
Abstract
Objective
Human provocation models are widely used to investigate migraine mechanisms and validate therapeutic targets. Despite well-known sex differences in migraine, concerns persist regarding sex representation and reporting in experimental research. This systematic review evaluated sex distribution, sex-specific analyses, and the consideration of female-specific biological factors in randomized, placebo-controlled migraine provocation studies.
Methods
PubMed and Embase were systematically searched for randomized, placebo-controlled provocation studies in adults with migraine, following PRISMA 2020 guidelines. Data were extracted on participant sex distribution, sex-stratified outcome reporting, and consideration of female-specific variables, including menstrual cycle, hormonal contraception, and pregnancy status.
Results
Fifty-eight studies published between 1972 and 2025 were included. Women represented 82% of participants, while men accounted for 18%. No study performed sex-stratified analyses of provoked headache or migraine outcomes. Sex was rarely discussed as a biological variable or limitation. Female-specific factors were largely overlooked, with menstrual cycle phase unreported in over 90% of studies and inconsistent reporting of hormonal contraception and pregnancy status.
Conclusions
Migraine provocation studies show marked sex imbalance and a systematic lack of sex-disaggregated analyses. Although these models have demonstrated substantial translational relevance, particularly in supporting the development of anti-CGRP therapies, the absence of sex-disaggregated analyses and limited consideration of biological sex constrain the assessment of translational applicability across sexes.
This is a visual representation of the abstract.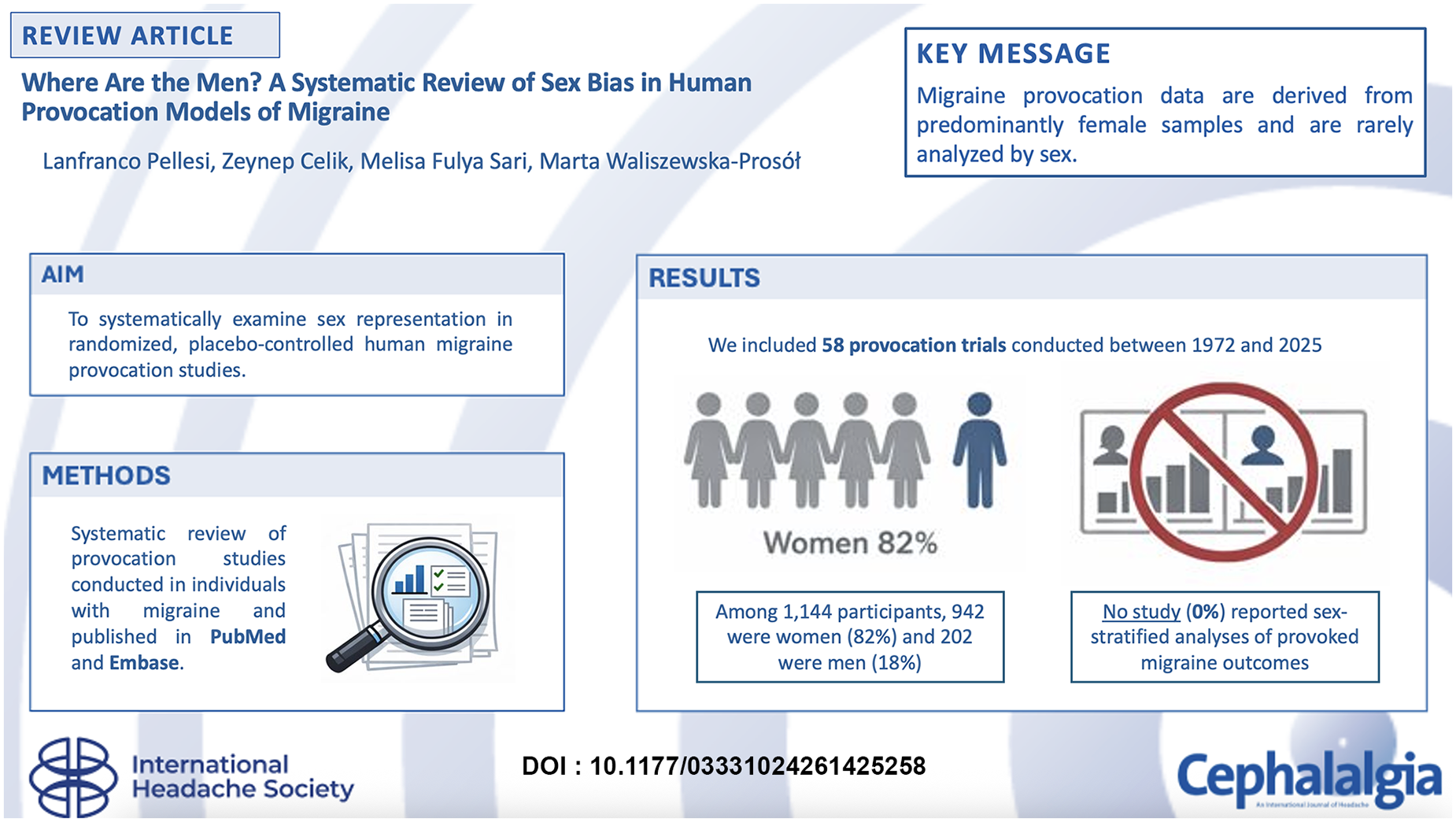
Introduction
Human provocation models of migraine involve the controlled administration of pharmacological or experimental stimuli to induce migraine or migraine-like attacks in individuals with migraine. 1 These models have been used to investigate mechanisms underlying migraine initiation and to evaluate biological pathways implicated in the disorder. Over the past decades, several provoking agents, including calcitonin gene-related peptide (CGRP), pituitary adenylate cyclase-activating polypeptide-38 (PACAP-38), nitric oxide donors and potassium channel openers have been tested in placebo-controlled trials, contributing to current understanding of migraine pathophysiology.2,3 Moreover, migraine is characterized by marked sex differences. 4 The condition is more prevalent in women than in men, particularly during the reproductive years, and clinical features such as attack frequency, duration and disability differ between sexes. Hormonal factors, including fluctuations across the menstrual cycle as well as changes during pregnancy and menopause, are known to influence migraine occurrence and severity. 5 These observations suggest that biological sex may affect susceptibility to migraine and response to migraine triggers. Despite these differences, concerns have been raised regarding sex representation in experimental migraine research. 