
Abstract
Introduction
Analyzing the epidemiology of headache disorders is fundamental for understanding their behaviour and designing effective public health strategies. Epidemiologic studies conducted in individual countries often lack consistent methodologies, limiting broader interpretation. The Americas’ Migraine Observatory Study (AMIGOS) is a Pan-American epidemiological study designed to evaluate the burden and access to treatment of migraine and other headache disorders across the Americas. Here, we present data on migraine prevalence and disability.
Objectives
To describe and compare the prevalence and burden of migraine in the Americas at a specific time point using a unified sampling methodology. Additionally, to identify regional variations and potential factors contributing to differences in prevalence, providing a foundation for targeted public health strategies.
Materials and Methods
Data were collected online or via telephone from a sample representative of the demographic and social characteristics of each country, with a confidence level of 98% and a margin of error of 5%. We conducted both qualitative and quantitative research on key aspects of headaches among 16,202 individuals in 19 countries from Canada to Chile. Migraine diagnosis was made based on the ICHD-3 criteria.
Results
The overall prevalence of migraine was 9.7% (13.2% among females, 6.5% among males). The highest prevalence was observed in Brazil (13.8%), Canada (13.2%), and the United States (12.7%), while the lowest prevalence was found in Bolivia (5.5%), Paraguay (7.1%), and Argentina (7.3%). Participants typically experienced 4 headache days per month, and chronic migraine prevalence was estimated at 1.3%. The migraine burden, as measured by Years Lived with Disability (YLDs), was highest in the United States.
Conclusion
This is the first comprehensive Pan-American migraine epidemiological study. Findings indicate that migraine is highly prevalent in the Americas, with significant variations among different countries. Genetic, socioeconomic, and environmental factors may explain these observed differences.
Introduction
Migraine is a multifactorial neurological disorder that significantly affects and impairs human populations. No country or region is exempt, but prevalence estimates vary between countries, across regions within the same country, and over different time periods. 1 Spanning from north to south, the Americas are home to approximately 1 billion people—roughly 13% of the world's population—across 35 diverse countries, with a huge research gap on headache disorders in sub-regions. 2 Although migraine prevalence data is available for some countries, it is missing for others and could possibly benefit from a revision in a few more.3,4
In both public health and clinical practice, accurate diagnosis is essential for effective treatment. However, diagnosing populations poses significant challenges, not only due to their size but also because of their diversity. In the Americas, previous studies have revealed substantial variation in migraine prevalence estimates between countries and within territories.5,6 Previous studies have indicated that differences in ethnic backgrounds and socioeconomic status significantly affect both the risk of developing this condition and access to appropriate care and are probably the major determinants of variations observed.7,8
In addition to the geographical, ethnic, and cultural diversity of populations, research has highlighted the critical role of the sampling instrument in estimating prevalence. 9 For instance, a comprehensive study conducted in South America observed significant heterogeneity when different questionnaires were used across countries. 5 Moreover, some estimates could not be accurately replicated in subsequent evaluations. 6 Adding to the complexity, fluctuations in prevalence over time have occasionally been reported, further jeopardizing comparisons between studies conducted in different periods.9,10
To overcome these limitations, reduce methodological bias, and facilitate meaningful cross-country comparisons, it is essential to use a single, standardized sampling instrument implemented consistently across all regions at a specific time point. 11 This approach offers the most reliable means of accurately evaluating a region as diverse and expansive as the Americas.
The Americas’ Migraine Observatory Study (AMIGOS) is a Pan-American, cross-sectional epidemiological study designed to assess the epidemiology and unmet treatment needs of patients with headache disorders across North and South America. This report focuses on migraine prevalence findings.
Materials and methods
Study design and population
This cross-sectional, population-based study included data from nineteen countries across North and South America: Argentina, Bolivia, Brazil, Canada, Chile, Colombia, Costa Rica, Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, United States, and Uruguay.
