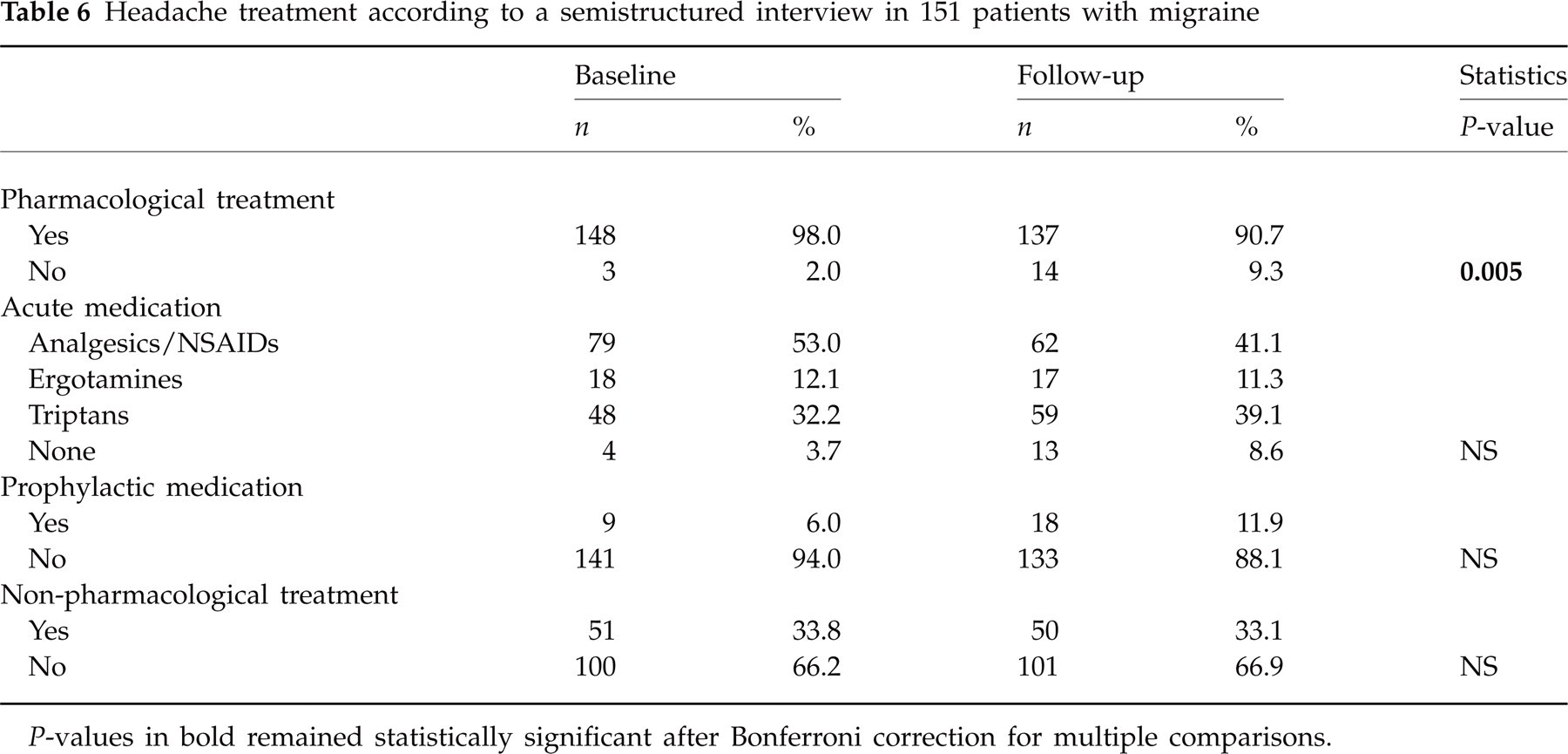
P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
According to the headache diaries, analgesics and NSAIDs were used most frequently (Table 7). There was a statistically significant increase in days without use of acute medication and a correlating trend of decrease in the use of analgesics and NSAIDs at follow-up compared with baseline. The days with triptans and ergotamines did not change significantly.
