
Abstract
Objectives
To evaluate the prevalence and the association of psychological disturbance in migraine patients with allodynia.
Methods
We recruited 434 migraine patients from an outpatient clinic. The participants completed three self-administered questionnaires, including a headache questionnaire, an allodynia symptoms checklist, and the Hospital Anxiety and Depression Scale (HADS).
Results
Among the migraineurs, 48.4% participants reported allodynia. The HADS total score (15.5 ± 7.8 vs. 13.7 ± 8.5, p = 0.022) and anxiety subscore (9.1 ± 4.5 vs. 7.6 ± 4.7, p = 0.001) were higher in migraineurs with allodynia than in those without allodynia. The anxiety subscore in patients with moderate to severe allodynia, mild allodynia, and no allodynia were 10.0 ± 4.5, 8.4 ± 4.3, and 7.6 ± 4.7 (p < 0.001, by one-way analysis of variance). Among patients with moderate to severe allodynia, there was a trend of higher depression subscore (7.1 ± 4.0, p = 0.059) than those with no (6.1 ± 4.4) or mild allodynia (5.8 ± 4.0). In a regression model, the presence of allodynia is an independent risk factor for clinically significant anxiety. Moderate to severe allodynia is an independent risk factor for clinically significant depression.
Conclusions
In migraineurs, the severity of cutaneous allodynia was associated with their mood status, especially anxiety.
Introduction
Cutaneous allodynia (CA) is a pain sensation in response to non-nociceptive stimulation. The frequency of CA is higher in the migraine population than in patients with other type of headaches (1). Among migraineurs, the prevalence of CA is approximately 60% to 75.3% (1–4).
Burstein and colleagues proposed an underlying mechanism of allodynia development in a temporal pattern during migraine attack (5). According to this proposal, initial intracranial hypersensitivity during a migraine attack might be due to sensitization of the trigeminal ganglion. Subsequent CA within the referred area might be due to the sensitization of trigeminal neurons in the brainstem, and the extracephalic allodynia that follows might be explained by sensitization of thalamic third-order neurons. Thus, both peripheral and central sensitizations are responsible for the development of allodynia. Since this mechanism was proposed, several studies have confirmed the role of neuronal sensitization in the brainstem and thalamus (5–8) in the formation of CA.
The presence of CA is a putative risk factor for migraine transformation, the process by which episodic migraine (EM) becomes chronic migraine (CM) (9). Reciprocally, CA influences the regression from CM to EM (6). CA in migraineurs is also associated with multiple comorbid pain conditions, such as irritable bowel syndrome, fibromyalgia, and chronic fatigue syndrome (4). Allodynic migraineurs tend to have more severe headache-related disabilities (10,11) and poor sleep quality (3). Some studies also suggested that treatment with triptans fails when CA has developed during a migraine attack (7,8).
Many risk factors of CA have been reported, including female sex, being African American, having low educational level, high headache frequency, high headache intensity, and a high level of disability. Meanwhile, depression and obesity are two important independent risk factors (1). Psychiatric disorders, such as depression and anxiety, are often comorbid with migraine. The odds ratio (OR) of developing migraine is significantly higher in patients with depression than in those without depression. Reciprocally, migraineurs also have a higher OR of developing depression (12). A prior study demonstrated that migraineurs have a higher OR of having depression, generalized anxiety disorder and panic attacks (13). The relationship between anxiety and migraine was even stronger than that between depression and migraine.
Central sensitization, which might be responsible for the formation of CA, can be modulated by supraspinal processes involving cognition, attention and emotion via descending pathways (14,15). Some studies have demonstrated that pain perception can be modulated by cognition and emotion, such as depression (14–17). Therefore, the presence of allodynia might be associated with depression and anxiety status in migraineurs. Nevertheless, few studies have examined the relationship between mood and allodynia in migraineurs, and this association remains unclear.
The aim of the present study was to explore the relationships between anxiety and depression and allodynia in migraine patients. We hypothesized that migraine patients with allodynia have a higher risk of having depression and anxiety.
Methods
Patients visiting the headache clinic at Taipei Veterans General Hospital (Taipei-VGH) were invited to participate in the study. Patients were diagnosed according to the criteria of the International Classification of Headache Disorders, second edition (ICHD-2), 2004 (18). Only patients with migraine with aura (code 1.2) or without aura (1.1) were included. In addition, they were classified into EM and CM groups (≥15 headache days/month for ≥ 3 months, with ≥ 8 days of migraine attacks per month) (19). We excluded patients with probable migraine and patients who had any difficulty in communication. The study protocol was approved by the Institutional Review Board at Taipei-VGH. Patients signed informed consent before entering the study.