Sampling was designed to reflect the demographic and social characteristics of each participating country, with a 98% confidence level and a 5% margin of error. A representative number of surveys was collected per country, adjusted for population size and density 12 (Figure 1, Supplementary table 1).

Population density based on the global human settlement layer (GHSL) (green), 12 our sampling density (red), and their overlap (orange).
Eligible participants were aged 18 years or older and deemed capable of completing the survey. Data were collected via a mixed-mode approach—online questionnaires and telephone—depending on regional feasibility and digital infrastructure. In countries with high internet penetration (e.g., Chile, Mexico, Argentina, Colombia), online self-administered surveys predominated; whereas in those with lower digital access (e.g., Bolivia, Peru, parts of Central America), telephone interviews were more frequent, often used to complement demographic quotas and improve coverage in rural or less connected areas. This combined approach was implemented to maximize inclusiveness and minimize digital exclusion, while maintaining methodological consistency across Latin America. The questionnaire required approximately 15 min to complete and covered demographic data, migraine-specific and other headache symptoms (based on ICHD-3 clinical criteria), medication use, and headache-related disability. It assessed headache occurrence, frequency, duration, characteristics, intensity, and associated symptoms (activity limitation, photophobia, phonophobia, and nausea/vomiting).
The initial screening question (“Have you experienced any kind of headache in the past 12 months?”) was intentionally broad to capture all headache types; migraine cases were subsequently identified using standardized clinical criteria. 13 All items were translated by bilingual headache-specialist clinicians and reviewed for conceptual equivalence, with minor adaptations to ensure cultural appropriateness (Supplementary Material).
Representativeness and response rates
Participants were selected through certified online research panels and local fieldwork providers in each country, ensuring diversity in demographic and socioeconomic profiles.
Data were weighted by sex, age group, and regional distribution to approximate national adult population structures. Estimated country-specific response rates ranged from 23% to 27%, anchored on Brazil (25%), where both online and telephone data collection were closely monitored. Rates were adjusted ± 2 percentage points according to three factors:
Digital infrastructure: higher internet penetration tended to yield slightly higher response rates Collection mode: mixed telephone/online methods increased cooperation and completeness Panel maturity: countries with established research panels achieved lower non-response.
This procedure ensured consistent response-rate estimation and methodological comparability across the 19 participating countries.
Migraine diagnosis
Migraine diagnoses were determined based on the International Classification of Headache Disorders, 3rd edition (ICHD-3). Participants were classified as having migraine if their headaches:
Lasted ≥4 h, Fulfilled at least two of the following: unilateral location, pulsating quality, moderate/severe pain intensity, and worsening with or leading to avoidance of routine physical activity, and Included either nausea/vomiting or both photophobia and phonophobia.
In addition, probable migraine was considered when only two of the above diagnostic criteria were fulfilled, provided that criteria for tension-type headache were not. 14
Calculation of migraine burden
The migraine burden was quantified in terms of Years Lived with Disability (YLDs) using the following formula:

Where:
- P: The prevalence of migraine in each country, - DW: The fixed disability weight for migraine, set at 0.434, as defined by the Global Burden of Disease Study
3
- T: The average time spent in the ictal period per year.
To estimate T, we calculated the product of monthly headache frequency (f) and average attack duration in hours (d) as reported by participants, then converted this into an annual value:

Where:
- f: The average number of headache days per month, - d: The average duration of each attack in hours, - (12 / (24 × 365)): A conversion factor to express hours as a fraction of a year.
This approach allowed for the direct calculation of the ictal period for the entire sample without further stratification or weighting. Participants reporting a non-zero monthly attack frequency, but a missing or null attack duration were assumed to have incomplete responses. For these cases, the duration was imputed using the country-specific median attack duration, calculated from all valid responses within the same country. This approach was also applied when respondents explicitly entered a duration of “0”, which was considered an implausible value. Imputation was conducted to preserve internal consistency and minimize downward bias in the estimation of migraine burden. To avoid overestimation, the ictal period was capped at 100% when T exceeded this threshold.