6 Previous studies have reported that men are underrepresented in clinical migraine studies, and that outcomes are rarely analyzed or reported separately by sex. 6 In the context of human provocation models, this imbalance may limit the interpretability and generalizability of findings, particularly when results are used to support mechanistic hypotheses or inform translational research. In addition to overall sex distribution, the extent to which female-specific biological factors are considered in provocation studies remains unclear. Variables such as hormonal contraception, menstrual cycle phase and pregnancy status may influence migraine susceptibility and response to provoking agents. The aim of this systematic review is to examine sex representation in randomized, placebo-controlled human migraine provocation studies. Specifically, we assess the proportion of male and female participants, the frequency of sex-stratified analyses and the reporting of female-specific biological factors. By summarizing current reporting practices, this review aims to identify methodological gaps relevant to the interpretation and design of future human migraine provocation studies.
Methods
A systematic literature search was performed in PubMed and Embase (Ovid) to identify human migraine provocation studies using pharmacological or experimental triggers. This systematic review was not registered in the PROSPERO database, as it did not aim to assess intervention effects or clinical efficacy. The search was conducted on 6 October 2025. Both Medical Subject Headings (MeSH) and free-text terms were used to maximize sensitivity. The search strategy combined terms related to migraine and migraine-like headache, provocation or challenge paradigms and randomized or placebo-controlled clinical trial designs. Filters were applied to exclude animal studies. Additional exclusion criteria were applied at the search level to remove papers related to medication-overuse headache, reviews, systematic reviews, meta-analyses, editorials, study protocols, letters and non-English publications. The full search strategy is available in the Supplementary Material. This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 7
Eligibility criteria
Studies were considered eligible if they met the following criteria: randomized, placebo-controlled provocation trials enrolling adults aged 18 years or older with a diagnosis of migraine with aura or without aura according to the International Classification of Headache Disorders; administration of a pharmacological or experimental trigger with the explicit aim of inducing migraine or migraine-like attacks; and assessment of headache or migraine outcomes following provocation. Randomized, placebo-controlled designs were required to ensure comparability across studies and to minimize confounding when evaluating sex representation and reporting practices. Studies were excluded if they were observational, non-randomized, post-hoc analyses, lacked a placebo or control condition, enrolled only healthy volunteers, focused on non-migraine headache disorders, involved pediatric populations or were conducted in non-human models.