Study assessment
We recorded demographic data and headache profiles, such as headache intensity, frequency, locations, characteristics, analgesics use and accompanying symptoms, on a headache intake form. The headache intensity was recorded on a 0–10 verbal numeric scale (VNS). Headache frequency was recorded by the average number of days the subject experienced headache every week. Body mass index (BMI) was calculated as body weight divided by body height squared (kg/m2).
CA symptoms checklist
The checklist was designed to identify the symptoms of CA, which comprised the following 17 daily activities: combing the hair, pulling the hair back, shaving the face, wearing glasses, wearing earrings, wearing contact lens, wearing a necklace, wearing anything on the head or neck, wearing anything on the wrist or arm, wearing a ring, wearing a watch, wearing tight clothing, covering the body with a thick duvet, washing the face, resting the face on a pillow, cooking and exposure to cold. The patients were asked to report whether they feel discomfort during these activities or if they avoid these activities during a migraine attack. The patients answered “yes,” “no,” or “I don’t know or it does not apply to me” to these questions. If the answer was “no” or “I don’t know or it does not apply to me,” the symptom would be scored 0. If the answer was “yes,” the symptom would be scored 1. The total score ranged from 0 to 17. According to the allodynia symptoms score, the severity of allodynia was classified as no allodynia (0–2), mild allodynia (3–5) and moderate to severe allodynia (≥6) (11).
Hospital and Anxiety Depression Scale (HADS)
HADS is a self-administered instrument that was developed to detect psychiatric comorbidity in the setting of a hospital medical outpatient clinic (20,21). By avoiding the somatic domain of anxiety and depression, HADS excludes confounding factors of physical signs and symptoms and focuses on specific affective symptoms. It has high sensitivity and specificity for detecting psychiatric disorders in patients with medical illnesses. The scale contains 14 questions, seven for anxiety (HADS-A) and seven for depression (HADS-D). The score of each scale ranges from 0 to 42. The higher the score is, the more severe the symptom. In this study, we used a cut-off point of 7 for the anxiety subscore and 4 for the depression subscore for clinically significant cases (22).
Data analysis
IBM SPSS Statistics, version 18.0, was used for the statistical analysis. Descriptive statistics were presented as means ± standard deviation or percentages. For categorical data, the chi-square test or Fisher’s exact tests were used to test the difference between groups. The Student’s t test and one-way analysis of variance (ANOVA) with the post-hoc least significant difference (LSD) test were used to compare the means of continuous variables. The logistic regression model was used to investigate the relationship between clinically significant depression and anxiety and the severity of allodynia after controlling for confounding factors. Its results were shown as an OR with a 95% confidence interval (CI). All calculated p values were two tailed, and statistical significance was defined as a p value of less than 0.05.
Results
Characteristics of the study population
Comparisons of demographics, headache features, and HADS scores of migraine patients with and without allodynia.

HADS: Hospital Anxiety and Depression Scale; BMI: body mass index; VNS: verbal numeric scale.
Allodynia symptoms
By defining allodynia as having three or more allodynic symptoms, 48.4% of participants were allodynic migraineurs. The average number of allodynic symptoms among all migraineurs was 4.3 ± 3.1. The most common three allodynic symptoms were avoiding wearing tight clothes, wearing glasses and cooking, and the three least common symptoms were avoiding shaving the face, wearing a ring and wearing earrings (Table 2). Among allodynic migraineurs (n = 210), 53.8% (n = 113) had mild allodynia and 46.2% (n = 97) had moderate to severe allodynia during migraine attacks.
The frequency of each allodynic symptom among migraineurs.

Anxiety and depression subscores and allodynia
Comparisons of demographics, headache features, and HADS scores of migraine patients with allodynia of different severities.

Analysis of variance (ANOVA) followed by least significant difference (LSD) test as a post hoc procedure was applied for the comparison of means, and the chi-square test was applied to compare proportions. ap < 0.05 vs. no allodynia, bp < 0.05 vs. mild allodynia, cp < 0.05 vs. moderate to severe allodynia. HADS: Hospital Anxiety and Depression Scale; BMI: body mass index; VNS: verbal numeric scale.
A logistic regression model with clinically significant anxiety and depression as the dependent variables and allodynia severity (no, mild, moderate to severe), age, sex, education and BMI as the independent variables was performed. The presence of allodynia was an independent risk factor of clinically significant anxiety, with an OR of 1.82 (95% CI = 1.11–2.99, p = 0.017) for mild allodynia and 2.91 (95% CI = 1.66–5.12, p < 0.001) for moderate to severe allodynia after controlling the confounding factors. Only the presence of moderate to severe allodynia was an independent risk factor for clinically significant depression with an OR of 2.14 (95% CI 1.19–3.86, p = 0.015) after controlling for the confounding factors.
Discussion
Our study showed that allodynic migraineurs had a higher frequency of anxiety. As the severity of allodynia increases, the severity of anxiety increases. In addition, moderate to severe allodynia is associated with clinically significant depression in migraine patients.