Statistical analysis
Data were analyzed using Microsoft® Excel® (version 2410).
Descriptive statistics were used to compare prevalence and burden across countries. Visualizations, including bar charts and maps, were created to illustrate sampling density and geographic patterns in migraine burden. Raw prevalence values refer to 12-month (1-year) estimates without age or sex adjustment. Age- and sex-adjusted prevalence values were calculated using 2023 population estimates (male and female, by single year of age) from the United Nations World Population Prospects 2024 (POP/01-1 and POP/01-2: Female and male population by single age, region, subregion, and country; Estimates 1950–2023; POP/DB/WPP/Rev.2024/POP/F01-1 and F01-2).
Ethics statement
All participants provided informed consent, and the study protocol was approved by the Brazilian National Research Ethics Committee (CONEP), under CAAE 82972424.4.0000.0076.
Results
A total of 16,202 participants from 19 countries completed the assessment. While precise overall participation rates could not be determined, country-specific estimates suggest response rates of approximately 25%, consistent with the 23–27% range anticipated during the study design. Response targets were adjusted based on each country's demographic characteristics, yielding between 604 and 1303 responses per country (median = 753) (Supplementary Table 1). The sample was sex-balanced, with 50.4% females, 49.4% males, and 0.2% identified as other genders. The mean participants’ age was 35.5 years (SD ± 12.2).