Acute treatment of headache according to a 30-day headache diary in 117 patients with migraine

P-values in bold remained statistically significant after Bonferroni correction for multiple comparisons.
The total number of patients overusing medication was the same at baseline and follow-up. Medication overuse was present at both points in eight patients and at only one point in seven patients each.
Discussion
To our knowledge, this is the first study to examine the course of migraine with both a semistructured interview and a headache diary. Our major findings do not point towards migraine as a progressive disease in the vast majority of patients. Recruiting migraineurs with at least one migraine day per month through newspapers, we found a decrease in headache days of 15% over a period of 30 months. This improvement was largely due to a decrease in days with co-existing TTH, which was markedly underestimated in the interviews compared with the diaries. The total number of migraine days did not change and the percentages of patients with chronic headache and medication overuse according to ICHD-IIR (17) remained stable. Psychiatric comorbidity, i.e. depression and anxiety disorder, increased with the number of migraine days, but not with the frequency of TTH. Depression at baseline was related to migraine frequency at follow-up.
Considering that almost 90% of patients had no prophylactic medication and only one-third had any non-pharmacological therapy during follow-up, our findings widely reflect the natural course of migraine.
The drop-out rate in our study was in the upper range compared with the relevant literature (8–12, 23). This may also be explained by the study design requiring a headache diary not used for follow-up previously. To ensure that results were not weakened by selection bias, we compared baseline data of patients with and without follow-up. There was a difference neither in biographical data and other diseases nor in headache diagnoses and characteristics, quality of life and psychiatric comorbidity. Patients without follow-up had a longer history of migraine, were more likely to have visited a neurologist and were more likely to use triptans. This could suggest that they were slightly more severely affected, but headache diaries of patients with and without follow-up did not differ from each other. Furthermore, in Austria prescription of triptans requires consultation with a neurologist according to regulations of the social insurance system. In summary, there is very little evidence for selection bias and the follow-up sample can be considered as representative of the whole group of baseline patients.
Patients were astonishingly accurate in estimating their headache frequency. According to the interviews, headache days decreased from 9.9 per month at baseline to 8.2 at follow-up. The figures derived from the headache diaries, i.e. 9.6 and 8.1 were almost the same. Similarly, patients were accurate in estimating the course of headache over the 30-month follow-up period.
The proportion of patients with new-onset chronic headache was 4% among our patients, thus being comparable to a community-based study (23) reporting 3%, but much lower than 14% found in a clinic-based study (12). Scher et al. (23) described the risk of new-onset chronic headache increasing exponentially with a frequency of three or more attacks per month. Considering that 97% of our patients recorded at least three headache days in their diary and 22% had a clinically relevant depression, the percentage of patients who evolved into chronic headache seems to be low in our study.
The headache diaries used at baseline and follow-up allowed diagnosis of each single headache attack according to ICHD-II without considering the use and efficacy of acute medication, however. Previous studies did not differentiate between migraine and TTH at follow-up (23) or relied on interviews and questionnaires (8, 9, 12).
Comparing the headache diagnoses according to the semistructured interviews with the diaries showed several discrepancies. TTH was considerably underdiagnosed and migraine without aura was slightly overdiagnosed in the interviews. Accordingly, a bias towards underestimation of TTH in previous studies not using diaries cannot be excluded. The large proportion of probable migraine in the diaries may be explained by the use of acute medication preventing the development of a full attack. Regarding the evolution of headache diagnoses from baseline to follow-up, the most prominent finding was a decrease in TTH according to the interviews as well as the diaries. The changes in migraine diagnoses were less marked. Shifts in headache diagnoses have been shown in previous longitudinal studies in adults as well as in young patients (8, 24). Over a period of 10 years Nachit-Ouinekh et al. (8) found that migraine evolves to a less disabling headache type in the majority of patients. The present study covering a shorter period of 30 months does not confirm this finding, since the improvement seen in our patients was largely due to a decrease in TTH, whereas overall migraine remained stable.