Study selection
All records identified through the database search were exported to EndNote (Clarivate Analytics), and duplicate records were removed prior to screening. Titles and abstracts were screened for relevance, followed by full-text assessment of potentially eligible articles. The study selection process was performed systematically, and reasons for exclusion at the full-text stage were documented. The overall study selection process is summarized in a PRISMA 2020 flow diagram (Figure 1).

Flowchart of the systematic search.
Data extraction
Data extraction was conducted manually using predefined extraction templates. For each included study, information was collected on publication year, country of study conduct, study design, provoking agent and comparator, migraine subtype, sample size, age range of participants and funding source. To specifically address sex representation and reporting practices, additional data were extracted on the number and proportion of female and male participants, whether provoked migraine or headache outcomes were analyzed separately by sex, and whether sex was acknowledged or discussed as a biological variable or methodological limitation. Furthermore, female-specific variables were recorded when available, including the use of hormonal contraception, reporting of menstrual cycle phase at the time of participation and information on pregnancy status or pregnancy-related exclusion criteria. When such information was not explicitly reported, it was recorded as not mentioned.
Data synthesis
Data were synthesized using a descriptive approach consistent with the objectives of this systematic review. No quantitative meta-analysis was planned or performed, as the primary aim of the review was not to estimate pooled effect sizes or compare clinical outcomes, but to characterize sex representation and reporting practices in human migraine provocation studies. The primary outcome was the number and proportion of male and female participants enrolled across included studies. Secondary outcomes included whether sex was addressed in the analysis or discussion of study results, either as a biological variable, a methodological limitation or a factor potentially influencing data interpretation. Additional analyses examined whether sex-stratified outcomes were reported and whether female-specific biological variables were considered. Results are presented as absolute numbers and proportions to allow comparison across studies and to summarize patterns of participant representation and reporting practices.
Results
A total of 764 hits were identified. During the screening of titles and abstracts, we excluded duplicates (n = 38), clinical studies and case reports not involving a migraine provocation (n = 510), preclinical and animal studies (n = 8) reviews, systematic reviews, comments, corrections, letters, protocols and perspectives (n = 67). The remaining 141 hits were retrieved in full text and subjected to a secondary screening. At the full text screening, we further excluded studies that did not evaluate migraine-like attacks (n = 19), studies that did not enroll participants with migraine (n = 20), non-placebo-controlled studies (n = 41) and post-hoc analysis (n = 3). The remaining studies met all the inclusion criteria and were included in the final analysis (n = 58). The extraction process is illustrated in the PRISMA flow diagram (Figure 1).
Characteristics of included studies
All included studies were randomized, placebo-controlled trials employing experimental migraine provocation paradigms.8–65 The studies were published between 1972 and 2025. The majority were conducted in Denmark (n = 46, 79%), followed by the United Kingdom (n = 5, 9%), Italy (n = 3, 5%), Norway (n = 1, 2%), and the Netherlands (n = 1, 2%). A broad spectrum of pharmacological provoking agents was investigated, most frequently nitroglycerin (n = 11, 19%), followed by cilostazol (n = 5, 9%), PACAP-38 (n = 5, 9%), levcromakalim (n = 5, 9%), CGRP (n = 4, 7%), sildenafil (n = 4, 7%), VIP (n = 3, 5%), prostaglandins (n = 2, 3%), and several other less commonly used substances. The study populations consisted predominantly of adults, with ages spanning from approximately 18 to 65 years. Most studies included only patients with migraine without aura (n = 38, 66%), whereas others enrolled patients with both migraine with and without aura (n = 15, 26%) or exclusively migraine with aura (n = 5, 9%). Funding was primarily provided by academic institutions (n = 47, 81%), with industry involvement reported in a small number of studies (n = 3, 5%); in 8 studies (14%), funding was shared between academic institutions and private companies. A comprehensive overview of the included studies is provided in Table 1.