The pooled, age-standardized migraine prevalence across the Americas was 9.7% (Table 1). The highest adjusted prevalence was observed in Brazil (13.8%), Canada (13.2%), and the United States (12.7%), while the lowest prevalence was found in Bolivia (5.5%), Paraguay (7.1%), and Argentina (7.3%) (Figure 2, Figure 3 and Table 1). The overall (raw) prevalence of migraine was 9.8% (12.6% among females, 7.0% among males, Supplementary Table 2). When including probable migraine, the combined prevalence reached 27.8% (Supplementary Table 3).
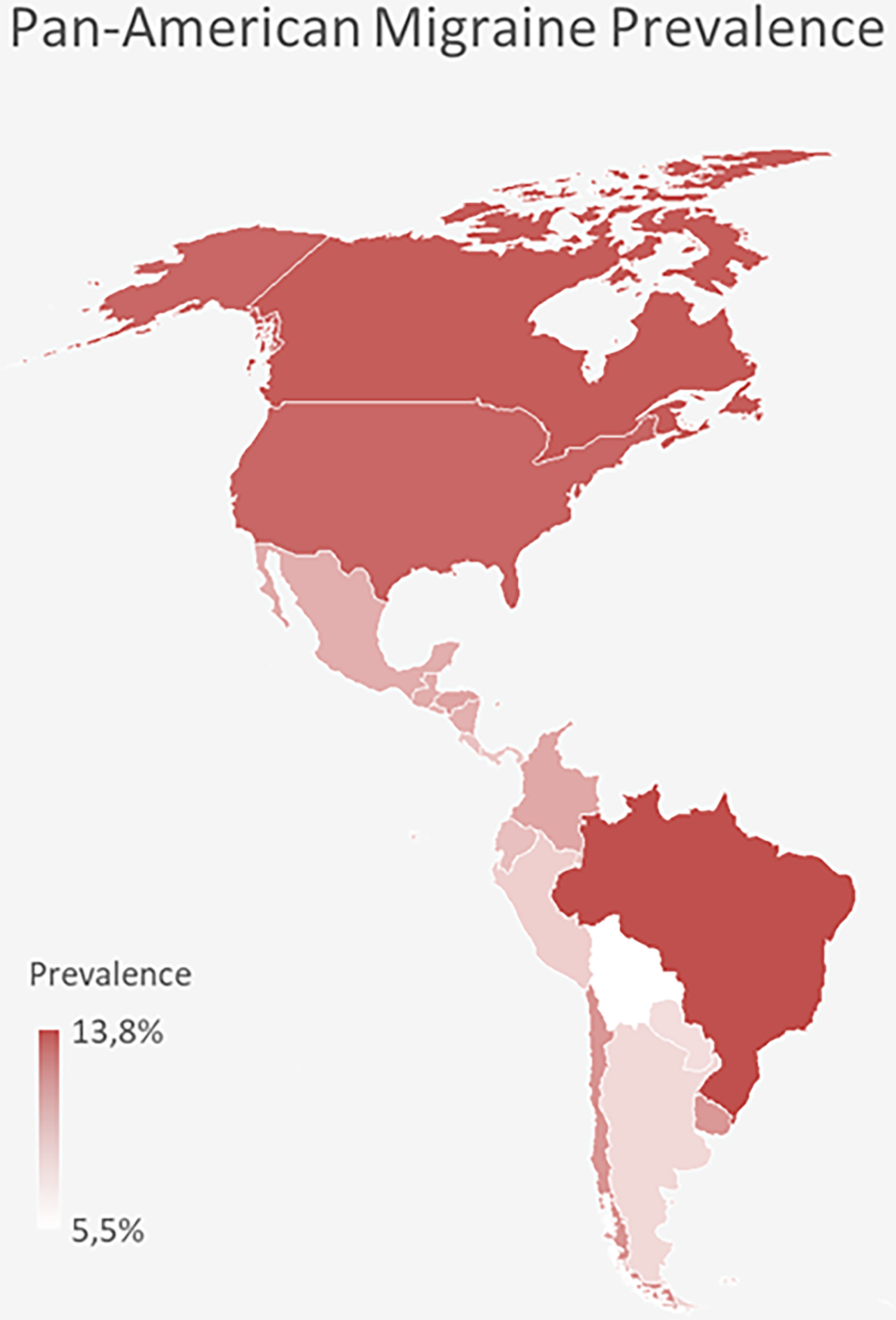
Prevalence of migraine across the americas, color-coded.

Migraine prevalence across the americas divided by sex and age.
Age-standardized prevalence of migraine by country and sex with 95% confidence intervals.

Migraine prevalence peaked in women between ages 30 and 54, while in men, it remained almost stable with a slight increase around the third decade of life (Figure 2).
On average, migraine sufferers reported experiencing headaches 6.5 days per month (median = 4), with 14% suffering fifteen or more monthly headache days. As a result, the mean prevalence of chronic migraine was estimated at approximately 1.3%.
The migraine burden, measured by YLDs, was highest in the United States and lowest in Bolivia. When comparing disease burden rankings to migraine prevalence rankings, nine countries ranked higher, eight ranked lower, and two had identical rankings (Figure 4 and Table 2).

Left: color-coded representation of migraine burden across the Americas based on YLDs. Right: Comparison of prevalence ranks (left column) and burden ranks (right column).
Migraine-Related years lived with disability (YLDs) across 19 countries in the americas.

Discussion
This study provides a comprehensive regional overview of migraine prevalence and disability burden, based on data from over 16,000 individuals across 19 countries in the Americas, highlighting significant geographic and demographic variations with critical public health implications.