Concerning the patients’ quality of life, it has been suggested previously that a decrease of headache frequency rather than diagnostic category is crucial. Headache frequency has been found to be one of the major determinants defining disease-related disability (25). We found a decrease in the number of patients reporting a severe impact of headache on quality of life and productivity at work as well as a decrease in HIT-6 scores parallel to the decrease in headache days, even though the number of migraine days remained stable.
The close relation between migraine and psychiatric disorders such as depression and anxiety disorders has been well documented. Migraineurs have an up to fourfold increased risk of comorbid depression and a more than fivefold risk of a comorbid anxiety disorder (26). In our sample, 25% of patients could be classified as having a clinically relevant depression at baseline. This number decreased, statistically not significantly, to 22% at follow-up and is therefore in line with or somewhat lower than previous findings (5, 27–29). Anxiety scores were above the cut-off value in 24% of patients at baseline and in 14% at follow-up, showing a significant decrease over time. Prevalence data in relevant literature range between 18 and 47% (5, 29). High comorbidity of migraine and psychiatric disorders, as well as the bidirectional relationship—meaning patients with migraine having an increased risk of developing depressive disorders and patients with depression having an increased risk of developing migraine (30)—led to speculations about a common neurobiology. The current hypothesis focuses on a dysfunction of dopaminergic and serotonergic systems (31). As a first step for common genetics, a polymorphism of the serotonin transporter, which has been associated with anxiety disorders and migraine, was found to be significantly more prevalent in migraineurs, who also exhibited higher anxiety scores than controls (32).
In two studies the level of depression and anxiety was related to the frequency of attacks (33, 34). Our study further supports this relationship. In contrast to previous surveys describing an equal correlation of anxiety and depression to migraine and TTH, we only found a correlation with migraine, but not with TTH. Concerning prognosis, previous clinical studies on headache progression did not focus on (8–11, 23) or exclude patients with major depression (8–11, 23). In our sample, a high SDS score at baseline predicted a high migraine frequency at follow-up, but this was not true for SAS scores.
Finally, when assessing headache treatment, we found a reduced need for acute medication, claimed by patients in the interviews and correspondingly documented in the headache diaries—a further hint for a favourable prognosis. Overuse of acute medication has been identified as a risk factor for development of chronic headache (12, 35). In our study, the prevalence of medication overuse according to ICHD-IIR (18) did not change from baseline to follow-up, and only half of these patients—seven at baseline and eight at follow-up—had chronic headache. Even though the average number of migraine days exceeded four per month, only a small minority of patients had prophylactic medication and just one-third had used non-pharmacological prophylactic therapy.
The favourable prognosis seen in our patients is only one side of the coin. The other side is persistent disability in many sufferers indicated by follow-up findings of more than four migraine days per month, > 70–80% of patients feeling moderately or severely impaired and almost 60% of patients with HIT-6 scores > 60.
The findings of our study may be limited by the large number of dropouts, even though baseline data of patients with and without follow-up did not differ statistically significantly with very few exceptions. Furthermore, we included volunteers recruited through newspapers with at least one migraine attack per month and therefore our data cannot be transferred to the general population. Finally, our study does not cover the whole period between baseline and follow-up.
In conclusion, this longitudinal diary study in unselected patients with migraine not excluding subjects with chronic headache, medication overuse, depression or anxiety does not point towards migraine as a progressive disease in the vast majority of patients and confirms the importance of psychiatric comorbidity. Despite the improvement seen over time, many migraineurs remain considerably affected.
Footnotes
Acknowledgements
The authors thank Sonja Schobesberger for editing the English text.