Characteristics of the included studies.

CGRP: calcitonin gene-related peptide; mCPP: m-chlorophenylpiperazine; PACAP-27: Pituitary adenylate cyclase activating peptide-27; PACAP-38: Pituitary adenylate cyclase activating peptide-38; VIP: vasoactive intestinal polypeptide.
Sex-related characteristics
Overall, 1278 participants were enrolled across the studies included, with sample sizes ranging from 8 to 80 participants per trial. Three studies did not report the number of participants stratified by sex; therefore, these studies were excluded from analyses of sex distribution. Among the remaining 1144 participants, 942 were women (82%) and 202 were men (18%), all diagnosed with migraine with or without aura. With respect to hormonal contraception, 37 studies (64%) allowed its use but did not account for it in the analysis or reporting of results, whereas 18 studies (31%) did not provide any information regarding hormonal contraceptive use. Two studies (3%) explicitly prohibited the use of hormonal contraception, and one study (2%) reported that none of the enrolled participants were using hormonal contraceptives. Consideration of the menstrual cycle was largely absent: 53 studies (91%) neither reported participants’ menstrual cycle status nor accounted for it in the results. One study (2%) scheduled experimental sessions at least three days before or after menstruation, one (2%) included women only if they had not menstruated within two days before or after the study and one (2%) excluded women who were menstruating at the time of the experiment. In addition, one study (2%) examined women within the first 10 days of their menstrual cycle, and another study (2%) matched female participants according to menstrual cycle phase to minimize pain modulation across the menstrual cycle. Regarding pregnancy status, 44 studies (76%) explicitly excluded pregnant individuals, while the remaining 14 studies (24%) did not report any information concerning pregnancy. This lack of reporting likely reflects an implicit exclusion of pregnant participants, which may not have been considered necessary to state explicitly. These characteristics of the included studies are summarized in the Supplementary Material (Table S2).
Sex-specific analyses and reporting