Regional comparisons of prevalence and burden
Migraine prevalence in the Americas (9.7%) remains well below the global estimate of 14% reported by GBD 15 and is also lower than that observed in AMPP, 16 but is consistent with prior regional population-based estimates.5,17 Importantly, the GBD study included both definite and probable migraine in its case definition—consistent with recommendations from the Global Campaign Against Headache—whereas the AMPP study, and the present analysis, considered only definite migraine. This methodological distinction largely explains the higher global estimates reported by GBD and underscores the relevance of explicitly defining diagnostic criteria when comparing population-based migraine studies. 18 The prevalence of chronic migraine (∼1.3%) also aligns with previous reports, supporting the validity of our estimate. Despite this moderate prevalence, the estimated YLDs for migraine in the Americas (∼720 per 100,000) would place it as the second most disabling condition globally, just behind low back pain and ahead of major depressive disorder, highlighting its substantial public health impact. 19
Our data also reveal notable inter-country differences. Brazil reported the highest prevalence (13.8%), followed by Canada (13.2%) and the United States (12.7%), underscoring marked cross-country variation even after demographic standardization. Conversely, countries such as Bolivia (5.5%) and Paraguay (7.1%) exhibited the lowest prevalence. These differences may reflect a combination of true epidemiological variation and methodological factors, including sampling, response rates, and case ascertainment, despite migraine being identified using standardized ICHD-3 criteria. Larger discrepancies observed across studies—particularly those including probable migraine—are likely to be influenced by differences in case definition and diagnostic hierarchy. Within our dataset, the observed variations potentially reflect both underlying epidemiological differences and methodological influences, providing informative comparative patterns across countries.
Countries with similar mid-level prevalence, such as Colombia (9.6%) and Chile (10.4%), showed markedly different levels of burden (1001.6 vs. 576.6 YLDs), emphasizing the importance of attack frequency and duration when assessing disease impact. El Salvador (8.8% prevalence, 938.2 YLDs) and Costa Rica (8.2%, 813.9 YLDs) exhibited a high burden relative to their prevalence, suggesting more severe or poorly controlled migraine presentations. Paraguay (7.1%, 551.5 YLDs), despite having one of the lowest prevalence estimates, carried a disproportionately high burden, underscoring the need for targeted interventions. In contrast, Bolivia (5.5%, 316.7 YLDs) had the lowest overall burden in both absolute and relative terms.
Age and sex patterns
Our age- and sex-specific data confirm well-established patterns in migraine epidemiology, while also revealing important nuances. 18 Female participants consistently reported higher prevalence across all age groups, peaking at 15% between ages 30 and 54. Notably, the distribution in females revealed a bimodal pattern, with a rise from early adulthood (18–23 years) to a first peak at 36–41 years, followed by a decrease (48–53) and a second peak at 54–59 years — a pattern consistent with hormonal fluctuations — particularly in estrogen levels — during reproductive and perimenopausal phases. 20 In contrast, no bimodal distribution was observed in males, whose prevalence remained lower and more stable, peaking at 8% between ages 36 and 41. These findings underscore the disproportionate impact of migraine on women and the need for sex-specific public health strategies. 21
While prevalence declined markedly after age 60 in both sexes—consistent with previous reports of natural remission 18 —men aged 66 and above reported slightly higher rates than women (6,4% vs. 5,6%), suggesting a narrowing of the sex gap in later life. These findings underscore the disproportionate burden of migraine in women during the most productive life stages and highlight the need for age- and sex-sensitive public health strategies.3,22–24
Public health implications
Observed variations in YLD-to-prevalence ratios underscore the need for targeted responses.25,26 For instance, El Salvador, Panama, and Costa Rica exhibited disproportionately high YLDs relative to prevalence, suggesting the need to address factors such as attack severity, frequency, and access to effective treatment. Meanwhile, countries like Paraguay may benefit from evaluating the disabling features of migraine even in low-prevalence settings. Countries with high migraine burden, such as Brazil, Canada, and Colombia, should prioritize preventive strategies and patient education on appropriate medication use.25,26
Strengths, limitations and future directions
This study provides an approximate regional overview of migraine burden, with several strengths but also important limitations. Notably, unlike the Global Burden of Disease estimates 3 —which derived migraine attack duration from indirect pooled global population-based, with limited direct information from studies in the region (historically one from the United States 27 and one from Chile, 28 and more recently only one from Peru)—this study directly collected individual-level data on attack frequency and duration across 19 countries. This enables a more regionally specific assessment of time spent in the ictal state, a key driver of disability-adjusted burden.