Comparison of studies regarding allodynia and psychiatric disorders in migraine patients.
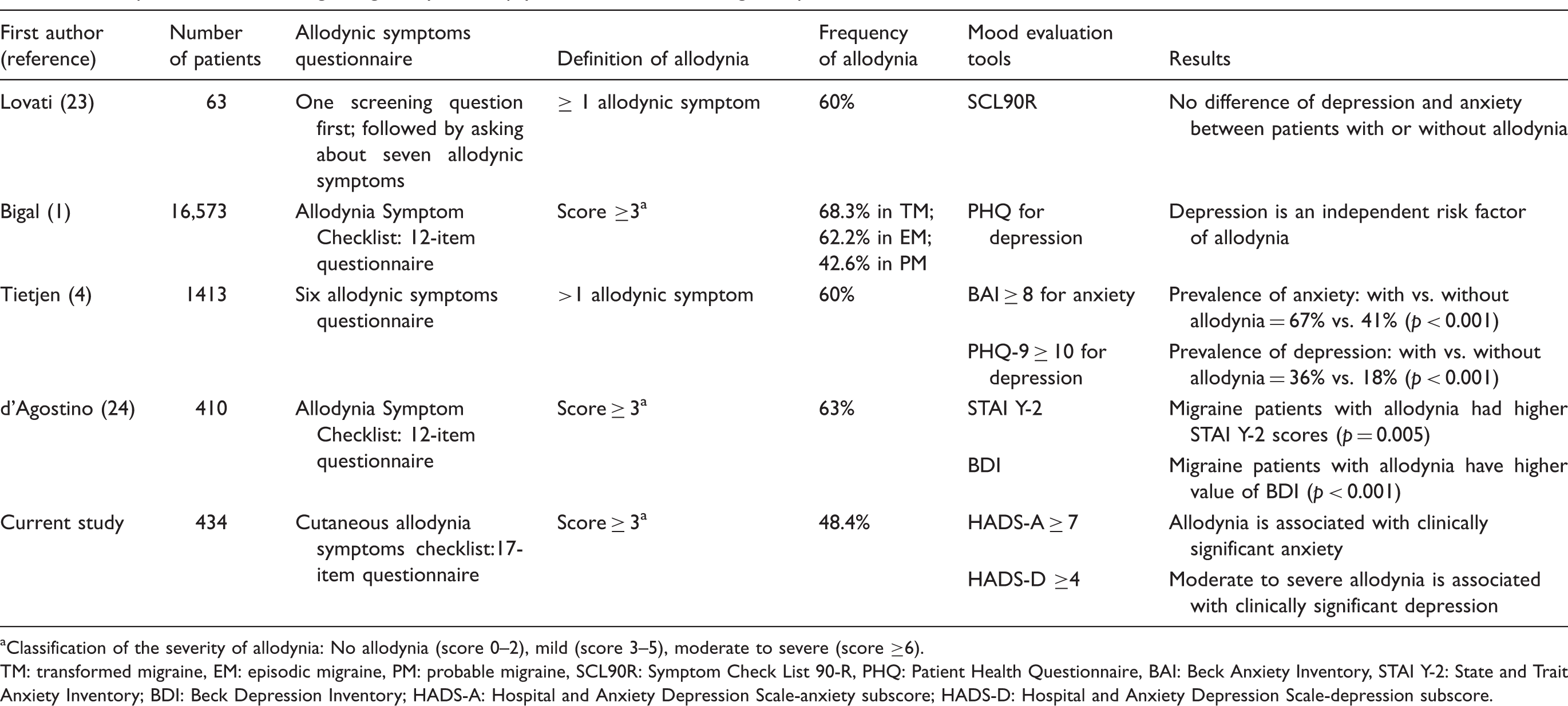
Classification of the severity of allodynia: No allodynia (score 0–2), mild (score 3–5), moderate to severe (score ≥6). TM: transformed migraine, EM: episodic migraine, PM: probable migraine, SCL90R: Symptom Check List 90-R, PHQ: Patient Health Questionnaire, BAI: Beck Anxiety Inventory, STAI Y-2: State and Trait Anxiety Inventory; BDI: Beck Depression Inventory; HADS-A: Hospital and Anxiety Depression Scale-anxiety subscore; HADS-D: Hospital and Anxiety Depression Scale-depression subscore.
This study provides evidence that allodynia is a risk of having anxiety and depression in migraine patients. Although the underlying mechanism has not been well established, neuroendocrine systems or neurotransmitters might modulate central sensitization, pain perception, as well as psychiatric disorders. For example, the hypothalamo-pituitary-adrenal (HPA) axis might involve pain processing, which is modulated by depression. Blockade of the HPA axis by administration of hydrocortisone or implantation of dexamethasone above the paraventricular nucleus of the thalamus could reduce stress-induced analgesia (26). Pharmacological management of fibromyalgia, another disorder involving central sensitization of the nociceptive system, can improve anxiety and depression (27). Therefore, it is reasonable to propose an underlying common mechanism modulating both central sensitization of the nociceptive system and psychiatric disorders.