None of the included studies (0%) reported a sex-stratified analysis of provoked headache outcomes, despite sex being systematically reported as a baseline characteristic. Similarly, no study (0%) evaluated provoked migraine outcomes according to the sex of the participants. Only three studies (5%) acknowledged sex as a relevant variable in the Discussion and/or Limitations sections, noting that the results might differ with a different sex distribution of the study population. An overview of these aspects across the included studies is provided in the Supplementary Material (Table S3).
Discussion
This systematic review describes a marked sex imbalance and the absence of sex-disaggregated analyses across five decades of human migraine provocation studies (Figure 2). Across the included trials, women constituted most participants (82%), while men were underrepresented. No study reported sex-stratified analyses of provoked headache or migraine outcomes. As a result, the current body of evidence primarily reflects female biology, and the extent to which these findings apply to men remains uncertain. Although the predominance of women partly reflects the epidemiology of migraine, this does not justify the absence of sex-disaggregated analyses. This observation should not be interpreted as a criticism of the inclusion of women in migraine research. On the contrary, the predominance of women has generated clinically meaningful and highly relevant data for female patients with migraine. However, the combination of unequal recruitment and the systematic omission of sex-specific analyses represent a methodological limitation that was rarely acknowledged by the original studies. In most cases, sex was treated as a descriptive demographic characteristic rather than as a biological variable with potential implications for migraine susceptibility and response to experimental triggers. Biological differences between women and men are well established in migraine.66,67 In women, fluctuations in sex hormones are strongly associated with attack initiation and modulation, as demonstrated by the increased risk of migraine during the perimenstrual period and by changes observed during pregnancy, the postpartum phase, and menopause. 68 Women also tend to experience longer attack duration, greater disability and higher recurrence rates compared with men. 69 A recent study showed that men were significantly less likely to report visual and sensory symptoms accompanying headache than women, and the time required to return to normal functioning was longer in men than in women. 70
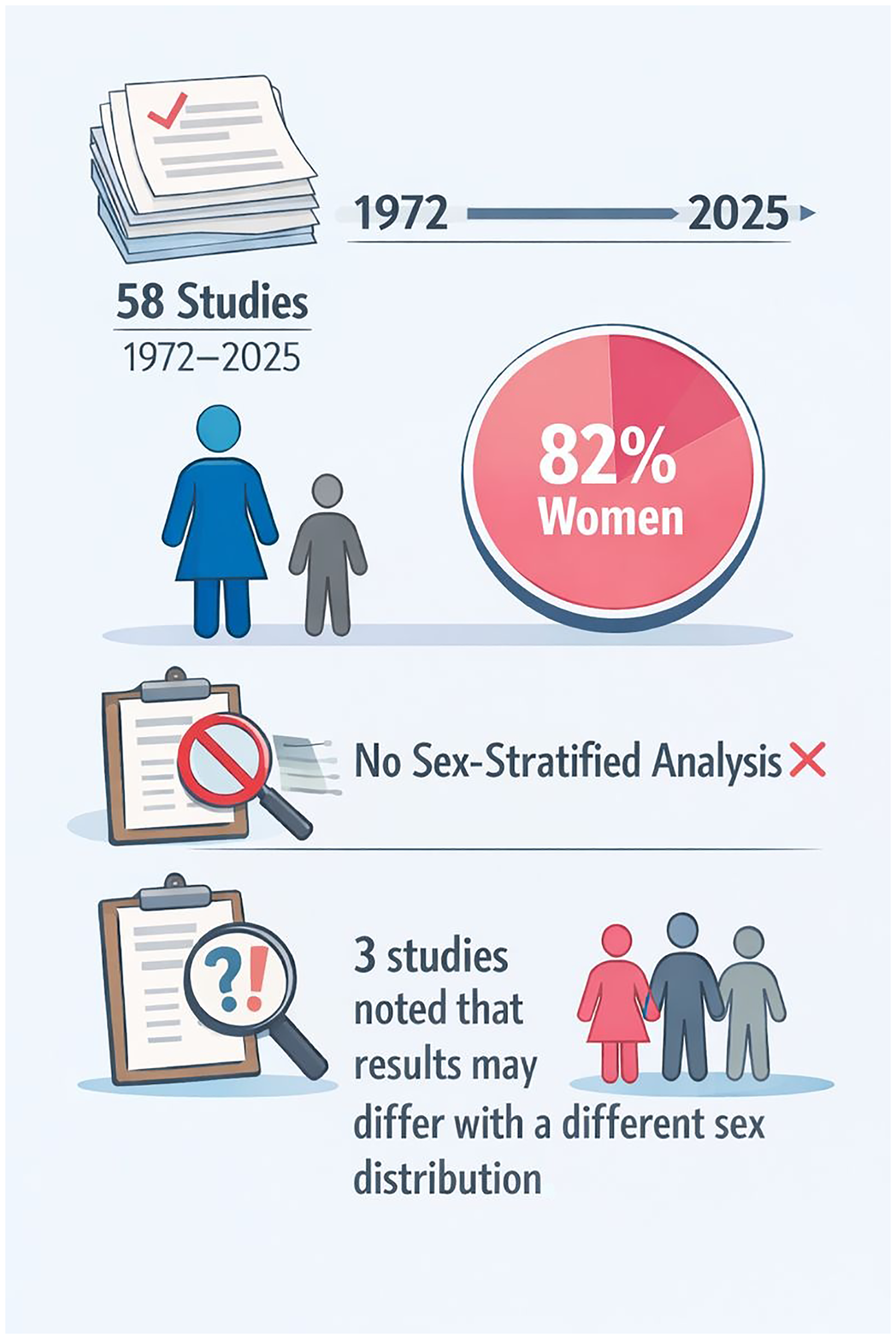
Sex imbalance and reporting practices in human provocation studies of migraine.