Although we did not cross-check or externally validate the methods we employed, it is reassuring that our data are in line with previous single-country29,30 and multicentric studies 5 from the region. One exception is Peru, where a recent study reported significantly higher prevalence (22.8%) rates than ours (7.8%). 17 The most likely contributors to the observed differences are the inclusion of probable migraine in that study and the overrepresentation of high-altitude regions, which are associated with increased migraine risk. When probable migraine was also included in our analysis, the combined prevalence in Peru (26.3%) became comparable to that reported by Quispe et al., indicating consistency with previously published national estimates. Aside from that study, our findings remain consistent with prior regional evidence.31,32
While face-to-face interviews are often considered desirable, implementing them across such a widespread territory would have been virtually impossible. First, allocating the necessary resources for this methodology would be unreasonable in several countries in the region, many of which are concurrently facing several urgent health priorities. Second, geographic barriers would have severely limited fieldwork feasibility, and in some locations, interviewer safety could not be guaranteed. As a pragmatic alternative, we employed an online survey approach, which is increasingly recognized as valid methodology in certain contexts,33,34 including migraine epidemiology. 35 In particular, for conditions where respondents may experience embarrassment or stigma —such as migraine— anonymous self-reporting has been shown to enhance disclosure and data quality. 36
Nevertheless, several limitations must be acknowledged. First, the reliance on self-reported data may introduce recall bias, particularly concerning attack frequency and duration. While this methodology differs from face-to-face clinical interviews, previous studies in the region—such as the American Migraine Prevalence and Prevention (AMPP) study by Lipton et al. 27 —have shown that structured, self-reported data can yield valid and pragmatic insights in large-scale headache research. Second, due to the nature of our sampling strategy, precise response rates could not be determined, which may have introduced some bias. However, outreach and recruitment procedures were broadly similar across countries and demographic groups, which likely minimized systematic bias. Third, while the questionnaire was carefully translated and reviewed for conceptual equivalence, minor cultural differences in interpretation across countries may have influenced responses. Fourth, cultural and environmental factors may shape how migraine is experienced, reported, and managed across countries, contributing to the observed variability in both prevalence and burden; for example, slightly higher prevalence in Brazil and the USA/Canada may reflect these influences.
Overall, our findings should be interpreted in the context of the study's methodological and practical constraints. Despite our best efforts to address the inherent challenges of a large, multicounty study, certain methodological compromises were unavoidable. The data presented here therefore represent not the ideal conditions for migraine epidemiology research, but the best achievable evidence within the contextual, logistical, and resource constraints of the region.
Future studies should consider incorporating clinical validation, longitudinal designs, and more detailed evaluations of healthcare access and treatment outcomes. Such efforts will be crucial for identifying drivers of regional differences and designing targeted, context-specific interventions—particularly in underserved populations.
Conclusion
This study provides new and valuable data on migraine prevalence and burden in the Americas. By integrating both prevalence and YLDs estimates, we highlight substantial cross-country disparities that warrant tailored public health responses. Countries with high prevalence and burden—such as Brazil, Canada, and the United States—should prioritize access to preventive care and educational initiatives. Meanwhile, countries with moderate or low prevalence but proportionally high burden—such as El Salvador, Panama, and Paraguay—may benefit from targeted strategies to reduce attack duration and disability. These findings deepen our understanding of the regional impact of migraine and lay a foundation for future research and intervention planning.
Article highlights
First standardized, multicountry study of migraine prevalence and burden across 19 countries from Canada to Chile.
Despite a lower regional prevalence than the global average, migraine ranks higher in disability burden (YLDs) than previously recognized.
Significant variation between countries, with some showing disproportionately high burden relative to prevalence.