Some neurotransmitters might be involved in both psychiatric disorders and the nociceptive system. Repeated administration of reserpine resulted in a sustained decreased pressure threshold for producing tactile allodynia in rats (28). These animals also showed depression-like behavior. Reduction of biogenic amines, such as dopamine, norepinephrine and serotonin, in the spinal cord, thalamus and prefrontal cortex were observed in these animals. In addition, the melatoninergic system might also play a role in the interaction between pain and depression (29). After peripheral nerve injury in Wistar-Kyoto rats, a preclinical animal model of depression, the mechanical allodynia and depression-like behavior worsened. This worsening can be prevented by administrating melatonin into the anterior cingulate cortex. Further studies are needed to verify the role of these pathways and neurotransmitters in both central sensitization and psychiatric disorders.
Compared with previous reports, the frequency of allodynia in migraineurs was lower in our study (48.4%). In another study in Taiwan (30), only 22.0% of migraine patients experienced brushing allodynia during a gauze-brushing test during migraine attacks. Ethnic differences might contribute to the lower frequency of allodynia in the migraine patients in our study.
Our results showed a lower BMI and a higher education level in migraine patients, whereas previous studies showed a higher BMI (1,4) and a lower education level (1). Because this study required patients to recall their allodynic symptoms during the interictal period, patients with a higher education level tend to have a better ability to complete the questionnaire and a better ability to recall their allodynic symptoms during an attack. Although a role of obesity in migraine pathophysiology and central sensitization has been proposed (31), the effect of obesity on migraine differs in different populations. In a Chinese population, although the prevalence of migraine was higher in those with morbidly obesity (BMI > 30), there was no association between obesity and migraine severity, frequency or disability (32). The variable impact of obesity in different populations might explain our results that allodynic migraineurs had a lower BMI.
Because of high prevalence of allodynia in migraineurs, evaluation of the presence and severity of allodynia is crucial. This evaluation can be performed using a simple allodynic symptoms checklist. Development of allodynia is associated with treatment failure with triptans and the risk of having clinically significant anxiety and depression. Once allodynia is confirmed, anxiety and depression evaluations and a tailored treatment plan are important.
The limitation of our study is recall bias because the allodynic symptoms checklist is a self-reported questionnaire that was filled in between migraine attacks. Also, this was a hospital-based study, which may not represent the whole migraine population. In addition, this is a cross-sectional study and the causal relationship between allodynia and depression/anxiety cannot be certain.
Another limitation of this study is the subjectivity of the participants while filling in the allodynic questionnaire. Patients with depression and panic disorder were associated with an increased frequency of pain complaints, such as low back pain (33). The prior study showed depression and anxiety did not correlate with ratings of physical pain, which was measured by a subjectively answered 100 mm visual analogue scale in patients with fibromyalgia (34). Thus far there is no evidence of whether anxious/depression migraine patients are more likely to have positive answers to allodynic or other pain-associated questions. Further studies exploring this issue are needed.
In conclusion, this study revealed an association between allodynia and psychiatric comorbidities in migraineurs. The presence of allodynia is associated with higher risk of having anxiety and depression, and the severity of allodynia correlates with the severity of anxiety as well as the severity of depression.
Clinical implications
The frequency of allodynia in migraine patients was 48.4%. Allodynia is associated with clinically significant anxiety in migraine patients. Moderate to severe allodynia in migraine patients is associated with clinically significant depression. Allodynia should be screened in all migraine patients and the treatment plan should be tailored individually.
Footnotes
Funding
This work was supported by grants from Taipei Veterans General Hospital (V101C-105, VGHUST101-G7-1-2), the Taiwan National Science Council (101-2314-B-075-037-MY2), NSC support for the Centre for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan (NSC 101-2911-I-008-001) and the Ministry of Education (Aim for the Top University Plan), Taipei, Taiwan.
Conflict of interest
Dr Jong-Ling Fuh is a member of a scientific advisory board of Elli Lilly and Norvatis, and has as well received research support from the Taiwan National Science Council, Taipei-Veterans General Hospital and Elli Lilly. Dr Shuu-Jiun Wang has served on the advisory boards of Pfizer, Allergan, and Elli Lilly Taiwan. He has received speaking honoraria from local companies (Taiwan branches) of Pfizer, Elli Lilly, Boehringer Ingelheim and GSK. He has received research grants from the Taiwan National Science Council, Taipei-Veterans General Hospital and Taiwan Headache Society.