In this context, the lack of sex-specific analyses in provocation studies limits the interpretability of the results and hinders assessment of whether experimentally induced migraine mechanisms are comparable between sexes. Translational relevance refers to the ability to generalize mechanistic findings from experimental models to the broader migraine population, including both women and men. Epidemiological representativeness alone does not ensure translational validity if biological sex is not analytically considered. Other gaps identified in this review concerns the handling of female-specific biological factors. Menstrual cycle phase was almost universally ignored: more than 90% of studies neither reported cycle status nor accounted for it in the study design or analysis. Similarly, the use of hormonal contraception was often permitted but rarely characterized in detail, with little or no information on formulation, dose, or recent changes. Given that different hormonal contraceptives can have divergent effects on migraine, 71 this lack of reporting introduces potential uncontrolled variability in susceptibility to provocation. The limited consideration of hormonal factors is particularly relevant in the context of provocation models, which aim to isolate and investigate specific pathophysiological mechanisms. Failure to account for variables known to influence migraine risk may obscure true biological effects and reduce comparability across studies. Although most trials excluded pregnant individuals, the overall approach to female-specific biological variables remained inconsistent and insufficiently standardized. It is noteworthy that human provocation studies have contributed to the validation of therapeutic targets, including the CGRP pathway, using populations largely composed of women.18,38,63 Clinical trial data with CGRP receptor antagonists do not indicate reduced efficacy in men compared with women, but these findings are largely derived from pooled analyses with limited statistical power for male subgroups. 72 Preclinical evidence from a murine model of post-traumatic headache demonstrates a clear sexual dimorphism, with sustained CGRP receptor blockade producing significantly greater analgesic and preventive effects in females than in males. 73 Overt sex-related differences in therapeutic response may not be detectable in current clinical datasets, and the lack of adequately powered, sex-stratified analyses precludes a definitive evaluation of potential sex-dependent differences in CGRP-targeting treatment efficacy. Future studies should aim, where feasible, for more balanced recruitment and should include sex-disaggregated analyses of provoked outcomes. In addition, standardized reporting of female-specific factors, such as menstrual cycle phase and hormonal contraceptive use, would strengthen the methodological rigor, interpretability, and translational relevance of experimental migraine models.
Conclusions
This systematic review demonstrates a substantial and persistent sex imbalance in randomized, placebo-controlled human migraine provocation studies, with a strong predominance of female participants and a consistent absence of sex-stratified analyses. Although the higher prevalence of migraine in women may partially explain recruitment patterns, the lack of analytical consideration of sex as a biological variable represents a major methodological limitation. Equally important is the insufficient reporting and control of female-specific biological factors. Variables known to influence migraine susceptibility, such as menstrual cycle phase and hormonal contraceptive use, were rarely accounted for, introducing potential uncontrolled variability and limiting comparability across studies. To enhance the scientific value and clinical relevance of future provocation studies, greater emphasis should be placed on balanced recruitment where feasible, routine sex-disaggregated analyses and standardized reporting of hormonal and reproductive variables. Addressing these gaps will improve interpretability, support more robust mechanistic conclusions and strengthen the translational pathway from experimental migraine models to therapeutic development.
Clinical implications
Migraine provocation data are derived from predominantly female samples and are rarely analyzed by sex, limiting the ability to assess the underlying mechanisms for male patients with migraine.
Poor reporting of menstrual cycle and hormonal contraception may confound trigger responses, reducing the clinical interpretability of provocation studies in women.
The lack of sex-specific analyses may hinder identification of clinically relevant sex differences in migraine mechanisms and treatment response.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261425258 - Supplemental material for Where are the men? A systematic review of sex bias in human provocation models of migraine
Supplemental material, sj-docx-1-cep-10.1177_03331024261425258 for Where are the men? A systematic review of sex bias in human provocation models of migraine by Lanfranco Pellesi, Zeynep Celik, Melisa Fulya Sari and Marta Waliszewska-Prosół in Cephalalgia
Footnotes
Acknowledgements
None
Author contributions
Conceptualization: Lanfranco Pellesi, Marta Waliszewska-Prosół
Data curation: Lanfranco Pellesi, Zeynep Celik, Melisa Fulya Sari
Formal analysis: Lanfranco Pellesi, Zeynep Celik, Melisa Fulya Sari
Writing – original draft: Zeynep Celik, Melisa Fulya Sari
Writing – review & editing: All authors
Consent to participate
Not applicable.
Consent for publishing
All authors have reviewed the final version of the manuscript and agree to publish it in Cephalalgia if accepted.
Data availability statement
Data sharing is not applicable to this article as no new datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethical considerations do not apply to this submission, as it is a review article and does not involve new data collection from human participants or animals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open practices
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.