Findings highlight the need for tailored public health strategies, especially in countries with low prevalence but high disability impact.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261420837 - Supplemental material for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS)
Supplemental material, sj-docx-1-cep-10.1177_03331024261420837 for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS) by Marco Lisicki, Joe Muñoz-Cerón, Elder Machado Sarmento, Adriana Polycarpo Ribeiro, Ana Carolina de Assis Dantas, Leandro Lara do Prado, Ana Karolina de Nunes, Arao B. Oliveira, Marcelo Moraes Valença, Juliana Ramos de Andrade, Karina Vélez-Jiménez, Ildefonso Rodriguez-Leyva, Alex Rodrigo Espinoza Giacomozzi, Ernesto Bancalari, Raúl Juliet, Pablo Schubaroff and Mario F. P. Peres in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261420837 - Supplemental material for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS)
Supplemental material, sj-docx-2-cep-10.1177_03331024261420837 for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS) by Marco Lisicki, Joe Muñoz-Cerón, Elder Machado Sarmento, Adriana Polycarpo Ribeiro, Ana Carolina de Assis Dantas, Leandro Lara do Prado, Ana Karolina de Nunes, Arao B. Oliveira, Marcelo Moraes Valença, Juliana Ramos de Andrade, Karina Vélez-Jiménez, Ildefonso Rodriguez-Leyva, Alex Rodrigo Espinoza Giacomozzi, Ernesto Bancalari, Raúl Juliet, Pablo Schubaroff and Mario F. P. Peres in Cephalalgia
Supplemental Material
sj-docx-3-cep-10.1177_03331024261420837 - Supplemental material for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS)
Supplemental material, sj-docx-3-cep-10.1177_03331024261420837 for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS) by Marco Lisicki, Joe Muñoz-Cerón, Elder Machado Sarmento, Adriana Polycarpo Ribeiro, Ana Carolina de Assis Dantas, Leandro Lara do Prado, Ana Karolina de Nunes, Arao B. Oliveira, Marcelo Moraes Valença, Juliana Ramos de Andrade, Karina Vélez-Jiménez, Ildefonso Rodriguez-Leyva, Alex Rodrigo Espinoza Giacomozzi, Ernesto Bancalari, Raúl Juliet, Pablo Schubaroff and Mario F. P. Peres in Cephalalgia
Supplemental Material
sj-docx-4-cep-10.1177_03331024261420837 - Supplemental material for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS)
Supplemental material, sj-docx-4-cep-10.1177_03331024261420837 for Pan-American migraine prevalence: Findings from the Americas’ migraine observatory study (AMIGOS) by Marco Lisicki, Joe Muñoz-Cerón, Elder Machado Sarmento, Adriana Polycarpo Ribeiro, Ana Carolina de Assis Dantas, Leandro Lara do Prado, Ana Karolina de Nunes, Arao B. Oliveira, Marcelo Moraes Valença, Juliana Ramos de Andrade, Karina Vélez-Jiménez, Ildefonso Rodriguez-Leyva, Alex Rodrigo Espinoza Giacomozzi, Ernesto Bancalari, Raúl Juliet, Pablo Schubaroff and Mario F. P. Peres in Cephalalgia
Footnotes
Acknowledgments
We thank the support from Pfizer.
Author contributions
Marco Lisicki: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing.
Mario F. P. Peres: Conceptualization; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Validation; Writing – review & editing.
Adriana Polycarpo Ribeiro; Ana Carolina de Assis Dantas; Leandro Lara do Prado; Ana Karolina de Nunes: Funding acquisition; Methodology; Validation; Writing – review & editing.
Joe Muñoz-Cerón; Elder Machado Sarmento; Arao B. Oliveira; Marcelo Moraes Valença; Juliana Ramos de Andrade; Karina Vélez-Jiménez; Ildefonso Rodriguez-Leyva; Alex Rodrigo Espinoza Giacomozzi; Ernesto Bancalari; Raúl Juliet; Pablo Schubaroff: Writing – review & editing.
Consent to participate
All participants provided informed consent.
Consent for publishing
All authors reviewed the manuscript, approved the final version, and agreed to its publication.
Data availability statement
Data available from the authors upon a reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study protocol was approved by the Brazilian National Research Ethics Committee (CONEP), under CAAE 82972424.4.0000.0076.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Pfizer Brazil.
Open practices
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.